
Abstract
Background:
The clinical use of serum thyroglobulin (Tg) as a tumor marker in papillary thyroid cancer (PTC) patients following total thyroidectomy continues to evolve, due in part to the introduction of more sensitive (second generation) Tg immunometric assays (Tg2GIMA, functional sensitivity ≤0.10 ng/mL), and the implementation of new recommendations against radioactive iodine ablation (RAIA) for patients at the lowest risk of recurrence. As a result, there is a need to establish the optimal timing and interpretation of serum Tg values while on levothyroxine-induced suppression of thyrotropin (TSH) in thyroidectomized PTC patients with a thyroid remnant. This study examines the pattern of decline and eventual baseline value of unstimulated Tg (uTg) concentrations following total thyroidectomy in patients with low-risk PTC who did not receive RAIA.
Methods:
The medical records of consecutive patients with thyroid cancer seen at the Los Angeles County+USC Medical Center were retrospectively reviewed. Serial uTg and TSH values from Tg-antibody negative low-risk PTC patients treated with total thyroidectomy and no RAIA were analyzed. Patients were stratified by degree of TSH suppression to assess the effect on uTg. Serial postoperative uTg values were evaluated for the temporal pattern of decline and ultimate baseline. Patients with medullary thyroid cancer (MTC) were studied as a surgical reference group.
Results:
Records from 577 consecutive thyroid cancer patients were reviewed, of which 36 met all criteria for inclusion. By 6 months, uTg fell to <0.5 ng/mL in 61% of patients and all patients demonstrated uTg <0.5 ng/mL 2 years after surgery. During a median follow up of 5.7 years, uTg values remained below this level. The median uTg values in patients with papillary microcarcinoma, PTC, and MTC were similar at 0.11, 0.12, and 0.09 ng/mL, respectively. Further decline in uTg was not observed once the TSH was <0.5 mIU/L.
Conclusions:
The uTg values during TSH suppression in Tg antibody–negative, low-risk PTC patients who did not receive RAIA were below 0.5 ng/mL by 6 months postoperatively in most cases and remained stable over the duration of patient follow-up.
Introduction
T
Serum thyroglobulin (Tg) measurement, along with neck ultrasonography (US), is the mainstay of long-term surveillance in PTC patients after total thyroidectomy (TTx), with undetectable Tg, specifically after recombinant human thyrotropin (rhTSH) stimulation, deemed consistent with disease-free status (6). Tg is made by the thyroid follicular cells, and its serum concentration reflects thyroid tissue mass (benign or malignant), the degree of thyrotropin (TSH) receptor stimulation, the capacity of that tissue to produce and release Tg, and any surgical manipulation or trauma to the thyroid gland (12). Over the last decade, more sensitive (second generation) immunometric assays (Tg2GIMA) have become available with a functional sensitivity limit ≤0.10 ng/mL (13 –15), allowing the detection of low unstimulated Tg (uTg) values that may be present in thyroidectomized patients without the use of exogenous (rhTSH) or levothyroxine (LT4) withdrawal (14).
It has been shown that in low-risk PTC patients with incidentally discovered papillary microcarcinomas (mPTC), defined as tumors <1 cm, most will have uTg values below the limit of detection, even without RAIA (16). However, patients with otherwise low-risk PTC who do not receive RAIA may also have detectable postoperative Tg levels when measured by more sensitive Tg2GIMA assays (16 –18). In addition, the expected uTg values measured by these assays in patients with a preserved thyroid remnant is still uncertain. Therefore, the purpose of the present study is to evaluate the post-thyroidectomy pattern of decline and absolute values of uTg in low-risk PTC patients compared to low-risk mPTC patients, without the use of RAIA therapy.
Patients and Methods
The medical records of consecutive patients with thyroid cancer who underwent TTx at the Los Angeles County+University of Southern California Medical Center (LAC+USC) between 2000 and 2010 were retrospectively reviewed. Patients with PTC or follicular variant of PTC, but not other variants (e.g., tall cell, insular, or Hürthle cell), were selected as having a low-risk for recurrence as defined by the American Thyroid Association (ATA) guidelines if the surgical pathology showed: a) a tumor size less than 4 cm in largest dimension; b) an intrathyroidal tumor without evidence of extension or lymphovascular invasion; and c) no lymph node involvement either by surgical or histologic assessment; plus, there was no clinical evidence of distant metastases at the time of surgery (6). All surgeries were performed by the same group of experienced thyroid surgeons (19).
