
Abstract


Scientific Meeting Program (as of 9/3/2013)
Thursday, October 17, 2013
Thyroid Hormone Metabolism & Regulation Thursday Highlighted Oral Basic 9:00 AM
Nuclear receptor co-repressor (NCoR) and silencing mediator of retinoid and thyroid hormone receptors (SMRT) are well-recognized co-repressors of the thyroid hormone receptor (TR) isoforms and other nuclear receptors. Defects in their function can lead to alterations in thyroid hormone (TH) signaling and metabolic dysfunction. Indeed, we have shown previously that deletion of NCoR function enhances TH action on TR target genes. However, whether NCoR or SMRT have have specific roles in TH action has never been tested previously in vivo.
To test our hypothesis that NCoR is the specific corepressor for the TR we generated mice that lack functional NCoR (NCoRΔID), SMRT (SMRT−/−) or both (DKO) in the liver only using cre/lox technology and then assessed TH and metabolic signaling in either euthyroid or hypothyroid animals.
Consistent with our hypothesis, the isolated deletion of SMRT in the liver had no effect on enhancing TH action in either the hypothyroid or euthyroid state on all TR target genes tested including fasn, thrsp, dio1, gpd2 and bcl3. In contrast and as seen previously the disruption of NCoR function greatly enhanced TH action on all TR targets. The phenotype of DKO mice in context of TH-signaling was similar to NCoRΔID mice confirming the dominant and necessary role of NCoR in TH action. To discern what role SMRT may be playing in the liver we further analyzed the phenotype of DKO mice. Remarkably, DKO mice have significant hepatic steatosis and decreased serum triglycerides compared to WT, NCoRΔID and SMRT−/− mice. Consistent with this, there was profound upregulation of both lipogeneic and lipid droplet formation gene expression in DKO mice. In contrast to TH-signaling, both NCoR and SMRT appear to be required for this steatotic program. Interestingly, the phenotype and gene expression profile of DKO mice closely parallels that found in mice which lack HDAC3 in the liver.
Taken together these data demonstrate that co-repressor specificity exists in vivo as NCoR plays a specific role in TH signaling that cannot be compensated for by SMRT. In contrast, both NCoR and SMRT control hepatic lipogenesis and lipid droplet formation and are absolutely required for the actions of HDAC3.
Thyroid Hormone Metabolism & Regulation Thursday Highlighted Oral Basic 9:15 AM
Type 2 deiodinase (D2) is expressed in skeletal muscle (SKM) at low levels but it is thought to play a role in SKM biology. However, SKM has ectopic deposits of brown adipose tissue (BAT) that could be the source of local D2.
To test this, we developed two new mice with tissue-specific D2 inactivation, i.e. SKM-D2KO or FAT-D2KO by crossing floxed Dio2 mice with the MLC-Cre or the AP2-Cre mice, respectively. In neonatal mice, all hind limb muscles (HLM) were dissected, pooled and processed for D2 activity. In adult mice the soleus muscle (SOL) was used: 200 ug total protein incubated for 3 h in PE buffer containing 20 mM DTT, 1 mM PTU and 0.1 nM 125I-T4 (100 nM for background); results expressed as fmol T4/mg/min; only littermate controls were used.
HLM D2 activity was 40–50% lower in SKM-D2KO as well as in FAT-D2KO. At the same time, SOL D2 activity was ∼75% lower in SKM-D2KO and ∼70% in FAT-D2KO. SOL D2 mRNA levels were also lower in SKM-D2KO by ∼37% and in FAT-D2KO by ∼40%. BAT D2 activity did not change in SKM-D2KO mice but it was ∼65% lower in FAT-D2KO. Hypothyroidism (6 wks on LID+PTU) increased SOL D2 activity by about 8-fold in all animals. However, D2 mRNA was not affected given the predominant post-translational D2 regulation. We studied MyoD, Myh2, Pgc1a, Glut4 and Serca2 gene expression in SOL, and only the latter was ∼20% reduced in SKM-D2KO. The expression of a larger group of genes was not affected in SOL D2KO, in agreement with the finding of normal exercise running capacity in D2KO. When placed on a high fat diet for 8 wks, SKM-D2KO mice exhibited similar body weight, body composition, VO2 and RER as littermate controls. Serum levels of TSH, T4 and T3 were not different in the SKM-D2KO, but there was a ∼24% elevation in serum T4 in FAT-D2KO mice.
In conclusion, D2 mRNA and activity in SKM reflect the combined expression in skeletal myocytes and adipocytes. D2 inactivation did not affect muscle function or energy homeostasis. Remarkably, D2 inactivation in adipose tissue, but not in SKM, resulted in impaired extrathyroidal conversion of T4 to T3.
Autoimmunity Thursday Highlighted Oral Clinical 9:30 AM
Multiple case reports and series suggest that rituximab (RTX), an anti-CD20 monoclonal antibody that induces transient B-cell depletion, might be effective therapy for patients with Graves' ophthalmopathy (GO).
We performed a prospective, randomized, double blind, placebo-controlled trial of RTX in patients with active GO [clinical activity score (CAS)≥4] and moderate to severe disease severity. Enrolled patients were euthyroid and either failed or refused glucocorticoid therapy. Patients received 2 RTX infusions (1000 mg each) or saline 2 weeks apart and were assessed by both endocrinologist and ophthalmologist at weeks 8, 16, 24 and 52. The primary end point at 24 weeks was a reduction in CAS assessed as a continuum. Secondary endpoints included success/failure rate (a composite variable of decrease in CAS ≥2 points and no need for additional eye treatment vs. either CAS decrease of <2 points or need for additional therapy), reduction in CAS of ≥2 points, decrease in NOSPECS by ≥2 classes, proptosis by ≥2 mm, lid aperture width by ≥3 mm, motility of ≥8 degrees, and improvement in a GO-specific quality-of-life scale ≥6 points.
21/25 patients completed the study to the primary outcome point. The treatment groups were similar in age, gender, smoking prevalence and CAS. CAS at 6 months decreased from baseline in most patients with no difference between groups [mean CAS change (standard deviation) was 1.4 (1.6) for placebo vs. 1.6 (1.8) for RTX, p=0.86]. Overall therapy failure rate at 6 months did not differ between groups (75% for placebo vs. 62% for RTX, p=0.67). There were 7 adverse events (AE) in 4 patients in the control group and 12 AE in 8 RTX-treated patients; optic neuropathy developed during the trial in 2 of the RTX-treated patients.
RTX was no more effective than placebo at 24 weeks in our population of patients with active and moderate to severe GO.
Thyroid Cancer Thursday Highlighted Oral Clinical 9:45 AM
In a randomized phase 3 study, cabozantinib extended progression-free survival (PFS) in pts with progressive, metastatic MTC (median 11.2 mo cabozantinib treated arm vs 4.0 mo placebo, p<0.0001; Schöffski, 2012) with a response rate (RR) of 28% in the cabozantinib arm.
Pts in the phase 3 study were evaluated for the presence of somatic and germline RET mutations using Sanger and next generation methods using blood, primary tumor, and metastatic tumor samples. Pts without evidence of RET mutation were evaluated for KRAS, NRAS, and HRAS mutations by next generation sequencing. Impact of tumor mutational status was evaluated with respect to PFS and RR according to RECIST.
