
Abstract
Background:
One possible result of fine-needle aspiration (FNA) in patients with thyroid nodules is “follicular lesion of undetermined significance” (FLUS) or “atypia of undetermined significance” (AUS). The risk of malignancy is relevant information to define appropriate management, and knowledge of predictors of malignancy in these nodules is therefore important. The objective of this prospective study was to evaluate clinical, laboratory, ultrasonographic, and cytological predictors of malignancy in patients with thyroid nodules and FLUS/AUS cytology.
Methods:
The sample consisted of 150 patients with thyroid nodules and an indication for FNA whose cytology was classified as FLUS/AUS according to the Bethesda classification criteria.
Results:
In the second FNA, cytology was nondiagnostic in 2 (1.3%) nodules and benign in 54 (36%), FLUS/AUS cytology persisted in 73 (48.6%), and cytology was suspicious for follicular neoplasm in 11 (7.3%) and for malignancy in 10 (6.6%). The rate of malignancy was 22.6%. Clinical and laboratory data or nodule size were not predictors of malignancy. The rate of malignancy was lower in nodules initially classified as FLUS (10.8% versus 41.3% with AUS). Ultrasonography (US) was also useful for predicting malignancy, with sensitivity, specificity, and positive and negative predictive values of 79.4%, 90.5%, 71%, and 93.75%, respectively. Different malignancy rates were obtained when the two parameters, cytological subcategory and US, were combined: (i) 3.9% for nodules nonsuspicious on US and FLUS, (ii) 11.4% for nonsuspicious nodules with AUS, (iii) 46.6% for suspicious nodules with FLUS, and (iv) 87% for suspicious nodules with AUS.
Conclusions:
The combination of cytological subcategory (FLUS or AUS) and US provides different risks of malignancy for nodules initially classified as Bethesda category III.
Introduction
O
Three possible types of management are recommended by current guidelines for this cytology result: (i) exclusive follow-up (6,7); (ii) repeat fine needle aspiration (FNA), with management being based on the result of the last exam (1,6 –9), or (iii) thyroidectomy without collection of a new sample (6). A fourth option, which is not found in these guidelines (1,6 –9), is core-needle biopsy (CNB) (5,10). The risk of malignancy is relevant information for management decisions, and knowledge of predictors of malignancy in nodules with FLUS/AUS cytology is therefore important.
Although molecular tests are useful in defining the nature of the nodule, these tests are not available at all centers, their cost is high, and greater experience is needed, particularly in the case of FLUS/AUS. Regardless of these limitations, molecular tests alone can be insufficient to define appropriate management. For example, even in the absence of mutations (RAS, BRAF, RET/PTC, PAX8-PPAR-γ rearrangement), 10% of nodules ≥2 cm with FLUS/AUS cytology are malignant (11); 5.4% of nodules with this cytology and expression of genes suggesting a benign nature are carcinomas (12), whereas approximately 60% of nodules expressing genes suggestive of malignancy are benign (12). The information obtained through fluorodeoxy glucose–positron emission tomography (FDG-PET) imaging also has limitations: (i) availability, (ii) cost, (iii) little experience specifically with FLUS/AUS, (iv) an excellent negative predictive value only for nodules >1.5 cm, and (v) a low positive predictive value (13). Therefore, knowledge of clinical, laboratory, ultrasonographic, and cytological predictors of malignancy is interesting, because although they are not sufficient for defining management decisions, they can contribute to the selection of candidate cases for molecular tests.
Specifically in the case of FLUS/AUS, few series have evaluated the value of clinical data (3,4,11,14), laboratory data (4), cytological findings (5), or nodule size (3,4,11,14) for predicting malignancy. A larger number of studies investigating the predictive value of ultrasonography (US) are available (2,3 –5,11,15). These studies included only a subgroup of patients with FLUS/AUS, that is, (i) only individuals referred for repeat FNA (15) or CNB (5) without histology in all patients with the second FNA or CNB being nonbenign; (ii) only patients referred for surgery (11,14), surgery, or CNB (2,4) or surgery or second FNA (3). In view of this selection bias, the results found may not be applicable to patients in whom initial cytology showed FLUS/AUS and the physician needs to define appropriate management. In addition, none of these studies followed a uniform management protocol (i.e., indication for repeat FNA or CNB, decision for exclusive follow-up, or indication for surgery).
