
Abstract
Background:
Thyroid hormones are crucial for metabolism in all tissues in humans, including the nervous system and muscles, and could thus affect handwriting, which is the synthesis of complex and fine movements. Hyperthyroidism, characterized by symptoms such as tremor and weakness, could affect handwriting, although this has not been studied yet. The aim of this study was to evaluate handwriting characteristics before and after therapy for hyperthyroid Graves' disease (GD).
Methods:
Twenty-two patients (15 women, 7 men) with untreated GD (median age: 44 years; range: 20–70 years) were asked to write a “standard text” before and 12 months after being rendered euthyroid. The letters underwent a standardized detailed analysis by a handwriting expert, through inspection and stereoscopic microscope and magnifying glass.
Results:
All patients demonstrated handwriting variations, perceptible even to direct observation. Graphological examination showed statistically significant changes after patients become euthyroid, in the following parameters: size of letters (4.5±1.1 vs. 5.9±1.3 mm; p<0.01), distance between letters (62.9±1.1 vs. 55.2±0.8 mm; p<0.01), width of letters (1.75±0.06 vs. 2.2±0 .06 mm; p<0.01), distance between words (216.2±3.2 vs. 198.7±2.4 mm; p<0.01), extension of letters (8.7±0.2 vs. 7.7±0.2 mm; p<0.01), angles (17±0.3 vs. 15.8±0.4 mm; p<0.01), and groove depth (0.2±0.05 vs. 0.4±0.05 mm; p<0.01).
Conclusions:
Hyperthyroid GD was associated with significant changes in handwriting in all patients. Following recovery from hyperthyroidism, a state of hypertrophic and contracted handwriting resulted in greater fluency and fluidity. Variations in handwriting should be included as signs/symptoms in GD.
Introduction
T
Thyroid hormones play a crucial role in the functioning of all tissues in man, including that of the central and peripheral nervous system and muscles (9). Hyperthyroidism is associated with well-accepted symptoms and signs, some of which (e.g., fine distal tremor, fatigue, and muscle weakness) are the consequence of the effects on nerve and muscle tissues.
Handwriting is dependent on complex and delicate movements coordinated by the pyramidal and extra-pyramidal systems. The close interaction between the two ensures the smooth coordinated functioning which leads to the act of handwriting. This is highlighted by several studies on variations in handwriting in subjects treated with neuroleptic drugs, known to induce extra-pyramidal side effects (10). Thus, such variations in handwriting have been demonstrated in patients suffering from alcoholism (11), Parkinson's disease (12), multiple sclerosis (13), various psychiatric disorders (14), and other pathological conditions characterized by tremor.
To our knowledge, with the exception of case reports, there is no systematic study on the influence of hyperthyroidism on aspects of handwriting. Our aim was to investigate the influence of well-characterized GD on a number of handwriting characteristics, at the onset as well as following 12 months of stable euthyroidism, in a paired design.
Patients and Methods
Patients
Consecutive patients >18 years old with untreated overt thyrotoxicosis referred to the Outpatient Thyroid Unit, Department of Internal Medicine, “Ramazzini” Hospital, Azienda USL Modena, Italy, between January 2006 and June 2012 were evaluated for potential inclusion. Overt thyrotoxicosis was defined as an elevated serum free thyroxine (FT4) and/or free tri-iodothyronine (FT3) level with concomitant subnormal serum thyrotropin (TSH) concentrations. The diagnosis of GD was based on the above biochemical criteria, signs, and symptoms suggestive of hyperthyroidism, and an elevated serum TSH-receptor antibody (TRAb) level.
Exclusion criteria were as follows: (a) age <18 years or >70 years; (b) subclinical hyperthyroidism (low/undetectable TSH levels and normal thyroid hormones values); (c) hyperthyroidism not caused by GD; (d) relapse of GD; (e) personal history of Parkinson's disease, multiple sclerosis, diabetes mellitus, vascular disease, previous head injury, chronic liver disease, psychiatric disorders, and/or peripheral neuropathy; (f) use of any medication; (g) smoking; (h) consumption of >3 cups of coffee (espresso) per day; (i) consumption of a daily amount of wine >200 mL (1–2 glasses), or beer >400 mL (2–4 glasses), or spirits >50 mL (1 shot glass).