Sixty-five percent of study pts had their RET status determined (215 of 330 total pts). Of those, 79% harbored an activating mutation (59% exhibited the poor prognosis mutation M918T) and 21% lacked a RET mutation. Generally only a single tumor sample was provided per pt, either primary tumor (117 of 215) or metastasis (65 of 215). Two of 14 pts who had both primary tumor and metastasis samples evaluated showed a RET mutation in the metastasis but not the primary tumor. Approximately 30% of the pts lacking a RET mutation were subsequently found to harbor a mutation in HRAS, KRAS, or NRAS. The greatest benefit was observed in the following: the subgroup of pts who are RET mutation positive (hazard ratio 0.23), the subset of those pts with RET M918T mutations (hazard ratio 0.15) and the subgroup of pts with RAS mutations (hazard ratio 0.15). Kaplan-Meier analysis of the RET mutation negative subgroup (n=46) indicates a heterogeneous population, with PFS benefit largely attributable to pts with RAS mutations. Pts who were both RET and RAS mutation negative (n=30) showed a 21% RR but little prolongation of PFS on cabozantinib. The common polymorphism RET G691S did not show an effect on PFS in either arm. RRs are highest in the subgroups which show the greatest prolongation of PFS: all RET mutations, RET M918T mutations, and RAS mutations (RRs of 32%, 34%, and 31%, respectively).
Pts with activating RET and RAS mutations show the greatest improvement in PFS and tumor response on cabozantinib although benefit was seen across mutational subgroups.
Iodine Uptake & Metabolism Thursday Oral Translational 1:50 PM
A genetically engineered mouse model (GEMM) of pancreatic ductal adenocarcinoma (PDAC) is induced by activation of constitutively active KrasG12D in combination with a deletion of p53, which shows the typical changes of human disease.
In previous proof-of-principle studies using xenograft mouse models the sodium iodide symporter (NIS) as well characterized theranostic gene allowed detailed molecular imaging of transgene expression and highly effective application of therapeutic radionuclides. As a next step towards clinical application, in the current study we investigated tumor specificity and transduction efficiency of tumor-targeted polyplexes as systemic NIS gene delivery vehicles in the advanced GEMM of PDAC. Therefore, we used novel tumor-targeted polyplexes based on linear polyethylenimine (LPEI), polyethylene glycol (PEG), and the synthetic peptide GE11 as an epidermal growth factor receptor (EGFR)-specific ligand (LPEI-PEG-GE11) to target a NIS-expressing plasmid to the high EGFR-expressing PDAC.
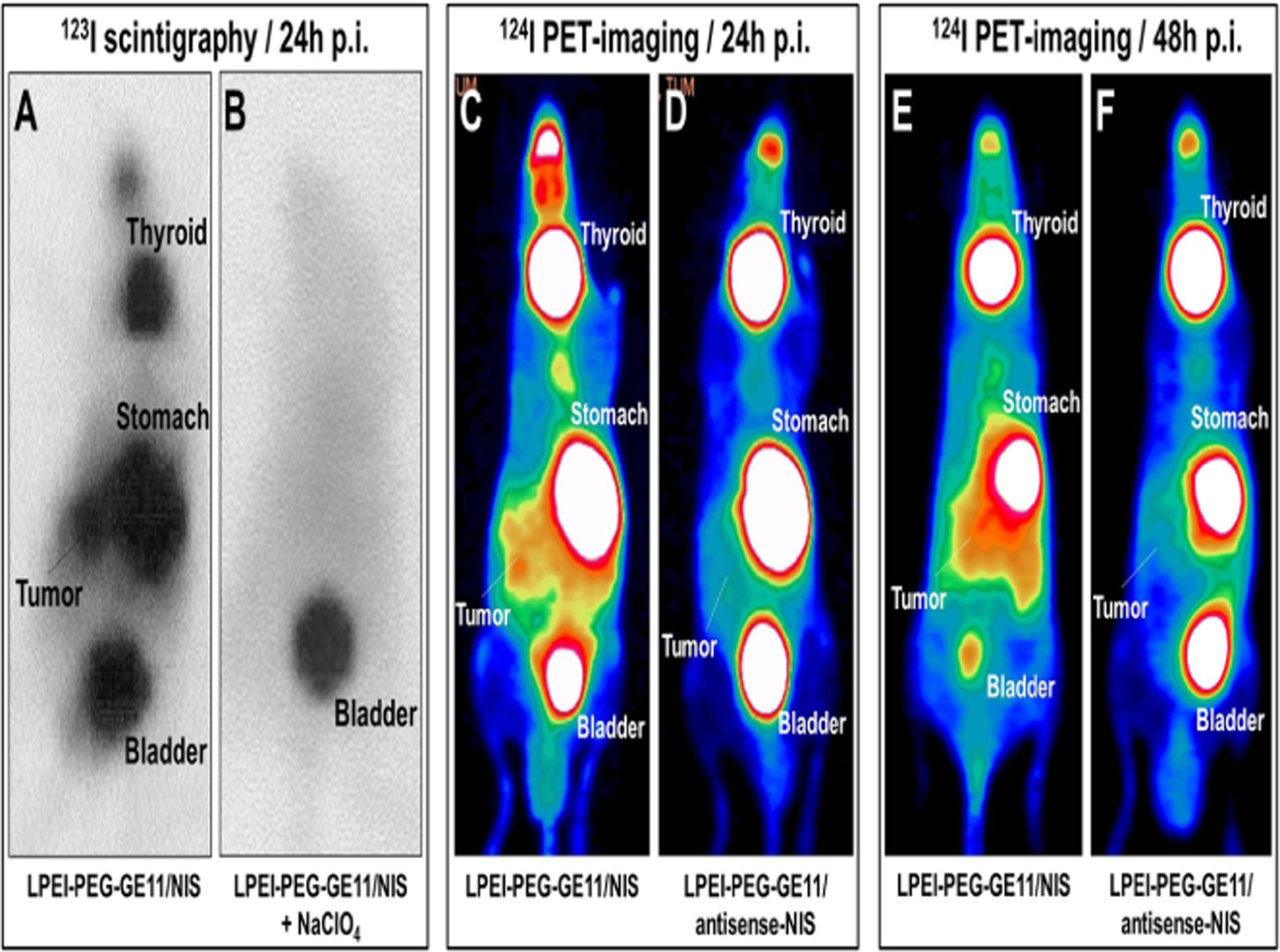
In vitro iodide uptake studies with cell explants derived from murine EGFR-positive and EGFR-knockout PDAC lesions demonstrated high transduction efficiency and EGFR-specificity of LPEI-PEG-GE11/NIS. In vivo 123I γ-camera-imaging and 3-dimensional high-resolution 124I-PET-imaging experiments showed significant tumor-specific accumulation of radioiodine. These results were further confirmed by NIS-specific qPCR analysis and immunohistochemistry. A first series of therapy studies indicates that the tumoral accumulation is high enough for a dramatic therapeutic effect of 131I as demonstrated by significant reduction of tumor volume that was measured by magnetic resonance imaging.
In conclusion, our preclinical data in an advanced GEMM of PDAC clearly demonstrate the enormous potential of EGFR-targeted synthetic polymers for systemic NIS gene delivery allowing for targeted radionuclide therapy of non-thyroidal cancers.
Thyroid Cancer Thursday Oral Basic 2:05 PM
With a median survival of 5 months and lack of curable therapies, Anaplastic thyroid carcinoma (ATC) represents one of the most aggressive forms of cancer. Recently, advances in immunotherapy have resulted in clinical responses in patients with cancer, although against solid tumors, the success has been limited to a few immunogenic cancers such as malignant melanoma. We sought to investigate whether ATC is a suitable target for immunotherapy.
16 ATC and 3 PTC cell lines were established from fine-needle aspirates (FNA) and analyzed for 1) their susceptibility to killing by natural killer (NK) cells in vitro by 51Cr-release cytotoxicity assay; 2) expression of ligands to activating NK cell receptors by flow cytometry for; and 3) their propensity to secrete NK cell attracting chemokines by ELISA. Furthermore, FNA and peripheral blood was obtained from 4 untreated ATC patients and analyzed for infiltration and phenotype of NK cells as well as tumor cells.