The objective of this prospective study was to evaluate clinical, laboratory, ultrasonographic, and cytological predictors of malignancy in patients with thyroid nodules and initial cytology showing FLUS/AUS (1).
Patients and Methods
Design
The study was prospective.
Patients
All patients with a thyroid nodule continuously seen by the authors between 2009 and 2013, with an indication for FNA and initial FLUS/AUS cytology according to the Bethesda criteria (1), were selected. This result corresponded to 9.3% of the cytologies of thyroid nodules.
Protocol
The study was approved by the Research Ethics Committee of our Institution and all subjects gave written informed consent. Based on the unequivocal indication for surgery, patients with (i) voluminous goiter and/or compressive symptoms, (ii) malignant cytology in another nodule, (iii) apparent extrathyroid invasion, (iv) lymph nodes with positive cytology for thyroid carcinoma, and (v) known distant metastases were excluded. Clinical data (sex, age, personal and family history of cancer, history of radiation exposure, use of levothyroxine or antithyroid drugs); measurements of thyrotropin (TSH), calcitonin, and antithyroperoxidase antibodies (TPOAb); ultrasonography (US) classifying nodules as “suspicious” or “nonsuspicious”; and cytological subcategory (AUS or FLUS) were obtained for all patients.
FNA was repeated after 3 months (1,7 –9). When the second cytology was unsatisfactory, FLUS/AUS persisted, or cytology was compatible with follicular neoplasm (FN), suspicious for malignancy, or nondiagnostic, the patients were referred for thyroidectomy. Patients with benign cytology and suspicious nodules on US were also submitted to surgery. Surgery was also indicated for patients with benign cytology and nonsuspicious nodules on US, but the option of follow-up was given.
The study protocol is summarized in Figure 1.
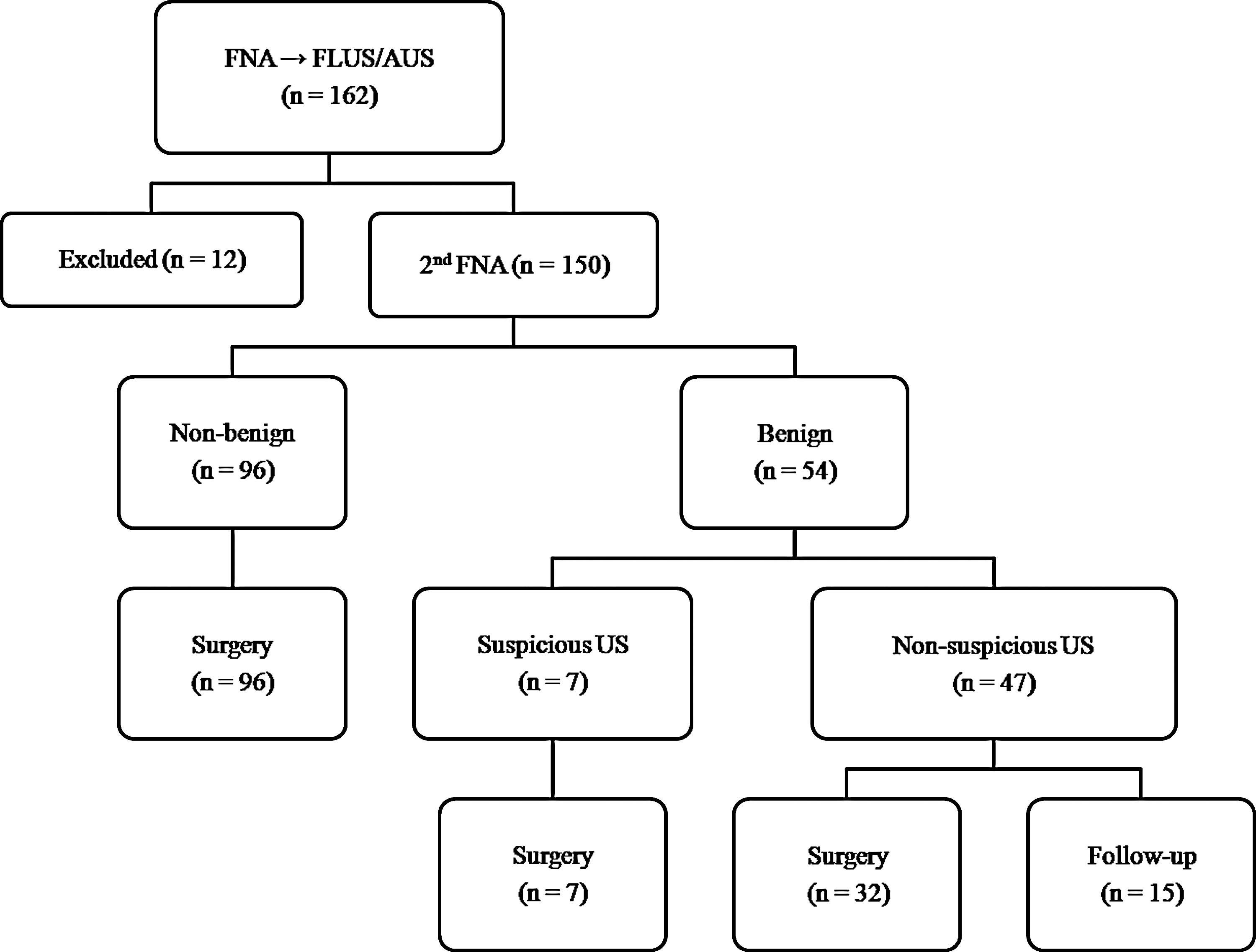