To ensure the ability to evaluate uTg under recommended levels of TSH suppression for low-risk PTC (6), patients were excluded if a TSH below 0.5 mIU/L was not achieved within 2 years of surgery. Patients were additionally excluded if Tg antibody (TgAb) was present at the initial Tg assessment to avoid TgAb interference causing falsely low/undetectable Tg2GIMA values (20 –22) and because higher recurrence risks are reported for TgAb-positive patients (23,24). The postoperative management of patients consisted of serial uTg measurements while under LT4-induced TSH suppression every 6–12 months and was handled in one clinic by the same treating physician (J.S.L.). The use of rhTSH stimulation prior to Tg measurement was not routinely employed.
Patients with medullary thyroid cancer (MTC) who were retrospectively found to have undergone a simultaneously measured TSH and Tg within the LAC+USC system at any point postoperatively were also selected. MTC is a neuroendocrine-derived thyroid cancer constituting 5% of all thyroid cancers and does not produce Tg (25). Surgeries in these patients were completed by the same surgical team and consisted of an aggressive TTx with lateral neck dissections bilaterally in all cases. Postoperative thyroid hormone replacement was designed to keep TSH values at the low-normal part of the reference range. Because MTC patients receive a similar surgery to PTC patients, do not receive RAIA, and do not have Tg producing tumors, postoperative MTC patients provide an ideal control group to study the contribution of the postoperative thyroid remnant to uTg concentrations.
Patient samples were stored at −20°C until the time of measurement, based on previous data demonstrating the long-term stability of Tg (26). All samples were analyzed in the same laboratory (USC Endocrine Laboratory) by the same assay. Tg measurements were performed using the Access immunochemiluminescent method (Beckman Coulter, Fullerton, CA), which was directly standardized against the certified reference material (CRM-457). Functional sensitivity established according to current guidelines was 0.1 ng/mL. Between-run precisions assessed in TgAb-negative human serum pools measured over a 14-month period were 13.0%, 6.5%, 4.2%, and 4.0% for serum Tg concentrations of 0.13, 0.59, 7.0 and 54 ng/mL (μg/L), respectively. Each serum was screened for the presence of TgAb using the Kronus radioassay method (Boise, ID). Tests having serum TgAb ≥0.4 kU/L were considered positive. Between-run precisions assessed in human serum pools measured over a 1-year period were 14.3%, 9.5%, 8.7%, and 11.1% for TgAb concentrations of 0.7, 2.6, 5.2, and 11.0 kIU/L, respectively. Serum TSH was measured using either the Immulite 2000 (Siemens, Erlangan, Germany) or Roche Cobas (Roche Diagnostics, Indianapolis, IN), third-generation assays (functional sensitivity=0.01 mIU/L).
Continuous data is reported as mean±standard deviation (SD) or median with range, and compared using a Student's t-test, Mann-Whitney U-test, one-way ANOVA, or Kruskal-Wallis test, as appropriate. Categorical data was analyzed using the Fisher's exact test. Correlations were performed using Pearson's linear correlation. All tests were two-tailed and a p value of <0.05 was considered statistically significant. Analyses were performed using GraphPad Prism version 6.0b for Mac OS X (GraphPad Software, La Jolla, CA).
This study was approved by the Institutional Review Board of the University of Southern California.
Results
Baseline patient characteristics
There were 577 consecutive PTC patients from 2000 to 2010 whose cases were reviewed, of which 250 met the presurgical inclusion criteria. One hundred six patients (42.4%) had tumors of less than 4 cm, along with no evidence of invasion, extension, or lymph node metastases. Of these 44 (41.5%) were TgAb positive, and a further 28 patients were excluded for lack of TSH suppression or follow-up of less than 2 years, leaving a total of 36 subjects whose characteristics are summarized in Table 1. Thirty-three of 36 patients (92%) were women. The median age was 50.5 years (22–76 years), and 23/36 (63.8%) were older than 45 years of age. Tumors smaller than 1 cm were present in 17/36 (47.2%) of subjects. The median duration of follow-up was 5.7 years (range 2.2–12.1 years). Follow-up in patients with mPTC was shorter than for those with PTC, with a median follow up of 4.75 versus 6.5 years, respectively (p=0.03). None of the 36 PTC patients received RAIA as part of initial therapy or during follow-up. Nine patients with MTC who had a serum Tg measured postoperatively were identified, and their clinical characteristics are summarized in Table 1.