All patients enrolled at the time of diagnosis and before starting any specific therapy for thyroid disease were asked to write a “standard text” (see below) on a blank sheet of paper, size A4, beneath which another 10 A4 sheets were placed to evaluate the depth of the grooves left by the pen. Immediately following this, the patients started therapy with either methimazole or propylthiouracil, which was titrated individually depending on the results of thyroid function tests. Assessment of thyroid function was performed 4 weeks after initiation of therapy, and every 4–8 weeks thereafter. Reevaluation of the initially administered standard text was performed in patients who had stable biochemical euthyroidism for 12 consecutive months.
All patients provided a signed informed consent form and the study was approved by the institutional review board.
Laboratory tests
Serum TSH (normal range: 0.3–4 mIU/L; sensitivity: 0.005 mIU/L), FT4 (normal: 7–15 pg/mL), and FT3 (normal range: 1.7–3.7 pg/mL) were measured using a commercial immunometric assay (Architect, Abbott Laboratories). Another immunometric assay (DXI800, Beckman Coulter, Inc.) was used to measure serum TRAb concentrations (normal <0.4 IU/L).
Standard text
The standard text that patients were asked to write in cursive script at the time of diagnosis/enrollment and 12 months after the attainment of stable euthyroidism, was: “La categoria degli allenatori di calcio è costituita da coloro che sono veri e propri allenatori, i quali hanno fatto di questo sport una vera professione e dai dilettanti, i quali invece allenano ragazzi per diletto, apprezzando la loro spontaneità e la naturalezza con la quale i bambini giocano al calcio” (English translation: “The category of football coaches is represented by those who are professional coaches and have turned this sport into a profession, and amateur athletes who train boys for passion instead, by appreciating their spontaneity and the naturalness by which children play football”).
Handwriting examination
The texts were analyzed, in random order and without knowledge of thyroid function results, by the handwriting expert C. Botti, Esq., first through inspection for transparency and with a radiant light for the evaluation of depth of the grooves left by the pen on the sheet of paper. Next, a stereoscopic microscope (Euromex Miscroscopes) and a graphed magnifying glass (Peak Light Scale Lupe 7×), with foci magnification ×7, were used to analyze the detail of the letters, in particular, the size of the letters, width of the letters, distance between the letters, distance between the words, extension, and number of angles. The following operational definitions were used (15):
Size of the letters. The measurement in mm of the longitudinal diameter of the letters.
Width of the letters. The relationship between internal width and external height of the letters.
Distance between the letters. The spaces in mm between a letter and another letter of the same word.
Distance between the words. The space in mm between one word and another.
Extension. Part of the letter that surpasses the letter itself.
Angle. The presence of the letters a, d, g, and q, ascending and descending lines that join to form an acute angle.
The extension was assessed in the letters l, t, g, and p and was reported as the average of the measurements in millimeters. The size of the letters and the width were measured in the letters a, d, and o. The distance between the letters was reported as the sum of the spaces between the letters of the words in the first line of the text. The distance between words was calculated as the sum in millimeters of the spaces between the words of the overall text. The angles were reported as the sum of the angles present throughout the whole text.
Statistical analyses
Results are reported as mean±standard deviation. For the comparison between paired data—before and after therapy for GD–the Student's t test for paired data was used. Pearson's correlation coefficient (r) was used when testing for correlation between thyroid function variables and handwriting characteristics. p-Values <0.05 were considered statistically significant.