Study protocol. AUS, atypia of undetermined significance; FLUS, follicular lesion of undetermined significance; FNA, fine-needle aspiration; US, ultrasonography.
Ultrasonography
Ultrasonography was performed with a linear multifrequency 14-MHz transducer for morphological analysis (B-mode) and for power Doppler evaluation. The images were analyzed by experienced professionals before FNA. Solid or predominantly solid nodules with the following features were defined as “suspicious”: (i) marked hypoechogenicity (a relatively hypoechoic pattern when compared with the adjacent strap muscle); or (ii) microcalcifications; or (iii) hypoechogenicity combined with microlobulation or irregular margins or a taller-than-wide shape (being greater in the anteroposterior dimension than in the transverse dimension) or predominantly or exclusively central vascularization. This definition has been used at our institution (16 –19) and its value was demonstrated for nodules with benign cytology (16) or FN (17) and nodules suspicious for malignancy (18).
FNA
FNA was performed with a 22-gauge needle and a 5- or 10-mL syringe and was guided by US. Only the histological diagnosis of a thyroid nodule with FLUS/AUS cytology was considered for analysis. The smears (cytology and histology) were analyzed by pathologists experienced in thyroid pathology. The pathologist analyzing the second cytology was unaware of the first cytology result.
Cytology was subcategorized into AUS (cytology demonstrating nuclear atypia, but not diagnostic of suspicious for malignancy or malignant tumor) and FLUS (cellular follicular nodules in which a distinction between FN and a hypercellular hyperplastic nodule is not possible).
Assays
TSH, calcitonin, and TPOAb were measured with a chemiluminescent assay (Immulite, Diagnostic Products Corporation, Los Angeles, CA), with reference values of 0.4–4 mIU/L, up to 5 pg/mL for women and 8.4 pg/mL for men, and up to 35 IU/mL, respectively.
