
Abstract
Background:
Molecular testing for oncogenic gene mutations and chromosomal rearrangements plays a growing role in the optimal management of thyroid nodules, yet lacks standardized testing modalities and systematic validation data. Our objective was to assess the performance of molecular cytology on preoperative thyroid nodule fine-needle aspirates (FNAs) across a broad range of variables, including independent collection sites, clinical practices, and anatomic pathology interpretations.
Methods:
Single-pass FNAs were prospectively collected from 806 nodules 1 cm or larger by ultrasonography at five independent sites across the United States. Specimens were shipped in a nucleic acid stabilization solution and tested at a centralized clinical laboratory. Seventeen genetic alterations (BRAF, KRAS, HRAS, and NRAS mutations, PAX8-PPARG and RET-PTC rearrangements) were evaluated by multiplex polymerase chain reaction and liquid bead array cytometry in 769 FNAs that met inclusion criteria. Cytology, histology, and clinical care followed local procedures and practices. All results were double-blinded.
Results:
Thirty-two specimens (4.2%) failed to yield sufficient nucleic acid to generate molecular data. A single genetic alteration was detected in 80% of cytology malignant cases, 21% of indeterminate, 7.8% of nondiagnostic, and 3.5% of benign cases. Among 109 nodules with surgical histology reference standard, oncogenic mutations were present in 50% of malignant nodules missed by cytology. There were 14 cancers not identified by cytology or molecular tests, including 5 carcinomas with histologic sizes less than 1 cm (3 multifocal) and 8 noninvasive follicular variants of papillary carcinoma (4 encapsulated). No mutations were detected in 89% of the nodules benign by histopathology with 6 false-positive molecular results in 5 adenomas (2–5.5 cm) and 1 cystic nodule with an incidental papillary microcarcinoma (0.15 cm). The posttest probability of thyroid cancer was 100% for nodules positive for BRAF or RET-PTC, 70% for RAS or PAX8-PPARG, and 88% for molecular cytology overall.
Conclusions:
Centralized and standardized molecular testing for genetic alterations associated with a high risk of malignancy efficiently complements the local cytopathologic diagnosis of thyroid nodule aspirates in the clinical setting. Actionable molecular cytology can improve the personalized surgical and medical management of patients with thyroid cancers, facilitating one-stage total thyroidectomy and reducing the number of unnecessary diagnostic surgeries.
Introduction
C
However, in 20% to 30% of nodule aspirates, a definitive diagnosis cannot be made due to the inherent limitations of the aspiration procedure and/or overlapping cytomorphological features between benign and malignant lesions (1,2,5). Patients with cytologically “indeterminate” nodules are most often recommended to undergo surgery, even though a majority of these lesions will prove to be benign by postsurgical histopathology. Furthermore, for 10% to 40% of the patients with a confirmed histologic thyroid cancer but who underwent only a hemi-thyroidectomy, a second surgery is often required to “complete” the thyroidectomy (2,6). Addressing these shortcomings, several initial studies have shown that molecular testing in preoperative aspirates can improve the diagnostic yield of cytopathology (7 –9). Specifically, when a series of oncogenic gene mutations and chromosomal rearrangements were combined in a “molecular panel,” 61% to 75% of malignant nodules with indeterminate cytology were identified, thus improving the personalized surgical management of patients with thyroid cancer and reducing the number of unnecessary and two-step surgeries (10 –12). More recently, an RNA-based, 142-gene expression classifier was also shown to correctly identify approximately 50% of benign nodules with indeterminate FNA cytology, thus further reducing the number of unnecessary diagnostic surgeries (13).
These seminal studies have driven the clinical adoption of molecular cytology and risk-based management of thyroid cancer. A fundamental limitation, however, is that the predictive value of a molecular test (posttest probability of cancer) depends upon the pretest probability of cancer in the population evaluated (cancer prevalence); that is, the predictive value depends upon the performance of preoperative cytology and postoperative histology. Unfortunately, the high intraobserver and interobserver variability of interpretation of pathologic features can lead to broad differences in prevalence across institutions, including centers of excellence that follow the Bethesda System for reporting thyroid cytopathology (1,3). Although oncogenic gene alterations have been evaluated in multiple patient populations, these single-institution studies were not always prospective or fully blinded and relied on an array of molecular techniques with different performance characteristics (10 –12,14,15). In a large, blinded multisite molecular study, indeterminate aspirates were tested prospectively at a centralized laboratory using a single gene expression technology for all study sites; however, the pretest and posttest probabilities of cancer were not determined relative to representative local histopathology (13). Finally, very limited data are currently available regarding the utility of molecular testing in aspirates classified as inadequate for cytopathologic evaluation. “Nondiagnostic” or “unsatisfactory” is a very heterogeneous reporting category that can represent up to 20% of all preoperative FNAs and for which a second invasive FNA procedure is usually performed (1,6,16).