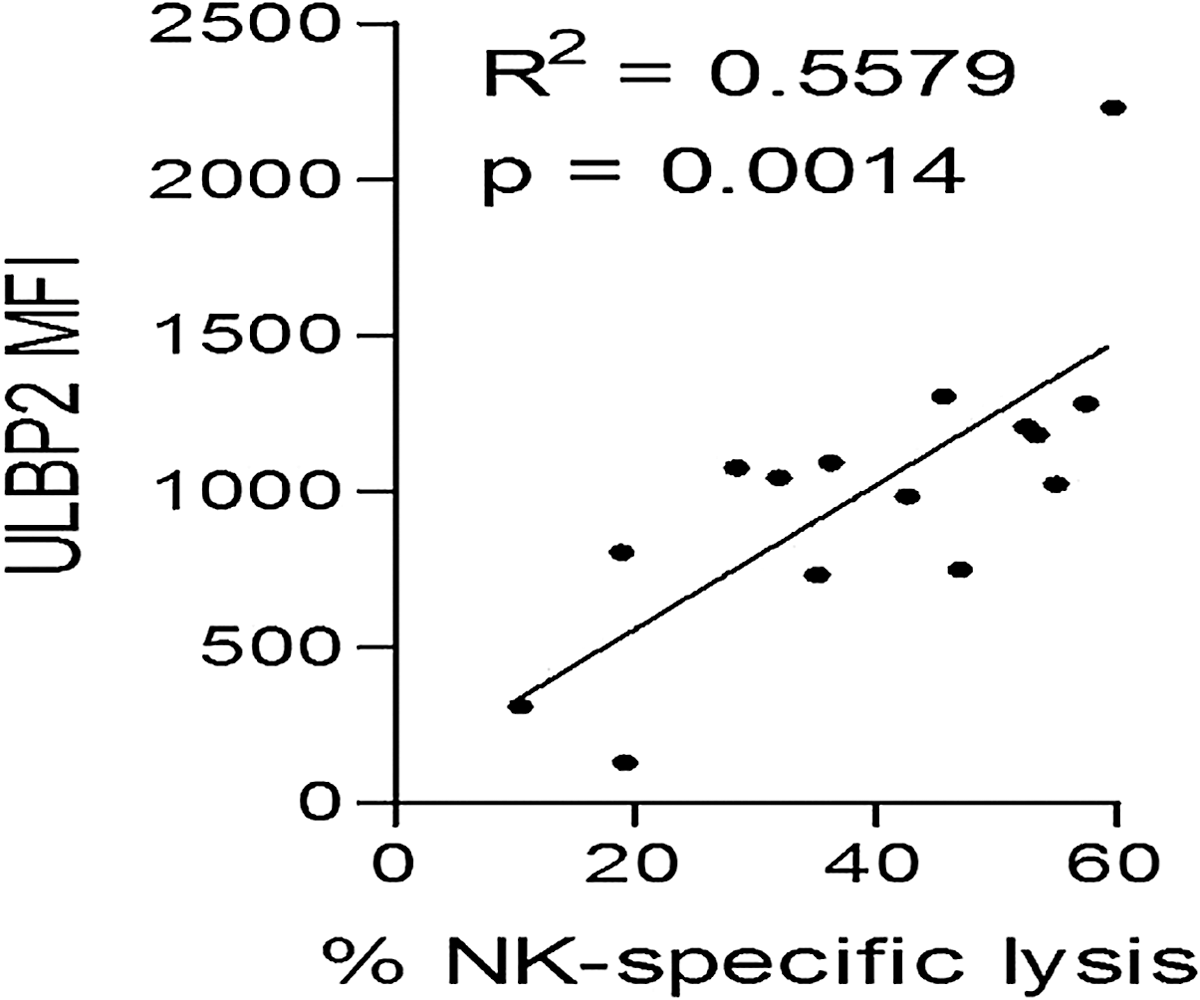
Linear regression analysis of NK cell mediated killing and mean flurorescence intensity (MFI) of ULBP2 on thyroid cancer cells.
Our functional analysis revealed that ATC cell lines are extremely sensitive to lysis by ex vivo expanded NK cells, despite a high expression of MHC class I (range NK cell killing=16.1–97.1%, mean=58.9%), while the PTC cell lines were more resistant to NK cell lysis (range NK cell killing=10.6–55.5%, mean=31.5%). NK cell mediated lysis of ATC cells was abrogated upon blockade of the NK cell activating ligand NKG2D. A phenotype analysis revealed that the level of sensitivity to NK cell lysis correlated with surface expression of the NKG2D-ligand UL 16 binding protein 2 (ULBP2) on thyroid cancer cells (p=0.0014). Moreover, silencing or blockade of the ULBP2 receptor on ATC cells resulted in increased resistance to NK cell mediated lysis. In addition, several of the ATC cell lines produced high levels of the chemokine CXCL10 and were able to stimulate migration of NK cells in vitro. In fresh ATC tumor samples NK cells had a reduced expression of the NKG2D receptor compared to NK cells in peripheral blood from the same patient.
Our findings demonstrate that ATC tumor cells are prone to attract and undergo lysis by NK cells. We conclude that ATC is a promising target for treatment strategies involving adoptive transfer of ex vivo expanded NK cells.
Thyroid Cancer Thursday Oral Translational 2:20 PM
MicroRNA-145 (miR-145) has been reported as a tumor suppressor. Ectopic expression of miR-145 in cancer cells leads to decreased proliferation and induces morphological changes. However, the role of miR-145 in thyroid cancer is undefined. The aim of this study was to characterize expression of miR-145, identify its function in thyroid cancer cells, and determine its diagnostic utility in thyroid cancer.
The viability of thyroid cancer cells was determined after transfection by either miR-145 or miR-C. Cell cycle progression and DNA fragmentation was investigated by flow cytometry and western blot. Luciferase expressing 8505C cells were transfected with miR-145 or miR-C for in vivo experiments. Subcutaneous flank injections into nude mice were used to determine whether miR-145 inhibits tumor growth. The role of miR-145 and tumor metastasis was explored by tail vein injection into IL-2 knockout mice. The expression of miR-145 was evaluated by quantitative RT-PCR in training and validation sets FNA samples and in serum samples from patients with PTC, benign lesions, and healthy controls. Exosomes were extracted from the thyroid vein, peripheral circulation, and medium.
Our results show miR-145 is downregulated in thyroid cancer. In vitro miR-145 overexpression resulted in G2/M cell cycle arrest, decreased cellular proliferation, migration, invasion, expression of EMT markers, and VEGF secretion, as well as inhibition of the PI3K/Akt pathway. In vivo miR-145 overexpression decreased tumor growth, metastasis, and VEGF secretion. Furthermore, inhibition of miR-145 in normal thyroid primary culture decreased expression of key regulators of thyroid cell differentiation. Serum miR-145 levels were higher in patients with thyroid cancer, and a gradient based on proximity to the tumor was demonstrated. As a diagnostic biomarker, miR-145 had a negative predictive value of 92% in distinguishing between benign and malignant thyroid nodules in indeterminate FNA.
These data show miRNA-145 to be a master regulator of thyroid cancer growth which is likely mediated through its effect on the PI3K/Akt pathway. Mir-145 is likely secreted by thyroid cancer cells, and may be a helpful adjunct marker for thyroid cancer diagnosis.