Statistical analysis
Fisher's exact test or the chi-squared test was used to detect differences in the proportion of cases. A p-value of less than 0.05 was considered significant. Multivariate logistic regression was then used to assess the association of individual predictor variables with the risk of malignancy after accounting for other covariates.
Results
A total of 150 patients were included. None of the patients had a history of exposure to ionizing radiation or neck radiotherapy in childhood or adolescence, a previous diagnosis of thyroid carcinoma, a clinical suspicion of multiple endocrine neoplasia type 2, or a family history of medullary carcinoma. Twenty-four patients had a history of papillary carcinoma in a first-degree relative.
Only 15 patients (with a benign second cytology and a nonsuspicious nodule on US, 10 with two benign cytologies) chose not to undergo surgery and opted for observation (Fig. 1). So far, these patients have not shown an increase in nodule size on US or clinical progression (follow-up of 10 to 48 months). The characteristics of the patients and nodules are shown in Table 1.
The p-value was >0.5 for all variables except for a family history of thyroid cancer (p=0.18).
Excluding patients who used levothyroxine.
Basal calcitonin: 18 and 32 pg/mL; after stimulation with calcium: 45 and 75 pg/mL, respectively.
TPOAb, antithyroperoxidase antibodies; TSH, thyrotropin.
In the second FNA, cytology was nondiagnostic in 2 (1.3%) nodules and benign in 54 (36%), FLUS/AUS cytology persisted in 73 (48.6%), and cytology was suspicious for FN or was FN in 11 (7.3%) and was suspicious for malignancy in 10 (6.6%).
The overall rate of malignancy was 22.6% and 28.7% in nodules with persisting FLUS/AUS cytology in the second FNA. These tumors were follicular carcinomas in 3 (2 minimally invasive and 1 angioinvasive) and papillary carcinomas in 31 (follicular variant in 12).
Clinical and laboratory data or nodule size were not predictors of malignancy (Table 1).
Differences were observed between cytological subcategories. The chance of the second FNA being benign was higher in nodules with FLUS versus AUS cytology (45.6% versus 20.7%, p<0.01). In contrast, a second FNA suspicious for malignancy was not seen in nodules with FLUS cytology and was observed in 17.2% of nodules with AUS cytology. The rate of malignancy was lower for nodules with FLUS cytology (10.8% versus 41.3% for nodules with AUS, p<0.001). Among nodules in which FLUS cytology persisted, 15.8% were malignant; among those with AUS cytology on two occasions, 42.8% were malignant (p=0.02). The rates of malignancy considering the results of the first and second FNA are shown in Table 2.
AUS, atypia of undetermined significance; FLUS, follicular lesion of undetermined significance; FN, follicular neoplasm; FNA, fine-needle aspiration; ND, nondiagnostic.
The ultrasonographic criterion used in this study (see Patients and Methods) was useful for predicting malignancy, with a sensitivity, specificity, positive predictive value and negative predictive value of 79.4%, 90.5%, 71%, and 93.75%, respectively. Repeat FNA revealed benign cytology in 7/38 suspicious nodules (18.4%) versus 47/112 (42%) nonsuspicious nodules on US (p=0.01); cytology was suspicious for FN or malignancy in 10 of 38 (26.3%) versus 11/112 (9.8%) (p=0.03); and FLUS/AUS cytology persisted in 21/38 (55.2%) versus 52/112 (46.4%), respectively (Table 3). The risk of malignancy was 71% for suspicious nodules on US and 6.2% for nonsuspicious nodules (p<0.001). The rate of malignancy was 76.2% for suspicious nodules on US and with FLUS/AUS cytology on two occasions, whereas this rate was 9.6% for nonsuspicious nodules (p<0.001) (Table 3).
US, ultrasonography.
Cytological subcategory AUS versus FLUS (odds ratio 3.04 [CI 1.8–5.6]) and US suspicious versus nonsuspicious (odds ratio 7.5 [CI 3.4–12.1]) were independent predictors of malignancy. Different rates of malignancy were obtained when these two parameters were combined (Table 4).