The aim of the present study was to prospectively evaluate the performance of FNA cytology combined with the molecular analysis of 17 oncogenic gene alterations in a multisite, double-blinded study. The reference diagnosis was established using local pathology expertise while molecular testing was performed using standardized molecular methods at a centralized clinical laboratory (17 –19). All cytologic, molecular, and histologic results were collected and analyzed, including aspirates with nondiagnostic cytopathology.
Materials and Methods
Study design and protocol
The prospective noninterventional study was designed to evaluate subjects with thyroid nodules 1 cm or larger as part of their routine diagnostic workup in five different academic or community health care centers. Diagnostic and treatment procedures entirely followed local standard clinical practices and the study protocol was approved by investigational review boards at each of the five participating sites in three different states (California, Massachusetts, and Texas). Following the standard of care FNA, one additional needle stick was collected in RNARetain® (Asuragen Inc., Austin, TX), a single-use vial containing a nontoxic solution for the preservation and stabilization of intracellular nucleic acids. Specimens were stored at room temperature for 2 hours, then below −15°C for batch-shipping via FedEx priority overnight on cold packs to a centralized Clinical Laboratory Improvement Amendments (CLIA)-certified laboratory in Austin, Texas (Asuragen Clinical Laboratory) where nucleic acid extraction and molecular testing were performed. Ultrasound-guided nodule aspiration, cytologic diagnosis, and postsurgical histologic diagnosis were performed at each study site using site-specific procedures. The study manager (S.B.H.) and the clinical manager (E.L.) reviewed and compiled the cytology and histology reports provided by each site and had access to all molecular data and analyses. Each of the authors received and reviewed their respective study results and approved the decision to submit the manuscript.
Study subjects were enrolled between July 2010 and October 2012 and provided a written informed consent to participate in the study. All specimens collected were deidentified. No protected health information or other information identifying patients was released and no molecular results from this investigation were used for treatment decisions. Among the 618 study participants (806 FNA), 18 subjects (37 FNA) were excluded as a result of a protocol deviation. Specifically, 1 study subject was younger than 18 years. Thirteen FNA were duplicate aspirations collected at a later clinical visit but obtained from an identical thyroid nodule (and study subject) previously enrolled. To avoid study bias, only the specimens representative of the diagnostic workflow, that is collected during the initial FNA biopsy visit, were included in the comparative analysis. Eight additional aspirates from 6 subjects did not meet the inclusion criteria because of deviations during specimen shipping or handling (1 FNA received in a broken empty collection vial, 2 FNA received after delayed shipping, 5 purified nucleic acids not stored below −15°C). Finally, 15 consecutive specimens from 11 subjects collected at a single study site showed an uncharacteristic molecular result (double-positive for PAX8-PPARG and RAS) suggesting external cross-contamination during processing of this series. To avoid study bias, these 15 specimens were all excluded. Additional information on the specimen set and on data collection and tracking is available in the Supplementary Materials and Methods (available online at
Molecular Testing
All eligible specimens were evaluated for the presence of 17 distinct genetic alterations: 14 single nucleotide substitutions in the BRAF, HRAS, KRAS, or NRAS genes and 3 fusion transcripts, PAX8-PPARG, RET-PTC1, and RET-PTC3 (Supplementary Table S1). Total nucleic acid (TNA) was extracted from RNARetain-preserved FNAs using a proprietary laboratory-validated method and quantified using a NanoDrop ND1000 (NanoDrop Technologies, Waltham, MA). DNA- and RNA-based tests were performed using 20 or 40 ng of purified TNA, a single qualitative multiplex assay system based on the Signature technology platform (17 –19) and reagents developed, manufactured, qualified, and released under controlled processes by Asuragen Inc., Austin, Texas. To generate qualitative positive or negative test results, assay outputs (median fluorescence intensity signals) were interpreted relative to target-specific, predetermined, laboratory-validated qualitative cutoff values corresponding to an analytical sensitivity of 0.5% to 2.5%. Additional information on molecular methods is available in the Supplementary Materials and Methods.