Fisher exact test.
Analysis of variance (ANOVA).
Student's t-test.
Comparison between PTC and MTC groups.
PTC, papillary thyroid cancer; MTC, medullary thyroid cancer; TTx, total thyroidectomy; PCND, prophylactic central neck dissection; BMRND, bilateral modified radical neck dissection; TNM, tumor-node-metastasis; FV, follicular variant.
Threshold TSH suppression level for lowering uTg
There were 425 patient specimens of concurrent TSH and uTg measurement obtained during patient follow-up, with a mean of 12±6 measurements performed per patient, and a median TSH of 0.03 mIU/L (range <0.01 to 85.1 mIU/L). When analyzed as TSH subgroups of <0.1, 0.1–0.49, 0.5–3.5 (reference range), and >3.5 mIU/L, these specimens had median uTg values of 0.12 (<0.1–2), 0.11 (<0.1–3.8), 0.15 (<0.1–6.2), 1.20 (<0.1–18.1) ng/mL, respectively. The median uTg for patients with a TSH <0.1 mIU/L was similar to those with TSH 0.1–0.49 mIU/L but was lower in the TSH 0.1–0.49 mIU/L group compared to the TSH 0.5–3.5 mIU/L group (p<0.05) (Fig. 1A). TSH and uTg showed no correlation when the TSH values were less than 0.5 mIU/L (p=0.67), but demonstrated a positive correlation if the TSH concentration was at or above 0.5 mIU/L (r 2=0.27, p<0.001) (Fig. 1B). Because TSH appeared to least affect Tg values once TSH was <0.5 mIU/L, only Tg values obtained under this degree of suppression were utilized for evaluation of postoperative trends.

Relationship between unstimulated Tg (uTg) and thyrotropin (TSH) values in 36 patients with low-risk papillary thyroid carcinoma.
Postoperative uTg trends under TSH suppression
Within 2 years postoperatively, patients received a mean of 4.35±1.7 uTg assessments. In all patients, uTg fell to<0.5 ng/mL by the second year postoperatively as shown in Figure 2A. The mean time to achieve uTg <0.5 ng/mL was 6.45±4.85 months. By 3, 6, and 12 months postoperatively, uTg reached<0.5 ng/mL in 13/36 (36%), 22/36 (61%), and 34/36 (94%), respectively. In the first 2 years after thyroidectomy, only four patients had uTg values >0.5 ng/mL (Fig. 2B). In two cases, uTg values >0.5 ng/mL represented a transient elevation, while in the remaining two cases, uTg values >0.5 ng/mL were part of a gradual decline to <0.5 ng/mL by 19 and 20 months, respectively. Beyond 2 years, only three patients had an uTg value >0.5 ng/mL and all were isolated and returned to baseline without intervention. The overall median uTg was 0.11 ng/mL (range <0.1 to 3.8 ng/mL), and this median value did not differ for uTg values measured during 0–6, 6–12, and 12–24 months postoperatively, or at last patient follow-up. The duration required to reach a uTg value <0.5 ng/mL was similar between PTC and mPTC tumors (p=0.2). No patient had a TgAb-positive measurement during follow-up.