Discussion
First, we highlighted the prospective design of the study using a predefined protocol and procedures that were observed in all participants. Second, the whole group of patients with FLUS/AUS was included—not just a subgroup as done in previous series [referred for repeat FNA (15) or CNB (5); referred for surgery (11,14), surgery or CNB (2,4), and surgery or second FNA (3)]. In view of the absence of this selection bias, we believe that the results of this study are more applicable to the daily scenario of a patient with a thyroid nodule and initial cytological diagnosis of FLUS/AUS in which the physician needs to define a management decision [observation (6,7), repeat FNA (1,6 –9), CNB at centers where this procedure is performed (5,10), molecular tests if available (11,12), direct indication for surgery (6)] and the knowledge of the risk of malignancy is therefore fundamental. Third, since repeat FNA is the most frequently recommended management in these cases (1,6 –9), we routinely perform this procedure and also analyze the result of the second FNA. Finally, histology was obtained in 90% of cases. The few nodules in which histology was not available had a second benign cytology result (10/15 had a third benign FNA), nonsuspicious US, and follow-up without progression; we therefore believe that these findings together make malignancy unlikely, as shown in other series (10,20,21) and in the present study (0/32 cases with a second benign FNA and nonsuspicious US were carcinomas on histology).
A family history of papillary thyroid carcinoma or a personal history of radiation exposure is absent in most individuals with thyroid nodules and, even if present, does not seem to significantly increase the risk of malignancy in cases with FLUS/AUS cytology (4,11,14). Sex or age also does not seem to be a predictor of carcinoma in these nodules (3,4,11,14). The same was observed in the present study. Similar to the present series, nodule size has not been associated with malignancy in most studies (3,4,14). In contrast, Mehta et al. (11) correlated the risk of malignancy specifically in nodules with FLUS/AUS without mutations; the authors observed the absence of carcinoma in nodules <1.85 cm and a linear increase in risk for larger nodules (11). It has been suggested that larger serum concentrations of TSH are associated with a higher risk of malignancy in patients with thyroid nodules. However, no difference in TSH levels was observed between patients with benign and malignant disease in the present study or in a previous study specifically evaluating patients with FLUS/AUS cytology (4). The presence of hypercalcitoninemia would be useful for the diagnosis of possible sporadic medullary thyroid carcinoma, but this finding is uncommon; therefore, serum calcitonin in the absence of a history or cytology suspicious for medullary thyroid carcinoma is not consensually recommended (6,7,9,22).
We found a difference in cytological subcategory. Comparing nodules with AUS versus FLUS cytology, the former presented a higher frequency of suspicious US, a lower chance of a benign second FNA, a higher chance of the second cytology being suspicious for malignancy, and a higher rate of malignancy. Similar results have been reported by Choi et al. using CNB instead of repeat FNA (5). This distinction of subcategories within Bethesda category III has been proposed mainly because of the difference in the risk of malignancy, which can be significantly higher among nodules with doubtful nuclear atypias (5,23 –26).
When US reveals suspicious lymph nodes or apparent extrathyroid extension of the nodule, the diagnosis of malignancy is facilitated, but these cases are rare [4,11,14,15, present series (about 2%)]. In the absence of these findings, specifically when cytology reveals FLUS/AUS, the ultrasonographic features of the nodule seem to help predict malignancy (2–5,15, present series). As observed in the present study, intense hypoechogenicity, the presence of microcalcifications, irregular margins, and a taller-than-wide shape are features that significantly increase the risk of malignancy in nodules with FLUS/AUS cytology (2 –5,15).
The results of this study show that the combination of cytological subcategory (FLUS or AUS) and US provide different risks of malignancy for nodules whose initial cytology result was classified as Bethesda category III. These rates may help the physician decide whether to choose exclusive observation, repeat FNA or CNB (at centers where the procedure is performed), direct indication for surgery, or to select candidate patients for molecular tests (when available).
Footnotes
Author Disclosure Statement
No competing financial interests exist.