
Abstract
Background:
Most current guidelines suggest one or two weeks of low iodine diet (LID) before radioactive iodine ablation therapy (RAIT) to increase its efficacy in differentiated thyroid cancer (DTC) patients after total thyroidectomy. LID duration is particularly important for patients living in iodine excess areas. However, there is no standardized LID protocol and there are limited reports regarding the relationship between LID and ablation outcome. Therefore, we aimed to evaluate the optimal LID duration and define clinical features that affect ablation outcome.
Methods:
A total of 202 papillary thyroid cancer patients with total thyroidectomy preparing for RAIT were enrolled. All patients had undergone two weeks of LID before 131I administration. Morning spot urine specimens were obtained twice (one week or two weeks after LID, respectively) from each patient. Urine iodine excretion (UIE) values were used to evaluate LID efficacy. Successful ablation was defined using two definitions: (i) no visible uptake on a follow-up diagnostic 131I scans, and (ii) no visible uptake on a follow-up diagnostic 131I scans and stimulated serum thyroglobulin (Tg) levels <1 ng/mL.
Results:
The UIE median values after LID for one and two weeks were lower than 50 μg/L, and the median UIE values were not significantly different according to the LID duration. Based on the first criterion for successful ablation, 175 of the 195 patients were successfully ablated. There were no significant differences in mean and median UIE levels between the ablated and non-ablated groups after LID for two weeks. The rate of ablation did not differ between the mild and moderate iodine deficient groups. Based on the second criterion for successful ablation, 149 of 188 patients were successfully ablated. The ablation success rate did not differ between UIE levels. When we analyzed clinical factors that affect ablation outcome, serum Tg level at the time of ablation was the only significant variable in multivariate logistic analysis.
Conclusion:
Strict LID for one week was sufficient to achieve target UIE values for RAIT preparation, even in iodine-rich areas.
Introduction
R
Delivery of optimal radiation doses to the thyroid remnant or tumor is an important factor for successful radioactive iodine therapy (RAIT) (2,3). There are two main approaches to increase ablation efficacy. The first approach is increasing serum thyroid stimulating hormone (TSH) concentrations (4), whereas the second is depletion of the whole-body iodine pool (3). The former is achieved by thyroid hormone withdrawal or recombinant human TSH (rhTSH) injection (1). Withdrawal of thyroid hormone prior to RAIT is the more traditional and typical method, but it causes patients to suffer from hypothyroidism symptoms (5). The latter is obtained by restriction of daily iodine intake thorough a low iodine diet (LID) before RAIT (6,7). Most guidelines recommend limiting dietary iodine intake to 50 μg daily for one to two weeks, but there are still no standardized LID protocols (8 –10). Evaluation of the body iodine pool using urine analysis is recommended before RAIT because urine iodine excretion reflects very recent dietary iodine intake well (11,12). Previous reports have demonstrated that morning spot urine analysis can be an alternative method to 24-hour urine sampling for assessment of iodine nutrition status (13 –15). The European Association of Nuclear Medicine (EANM) Therapy Committee in 2008 proposed to defer RAIT in patients with DTC when the random urinary iodine concentration is above 150–200 μg/L (16).
The stringency and duration of LID for achieving adequate iodine depletion before RAIT may vary due to geographic differences in dietary iodine intake (17 –19). For example, Korea is bound by the sea on three sides, and the dietary iodine intake level from seafood is higher compared with all other countries except Canada and Japan (18 –20). A strict LID for two weeks is often recommended in Korean clinics due to the common belief that a longer LID period is necessary to achieve sufficient iodine depletion in this iodine excess area. However, the optimal LID duration is still debatable and a two-week LID may be too long for the patient to tolerate, decreasing their quality of life quality compared to other countries. The disadvantage is due to the Korean patients' greater reliance on an iodine-heavy diet. While the period of LID may be the same, a Korean patient has to make a greater change to restrict his or her diet. For instance, salted, fermented food prepared with iodized salt—including kimchi, red pepper paste, pickled seaweed or fish, and soybean paste—are essential to Korean cuisine. Many Koreans just cannot have a meal without it and these foods are hard to avoid. However, the low-iodine guidelines prohibit intake. The maintenance of LID, therefore, can be a more difficult task for Koreans than patients in other countries. In our experience, a LID could be a source of anxiety because the patients feel that the variety of foods that could be eaten safely is low. It can cause significant dietary disruption and restriction of patients' social life. Based on these considerations, we aimed to evaluate the optimal duration of LID required to reach an adequate body iodine pool level before RAIT administration for patients in iodine rich areas. We also examined the relationship between body iodine pool levels and ablation efficacy using spot urine analyses.
