
Abstract

At the end of 2004, a 55-yr-old man was referred to one of us (L.C.) for evaluation of a fast growing lump in the neck. The patient denied pain, hoarseness, dysphagia or dyspnea, or a relevant medical history, including neck irradiation or a family history of thyroid cancer. He was a lifetime nonsmoker.
Neck ultrasonography showed a multinodular goiter with a dominant solid nodule in the left lobe measuring 5.2 cm in its largest dimension presenting coarse calcifications. No lymph nodes were detected. Thyroid function tests were normal. Fine needle aspiration cytology was reported as “suspicious for malignancy.” No preoperative calcitonin levels were measured.
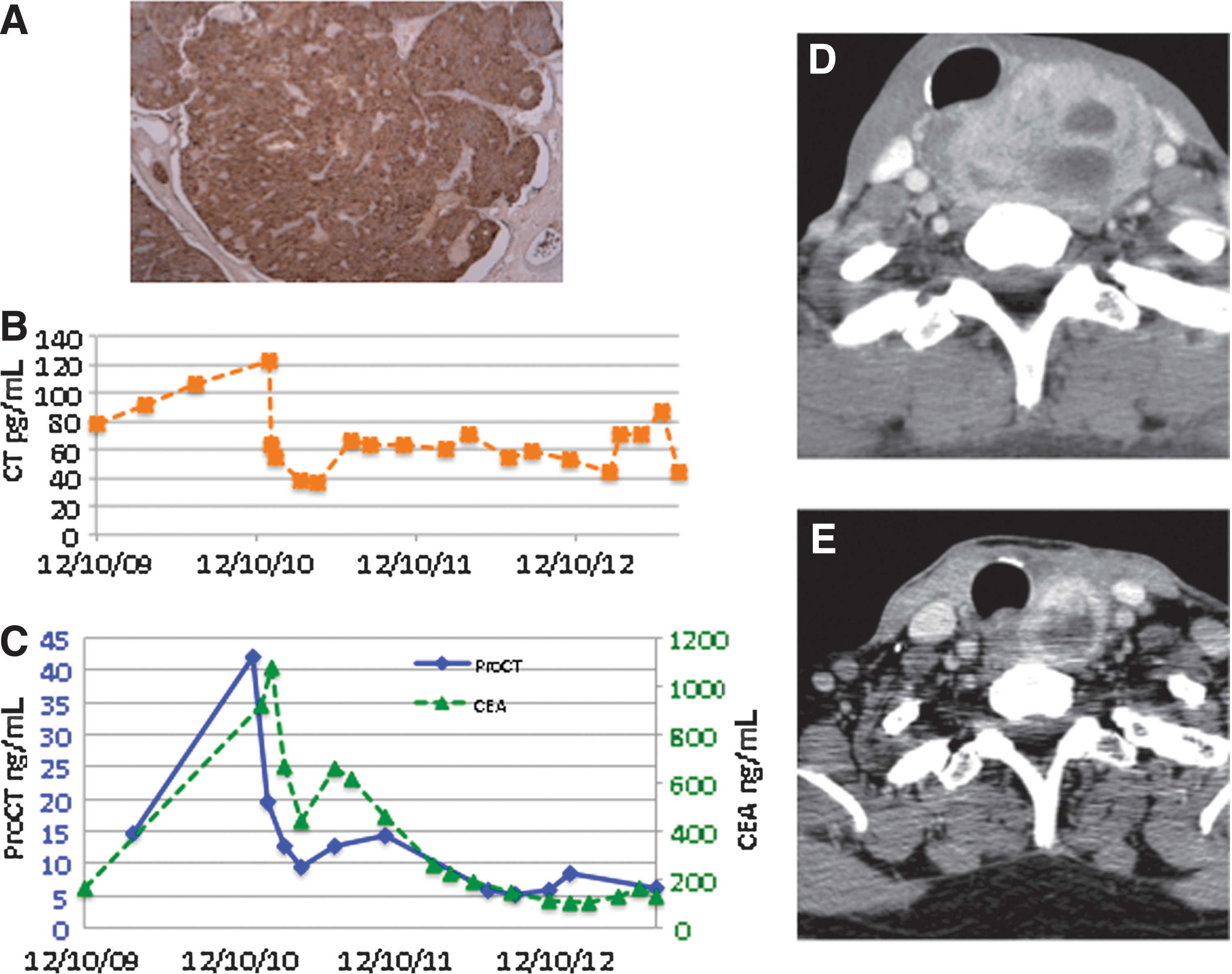
A total thyroidectomy and central neck dissection were performed (March 2005). Pathology demonstrated bilateral medullary thyroid cancer (MTC) with 1 of 5 dissected nodes involved (pT3, pN1a, pMx). Immunostaining (Fig. 1A) was performed instrumentally on a Leica Bond III instrument. Three micrometer thick sections on Superfrost plus slides were submitted to heat mediated antigen retrieval and incubated with a primary calcitonin antibody (Dako polyclonal, 1:12,000) followed by detection with a secondary peroxidase-linked antibody (Leica Bond Polymer refine DS9800).