Thyroid Development Thursday Oral Basic 2:35 PM
Thyroid follicular cells (TFCs) are recognized by their expression of a gene quartet including thyroglobulin (Tg), thyroperoxidase (TPO), thyroid stimulating hormone receptor (TSHR) and the sodium/iodide symporter (NIS) genes. The expression of this gene quartet is dependent on a unique set of transcription factors including NKX2 homeobox 1 (NKX2-1, formerly called TTF-1), forkhead box protein E1 (FOXE1, formerly called TTF-2) and paired box gene 8 (PAX8) which are not expressed simultaneously in any other cell type. NKX2-1 and PAX8 are known to associate biochemically and synergistically in their role as thyroid gene activators. We have successfully used the ectopic expression of PAX8 and NKX2-1 to induce the differentiation of murine embryonic stem (ES) cells into TFCs (Thyroid 23:385, 2013) and following further development toward the endodermal lineage such cells developed into three-dimensional thyroid follicles and expressed abundant thyroglobulin protein in vitro.
To assess the in vivo potential of such ES cells, expressing both PAX8 and NKX2-1, we injected, subcutaneously, increasing numbers (104–106) of embryoid body cells suspended in a soluble basement membrane extract (Matrigel) into nude mice and observed their development.
Histological analysis revealed the formation of thyroid tissue, 4 weeks after injection, forming what we have previously termed a “thyroid organoid”, with fully developed, and developing, follicles and reaching ∼0.8 cm in size. Immunohistochemical analysis of the graft tissue showed intracellular Tg and Tg deposition in the luminal compartments.
This thyroid transplantation model using ES cells furthers the possibility of thyroid gland replacement for patients with congenital hypothyroidism or following total thyroidectomy.
Thyroid Hormone Action Thursday Oral Basic 2:50 PM
The human syndrome resistance to thyroid hormone (RTH) is characterized by high thyroid hormone (TH) and thyroid stimulating hormone (TSH) levels. Mice with mutations in the thyroid hormone receptor beta (Thrβ) gene that affect its ability to bind the steroid-receptor coactivator 1 (SRC-1) or mice that are null for SRC-1 have a phenotype similar to RTH. In contrast, mice that express a mutant nuclear corepressor 1 (Ncor1) allele that cannot interact with TRβ, termed NCoRΔID, have low TH levels and normal TSH. We hypothesized that RTH present in Src-1−/− mice is due to unopposed corepressor action blocking appropriate T3-mediated regulation.
To test our hypothesis we crossed NCoRΔID/ΔID and Src-1−/− mice resulting in mice deficient for both coregulators in all cell types. We measured TH levels in WT, NCoRΔID/ΔID, Src-1−/− and NCoRΔID/ΔID Src-1−/− mice by performing radioimmunoassays. TSH levels were measured in all genotypes with a Multiplex™ assay (Millipore). Using quantitative real time PCR, we evaluated mRNA levels in the pituitary and the liver. Lastly, to test recruitment of coregulators by the TR we performed chromatin immunoprecipitation assay (ChIP) for SRC-2 in the livers of WT and NCoRΔID/ΔID Src-1−/− mice.
Remarkably NCoRΔID/ΔID Src-1−/− mice have normal TH and TSH levels and are T3 sensitive at the level of the pituitary thyrotroph. Although the absence of SRC-1 prevented T3-activation of key hepatic gene targets, the expression of NCoRΔID in Src-1−/− mice allowed these targets to reacquire T3 sensitivity. We next asked if the removal of both NCoR and SRC-1 allowed other coregulators to be recruited by the TR on the promoters of target genes? Using ChIP, we found enhanced recruitment of SRC-2 to the promoter of T3-sensitive genes Thrsp14 (Spot14) and Gpd2 in NCoRΔID/ΔID Src-1−/− mice suggesting that SRC-2 is responsible for T3 sensitivity in NCoRΔID/ΔID Src-1−/− mice and that removal of WT NCoR1 augments SRC-2 binding to the TR.
In conclusion, T3 targets require a critical balance between NCoR1 and SRC-1 in order to respond appropriately to T3. Furthermore, expression of the mutant NCoRΔID allele in Src-1−/− mice corrects their RTH phenotype by allowing increased recruitment of SRC-2 to the TR.
Thyroid Hormone Action Thursday Oral Basic 3:05 PM
Genetic evidence from patients with mutations of the thyroid hormone receptor α gene (THRA) indicates that the dominant negative activity of mutants underlies pathological manifestations. Using a mouse model expressing a dominant negative TRα1 mutant (PV) and a mutated nuclear receptor corepressor (NCOR1ΔID) (Thra1PV/+Ncor1ΔID/ΔID mice), we recently showed that aberrant release of TRα1 mutants from the NCOR1-histone deacetylase (HDAC) repressor complex mediates the dominant negative actions of TRα1 mutants.
We tested whether HDAC could be a potential molecular target by treating Thra1PV/+ mice with an HDAC inhibitor, SAHA, daily for 2 months and evaluating its effects.
SAHA treatment did not significantly correct the abnormalities in body weight of Thra1PV/+ mice, but it ameliorated the impaired bone development and adipogenesis. A 19% reduction in femur length of vehicle-treated Thra1PV/+ mice was partially corrected to a 15% reduction in SAHA-treated mice. We previously showed that the expression of NCOR1ΔID reverted the 19% reduction in femur length of Thra1PV/+ mice to a 17% reduction in Thra1PV/+Ncor1ΔID/ΔID mice. SAHA treatment further corrected this to a 12% reduction. Moreover, a 69% reduction in white adipocyte tissue (WAT) mass in vehicle-treated Thra1PV/+ mice was partially corrected to a 44% reduction in SAHA-treated Thra1PV/+ mice. The expression of NCOR1ΔID reverted the 69% reduction in WAT mass of Thra1PV/+ mice to a 24% reduction in Thra1PV/+Ncor1ΔID/ΔID mice. Remarkably, SAHA-treated Thra1PV/+Ncor1ΔID/ΔID mice exhibited normal WAT mass and histology. Analysis showed that the expression of PPARγ and C/EBPα, the 2 master regulators of adipogenesis, were markedly higher in WAT of SAHA-treated Thra1PV/+ and Thra1PV/+Ncor1ΔID/ΔID mice than the respective vehicle-treated mutant mice, indicating de-repression of these 2 genes in SAHA-treated mutant mice.
Our studies show that the effectiveness of SAHA treatment is target tissue-dependent. In WAT, together with lack of recruitment of NCOR1 by TRα1PV, an HDAC inhibitor completely corrected the impaired adipogenesis. Thus, the NCOR1-HDAC repressor complex could be considered a potential therapeutic target for treatment.
Autoimmunity Thursday Oral Clinical 1:50 PM
Presence of thyroid antibodies in pregnancy, even in euthyroid women, has been associated with increased risk of abortion and preterm delivery. We investigated the prevalence of thyroid peroxidase antibodies (TPOAb) in pregnant Danish women before and after the implementation of the national iodine fortification program (IFP), and compared this to the development in preterm deliveries over the same course of time.
The study was a comparative cohort study of 1722 Danish pregnant women. In three cohorts, data was collected before (1998–2000), during (2000–2003), and after (2008) the IFP, respectively. In the first cohort (n=282) TPOAb were measured with the DYNOtest radioimmunoassay (BRAHMS, Hennigsdorf, Germany; functional assay sensitivity 30 mU/l). In cohorts 2 (n=151) and 3 (n=1273), TPOAb-levels were measured with automated Kryptor immunoflourescent assays (BRAHMS, Hennigsdorf, Germany; functional assay sensitivity 28 and 50 mU/l, respectively). Tests for trends were performed with χ2-tests. Risk of preterm delivery (gestational age at delivery <37 weeks) according to TPOAb-positivity (TPOAb>60 mU/l) was tested by binary logistic regression to adjust for the following covariates: cohort origin, gestational age at visit, maternal age, smoking status, pre-pregnancy BMIxBMI, pregnancy achieved by assisted reproductive techniques, and thyroid hormone levels (z-scores of logtransformed TSH, free T3, and free T4).
