
Abstract
Background:
Malignant pleural effusion (MPE) caused by metastatic differentiated thyroid carcinoma (DTC) is usually associated with a rapid fatal outcome and should be recognized as a grim prognostic indicator. A standard therapeutic strategy has not been established for this situation. Here, we report a radioiodine-refractory follicular thyroid carcinoma (FTC) patient in whom a notable decrease of MPE was achieved after treatment with sorafenib.
Patient Findings:
A 50-year-old patient underwent a total thyroidectomy and resection of recurrence for poorly differentiated FTC followed by radioiodine therapy with a negative whole body scan. One year later, dissection of the inferior lobe of the left lung was performed because two fluorodeoxyglucose-avid nodules were identified; pathological examination revealed a metastatic poorly differentiated FTC. Half a year later, he was referred to our clinic because of cough, thoracic pain, nausea, and loss of appetite. Chest computed tomography showed right lung multiple nodules, left pleural effusion, and left lung collapse with left-sided pleural thickening. We treated him with sorafenib. Clinical and radiographic assessments were performed periodically.
Summary:
Symptoms and signs improved dramatically and continuously after initiation of sorafenib treatment. A duration of more than 12 weeks of apparent reduction of pleural effusion was achieved, which was confirmed by consecutive computed tomography examinations. Despite grade 1 alopecia, no other obvious treatment-related adverse events occurred.
Conclusions:
As a grim prognostic indicator for patients with DTC, no standard treatment recommendation for pleural effusion exists. Targeted therapy using sorafenib may be an effective therapeutic strategy in the treatment of MPE caused by FTC.
Introduction
P
A frequency of 0.56% (10/1772) and poor prognostic significance of pleural effusion in patients with papillary thyroid carcinoma (PTC) was reported by the MD Anderson Cancer Center (4). No cases of pleural effusion occurring in patients with follicular thyroid carcinoma (FTC) have been reported. Because of limited experience, management of thyroid carcinomas with pleural effusion is often problematic. There is no standard treatment recommendation in this setting in view of paucity of published data in the literature. Once malignant pleural effusion (MPE) appears, it is usually associated with a rapid progression and fatal outcome. The only conservative treatments are palliative thoracentesis and thoracoscopic pleurodesis. At present, management decisions are usually made based on case reports and retrospective series. Data from a meta-analysis suggests that thoracoscopic pleurodesis with talc may be an effective technique in patients with MPE (5). However, a number of questions with regard to pleurodesis for MPE remain unanswered. The principal question relates to the timing of pleurodesis in patients with metastatic disease. Data concerning quality of life, duration of hospital stay, and relative cost of the procedures have either not reported or are inadequate (5).
Recently, a growing understanding of molecular oncology has allowed the development of targeted agents in different types of advanced thyroid carcinomas, offering promising results (6). Sorafenib is an oral, small-molecule tyrosine kinase inhibitor targeting vascular endothelial growth-factor receptors (VEGFRs), RET/PTCs, and Raf/MEK pathways (7). Four phase II trials with sorafenib have been conducted at a dose of 400 mg twice daily, demonstrating the clinical benefits and acceptable safety of the agent (8 –11). We have also successfully performed two studies on sorafenib therapy for pulmonary metastases from PTC and brain metastasis from FTC, using a low-dose strategy (200 mg, twice daily), in which tolerance to the drug and a potential therapeutic effects were demonstrated in patients with radioiodine-refractory DTC (12,13). More recently, The U.S. Food and Drug Administration has expanded the approved uses of sorafenib for the treatment of patients with locally recurrent or metastatic, progressive DTC that is refractory to 131I treatment. However, the therapeutic effect and safety of sorafenib have not been assessed in the treatment of pleural effusion from DTC.