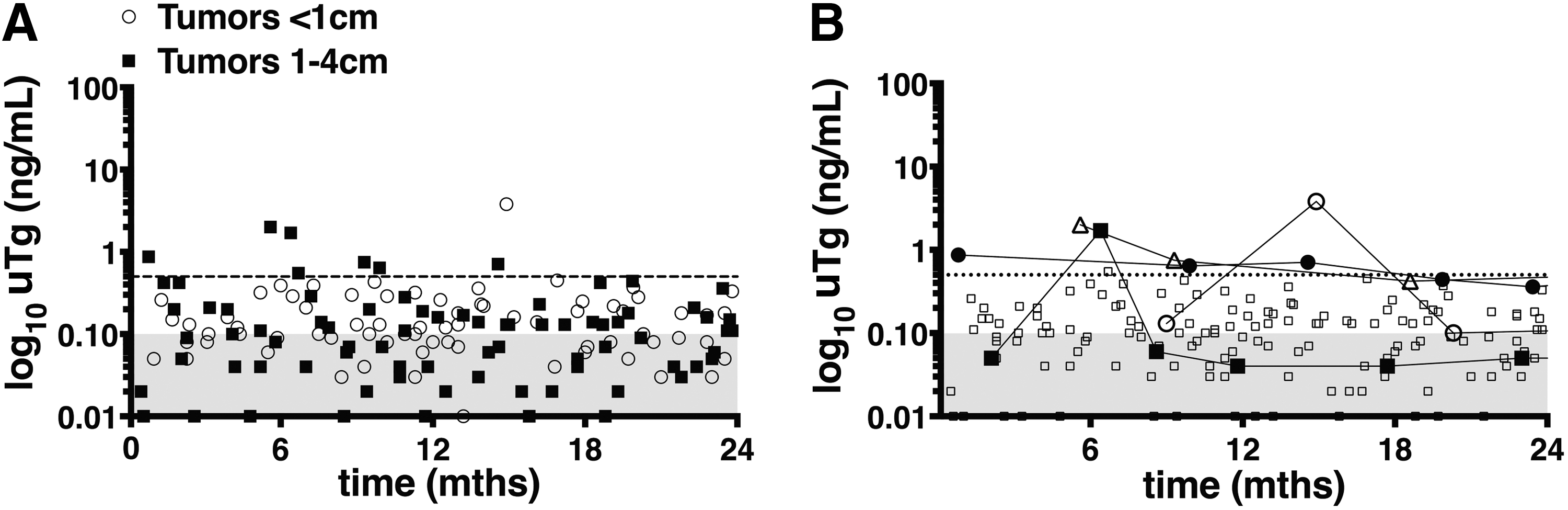
Unstimulated Tg values during the first 2 years for 36 Tg antibody–negative patients with low-risk PTC after total thyroidectomy.
Clinical characteristics and uTg concentrations under TSH suppression
Associations between uTg and clinical features are shown in Figure 3. The median uTg was 0.14 and 0.12 ng/mL for PTC patients ≥45 compared to <45 years of age, respectively (p<0.01). Patients who underwent prophylactic central neck dissection (PCND) compared to TTx alone had a median uTg of 0.18 versus 0.11 ng/mL, respectively (p<0.0001).
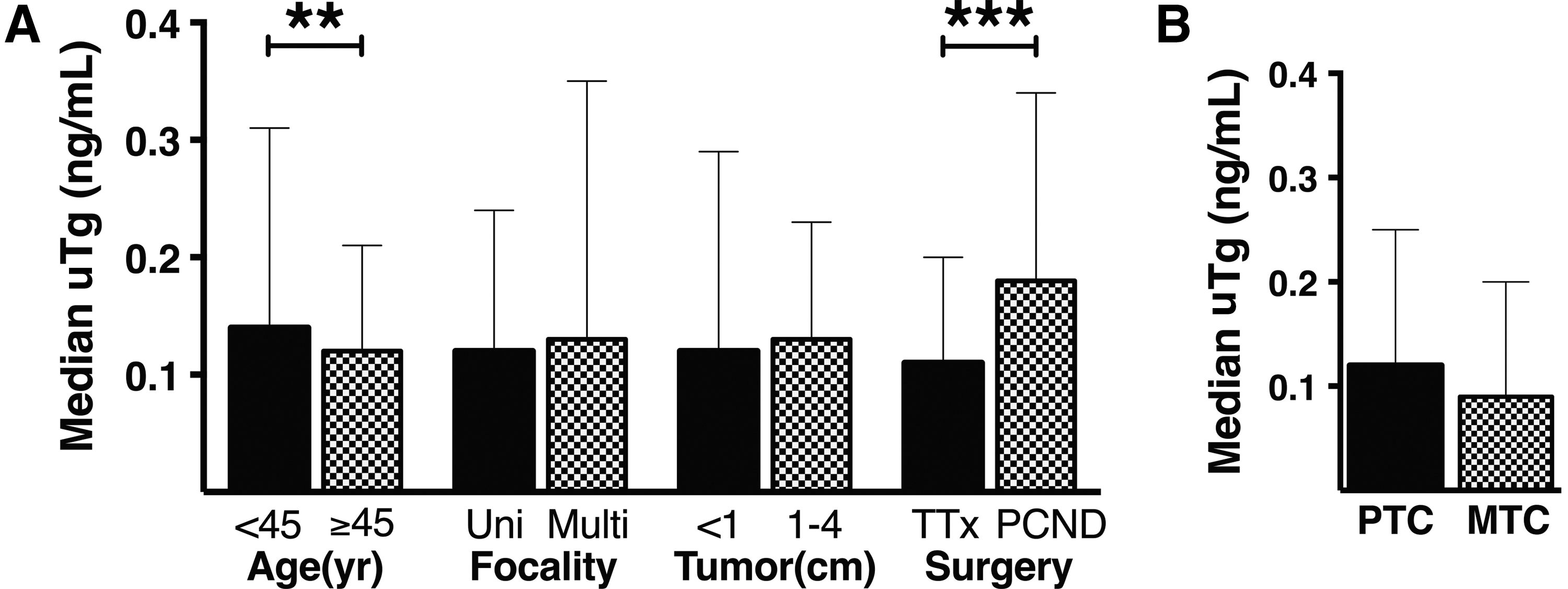
Comparisons of median uTg by clinical features of PTC patients and histologic subtype. Median uTg with interquartile range is shown.