Materials and Methods
Patients
Patients (n=202) preparing for RAIT after total thyroidectomy due to papillary thyroid cancer were enrolled between April 2012 and July 2013 at the Thyroid Cancer Center at Gangnam Severance Hospital. They were referred for the purpose of thyroid remnant or metastasis ablation after surgery and no grossly visible thyroid remnants remained in any cases. Applied 131I doses were determined depending on the initial cancer extension (range, 3.70–7.40 GBq) using the tumor, lymph node, metastasis classification system of the American Joint Committee on Cancer classification. For postoperative ablation of thyroid bed remnants, 3.7 GBq of 131I was administered. Activities in the range of 4.81–5.55 GBq were typically administered for treatment of presumed thyroid cancer with central neck node metastasis. In cases of thyroid cancer with lateral neck or mediastinal node metastasis, activities in the range of 6.66–7.40 GBq were given. Patients who did not wish to participate in the study were excluded. Additionally, patients with a history of chronic renal disease or patients who could not follow instructions due to his/her psychiatric disability were also excluded. Post-therapy 131I-whole body scintigraphy (WBS) was performed 9 to 10 months after ablation using a dual-head gamma camera (Symbia E; Siemens Medical Solutions, Malvern, PA) equipped with parallel-hole, medium energy collimators and 364 keV energy peak with a 15% window and an acquisition time of 20 min/projection. Anterior and posterior projection images were obtained. According to the ablation and follow-up protocols, all patients were withdrawn from levothyroxine four weeks prior to RAIT and WBS, which was replaced with liothyronine for two weeks followed by withdrawal of T3 for 2 weeks (thyroid hormone withdrawal, THW). Patients completed a specific LID for two weeks before 131I administration. Prior to starting LID, they were educated by specially trained nurses who provided information about drugs and foods that are allowed or not during the LID period. The patients were also given a dietary guide (Table 1) and sample LID menus to take home. The Gangnam Severance Hospital Review Board approved the study design, and written informed consent was obtained from all patients.
Laboratory data analyses
Morning spot urine specimens were obtained twice from each patient and the urine iodine excretion (UIE) was obtained to evaluate LID efficacy. The first urine sample was taken one week after starting LID and the second one was taken two weeks after the LID protocol. Urine iodine was measured using inductively coupled plasma mass spectrometry and an Agilent 7500 series instrument (Agilent Technologies, Inc., Tokyo, Japan). The reference range was 23.9–4322.8 μg/L.
Urine iodine depletion was categorized based upon previous reports and World Health Organization (WHO) criteria for assessing iodine nutrition status: median urinary iodine concentrations of ≥100 μg/L define a population that has no iodine deficiency. UIE concentrations <50 μg/L were considered moderately iodine deficient, whereas levels ≥50 μl/L but <100 μg/L correspond to mild iodine deficiency (15). These two criteria are regarded as adequate LID preparation for RAIT administration. The cutoff value of UIE, which indicates poor LID preparation, was ≥100 μl/L. Seven patients with poor compliance (the patients did not follow the LID recommendations) were excluded from the analyses. Poor compliance was defined as (i) UIE levels greater than the mean UIE values of normal Korean patients (478.6 μg/day) (20) in both the first and second week LID, and (ii) patients who achieved adequate UIE levels during the first week LID but showed high UIE levels (≥50 μl/L) during the second week LID.