Results
During the period January 2006 to June 2012, patients with thyrotoxicosis were examined at the Outpatient Thyroid Unit, Department of Internal Medicine, “Ramazzini” Hospital. Of the 386 patients who were examined, 163 (42.2%) had GD, but 130 of these patients had at least one exclusion criterion. Of the remaining 33 patients, 11 were lost to follow-up, leaving 22 patients, 15 (68%) females and 7 (32%) males, with a median age of 44 years (range: 20–70 years), as the study group. The right hand was used for writing by 21/22 (95%) subjects, and the left by 1/22 (5%). Thirteen out of twenty-two (59%) wore glasses. Regarding the level of education, 3/22 had a primary school education, 6/22 had an intermediate school education, 10/22 had a high school education, and 3/22 had university degrees. The mean thyroid function variables were, by design, significantly different between the initial and the follow up investigation 12 months after becoming euthyroid (Table 1).
Results are reported as mean±standard deviation.
FT3, free tri-iodothyronine; FT4, free thyroxine; TRAb, TSH-receptor antibodies; TSH, thyrotropin.
Characteristics of handwriting varied considerably between the hyperthyroid and the euthyroid condition (Table 1) and were perceptible at direct observation (Fig. 1). Changes in handwriting were the sole presentation symptoms of hyperthyroidism in one patient, and the major symptom among many in another patient. Examination of the handwriting categories disclosed statistically significant differences in size of the letters (Fig. 2), distance between the letters and width of the letters (Fig. 3), distance between the words (Fig. 3), extensions of the letters (Fig. 2), as well as angles and groove depth.
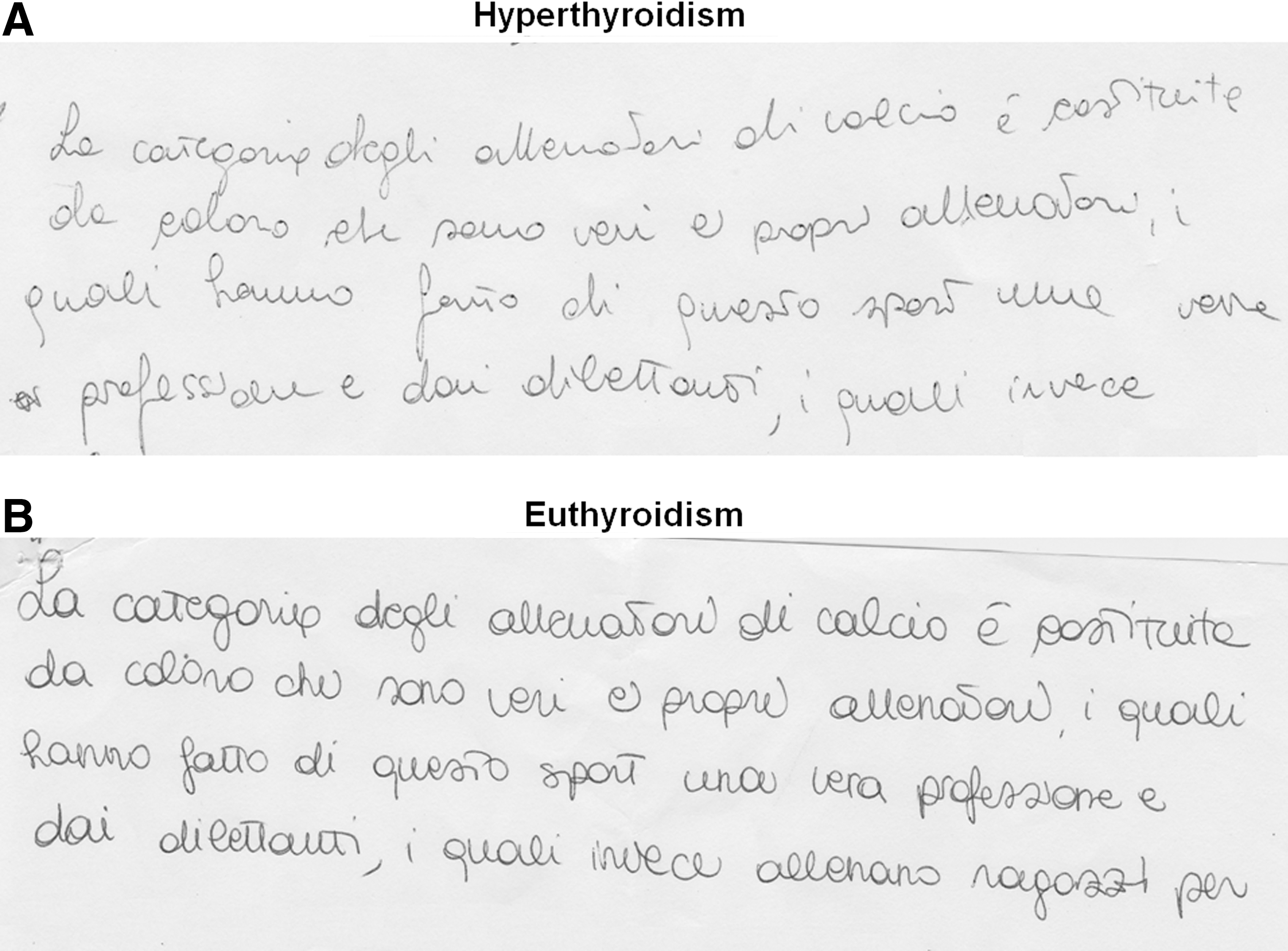
Seventy-year-old female with Graves' disease. Variations in handwriting are perceptible to direct observation.