The median uTg values in patients with low-risk mPTC compared to tumors of 1–4 cm were 0.11 and 0.13 ng/mL, respectively (p=ns). There was also no significant difference between the median uTg concentrations in patients with unifocal versus multifocal PTC.
In the nine cases of MTC, there were 14 simultaneous TSH and Tg values, occurring anywhere from 6 months to 7 years after TTx. The median TSH value for these measurements was 0.72 mIU/L, with a range of <0.01 to 4.23 mIU/L. The median uTg value in these patients was 0.09 ng/mL (range <0.1–0.47 ng/mL), which was not statistically different from PTC patients (Fig. 3).
Discussion
The incidence of papillary thyroid carcinoma, particularly that of small tumors (<2 cm), has increased dramatically over the last three decades (1 –5), and many of these patients will have a low risk of recurrence. Current guidelines recommend withholding RAIA in those at the lowest risk of recurrence (6,11), resulting in a growing number of patients treated without RAIA of the normal thyroid remnant. Preservation of the thyroid remnant has raised the question of how Tg, either as rhTSH-stimulated or unstimulated values, can be utilized in long-term surveillance of these patients. Given the strong correlation (∼10-fold) between uTg and stimulated Tg (13), and evidence that unstimulated values alone can predict prognosis (14), a clear description of the significance of uTg concentrations is essential.
In the present retrospective study, serial Tg measurements were analyzed in patients with PTC defined as low risk for recurrence, who were additionally TgAb negative and did not receive RAIA. During this period, rhTSH stimulation was not routinely employed, so Tg measurements were all unstimulated. This allowed for the evaluation of uTg in TSH-suppressed PTC patients with a preserved thyroid remnant and the assessment of the effect of TSH suppression on these values over a long period of follow-up.
TSH suppression below 0.5 mIU/L was not associated with further reduction in uTg values in the patients studied. Although the demonstration by Burmeister et al. (27) that TSH reductions below 0.4 mIU/L did not further decrease uTg is in agreement with the data here, this was not seen in more recent studies (16,28). This discrepancy may have resulted from differences in the sensitivities of the Tg or TgAb assays used in the various studies. Additionally, the TSH cut-off levels used differed between studies. Our data demonstrate that TSH suppression below 0.5 mIU/L was not associated with further reductions in uTg concentrations in low-risk PTC patients and is consistent with the ATA guidelines recommending an initial TSH suppression level of 0.1–0.5 mIU/L for low-risk patients (6).
Under this degree of TSH suppression, postoperative uTg fell to <0.5 ng/mL in 60% of patients by 6 months, 94% by 12 months, and in all patients by 2 years. The extended time over which uTg values decline is likely related to Tg release from traumatized and/or ischemic thyroid tissue after surgery. These data are in agreement with Padovani et al. (29) who described a slow postoperative decline in Tg concentrations that continued for 2 years in some patients. In the 2 years after surgery, only 2 out of 36 patients had a uTg value that acutely rose to >0.5 ng/mL. In both cases, uTg returned to <0.5 ng/mL at the next measurement without intervention. Whether these anomalous values resulted from laboratory error, unmeasured periods of TSH elevation, or another cause is uncertain. Regardless, these data suggest that uTg values <0.5 ng/mL may provide a baseline by which to monitor low-risk PTC patients who do not receive RAIA after thyroidectomy.