Blood samples for serum TSH, stimulated thyroglobulin (Tg), and thyroglobulin antibodies (TgAbs) were obtained on the day of RAIT administration. Serum TSH levels were analyzed using an immunoradiometric assay (TSH-CTK-3, SORIN Biomedica, Saluggia, Italy), and the reference range is 0.86–4.69 mU/L. 131I was administered when TSH levels were >30 mU/L in all patients. Serum Tg was measured using the Modular E170 (Roche Diagnostics, Mannheim, Germany) with an analytic sensitivity of 0.1 ng/mL. Serum TgAbs were detected using an immunoradiometric assay (Tg plus RIA; Brahms AG, Hennigsdorf, Germany) and values below 124.2 U/mL were considered negative.
Ablation success criteria
To evaluate the RAIT success rate, we used two criteria for successful thyroid ablation. The first criterion was no visible neck uptake in the diagnostic WBS. The second criterion was no significant neck uptake on a diagnostic WBS plus undetectable serum Tg levels (<1 ng/mL) after TSH stimulation in the absence of circulating TgAbs. Radioiodine WBS was visually interpreted by two experienced nuclear physicians to obtain consensus readings. The results are classified as positive or negative according to whether there was uptake in the neck.
Statistical analyses
Statistical analyses were performed using SPSS 18.0 statistical software for Windows (SPSS Inc., Chicago, IL). Numeric data are expressed as the mean±standard deviation. Wilcoxon signed-rank tests, Mann-Whitney U tests, McNemar's tests, and chi-square tests were used to assess statistical differences between groups. Multivariate logistic regression analysis was used to find the association between variables with ablation success. A p-value <0.05 was considered statistically significant.
Results
Patient characteristics
A total of 195 papillary thyroid cancer patients (149 females, 46 males) were enrolled. Their mean age was 44±11.08 years (range 22–73 years). Among the enrolled patients, 74.9% had lymph node metastasis at the initial presentation, and TSH levels were greater than 30 mU/L in all patients. The mean sTg level was 7.63±18.66 ng/mL (median 2.7 ng/mL, range 1–179.2 ng/mL) in patients with negative TgAbs at the time of 131I administration. The patient characteristics are summarized in Table 2.
Data are presented as the numerical value or the mean±standard deviation (SD).
RAIT, radioactive iodine ablation therapy; Tg, thyroglobulin; TgAb, thyroglobulin antibody; TNM, tumor, lymph node, metastasis classification system; TSH, thyroid stimulating hormone.
LID efficacy
The median values of UIE after 1-week LID and 2-week LID were 12.80 μg/L and 13.40 μg/L (Table 3). The median UIE values were not significantly different (p=0.03, Wilcoxon signed-rank test) according to LID duration. UIE levels lower than 50 μg/L were noted in 170 out of 195 patients (87.2%) after LID for 1 week and in 180 of 195 patients (92.3%) after LID for 2 weeks. Mild iodine deficiency was noted in 17 of 195 patients (8.7%) after LID for 1 week and in 15 of 195 patients (7.7%) after LID for 2 weeks. The frequencies of mild and moderate iodine deficiency did not differ between 1-week and 2-week LID (p=0.06 and p=0.84, McNemar's test). There were 8 patients (4.1%) with UIE levels over 100 μg/L after LID for 1 week. The highest UIE value in these patients was 148.5 μg/L. There were no inadequately prepared patients after LID for 2 weeks.
Data are presented as the numerical value or the mean±SD.
LID, low iodine diet.