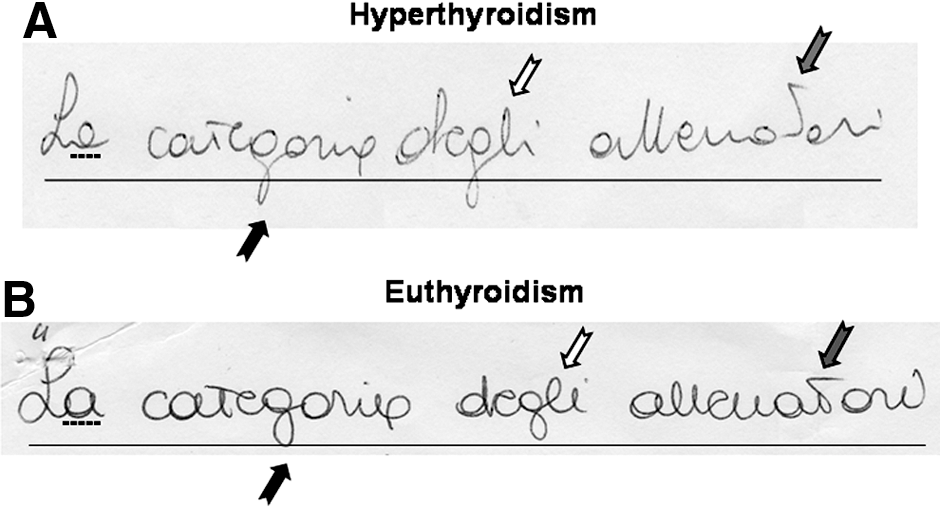
Magnification of Fig. 1. In the euthyroid state

Thirty-six-year-old female with Graves' disease. Following recovery from hyperthyroidism, the distance between the words (black dotted line) and the distance between the letters (gray line) are reduced, whereas the width of the letters (arrow) increased.
With the exception of a positive correlation between the change in serum FT3 levels (before and 12 months after attaining euthyroidism) and “distance between the words” (r=0.45; p=0.036), no significant correlations between any thyroid function variables and handwriting characteristics could be demonstrated. Even this correlation was insignificant when controlling for multiple testing.
Differences in the handwriting variables between the euthyroid and the hyperthyroid state were demonstrated in all patients, and all went in the same direction. For each study variable, individual delta ranges were: groove depth, +0.2 to +0.5 mm; size of letters, +1 to +2 mm; width of letters, 0.0 to +0.5 mm; distance between letters, +3 to +13 mm; distance between words, −32 to −6 mm; number of extensions, −1 to 0; and number of angles, 0 to +3.
Discussion
Using a well-defined phenotype in a paired design, we demonstrated that hyperthyroid GD, in addition to the well-accepted signs and symptoms, is also associated with significant changes in handwriting. To our surprise, changes in handwriting were the only symptom and the main presenting symptom, respectively, in two of our hyperthyroid patients. Therefore, we propose including handwriting variations as signs/symptoms potentially caused by hyperthyroidism.