In the three cohorts, TPOAb-levels above our clinical cut-off of 60 mU/l were found in 5.4, 7.9, and 13.7% (χ2(2, n=1722)=18.65, p<0.001) of the women, respectively. However, there was no significant increase in the proportion of preterm deliveries between cohorts (χ2(2, n=1497)=2.22, p=0.33). Preterm delivery occurred in 68 out of 1496 (4.5%) pregnancies with no significant effect of antibody-status (adjusted OR=1.44, 95%CI [0.56–3.71]).
Prevalence of TPOAb in Danish pregnant women has more than doubled upon the implementation of the IFP. However, this increase has not been accompanied by a rise in the proportion of preterm deliveries. Unlike previous studies, we did not find an increased risk of preterm delivery in thyroid autoantibody-positive women.
Autoimmunity Thursday Oral Clinical 2:05 PM
IgG4 related disease (IgG4-RD) is a new clinical entity that affects various organs with increased IgG4 positive plasmacytes and progressive fibrosis. While IgG4-RDs in association with Hashimoto thyroiditis or Riedel's thyroiditis have been reported, relation between IgG4-RD and Graves' disease (GD) is yet unknown. To elucidate the relation of GD to IgG4-RD, serum IgG4 levels and their clinical implications in patients with GD were investigated.
A prospective study. One hundred nine patients with GD were subjected to the measurement of serum IgG4 concentrations and classified into two groups based on the comprehensive diagnostic criteria of IgG4-RD: 1) GD with elevated serum IgG4 concentrations (≥135 mg/dL), and 2) GD with non-elevated IgG4 (<135 mg/dL).
Seven out of 109 patients with GD (6.4%) had elevated serum IgG4 levels; mean±SD (range), 175.0±44.5 (136–266) mg/dL and elevated ratios of IgG4/IgG, 12.7±4.5 (7.6–21.2) %. The remaining of patients with GD had serum IgG4 levels and IgG4/IgG ratios of 39.6±27.6 (3–132) mg/dL and 3.2±2.2 (0.3–11.5) %, respectively. Ages of elevated-IgG4 group were significantly higher than those of non-elevated-IgG4 group; 54.7±6.2 vs. 43.4±15.4 yr., respectively. Ultrasound examinations revealed that elevated-IgG4 group had significantly increased low echogenic area in the thyroid in comparison to non-elevated-IgG4 group (low echo scoring; 1.66±0.81 vs. 0.61±0.89, respectively. In the correlation analysis, TSAb (rs=0.385, n=42) titers were significantly correlated with serum IgG4 levels, while they were not significantly different between the two groups. In elevated-IgG4 group (n=7), patients were controllable with a small dosage of anti-thyroidal drug (ATD) (n=4), a combination treatment with ATD and L-T4 (n=1) or L-T4 administration only after 1 year from the first visit (n=2).
A small portion of GD patients harbored elevated serum IgG4 levels. They were older, had manifested lower echoic area in the thyroid, and appeared to be responsive or prone to be hypothyroid after ATD treatment. Thus, the present study suggests the presence of a novel subtype of GD. Measuring serum IgG4 levels may help to distinguish this new entity and provide potential therapeutic options for GD.
Thyroid Cancer Thursday Oral Translational 2:20 PM
Next-generation sequencing (NGS) allows for massively parallel sequencing of the human genome and becomes a powerful tool for the detection of genetic alterations. We report a novel targeted NGS panel (ThyroSeq) for the detection of mutations and chromosomal rearrangements in thyroid cancer.
ThyroSeq NGS panel was designed to sequence 42 regions of 12 thyroid cancer related genes for mutations and for 28 types of gene fusions using next generation sequencing on Ion Torrent PGM (Life Technologies). The panel was validated on 228 DNA and 70 RNA samples from thyroid neoplastic and non-neoplastic samples including 208 tissue and 90 FNA samples.
Small amount of nucleic acids (5–10 ng) was sufficient for successful analysis of 99% of thyroid tissue and FNA samples using ThyroSeq NGS panel. The analytical accuracy for mutation detection was 100% with sensitivity of 3–5% of mutant alleles or fusion transcripts. ThyroSeq DNA assay identified mutations in 70% of PTC, 83% of follicular variant PTC, 78% of conventional and 39% of oncocytic follicular carcinomas, 30% of poorly differentiated carcinomas, 74% of anaplastic, and 73% medullary carcinomas. In contrast, only 6% of histologically benign thyroid nodules were positive for mutations. The most common mutations detected were BRAF and RAS followed by PIK3CA, TP53, TSHR, PTEN, GNAS, CTNNB1 and RET. ThyroSeq NGS analysis identified common gene fusions including RET/PTC1, RET/PTC3, and PAX8/PPARγ, and also rare fusion types involving RET, BRAF, NTRK1 and NTRK3 genes. The method allowed for quantitative assessment of mutant alleles, demonstrating clonal origin of BRAF and most of other mutations.
ThyroSeq NGS panel (i) allows testing for multiple mutations and gene fusions with high accuracy and sensitivity; (ii) requires small amount of DNA and RNA and can be performed in tissue and FNA samples, and (iii) provides quantitative assessment of mutant alleles and fused transcripts. ThyroSeq NGS approach detects genetic alterations in a cost effective way and can be potentially used in clinical setting.
Thyroid Development Thursday Oral Clinical 2:35 PM
Thyroid hormone (TH) is essential for myelination and formation of white matter tracts. In rodents, early TH deficiency leads to significant reductions in white matter tracts, especially the corpus callosum (CC). Traditionally, CC is known to connect regions between hemispheres while recent neuroimaging evidence has identified specific subregions that form distinct fiber tracts with different regions of the cortex. Children with congenital hypothyroidism (CH) are TH deficient during a critical stage of CC development. Therefore, we asked whether they show abnormal CC development and if these are located within specific subregions and related to initial hypothyroidism severity and neuropsychological abilities.
Studied were 83 children (mean age 12.2 yrs), 41 with CH and 42 controls matched for age, sex, and socioeconomic status with CH. CH were diagnosed via newborn screening and in optimal care. All participants underwent extensive neuropsychological testing and MRI scanning. Scans were submitted to ANALYZE and CCs were traced from the midsagittal slice and subdivided into six subregions based on Hofer & Frahm (2006). Determined were areas of subregions, five linear measurements, and five angles reflecting CC shape (see Figure 1). Results were compared between groups and by CH etiology.
CH had significantly smaller genu areas and widths than controls (p<0.007 and p<.02). Children with athyreosis had the smallest genus (p<.05). No effect of CH on CC shape was observed. Mean IQ, which was significantly lower in CH than controls (105.5 vs 115.6, p<.05), was associated with genu size in CH but not controls (p<.05). Genu area was also correlated with visual memory and spatial planning (p<.05).
Lack of TH in late gestation and early infancy leads to a specific abnormality in CC development and this may partially explain some of the specific deficits observed in CH.

CC measurements: (i) and (ii) division of midsagittal callosal slice into 6 regions based on Hofer & Frahm (2006); (iii) linear measurements: A. maximum width, B. height of genu, C. width of genu, D. height of body, E. width of splenium; (iv) angles for CC shape quantification based on Gabrielli et al (1993)
Thyroid Development Thursday Oral Clinical 2:50 PM
Normal thyroid hormone synthesis is essential for normal mental and physical development and is dependent on adequate iodine intake. During the first few months of life, infants are reliant on breastmilk and/or infant formula as their sole sources of dietary iodine. The iodine status of U.S. newborn infants has not been well-studied.