Ablation outcomes based on the first criterion and clinical features associated with successful ablation
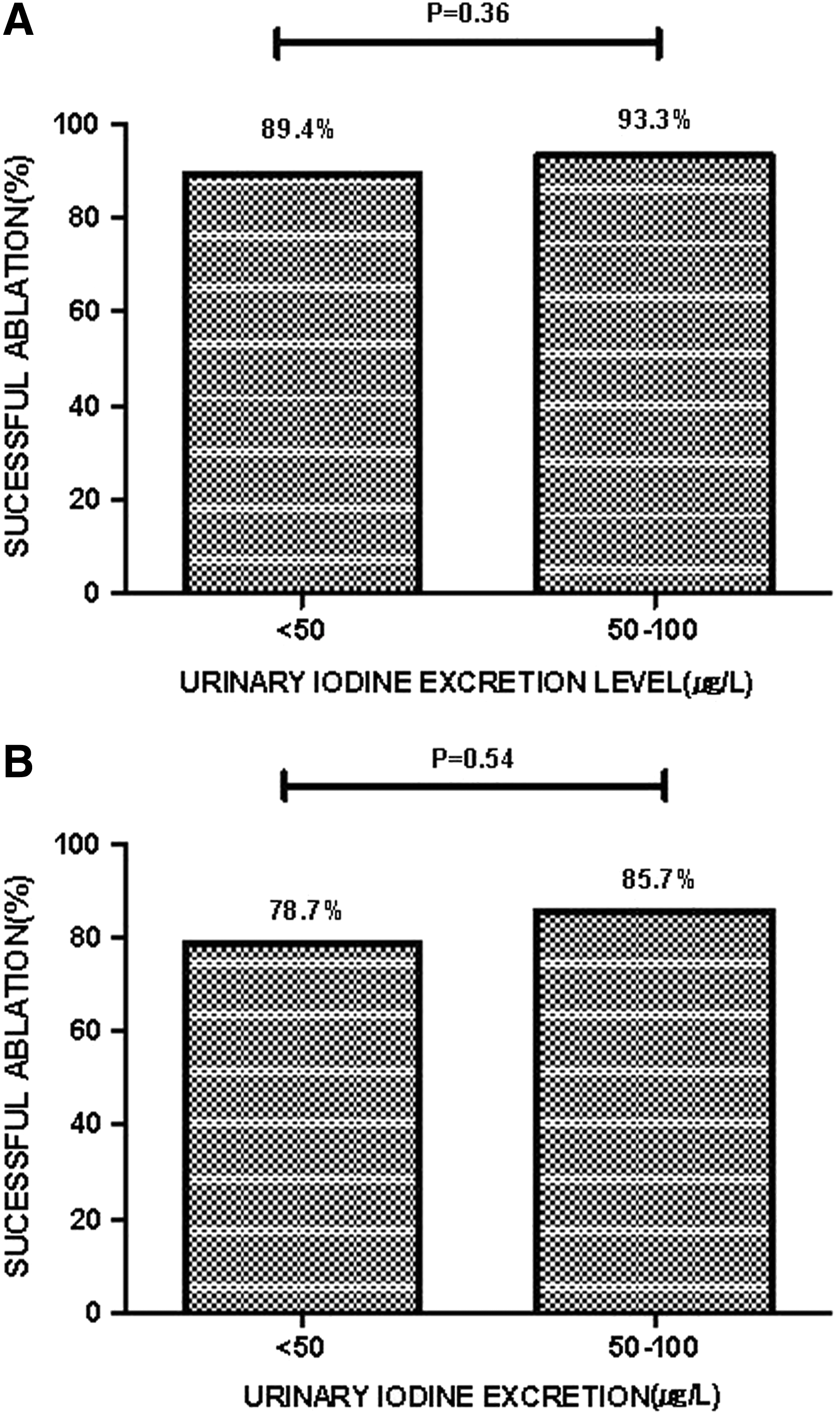
There were 175 patients (89.74%) patients classified as successfully ablated based on the first criterion. There were no significant differences in the mean and median UIE values between the ablated and non-ablated groups after LID for 2 weeks (p=0.40, Mann-Whitney test) (Fig. 1). Additionally, we analyzed other possible variables that affect ablation outcome, including age, sex, ablation dose, lymph node metastasis, and TSH levels. However, we could not find any significant clinical factors (Mann-Whitney and chi-square tests). The rate of successful ablation did not differ between the mild and moderately iodine deficient groups (p=0.36, chi-square test) (Fig. 2A).