Although a relationship between hyperthyroidism and handwriting has been previously described (16 –18), all of these reports have crucial shortcomings. They were case reports that failed to specify the type and severity of hyperthyroidism, failed to compare the hyperthyroid with the euthyroid state, and most importantly, did not rule out patients with other potential reasons for affected handwriting. In the present study, perhaps overzealously, exclusion criteria included factors such as smoking, high consumption of coffee, alcohol abuse, and intake of beta blockers.
The reason to focus on GD was to exclude transient hyperthyroidism, such as the thyrotoxicosis from destructive thyroiditis, and toxic nodular goiter, which has a more gradual onset and tends to resolve more slowly, passing through a long phase of suppression of serum TSH (19). It follows that our findings pertain solely to GD and cannot readily be extended to thyrotoxicosis in general.
In a well-accepted, standardized way, we have demonstrated statistically significant changes in nearly all aspects of handwriting characteristics, which were all improved by the antithyroid drug therapy and by achieving a euthyroid state. The changes were of a magnitude allowing perception by direct observation, but the details were assessed by more delicate measures. Thus, the significantly reduced depth of the groove left by the pen on the sheet can be interpreted as the consequence of either the reduction of the tone and muscle strength and/or the hyperhydrosis associated with GD, resulting in a lower pressure force on the sheet of paper.
The large number of extensions and angularity, which is characteristic for the writing of a GD individual, translates into a different handwriting rhythm. It is more “contracted” and nervous, more irregular and disorganized, and—as shown in the standard text—characterized by a longer distance between letters that make up the single words and the space between the words themselves.
Here, we speculate that in addition to myopathy from thyroid hormone excess, the commonly occurring anxiety and tremor both play a role. The tremor of the hyperthyroid patient is typically distal, fine rather than coarse, and caused by the involvement of nerves and muscles (20 –22). Already, Charcot (16), distinguishing the tremor based on the speed of the oscillations, had classified hyperthyroid GD among the diseases causing tremor with rapid oscillations, subsequently characterized as a series of short oscillations with an 8–9 per second frequency (17).
Euthyroidism restores the muscle energy and resolves the fatigue and the tremor. Following recovery from hyperthyroidism, our patients have gone from a state of hypertrophic and contracted writing to a condition of greater fluency with increased fluidity of the layout. Since we did not investigate handwriting at regular time intervals after commencing antithyroid drug therapy, we cannot pinpoint the speed with which these improvements occur. Ideally, we should have demonstrated correlations between severity of hyperthyroidism and handwriting characteristics, which would have favored an interpretation of a causal relationship. The failure to do so is probably due to a combination of the few cases studied, a limited variance in range of thyroid function abnormalities, and the fact that handwriting characteristics is a multifactorial trait.
Our findings might have some legal implications, in particular when the authenticity of a signature (e.g., in a handwritten will) is to be evaluated. Indeed, specific techniques that compare a document with others belonging to the same individual with certainty allow the forensic handwriting expert to determine the true origins with certainty.
We conclude that hyperthyroid GD is associated with significant changes in handwriting. Following recovery from hyperthyroidism, a state of hypertrophic and contracted handwriting is altered toward greater fluency and fluidity. We suggest inclusion of variations in handwriting as signs/symptoms of hyperthyroidism. Investigating a broader range of thyrotoxicosis and myxoedema phenotypes, as well as speed of recovery/normalization of handwriting characteristics in larger patient cohorts, could be a goal for future studies. These should also include observer variation of the handwriting characteristics.
Footnotes
Acknowledgments
We dedicate this paper to the late professor Clark T. Sawin, who for years devoted much time to maintain and strengthen the ties with the history of the thyroid gland and its function. We acknowledge Nicholas John Villamaino and Graziana Esposito who revised the text for language accuracy. L.H. is the recipient of an unrestricted research grant from the Novo Nordisk Foundation.
Author Disclosure Statement
The authors have no conflicts of interest and have not received specific funding for this work.