This was a cross-sectional study of 95 breastfed and/or formula-fed infants less than 3 months of age in the Boston area. Measured iodine content from infants' single spot urine samples was assessed for their associations with maternal demographic data, maternal salt and multivitamin use, maternal smoking, maternal diet, and infant type of feeding.
The overall median infant urine iodine concentration was 197.5 μg/L (range 40–897.5 μg/L). Median infant urine iodine concentrations were similar between infants who were breastfed (203.5 μg/L), formula-fed (182.5 μg/L), and both (197.8 μg/L) (p=0.88). There were no significant correlations between maternal salt use (regularly and in the past 24 hours), multivitamin use (regularly and in the past 24 hours), active and secondhand cigarette smoke exposures, infant weight, infant length, or recent ingestion of common iodine-containing foods.
Both breastfed and formula-fed infants less than 3 months of age in the Boston area are generally iodine sufficient. Larger studies are needed to determine the sources of infant iodine nutrition and confirm these observations among infants nationwide.
Thyroid Nodules & Goiter Thursday Oral Clinical 3:05 PM
Increasingly, patients with thyroid nodule cytology labeled AUS/FLUS, or FN undergo diagnostic analysis with the Afirma gene expression classifier (GEC). No long-term, multi-site analysis of Afirma GEC performance has yet been performed.
We analyzed all patients who had received Afirma GEC testing at 5 academic medical centers between 2010–2013. Nodule and patient characteristics, fine needle aspiration cytology, Afirma GEC results, and subsequent clinical or surgical follow up were obtained for 339 patients. Results were analyzed for pooled test performance, impact on clinical care, and site-to-site variation.
339 patients underwent Afirma GEC testing of cytologically indeterminate nodules (165 AUS/FLUS; 161 FN; 13 SUSP). 174 of 339 (51%) indeterminate nodules were GEC benign, while 148 GEC suspicious (44%). GEC results significantly altered care recommendations, as 4 of 175 GEC benign were recommended for surgery in comparison to 141 of 149 GEC suspicious (p<0.01). Of 121 Cyto Indeterminate/GEC Suspicious nodules surgically removed, 53 (44%) were malignant. Variability in site-to-site GEC performance was confirmed, as the proportion of GEC benign varied up to 29% (p=0.58), while the malignancy rate in nodules cytologically indeterminate/GEC suspicious varied up to 47% (p=0.11). 71 of 174 GEC benign nodules had documented long-term follow-up (mean 8.5 mo), in which 1 of 71 nodules proved cancerous.
These real-world, multicenter data confirm originally published Afirma GEC test performance, and demonstrate its substantial impact upon clinical care recommendations. Though non-significant site-to-site variation exists, such differences should be anticipated by the practicing clinician. Long-term follow-up of GEC benign nodules confirms the clinical utility of this diagnostic test.
Autoimmunity Thursday Poster Basic
BID, a pro-apoptotic Bcl-2 family member, functions as a bridge molecule between death-receptor and mitochondrial related apoptotic pathways to amplify apoptotic signaling. Our previous studies have found a substantial increase in BID expression in the primary normal thyroid epithelia cells treated with the inflammatory cytokines including the combination of IFNγ and IL-1β or IFNγ and TNFα. This increase can sensitize thyroid epithelia cells to death-receptor mediated apoptosis.
A transgenic mouse line that specifically expresses human BID in thyroid cells was established by fusing a rat thyroglobulin (Tg) promoter upstream to human BID (Tg-BID). We tested whether the increased expression of pro-apoptotic BID in thyroid would induce spontaneous autoimmune thyroiditis. In addition, those mice were given iodine water (0.3% of sodium iodide) for eight weeks.
Our data showed that both Tg-BID female and male mice in a CBA/J (H-2k) background, which was established by crossing Tg-BID positive C57BL/6J×CBA/J (H-2k) mice to CBA/J (H-2k) mice, did not spontaneously develop autoimmune thyroiditis for over a year. However, upon ingestion with iodine in drinking water, autoimmune thyroiditis developed in these female transgenic mice, evident by a significant increase in anti-thyroglobulin antibody and 30% of mice having mononuclear cell infiltration into the thyroid glands. But serum T4 levels were similar between iodine-treated and untreated groups.
Collectively, the increased BID expression in thyroids can facilitate the development of autoimmune thyroiditis induced by iodine uptake. Nevertheless, the overexpression of BID itself is not enough to initiate thyroiditis in CBA/J (H-2k) mice, which have a genetic predisposition to develop experimental autoimmune thyroiditis. These findings support the common concept that autoimmune thyroiditis is a multi-factorial disease, resulting from an interplay of genetic, environmental, and endogenous factors.
Autoimmunity Thursday Poster Clinical
Surgical, radioiodine and antithyroid drug (ATD) therapy all have their indications in the therapy of Graves' disease (GD). However, current recommendations on surgery (near total) and radioiodine (near ablation) restrict the hope of returning to normal thyroid physiology with no medication to patients that enter remission during a course of ATD. A main obstacle to sustained cure in such patients is the tendency to relapse after stop of ATD.
RISG is a multiphase two center Danish prospective study aiming to promote better targeting of ATD therapy in individual patients. The results of the observational (up to 24 months(m)) protocol RISG1 with titration ATD to GD remission (TRAb negative with normal TSH for 2 m on <5 mg Methimazole (MMI)/d) are reported. In addition an interim status on RISG2, a subsequent 24 m prospective randomized study of no therapy vs continuous low dose MMI, will be given. 208 newly diagnosed GD patients (Aalborg/Copenhagen n=167/41, F/M 176/32, age 45 (35–53) yrs (median (25–75% range)), T3 5.40 (4.22–7.08), T4 210 (175–255) nM were included. TRAb at inclusion was 9.1 (5.2–15.0) IU/L; thyroid volume 20.0 (14.5–31.9) ml; smokers 26.9%, eye signs 29.8%. Initial dose of MMI (20 (15–30) mg/d) was gradually reduced based on standardized thyroid function testing.
173 patients (83.2%) completed the study protocol to remission or for 2 yrs. Frequencies of having entered remission after 12, 18, 24 m of ATD were 24.3/43.4/53.2%. Predictors (p<0.05) at time of diagnosis of NOT being in remission at 24 m in univariate logistic regression analyses were: Age <45 y (OR 2.26); BMI>25 (OR 0.52); eye signs (OR 1.99); T4>240 nM (OR 2.5); TRAb 5–12 IU/L (OR 3.4); TRAb>12 (OR 6.9); thyroid vol >40 ml (OR 3.0); but sex, smoking, previous hyperthyroidism, GD in family, estrogen use, region of living, and TPO-Ab were not. In a multivariate model including the significant predictors, only age <45 y, eye signs, and high TRAb remained significant independent predictors.
Many GD patients are not in remission after recommended standard ATD of 12–18 m duration. A more individual approach with longer therapy of especially patients with young age, orbitopathy, and high TRAb may be warranted.
Autoimmunity Thursday Poster Clinical
Previous data demonstrate that thyrocytes (TFC) secrete CXC chemokines, particularly CXCL8 and CXCL10. The physiopathological significance of such secretion and the effects of a combination of proinflammatory stimuli in terms of preferential CXCL8 and CXCL10 release is unclear.