Postoperative basal and pentagastrin stimulated serum calcitonin levels were <10 pg/mL. The patient was placed on thyroid hormone replacement plus oral calcium supplements and vitamin D to correct postoperative hypoparathyroidism. RET testing, for germline and somatic mutations (exons 5, 8, 10–16), was negative. After a loss to the follow-up period of almost 4 years, the patient returned (January 2009) complaining of hoarseness. Left vocal cord palsy was observed.
Anatomic imaging with computed tomography documented recurrence in the left thyroid bed, adenopathy within the right lung hilum, and hypodense liver lesions, the largest with 34 mm lesion in segment IV, suspicious for metastases. Immunostaining studies carried out in samples from the thyroid bed and liver documented a strong staining reaction for calcitonin. Blood tests revealed serum calcitonin (Immulite 2000, Siemens Healthcare Diagnostic products Ltd.) no higher than 50 pg/mL (normal <10); carcinoembryonic antigen (CEA) (Architect Ci8200, Abbott Diagnostics), 54 ng/mL (normal for nonsmoking <3); and chromogranin (CIS bio international, Gif-Sur-Yvette), 240 ng/mL (normal <100). At this point, measurement of procalcitonin was considered. In the absence of clinical and/or biochemical signs of infection, the procalcitonin concentration (Advia Centaur, Siemens Healthcare Diagnostic products Ltd.) was 10.3 ng/mL (normal <0.5).
In October 2009, the patient was referred to the Portuguese Cancer Center in Lisbon. Restaging by 18F-fluorodeoxyglucose positron emission tomography confirmed the presence of previously identified metastases. In the absence of symptoms other than hoarseness, the patient remained under observation without any medical intervention. One year later, there was clear evidence of progression by Response Evaluation Criteria in Solid Tumors as well as progression of procalcitonin and CEA. After approval by the institutional review board and written informed consent, off-label treatment with Sunitinib (sunitinib malate, SU11248, Sutent®; Pfizer, Inc.) was started, initially 50 mg/day for 28 days, followed by 14 days of no treatment. Interruption periods and dose adjustment were necessary for managing hypertension. After 20 cycles of therapy, restaging showed a sustained response with tumor volume decreased by 46% (Fig. 1D, E). Evolution of tumor markers is summarized in Figure 1B and C.
Serum calcitonin is the most sensitive marker for the diagnosis and follow-up of MTC patients. On rare occasions, MTC without calcitonin secretion has been described (1 –4). To the best of our knowledge, procalcitonin has never been assayed in these cases.
In the patient presented here, preoperative fine needle aspiration cytology did not raise the suspicion for MTC. Calcitonin measurement in the evaluation of thyroid nodules is not a routine, and in this particular case it was not performed. The diagnosis of MTC was established by histological examination and immunostaining. Early postoperative, basal, and post stimulation values of calcitonin were normal.
The main reasons known to interfere with calcitonin measurement were ruled out. The “hook effect” was excluded by measuring calcitonin after serial dilutions and heterophilic antibodies by measuring calcitonin before and after incubating samples in heterophilic-blocking tubes (Scantibodies Laboratory, Inc.).
The dissociation between procalcitonin and calcitonin levels is suggestive of a defective prohormone-processing by convertases as already reported for other prohormones. Despite low levels of serum calcitonin, the strong immunostaining for calcitonin may be explained by the recognition of the calcitonin epitopes present in the prohormone.
In summary, the present case demonstrates that MTC might preferentially secrete procalcitonin. It is conceivable that some MTC might exclusively secrete procalcitonin. This hypothesis should be considered whenever calcitonin is inappropriately low for the extent of disease or undetectable in the serum of patients with tumors showing positive immunostaining for calcitonin.
Footnotes
Author Disclosure Statement
No competing financial interests exist.