Patient
A 50-year-old male with hoarseness was found to have a nodule in his thyroid gland in December 2011. A total thyroidectomy was performed with pathologically confirmed poorly differentiated FTC. 131I ablation was carried out 3 months after operation using a dose of 3700 MBq. A 131I whole body scan (131I-WBS) showed mild radioiodine accumulation in the thyroid remnant without any 131I-avid extra-thyroidal lesion. In December 2012, he again received a resection because of tumor recurrence in the left tracheo-esophageal groove. In January 2013, two nodules in the inferior lobe of the left lung were identified as fluorodeoxyglucose (FDG)-avid lesions by positron emission tomography–computed tomography (PET-CT) (Fig. 1). The inferior lobe of the left lung was then removed, and pathological examination revealed a poorly differentiated metastatic FTC. 131I-WBS 5 days after the administration of a therapeutic dose of 7400 MBq revealed no abnormal 131I-avid lesion (Fig. 2).
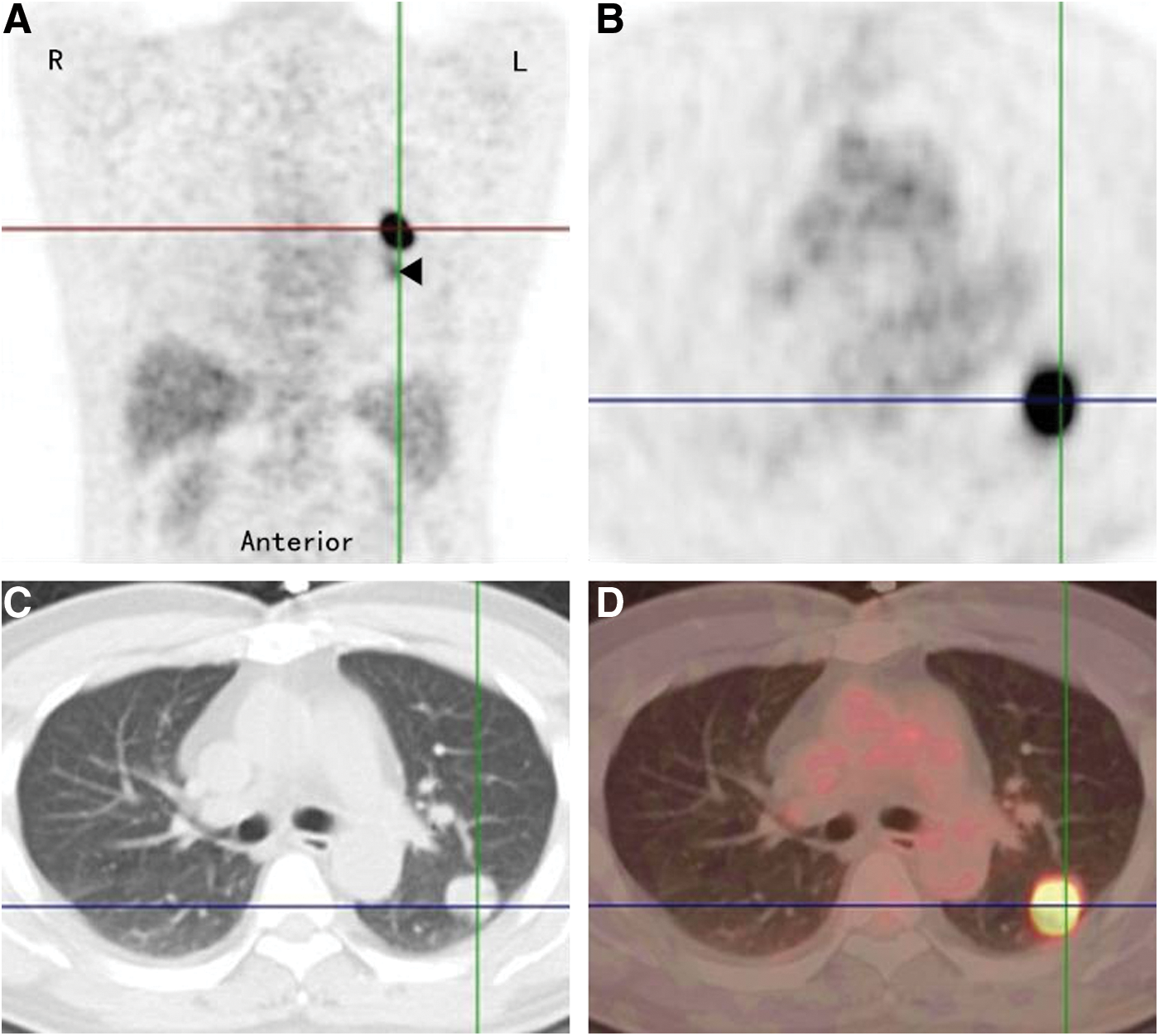
18-Fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) showing two nodules in the inferior lobe of the left lung with maximum standard uptake values of 13.2 (upper lesion, crossing of threads) and 4.7 (lower lesion, arrowhead).