Data analysis
Diagnostic performance was calculated using standard statistics and contingency tables for qualitative molecular test results (positive or negative) and gold standard results (malignant or benign histopathology diagnosis for 109 specimens). All nodules with malignant histology and molecular-negative preoperative FNA were classified as false-negative. The 95% confidence intervals were calculated using the exact Clopper-Pearson method for proportions or the method described by Armitage and Berry (20) for odds ratios (21). p Values were calculated at 95% confidence using the Fisher exact test for categorical variables or the Student's t-test for continuous variables.
Results
Study design and population
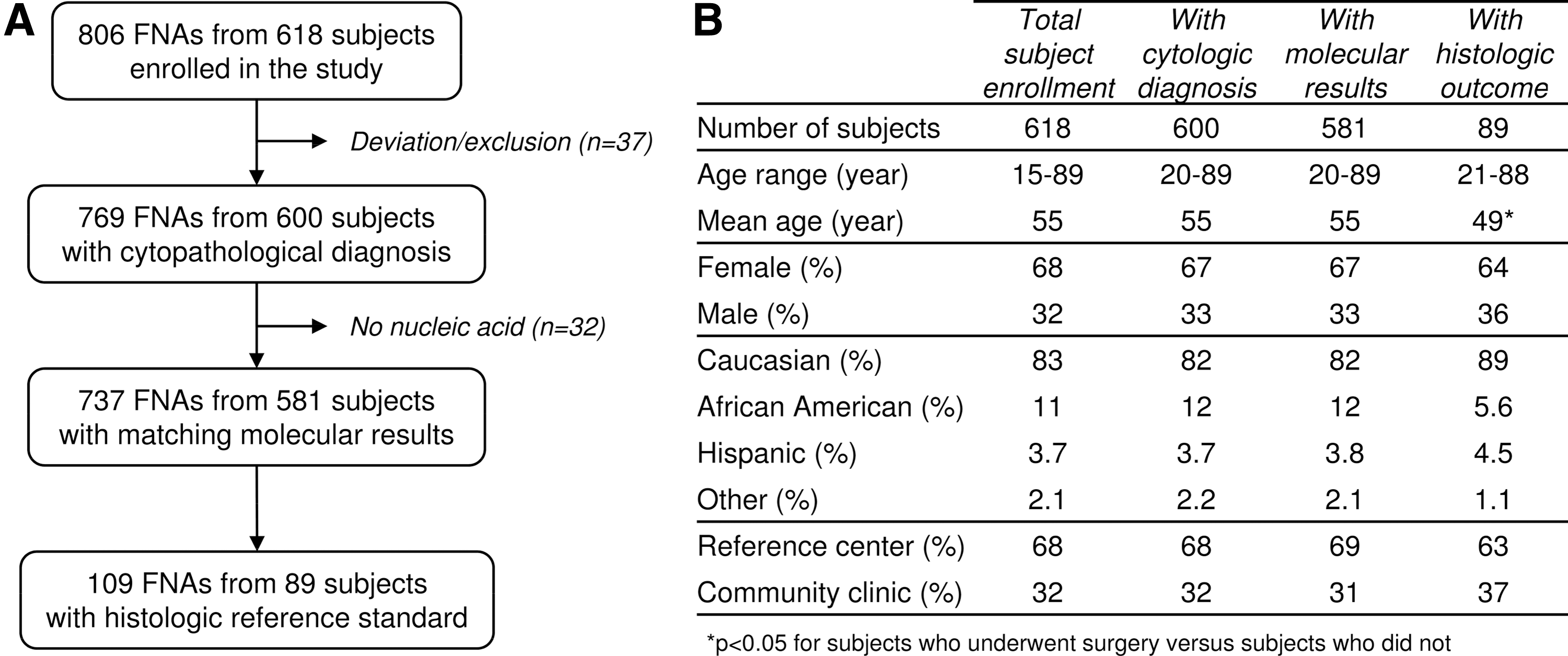
A total of 806 nodule aspirates from 618 study subjects were prospectively collected at 5 clinical sites in the United States over a 27-month period (Fig. 1A). Of the 806 specimens, 37 were determined to be ineligible for evaluation because of a protocol deviation during subject enrollment (n=14) or specimen handling (n=23; see Materials and Methods). Among the remaining 769 FNAs that met inclusion criteria and were processed, 32 contained an insufficient amount of nucleic acids for testing (4.2%). Therefore, the study cohort consisted of 737 independent nodule aspirates from 581 subjects. At the completion of the study, a valid postsurgical histopathology reference diagnosis was available for 109 specimens (89 study subjects, median follow-up time of 65 days after FNA collection). The study population ranged in age from 20 to 89 years old and was mostly female (68%) and Caucasian (83%; Fig. 1B). Study subjects were enrolled in 2 large hospitals/reference centers (68%) and 3 smaller community clinics (32%). There was no statistical difference between the enrollment, cytology, molecular, and histology study groups for sex, ethnicity, or specimen origin (p>0.05). The mean age was 55 years for the enrolled population and 49 years for the subjects who underwent surgery (p<0.001).