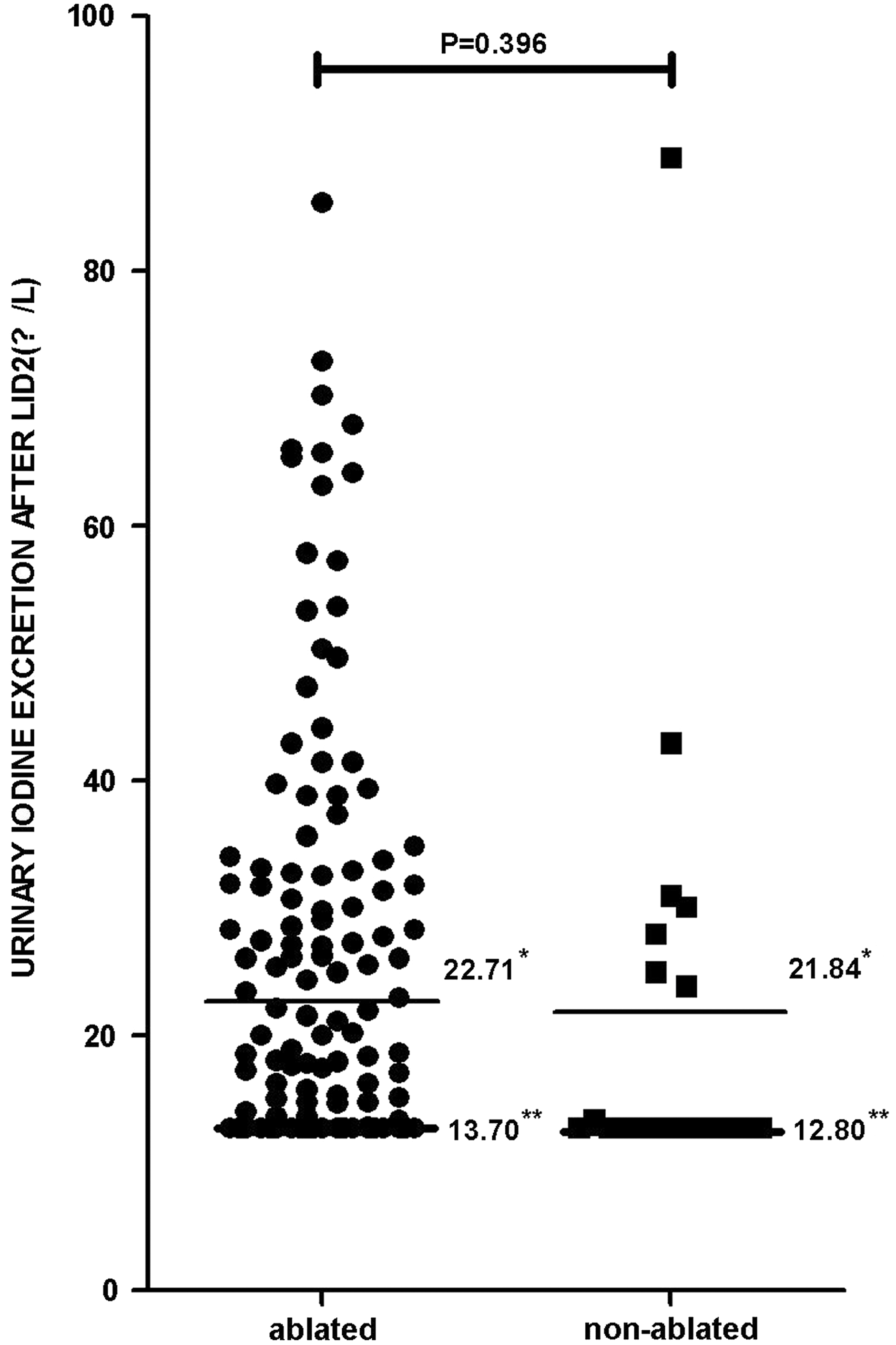
Differences in mean and median urine iodine excretion (UIE) (μg/L) values according to ablation outcome (based on criterion 1; negative whole body scintigraphy [WBS]). *Mean, **median.