We study the modulation of the secretion of CXCL8 vs. CXCL10 by TFC in Graves' disease (GD), and in primary fibroblasts (OF) or preadipocytes (OP) from Graves' ophtalmopathy (GO).
CXCL8 and CXCL10 were measured in supernatants of TFC, OF or OP cells basally and after 24 h stimulation with IFNg (1000 IU/ml) and/or TNFa (10 ng/ml). CXCL8, not CXCL10, was detected in basal conditions in TFC, OF and OP. CXCL10 secretion was significantly induced by IFNg (P<0.01) but not TNFa, whereas CXCL8 was secreted in response to TNFa (P<0.01), inhibited by IFNg (P<0.01), in TFC, OF and OP. TNFa+IFNg synergistically increased the IFNg-induced CXCL10 secretion (P<0.01) and reversed the TNFa-induced CXCL8 secretion (P<0.01), in TFC, OF and OP.
In conclusion, we first show that TFC, OF and OP secrete CXC chemokines. CXCL8 and CXCL10 secretion is differentially sustained by specific proinflammatory cytokines or their combination, which ultimately determines the nature of the infiltrating lymphocytes in human GD and GO.
Withdrawn
Withdrawn
Disorders of Thyroid Function Thursday Poster Translational
Despite early optimal care, children with congenital hypothyroidism (CH) show persisting cognitive impairments. Commonly observed are weak memory functions on tasks of spatial and verbal associative recall that rely on an intact hippocampus. Using MRI, we previously reported children with CH show reduced hippocampal size and atypical functioning for recalling associations and places. Another major critical hippocampal function is the recall of past personal events or autobiographical memory (AM), which is impoverished in children with CH (Willoughby et al, 2013). However, the relation between AM and atypical hippocampal structure and function is not known. Thus the current study sought to evaluate AM relative to hippocampal size and function in children with CH.
Participants were 58 9–14 years olds, 26 with CH diagnosed via newborn screening who received optimal care and 32 age-matched controls. All were assessed with the Children's Autobiographical Interview (CAI) requiring them to describe two past personal events and structural MRI scans from which traced hippocampal volumes were determined. One year later, a subset (7 CH, 19 controls) underwent fMRI with a paradigm requiring them to judge the validity of statements about past personal events (episodic) or personal facts (semantic). Critical contrast was the different signal strength between episodic and semantic statements.
On CAI, CH recalled fewer episodic but not semantic details than controls, suggesting impoverished memories. CH also had smaller left hippocampal volumes than controls. However episodic details and hippocampal size were not correlated (all ps>0.05). On fMRI, both groups indicated bilateral hippocampal activation, which was significantly stronger on the left in CH than controls. CH also activated the entorhinal cortex (ERC) region to a greater degree than controls (p<0.01). Higher TSH at diagnosis predicted increased ERC activity in CH.

Increased Hippocampal Activation for CH versus Controls on Personal Episodic Minus Personal Semantic Contrast
Children with CH show abnormal hippocampal engagement and increased ERC engagement in remembering past personal events, signifying early TH insufficiency leads to functional disorganization of the personal memory system. Thus despite early optimal care, brain development may still be compromised in CH.
Disorders of Thyroid Function Thursday Poster Clinical
Our objective was to compare the performance of liquid chromatography tandem mass spectrometry (MS) versus immunoassay (IA) for measuring thyroid hormones in a diverse group of inpatients and outpatients, some of whose blood samples would provide the types of problems which challenge the performance of IA, such as binding protein abnormalities.
100 patients gave a single blood sample for the study. Their inpatient or outpatient status was documented. The blood samples were assayed for thyroxine (T4), triiodothyronine (T3), free thyroxine (FT4), and free triiodothyronine (FT3) measured by MS. At the same time T4, T3, FT4, and FT3 were measured by IA. IA reference intervals from the manufacturer were confirmed in-house, and MS reference intervals were based on a population of 1700 adults and children.
Although T4 and T3 values measured by the two different assays correlated reasonably with each other, the correlation was best in the mid-range of hormone values and was quite poor at the extremes. This was particularly notable for T3 at the lower end of the range. 13% of T3 values measured by IA were below the 2.5th percentile, which contrasted with 47% of values measured by MS. For T4 measurements 3% of values measured by IA were below the 2.5th percentile, which contrasted with 9% of values measured by MS. FT4 and FT3 values measured by the two assays did not correlate well with each other. In addition, 12% of the FT4 values measured by MS were above the 97.5th percentile, compared with 25% by IA. For FT3 values measured by MS, 1% were above the 97.5th percentile, compared with 6% by IA. FT4 assays also performed differently at the lower end of the range, with 4% of FT4 values measured by IA falling below 2.5th percentile, which contrasted with 29% of values measured by MS.
The greatest discrepancy between these two assays is thus demonstrated at low and high extremes of hormone concentrations, in the concentration ranges where accurate assay performance is most clinically important. Based on the lesser susceptibility of MS to interferences from conditions such as binding protein abnormalities, it is suggested that MS is representative of the clinical situation.
Disorders of Thyroid Function Thursday Poster Clinical
Adequate maternal iodine intake is critical for fetal neurodevelopment. Perchlorate (ClO4) and thiocyanate (SCN) decrease thyroidal iodine uptake by competitively inhibiting the sodium/iodide symporter (NIS). There are conflicting data on whether ClO4 and SCN exposure affects thyroid function. In Thailand, where iodine intake is sufficient, it is unclear whether environmental exposure to ClO4 and/or SCN adversely affects thyroid function during early pregnancy. The present study was carried out to determine the effects of environmental ClO4 and/or SCN exposure on thyroid function in first trimester pregnant Thai women.
Two hundred pregnant Thai women with a gestational age less than 14 weeks were studied. Urinary ClO4, SCN, iodine and serum thyroid function tests were measured. Data are expressed as mean±SD.
The women were aged 28.6±6.1 years and the mean gestational age at the time of sampling was 9.6±2.7 weeks. Median (range) urinary iodine concentrations were 153.5 μg/L (50–1,219 μg/L). Urinary ClO4 and SCN levels were detectable in all women (median 1.9 μg/L, range 0.1–35.5 μg/L and median 510.5 μg/L, range 68–3,525 μg/L, respectively). Using Spearman's rank correlation analyses, there was no association between serum free thyroxine (FT4) and urine ClO4 (r−0.07, p=0.26) or between serum TSH and urine ClO4 (r 0.09, p=0.17). In multivariate analyses adjusted for log urine iodine, log urine SCN, log urine creatinine and gestational age, log urine ClO4 was positively associated with log serum TSH (p=0.006) and inversely associated with log serum FT4 (p=0.003). In the multivariable models, log SCN was not a significant predictor of thyroid function.
Low-level ClO4 and SCN exposure is common in Thailand, where iodine intake is adequate. In adjusted models, low-level ClO4 exposure was significantly associated with increased serum TSH and decreased serum FT4 in first-trimester pregnant Thai women, although serum TSH and FT4 were almost all within the trimester-specific normal range. These data are in conflict with our previous findings in pregnant cohorts. More studies are needed to understand these effects.
Disorders of Thyroid Function Thursday Poster Clinical
The use of Armour Thyroid (desiccated thyroid) in the treatment of hypothyroidism has generated considerable debate. Recent studies have demonstrated both a patient preference for replacement regimes which include T3 as well as providing a scientific basis for potential benefits of combination T4 and T3 treatment in a subgroup of hypothyroid individuals with resistant disease symptoms. Biochemical and clinical data is presented here from a retrospective analysis of 153 consecutive patients with persistent symptoms of hypothyroidism on T4-only treatment who were switched to Armour Thyroid (AT).