Study overview.
Cytology and molecular results
Among 737 aspirations, 546 (74%) were classified as benign and 30 (4.1%) as malignant according to the Bethesda system for reporting thyroid cytopathology (Table 1). A total of 97 aspirates (13%) were cytologically indeterminate with the AUS/FLUS (atypia of undetermined significance or follicular lesion of undetermined significance), FN/FSN (follicular neoplasm or suspicious for a follicular neoplasm), and SM (suspicious for malignancy) categories each representing 43%, 39%, and 18%, respectively. Sixty-four nodule aspirates (8.7%) were inadequate for cytologic evaluation (nondiagnostic or unsatisfactory, ND/U). Single mutations (BRAF, KRAS, HRAS, or NRAS) or fusion transcripts (PAX8-PPARG or RET-PTC) were detected in all Bethesda categories with a positivity rate ranging from 3.5% for benign nodules to 80% for malignant nodules (Table 1). Results are also presented per study site and per cytopathology diagnostic category in Supplementary Tables 2 and 3. The molecular detection rate was 5.6% to 15% across sites (p>0.05) and 9.2% overall (68/737). Mutations in the RAS oncogene family were detected most frequently (n=33, 4.5%) followed by BRAF (n=26, 3.5%). The fusion transcripts PAX8-PPARG (n=7) and RET-PTC (n=2) each represented less than 1% of the evaluated FNAs.
ND/U, nondiagnostic or unsatisfactory; AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance; FN/SFN, follicular neoplasm or suspicious for a follicular neoplasm; SM, suspicious for malignancy.
Correlation with histopathologic diagnosis
Results from local cytopathology and centralized molecular testing were compared against the gold standard histopathology diagnoses established at each study site (Table 2). A total of 56 nodules of 737 (7.6%) were histologically malignant. A definitive cytologic diagnosis of malignancy was made in 50% (28/56) of these nodules while oncogenic mutations were identified in 66% (37/56). Eighty-five percent (23/28) of the nodules malignant by cytology were positive for one of the genetic alterations evaluated, most commonly BRAF mutations (19/23 or 83%). All cytologically malignant nodules were confirmed as malignant by histology, including 5 carcinomas negative by molecular testing. Among the 26 aspirates benign by cytology with a postsurgical histologic diagnosis, 1 was positive for RAS and proved to be a 2 cm papillary carcinoma, while 3 were positive for RAS or PAX8-PPARG and were histologically benign. Among the 53 aspirates indeterminate by cytology, an oncogenic mutation was detected in 11 specimens of 25 with confirmed malignant outcome (44%). Conversely, 25 of 28 histologically benign nodules were mutation negative (89%). Finally, 2 nodules with ND/U aspirates were malignant by postsurgical histology and both were mutation positive (BRAF or PAX8-PPARG).
ND/U, nondiagnostic or unsatisfactory; AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance; FN/SFN, follicular neoplasm or suspicious for a follicular neoplasm; SM, suspicious for malignancy.