Ablation outcomes based on the second criterion and clinical features associated with successful ablation
Seven patients with positive TgAbs were excluded and a total of 188 patients were enrolled in the analyses. Among them, 149 patients (79.26%) were successfully ablated according to the second criterion. The ablation success rate did not differ between the mild and moderately iodine deficient groups (p=0.54, chi-square test) (Fig. 2B). Serum Tg levels at the time of ablation therapy (ablation-Tg) were higher in the non-ablated group compared with the ablated group, and the differences were statistically significant (p=0.00, Mann-Whitney test). However, other factors, including age, sex, administered radioactive iodine dose, UIE after LID for 2 weeks, and TSH levels, did not differ between the two groups (Mann-Whitney and chi-square tests) (Table 4). The stimulated Tg level was the only significant variable (p<0.001) in multivariate logistic analysis (Table 5).
The second criterion for successful ablation is no visible uptake on a follow-up diagnostic 131I scan and stimulated serum thyroglobulin (Tg) levels <1 ng/mL.
LN, lymph node; UIE, urine iodine excretion.
The second criterion for successful ablation is no visible uptake on a follow-up diagnostic 131I scan and stimulated serum thyroglobulin (Tg) levels <1 ng/mL.
CI, confidence interval.
Discussion
Iodine is accumulated in thyroid tissue via the sodium/iodide symporter (NIS) (21). The NIS is a membrane protein that actively transports iodide ions into thyroid tissue and thus enables the high efficiency of radioiodine therapy (22). Iodine excess can result in saturation of iodine uptake sites in malignant and benign thyroid cells and cause decreased ablation efficacy. The study by Pluijmen et al. supported this theory (23): the LID group achieved higher successful ablation rates compared to the control group in their study. Goslings also reported that the effective half-life of radioactive iodine was increased after an 8-day LID (24). Similarly, Maruca et al. demonstrated that the lesional radiation was increased in two patients with metastatic thyroid carcinomas after a 5-day LID (25). Furthermore, several previous studies documented that NIS expression increased when the plasma iodine concentration was low (4,26,27), which can be an additional theoretical rationale for LID. Based on these data, in many countries, patients preparing for 131I ablation therapy are educated to avoid iodine-rich food and iodine-containing medications during the LID period. However, patients often complain of difficulties in maintaining a strict LID for extended periods of time. Thus, attempts to reduce the duration of a strict LID can be important in clinical situations, particularly iodine-rich countries.
The average iodine intake of normal Korean adults is 478.6 μg per day, and the average urine iodine concentration in the random urine is 674 μg/g (20,28). Considering that urinary iodine concentrations of 100 μg/L roughly correspond with a daily iodine intake of approximately 150 μg (15), mean UIE levels after LID for 1 and 2 weeks in our study were sufficiently low and both met the criteria for iodine deficiency. Successful iodine depletion was accomplished in 95.9% (187/195) of patients after LID for 1 week (87.2% of patients were moderately iodine deficient and 17% were mildly iodine deficient). Our results agree with data from a previous report that was also performed in Korea (29). These authors determined daily urinary iodine/creatinine ratios (I/Cr) and founded that the I/Cr ratio decreased below the cutoff value for iodine deficiency on day 6 of LID.
Sawka et al. examined all published literature on the topic of LID in 2010 (7). The authors reported that a LID does reduce urinary iodine output and LID for 2 weeks is about twice as effective as 1 week in their systematic review (7,30,31). Head-to-head comparison between our study and reviewed studies is difficult to perform because there is variation in methodologies, stringency of the restriction, duration of LID, geographic differences in dietary iodine intake, and disease-state of the subjects. Despite these limitations, the rates of successful iodine depletion after LID for 1 and 2 weeks in our data set were higher and UIE levels were lower than in previous reports (30 –32). Park et al. reported that 41% of patients obtained the targeted reduction of UIE (<100 μg/gCr) after LID for 1 week (30). Another study performed in Japan also found that 26% of patients achieved optimal UIE levels (<100 μg/gCr) after LID for 1 week (31). These discrepancies are possibly due to the effects of intense patient education and improved accessibility to medical staff. Previous reports provided a one-page sheet as an LID guide only at the regular visit to the outpatient clinic. In contrast, our hospital provides a 90-minute intensive LID education program to all patients by specially trained nurses and nutritionists. We have also established a hotline to answer patient questions regarding LID. These efforts might increase patient compliance with LID, resulting in higher LID success rates.