Previous studies of uTg in differentiated thyroid cancer patients after RAIA have demonstrated low Tg levels similar to those presented here (15,30,31). In a study by Durante et al. (16) of 78 low-risk papillary thyroid microcarcinoma patients (mean tumor size of 4 mm) who did not receive RAIA, uTg values fell to undetectable levels (<0.2 ng/mL) in 60% of subjects by 12 months post-thyroidectomy. In the current study, the fall in uTg after thyroidectomy was similar in low-risk patients with papillary microcarcinomas (<1 cm) compared to those with tumors 1–4 cm in size (Fig. 2). These results confirm those of Durante et al. (16) and extend the findings to low-risk PTC patients with tumors of <4 cm (mean tumor size 2.58±1.12 cm). Additionally, these low uTg values remained unchanged during a median follow up of 5.7 years.
The median uTg levels in MTC patients after surgery were not significantly different from the low-risk PTC patients evaluated in this study. These findings are similar to results from Tomoda and Miyauchi (32), who demonstrated that Tg values measured in 27 MTC patients after initial surgery and without RAIA therapy were <0.5 ng/mL, which was the detection limit for the assay used. The similar uTg values in low-risk PTC and MTC patients suggest that an uTg concentration of 0.5 ng/mL likely reflects residual normal thyroid remnant.
The higher median uTg in patients aged ≥45 compared to<45 years of 0.14 versus 0.12 ng/mL, respectively (p<0.01) was unexpected, though this difference is likely of little clinical significance. One explanation for this finding may be that older patients had a higher rate of occult autoimmune thyroid disease, which has been associated with higher Tg values in reference populations. However, thyroid peroxidase antibody assessments to support this hypothesis were not available in this study. There was also a higher median uTg in those who had received TTx with a PCND versus those who had TTx alone, 0.18 versus 0.11 ng/mL, respectively (p<0.0001). Some unrecognized clinical feature in our retrospective chart review may have influenced the decision to perform a PCND and thus confounds the observed association between PCND and uTg values.
There are several limitations in the current study. In order to carefully describe uTg values, only a specific group of low-risk PTC patients were included, which resulted in a small sample size with narrow clinical applicability. The completeness of thyroidectomy, as performed by experienced thyroid surgeons, likely resulted in small and consistent thyroid remnant size and may not be reproducible in all settings. Finally, because only 22/36 (61%) had an available imaging study during follow-up (e.g., neck ultrasound), we are unable to definitively exclude the presence of structural disease; however, in those subjects with US assessment, no evidence of soft tissue or lymph node recurrence was found. Finally, the retrospective design of this study introduces a greater potential for biases or confounding.
These data show that when TSH is <0.5 mIU/L, postoperative uTg values in low-risk PTC patients who did not receive RAIA, while detectable by current Tg2GIMA testing, fall to<0.5 ng/mL and remain stable over time. However at TSH values above 0.5 mIU/L, Tg was positively associated with TSH, suggesting stimulation of thyroid tissue by TSH. These elevated Tg values (>0.5 ng/mL) in low-risk PTC patients may represent the response of TSH-sensitive remnant tissue to transient or sustained serum TSH levels above 0.5 mIU/L and may not necessarily represent recurrence. Whether a similar pattern of uTg decline and stability is observed in PTC patients at intermediate or high risk for recurrence who did not receive RAIA therapy, and whether temporal trends such as Tg doubling time (33,34) identify more aggressive PTC, are the subjects of ongoing evaluations at our institution. Thus far, one report in the literature suggests that in intermediate-risk PTC patients, a low uTg does not preclude the possibility of distant metastasis by SPECT/CT evaluation (35).
In conclusion, in low-risk PTC patients who did not receive radioactive iodine therapy, serially measured uTg values fell to <0.5 ng/mL by the second postoperative year when TSH was suppressed below 0.5 mIU/L. The median value of 0.11 ng/mL in PTC was similar to that seen in MTC patients. Additionally studies are needed to determine if failure of uTg to fall to these levels in low-risk PTC patients is predictive of recurrence.
Footnotes
Acknowledgments
The authors thank Drs. Erin Atkinson (Ronald Reagan University of California, Los Angeles Medical Center, Los Angeles, CA) and Jennifer Chang (Huntington Memorial Hospital, Pasadena, CA) for their assistance in the review of medical records. The authors thank the USC Endocrinology Lab for performing thyroglobulin analysis of archival patient samples.
Author Disclosure Statement
The authors have no conflicts of interest to declare.