Within the histology study group, BRAF V600E was the most frequent mutation, detected in 21 of the 43 aspirates positive by molecular testing (49%; Table 2). All of the nodules positive for a BRAF mutation, including 19 with malignant cytology (90%), were subsequently diagnosed as papillary carcinomas. Mutations in the RAS genes were the second most common genetic alterations (17/43 or 40%). Thirteen RAS mutations (3 HRAS, 1 KRAS, and 9 NRAS) were detected in papillary carcinomas while 4 (2 HRAS and 2 NRAS) were detected in benign nodules. Fusion transcripts were detected in 3 papillary carcinomas and 2 benign nodules (12% of positive specimens). Overall, oncogenic mutations were detected in 44% (11/25) of the thyroid cancers with indeterminate cytology and 48% (13/27) of the cancers without a definitive benign or malignant cytologic diagnosis (Table 2). The presence of any genetic alteration in preoperative thyroid FNA was strongly associated with a confirmed histopathologic malignancy (p<0.001) and was 100% (23/23) for BRAF and RET-PTC and 70% (14/20) for RAS and PAX8-PPARG.
Performance of molecular cytology
The overall performance characteristics and 95% confidence interval for the molecular panel are summarized in Table 3. The diagnostic sensitivity and specificity of molecular testing independent of the cytopathologic diagnosis were 66% and 89%, respectively, with a statistically significant odds ratio (95% confidence interval >1). In nodule aspirates with positive molecular results, the observed posttest probability of thyroid cancer was 86% (positive predictive value or PPV). This performance corresponded to an increase of 35% between the pretest and posttest probabilities of thyroid cancer. When considering only the nodule aspirates without a definitive benign or malignant cytologic diagnosis (53 indeterminate and 2 ND/U), the specificity was similar but all other metrics were lower (Table 3). For combined molecular cytology (molecular positive or malignant cytology scored positive), the sensitivity and specificity were 75% and 89%, respectively, with a PPV of 88%.
Molecular positive scored positive.
Malignant cytology or molecular positive scored positive.
95% CI, 95% confidence intervals; PPV, positive predictive value; NPV, negative predictive value.
There were 6 mutation-positive aspirates classified as benign by local histology at 3 sites, contributing to a strict false-positive detection rate of 11% for molecular cytology (Table 4). Separately, there were 14 malignant nodules with associated indeterminate cytology and negative molecular result that contributed to a false-negative detection rate of 25% (Table 5). Eleven false-negative specimens (79%) were from a single site (p<0.05) and 8 of these cases (73%) had a histologic diagnosis of follicular variant of papillary carcinoma (FVPTC). Although fewer oncogenic mutations were detected in nodules collected at site 2, the specificity and PPV of both molecular testing and combined molecular cytology remained high and similar to the other sites (Table 3).
AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance; FN/SFN, follicular neoplasm or suspicious for a follicular neoplasm.
Elevated expression of miR-146b, miR-221, and miR-375 by polymerase chain reaction.
Positive for HRAS p.G13R by next generation sequencing.
Lower PAX8 mRNA expression.
FV, follicular variant; CT, classic type; SV, solid variant; AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance; FN/SFN, follicular neoplasm or suspicious for a follicular neoplasm; SM, suspicious for malignancy.
Discrepancy analysis
To verify the adequacy of the aspirates with apparent false-negative molecular results, the corresponding residual nucleic acid samples were tested for follicular cell content using an independent quantitative molecular assay targeting the PAX8 transcript specific for thyroid follicular cells (Fig. 2). The 14 true-positive aspirates with a confirmed malignant outcome were used as controls to determine the expected range of PAX8 expression in adequate specimens. Only 3 false-negative specimens had normalized PAX8 expression levels outside the 95% or 99.9% confidence intervals of the PAX8 control range. The 11 other false-negative aspirates had high-quality RNA with a follicular cell content similar to the true-positive controls (p=0.12). Further analysis of the residual nucleic acids suggested that at least 3 FNA specimens had likely been collected from mutation-negative carcinomas overexpressing other oncogenic markers (22 –24) and/or positive for a rare HRAS mutation not included in the molecular panel (Table 5 and data not shown). For the 8 other apparent false-negative aspirates a sampling error or a discrepancy between the cytology, molecular, and histology specimens could not be ruled out.

Evaluation of follicular cell content. Residual nucleic acids from the 14 false-negative (FN) from sites 2, 3, or 4 and 14 true-positive (TP) were tested by quantitative real-time polymerase chain reaction. The graph shows the expression level of PAX8 normalized to the expression level of the B2M internal endogenous control (ΔCt=PAX8 Ct − B2M Ct) plotted against the B2M control signal (Ct). The dash lines represent the 95% and 99.9% one-sided confidence intervals of the normalized PAX8 expression levels in the 14 true-positive controls. There was no significant difference between the true positive specimens from different sites (p=0.42). Ct, cycle threshold.