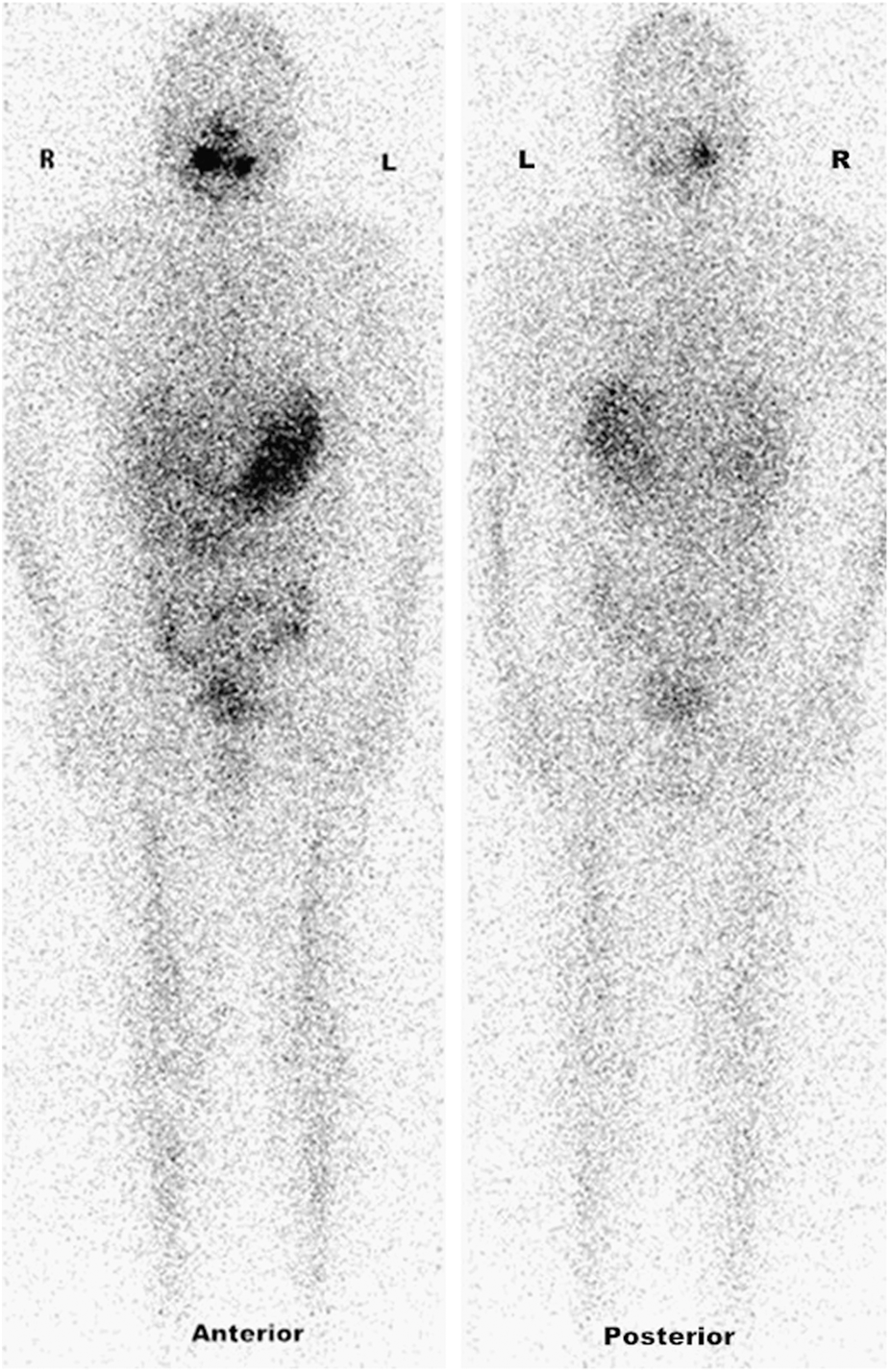
Whole-body planar scan 5 days after the oral administration of 7400 MBq 131I showing no abnormal accumulation after resection of pulmonary metastases and indicating that no 131I-avid lesions exist and 131I therapy is no longer indicated.
In September 2013, he was referred to our clinic because of cough, fatigue, thoracic pain, chest tightness, nausea, and loss of appetite. Compared with the PET-CT, a chest CT showed multiple new right lung nodules, left pleural effusion, and left lung collapse with pleural thickening. The serum thyrotropin, thyroglobulin, and antithyroglobulin antibody were 16.49 μIU/L, >1000 ng/mL, and 55.42 IU/mL, respectively. We made a diagnosis of multiple radioiodine-refractory metastases from FTC combined with MPE, considering the history of malignant tumor, pleural nodules, and pleural thickening. In view of the iodine-refractory and progressive nature of his disease, 131I therapy was no longer indicated. The patient was treated conservatively with palliative thoracentesis and drainage. A suggestion of pleurodesis was refused by the patient. The daily average of pleural drainage was 600 mL. After obtaining written informed consent, sorafenib was then administered orally at a dose of 200 mg twice a day as reported previously, followed by periodical CT examinations (13).
One week after the initiation of sorafenib treatment, the daily pleural drainage decreased to 250 mL. Two weeks after the start of sorafenib treatment, his cough, fatigue, nausea, and loss of appetite improved substantially, and he was extubated since drainage was no longer needed. Twelve weeks after the beginning of sorafenib therapy, his thoracic pain, and chest tightness decreased significantly. Consecutive CT examinations confirmed significant and sustained reduction of the pleural effusion and the diameter of the pleural nodules (Fig. 3). A partial response was achieved in lung metastases according to Response Evaluation Criteria in Solid Tumor criteria. Despite grade 1 alopecia, other obvious treatment-related adverse events did not occur. The total duration of sorafenib treatment was at least 14 weeks, and at the time of this writing, the patient was still taking sorafenib.