In our study, there were eight patients (8/195, 4.1%) classified as poorly prepared (≥100 μl/L, highest value: 148.5 μg/L) after LID for 1 week. Although their UIE levels did not satisfy WHO criteria for iodine deficiency (UIE levels <100 μg/L) (15) they complied with the recommendation of the EANM guidelines (UIE levels <150–200 μg/L) (16). Furthermore, ablation success rates based on the first criterion were not significantly different between the mild (UIE <50 μg/L) and moderatly iodine deficient (50≤UIE <100) groups. A similar result was obtained based on the second criterion. These data indicate that strict LID for 1 week is enough to achieve appropriate decreases in the body iodine pool before 131I ablation therapy, even in areas of iodine excess. Therefore, in subjects with UIE levels below 100 μg/L, efforts to turn mild iodine deficiency into moderate iodine deficiency by maintaining a strict LID for longer than 1 week will not increase the dietary efficacy of LID or the rate of successful ablation. However, it will increase patient inconvenience.
During long-term follow-up, serum Tg is a sensitive and reliable tumor marker for detection of disease recurrence and residual viable tumor after total thyroidectomy with or without RAIT in patients with DTC. Recent studies proposed that measurement of ablation-Tg forecasts treatment outcome. Lee et al. suggested that a post-operative stimulated Tg <2 ng/mL predicted disease-free status (33). Another study also suggested that ablation-Tg values correlate well with serum Tg levels at the time of initial diagnostic WBS and have a complementary role for predicting persistent or recurrent DTC (34). These results agree with our present results. When we evaluated potential factors that affect successful ablation, ablation-Tg in patients with negative TgAbs was the only factor associated with ablation success. This result suggests that patients who have small volumes of potential Tg-expressing foci, including remnant thyroid tissue or lymph nodes, tend to be easily ablated. Therefore, it is not the body iodine pool level but rather the ablation-Tg level that is a decisive factor to determine ablation outcomes when UIE levels enter into the target value (<100 μg/L).
In our study, the administered dose of 131I was not a significant indicator of ablation success. This result has a limitation because it was not derived from the data on radiation absorbed dose to the blood (BD). The mode of TSH stimulation (THW or rhTSH), renal clearance rate, and body iodine concentration are possible factors that can impact radioactive iodine (RAI) kinetics (35). In a study by Verburg et al., the success of ablation increased with increasing BD, but no dependence of the ablation rate on the administered activity was demonstrable (36). This means that the BD is a more powerful predictor of the successful ablation than the administered dose of 131I, considering the variation of iodine kinetics in each individual. A direct comparison between our results and theirs are difficult. However, the better successful ablation rates of our study than those in the study by Verberg et al. (89.74% vs. 76%, based on criterion 1 and 79.26% vs. 57%, according to criterion 2) may be partly related to the difference in RAI kinetics. Therefore, it should be studied further whether the BD affects ablation outcomes and which factors besides the ablation-Tg level provide a better forecast of the ablation success.
Based on the systematic review by Sawka et al. (7), there are still no studies examining long-term recurrence or mortality rates in patients treated with an LID compared to an unrestricted diet. Thus, further studies comparing the long-term outcomes in a strict LID group and less strict LID groups, or regular-diet groups, may be required.
In conclusion, our results show that a strict LID for one week is sufficient to achieve an adequate decreased of the body iodine pool before RAIT. Because the results of the current study were obtained in an iodine-rich area, we infer that an LID period of less than one week may be sufficient for patients who live in low dietary iodine intake areas. LID is a laborious process for most DTC patients and reducing its duration should have an immediate influence on patient quality of life.
Footnotes
Author Disclosure Statement
All authors state that they have no competing interests, financial or otherwise, to declare.