Discussion
One objective for molecular cytology in preoperative thyroid nodules is to accurately identify malignant lesions following an indeterminate or nondiagnostic cytopathologic diagnosis (2). In the present work, we demonstrate that centralized molecular testing for a panel of oncogenic gene alterations complements the baseline cytologic analysis of thyroid nodules in the clinical setting. Our data further validate the value of this relevant molecular panel for the clinical risk assessment of thyroid nodules and confirm that the performance of molecular testing depends upon local interpretation of pathological features and local distribution and frequency of specific histologic subtypes and associated mutations.
Many of the cytology and molecular results in our prospective, blinded, multisite study were consistent with, and uphold, recently published findings. For example, the rates of indeterminate (13%) and false-negative (3.8%) by cytology were in agreement with data reported in independent multicenter and meta analyses (2,3,13,16). Only 2.9% of the specimens were excluded because of a process deviation and valid molecular results were obtained for 96% (737/769) of tested specimens in all cytologic categories (10 –14). The observed thyroid cancer detection rates were also within the ranges previously reported for cytology (44–59%, 50% observed) and for molecular testing using similar multigene molecular panels (62–78%, 66% observed; Supplementary Table 4) (10 –12). However, rates were lower than anticipated for molecular testing in aspirates without a definitive cytology (61–75%, 50% observed) and for combined molecular cytology (80–90%, 75% observed). These differences were not statistically significant, yet they suggest that an unexpectedly large number of specimens in our study were either inadequate for molecular testing or from thyroid lesions with a low frequency of the oncogenic mutations included in the molecular panel. The use of distinct needle sticks for cytologic and molecular evaluations may also have contributed to some of the discrepancies.
The 14 aspirates from nodules with a negative molecular result and classified as malignant by local histopathology were from study subjects who were 21 to 70 years old, 10 females and 4 males, all Caucasian. Five carcinomas from nodules 1 cm or larger by ultrasonography had a size of 0.2 to 0.9 cm by histology, including 3 multifocal papillary thyroid carcinoma (PTC). Three were shown to have low follicular cell content, suggesting that insufficient nodule sampling could have contributed to the false-negative results. There were also 8 molecular-negative FVPTC, including 4 encapsulated variants, all characterized by the absence of extrathyroidal extension, lymphovascular invasion, or lymph node involvement. These observations are consistent with the previously reported low frequency of oncogenic mutations and low metastatic potential and recurrence risk for encapsulated or well-circumscribed FVPTC (25 –27). In a large study in 513 indeterminate preoperative aspirates, Nikiforov and colleagues (12) further showed that 62% of the malignant nodules with an apparent false-negative molecular result were noninvasive encapsulated FVPTC.
In addition, the differential histologic diagnosis of follicular-pattern lesions, such as encapsulated FVPTC, minimally invasive follicular thyroid carcinoma (FTC), and other well-differentiated tumors of uncertain malignant potential, is well documented and associated with a high interobserver variability in benign/malignant classification (28 –31). Local variations in the interpretation of histologic features can result in variable diagnostic rates of tumors with a low frequency of oncogenic mutations (e.g., encapsulated FVPTC or FTC) which, in turn, can affect the apparent diagnostic sensitivity of molecular testing (12,15,25,27,31). In our study, most false-negative specimens originated from a single site (79%, p<0.05) where the majority of the carcinomas were FVPTC, and 61% were reported as encapsulated FVPTC by local pathology. For the 4 other sites (n=370 specimens analyzed), the cancer detection rates were within the ranges reported in independent molecular studies (10 –12), 63% in indeterminate aspirates (61–75% expected), and 88% for combined molecular cytology (80–90% expected).
There were also 6 nodule aspirates from subjects who were 22 to 59 year old (4 males and 2 females) with a positive molecular result confirmed by retesting and a benign histologic outcome. One specimen was from a 2.0 cm cystic nodule with multinodular hyperplasia and an incidental 0.15 cm papillary microcarcinoma; the 5 others were relatively large (2 to 5.5 cm), well-circumscribed, solitary nodules with benign follicular-patterned lesions and absence of definitive features characteristic of carcinoma. These findings are consistent with the challenges of thyroid histopathologic classification and the presence of PAX8-PPARG and RAS mutations at all stages of thyroid tumorigenesis, including in adenomas, indolent encapsulated FVPTC and preinvasive FTC lacking obvious capsular or vascular invasion (7,12,15). More broadly, these mutation positive cases support the model of a multistep adenoma-carcinoma molecular progression, in which the presence of oncogenic gene alterations would drive the progression of preinvasive or in situ carcinomas (8,12,15).