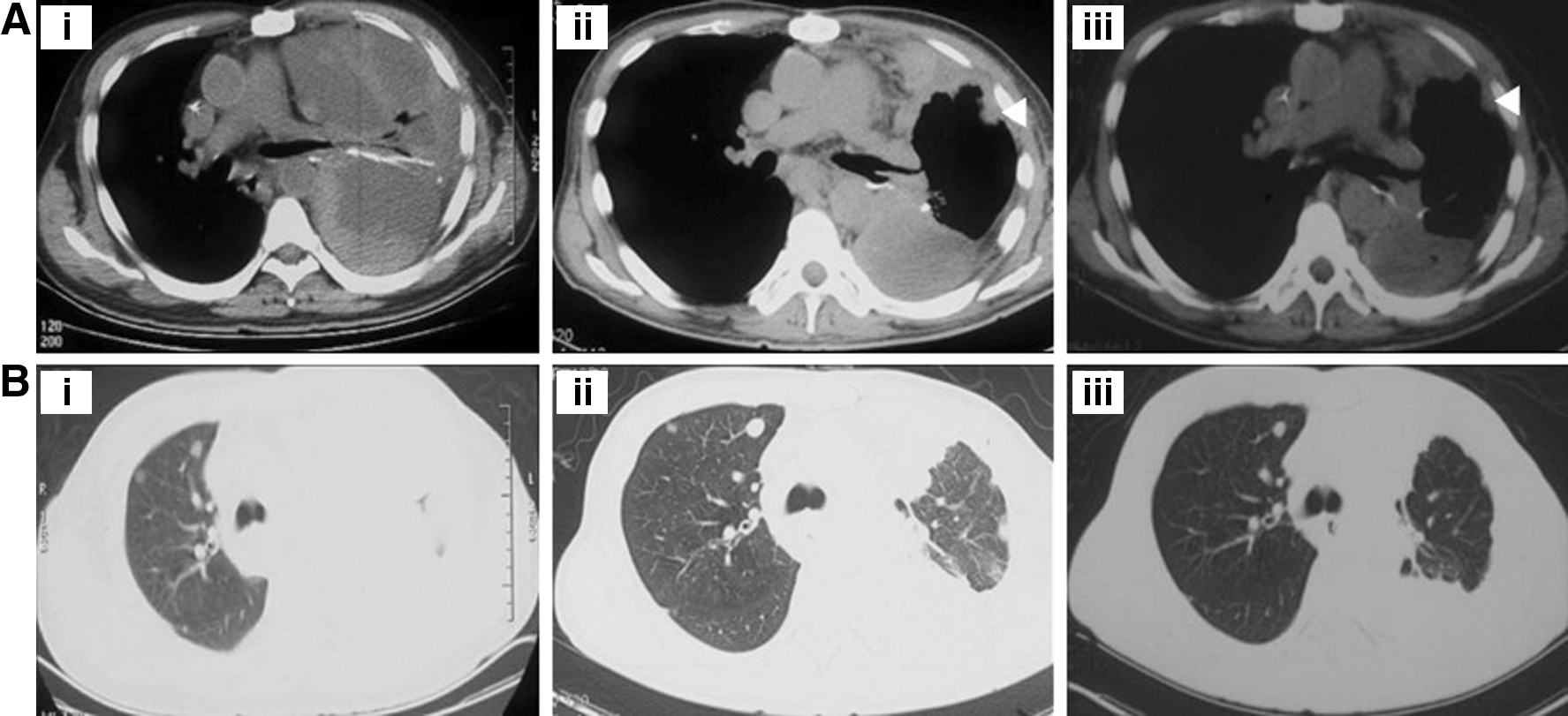
Computed tomography scans of the chest [axial view, mediastinal
Discussion
The incidence of thyroid cancer has increased throughout the world in the past two decades, with PTC being more frequent than FTC. Although the incidence of cervical lymph metastases at the time of diagnosis of DTC is 45%, this is not always associated with a poor prognosis. The most common cause of death from thyroid carcinoma is local recurrence, followed by lung metastasis (14). Especially in those with iodine-resistant disease, the therapeutic effect of 131I is poor.
MPE is most commonly caused by lung cancer or metastases from breast cancer, gastrointestinal carcinoma, or ovarian or lymphoid malignancies (15). The fluid compresses the lung and causes respiratory problems, and hospital treatment is usually necessary. The prevalence of effusions associated with malignant thyroid carcinomas was 0.13% of all effusions and 0.67% of all malignant pleural effusions (16). With respect to thyroid carcinoma, MPE was found in only 0.56% of patients as reported in a large case series over a period of 47 years, and it may occur many years after pulmonary metastases have been identified. Typically, the presence of MPE portends a dismal prognosis, with a reported median survival of 11 months (4). To the best of our knowledge, MPE has been found only in patients with PTC, with the exception of one patient with a Hürthle cell carcinoma (4,17,18). Hence, this is the first report of MPE caused by FTC.