Three of the six apparent false-positive specimens were benign by cytology, a diagnostic category that would not be evaluated for molecular markers in routine clinical practice (2). The corresponding posttest probability of cancer for a RAS or PAX8-PPARG-positive result was 70% overall and 79% after exclusion of the benign cases, in line with previously published results (Supplementary Table 4) (10 –12). In contrast, all aspirates positive for BRAF or RET-PTC were confirmed malignant by histology (100% posttest probability of cancer). To date, the presence of these oncogenic alterations in preoperative thyroid FNAs has consistently been associated with a malignant diagnosis (10 –12). The knowledge of BRAF mutational status also provides valuable prognostic information because p.BRAFV600E is strongly associated with radioactive iodine resistance and more aggressive features such as local invasion, lymph node metastasis, recurrence, and perhaps higher mortality rate (32 –34). Detection of genetic alterations strongly associated with aggressive phenotypes in preoperative FNAs can therefore facilitate the selection of tailored treatments and further decrease the rate of unnecessary second surgeries by identifying patients who would benefit from initial total thyroidectomy and potential central neck dissection.
Overall, the presence of any oncogenic mutation in preoperative aspirates was strongly associated with malignancy (p<0.001) and the posttest probability of thyroid cancer was 86%. Similar to other validation studies (10 –14), patients in our cohort were managed according to local clinical practices and performance was calculated relative to histopathology. Although widely accepted as the gold standard, this may induce possible selection bias. Ideally, all patients with nodule aspirates would undergo surgical removal and histologic assessment. However, sending all consecutive patients to surgery is not the current standard of care. For example, some patients with AUS/FLUS cytology in our cohort did undergo repeat sampling for secondary cytology or analysis with other molecular tests. If these were benign, patients were typically not referred for surgery. Ultimately, a final histopathologic reference standard was obtained for only 51% of the nodules with AUS/FLUS or FN/SFN cytology, 71% for SM cytology. Therefore, we acknowledge that local clinical procedures may have increased the risk of malignancy or the proportion of specific histologic subtypes with distinct mutation frequencies in the surgical group. In the clinical setting, the local standard of care, performance of pathology and pretest probability of thyroid cancer may be different from our study, and physicians should take this into account when translating these data into clinical practice. The odds ratio (relative difference between the positive and negative likelihood ratios) may provide additional meaningful and clinically relevant information as it is a global indicator of diagnostic test performance independently of the pretest probability of cancer (35). An odds ratio of 15 means that the odds of a true positive result in malignant nodules (37/19) was 15 times higher than the odds of a false-positive result in benign nodules (6/47).
In summary, our prospective multisite study demonstrates that centralized molecular testing in combination with local cytopathologic evaluation of preoperative thyroid nodule FNA can improve the personalized management of thyroid cancer patients. Clinically actionable information was obtained in benign or malignant FNAs as well as in indeterminate and nondiagnostic aspirates, thus reducing the need to perform a diagnostic lobectomy or a second invasive FNA procedure. One inherent limitation of the current molecular panel is that the full mutational spectrum of thyroid carcinoma is not known. Therefore, not all malignant tumors carry one of the 17 genetic alterations evaluated, and it is important to emphasize that, unless the local pretest probability of cancer is known and sufficiently low, a negative molecular result alone should not be used to rule out surgical therapy for nodules with an indeterminate or nondiagnostic cytologic diagnosis. Testing for additional oncogenic gene alterations or novel expression-based markers while maintaining the high specificity required for an efficient “rule in” diagnostic application may further decrease the rate of molecular-negative malignant thyroid nodules in the future.
Footnotes
Acknowledgments
The authors wish to thank Drs. Salman Haq and Chu-Tang Yee as well as Rupali Shinde, Laura Langfield, Julie Krosting, Maura Lloyd, and the personnel from each clinical site that participated in the study.
Author Disclosure Statement
This study was sponsored by Asuragen Inc. S.B.H., B.A., and E.L. are employees of Asuragen. E.K.A. received compensation for his participation in Asuragen's clinical advisory board, and is a consultant to Genzyme, Inc. and Veracyte, Inc. The other authors have no conflicts of interest to declare.