In the management of DTC, 131I avidity is a crucial factor, as 131I therapy is used not only for postoperative ablation of the thyroid remnant, but also as primary choice for the treatment of locoregional recurrences and distant metastases (19,20). However, some recurrences or metastatic lesions of DTC fail to concentrate iodine, leading to false negative 131I-WBS, as shown in Fig. 2, and poor outcomes. In our patient, the interval between resection of pulmonary metastatic lesions and the development of MPE was merely 8 months, suggesting a progressive nature of the disease. During this interval, another course of 131I therapy using a high dose of 7400 MBq still failed to control the progression of the disease, indicating a poor outcome.
18F-FDG uptake often reveals malignant tumors because neoplastic cells exhibit increased rates of glycolysis and glucose consumption with accelerated production of glucose transport proteins (21). In a review, the maximum standard uptake values (SUVmax) were collected from eight studies, and the mean SUVmax was calculated as 4.8–3.1 for benign lesions versus 6.9–4.7 for malignant lesions. This suggests a potential utility of SUVmax in differentiating malignant lesions from benign lesions, although there is pronounced overlap (22). In this patient, serum thyroglobulin was found to be higher than 1000 ng/mL, and lung lesions with high glucose metabolism were revealed by FDG-PET/CT. The SUVmax of 13.2 and 4.7 were strongly suggestive for malignant lesions. Based on the negative WBS after the administration of a therapeutic dose of 131I, additional courses of 131I therapy were no longer suitable. Although a resection of the inferior lobe of the left lung was performed, new pulmonary lesions with MPE occurred half a year later, indicating a progressive disease needing new therapeutic strategies. Since the volume of daily drainage was large and the suggestion of pleurodesis was refused, targeted therapy was initiated.
Increasing knowledge about the molecular mechanisms underlying thyroid cancer identifies the RAS/RAF/MAPK/ERK and RET kinase pathways and pronounced angiogenesis as important drivers of the progression of metastatic thyroid cancer (23). BRAF is a member of the RAF kinase family of serine/threonine-specific protein kinases. This protein plays key role in regulating the MAPK/ERK signaling pathway, which affects cell division, differentiation, and secretion (24). VEGF is a signal protein produced by cells and stimulates angiogenesis. Additionally, the fact that VEGF contributes to the formation of malignant effusion by increasing vascular permeability has been demonstrated (25). Therefore, inhibition of such pathways may effectively treat tumors and reduce effusion as well. This possible mechanism has been verified by our previous study, in which partial response of brain metastasis and continuous improvement of perilesional edema were both achieved by treatment with sorafenib (12).
As a novel therapeutic strategy, targeted therapy using sorafenib or other agents has been proved to be useful in the treatment of advanced or metastatic 131I-refractory DTC, especially when there are pulmonary metastases (13,26,27). To the best of our knowledge, this is the first exploratory study of sorafenib treatment for MPE caused by a thyroid carcinoma. As demonstrated by sustained improvement of clinical features and radiologic findings, a notable response to sorafenib treatment for MPE was achieved in our patient, suggesting that targeted therapy may be a novel strategy in the control of MPE caused by FTC.
Conclusions
As a grim prognostic indicator for patients with DTC, no standard treatment recommendation for pleural effusion exists. This is the first report describing an effective use of sorafenib for the treatment of malignant pleural effusion caused by a follicular thyroid carcinoma.
Footnotes
Acknowledgments
This study was sponsored by the National Natural Science Foundation of China (30700187), Shanghai Rising-Star Program (08QA14040), and the Public Health Bureau of Shanghai Municipality (2006Y34). The work was also partially sponsored by the National Natural Science Foundation of China (81271609) and the Shanghai Rising-Star Program (12QH1401600).
Author Disclosure Statement
No competing financial interests exist.