450 consecutive patients being treated for hypothyroidism within a single endocrinology practice were screened. Of these, 153 had previously been switched from either generic or brand T4 replacement to AT for treatment of persistent symptoms of hypothyroidism. Total T4, total T3, and TSH levels on T4-only and during AT treatment were analyzed. Patients were asked to compare AT treatment versus T4-only treatment using a 5 point satisfaction rating scale. Results are reported as mean±SD.
On a 5 points scale, with “5” corresponding to AT “definitely superior” to prior T4-only treatment and “1” corresponding to AT “definitely worse” the reported score was 4.3±1.0, P<0.001. 113 patients gave a score of greater than “3”. Two patients reported adverse events on AT, none serious. T4 to T3 ratio on T4-only was 7.9±3.81 while it was 4.7±1.97 (p<0.001) on AT. TSH was 1.30±1.9 μIU/mL and T3 1.21±0.56 ng/mL on T4-only while TSH 1.27±2.2 μIU/mL and T3 1.49±0.87 ng/mL on AT (NS for TSH and p<0.003 for T3). There was no significant correlation between TSH and satisfaction rating.
AT treatment was highly efficacious for improving symptoms of hypothyroidism in a sub-group of patients resistant to T4-only therapy. TSH levels were comparable on T4-only and AT therapies indicative of similar intensities of thyroid hormone replacement between replacement regimes.
Disorders of Thyroid Function Thursday Poster Clinical
Iodine and selenium are essential elements in thyroid hormone synthesis. Iodine is incorporated into thyroid hormones, while selenium is a key component at the catalytic site of several selenoproteins involved in protecting the thyroid gland from free radicals produced during thyroid hormone synthesis, and in peripheral tissue conversion of thyroxine to triiodothyronine. Bromine and arsenic are antagonists of thyroid hormone synthesis: as the former competes with iodine in the thyroid, while the latter forms a tight complex with selenium, preventing its incorporation into selenoproteins. To better understand the interplay of bromine on iodine and arsenic on selenium, we developed a new method to measure these four elements in urine dried on filter paper.
Twenty five volunteers collected four spot urine samples on Ahlstrom grade 226 filter paper (morning, lunch, afternoon and night) during a 24-hour period. Liquid standards, calibrators, blanks and urine samples were dried on filter paper, punched into a 96-well filter block and extracted with ammonium hydroxide containing germanium as an internal standard. The extract was then simultaneously analyzed for iodine, bromine, selenium and arsenic using inductively coupled dynamic reaction cell mass spectrometry (ICP-DRC-MS). Remaining extract was further analyzed for creatinine in a 96-well format using a modified version of Jaffe's reaction to correct for hydration status. After creatinine correction, we compared the average of all four spot urine collections to averaged morning and night spot urine collections.

Detection limits, recoveries, inter- and intra-assay variations, and linearities were acceptable for each analyte. Accuracy was validated using certified reference materials. Urine dried on filter paper is stable for at least a month at room temperature, allowing for convenient shipment and storage. The average of four spot urine collections correlated well with the average of morning and night spot urine collections.
The method described is ideal for large population studies and clinical testing investigating the role of iodine, selenium and their antagonists, bromine and arsenic, in thyroid hormone synthesis and function.
Disorders of Thyroid Function Thursday Poster Clinical
The purpose of this study was to evaluate the incidence and predisposing factors of postoperative hypothyroidism after hemithyroidectomy
We analyzed 91 patients who underwent hemithyroidectomy between October 2008 and January 2009. The definitions of euthyroid and subclinical hypothyroid (hypothyroidism) were based on TSH laboratory data
Postoperative hypothyroidism was diagnosed in 25 (27.5%) of 91 patients with a mean postoperative TSH level of 8.55 (5.2–18.2) μU/ml. The mean of last follow up duration was 18.94 months. The preoperative TSH had relationship with postoperative hypothyroidism with significant cut-off value at higher than 3.0 μU/ml and (p<0.05). Among 25 patients, 12 (46.0%) had preoperative TSH higher than 3.0 μU/ml. The overall mean TSH of immediate postoperative and the last were 6.34 and 3.99 μU/ml, respectively.
Even though the immediate postoperative TSH seems higher than the normal range, the last showed mean TSH below 5.0 μU/ml. These findings indicate that TSH should be followed for long-tem duration before the diagnosis of postoperative hypothyroidism. Also, within the patients having preoperative TSH higher than 3.0 μU/ml, half of them should be considered to develop postoperative hypothyroidism.
Disorders of Thyroid Function Thursday Poster Clinical
To determine the necessary dose of levothyroxine in different types of hypothyroidism, time since the diagnosis, and the initial level of TSH in primary hypothyroidism.
Retrospective cohort study in patients over 14 yo, normal TSH range for at least 2 consecutive measures 3 months since the primary hypothyroidism diagnosis, and normal free T4 for central hypothyroidism.
518 patients met the inclusion criteria of which 90% were women. Overall, 50.9% had primary hypothyroidism with TPO unknown o negative in clinical history, 15.4% positive TPO, 13.1% total thyroidectomy, 6.1% hemithyroidectomy, 5.9% central hypothyroidism, 5.7% post radioactive iodine, and 2.5%. post thyroiditis. The necessary dose of levothyroxine (μg/kg/d) to get a normal TSH o free t4 in central form was 1,03±0,46, 1,21±0,54, 1,65±0,46, 1,11±0,52, 1,33±0,6, 1,51±0,58 and 1,11±0,72 respectively. In patients with primary hypothyrodism, with initial TSH of less than 10 and less than 2 years since the diagnosis the requirement was 0.65±0,33 μg/kg/d, when the initial TSH was more than 20: 1,34±0,68 μg/kg/d. (p<0,001). There was a progressive increment in the needed dose of levothyroxine proportional to the years since diagnosis: less than 2 years since diagnosis: 0,77±0,38, between 2 to 5: 0,90±0,40, and more than 5 years: 1,07±0,48 μg/kg/d (p<0,001)
The necessary dose of levothyroxine to achieve a normal TSH level is variable and depends of the type of hypothyroidism, initial TSH level, and time lapsed since diagnosis. The initial dose in mild hypothyroidism is less than the usual recommended dose in overt hypothyroidism.
Disorders of Thyroid Function Thursday Poster Clinical
Case of a 29 y/o female patient status post C/S of twins at 38 weeks of gestational age who comes to ER presenting with vaginal bleeding, palpitations, headaches, tremors, shortness of breath and fever of 5 weeks evolution. Further inquiry revealed that she had been bleeding per vagina for more than a month and that she had to be admitted for PRBC's transfusions due to symptomatic anemia secondary to vaginal bleeding that started 3 days after delivery. On that admission dilatation and curettage done due to suspected retained placental tissue and discharged after hemoglobin levels stabilized. She had no other history of note.
At our evaluation patient found with unstable vitals signs. She also presented with respiratory distress, icteric sclera, hyperreflexia, bilateral lung crackles and a palpable hard uterus just below umbilical line.
Pertinent labs included TSH<0.002 mIU/dL, elevated free T4 levels 4.5 ng/dL, Hbg levels 9.3 g/dL (stable), total bilirubin 4.89 mg/dL and tumor marker HCG 161, 412,000 mIU/ml. Pathology report of D/C showed trophoblastic tissue with necrotic material consistent with a choriocarcinoma. CT scan showed large enhancing pelvic mass of 10×14×15 cm representing the suspected choriocarcinoma with extensive pulmonary metastatic burden, no evidence of pleural effusions. Due to her clinical presentation, Thyroid Storm suspected with a Burch and Wartofsky Criteria >55. She was started rapidly on antithyroid medications, B-Blockers, Steroids, IV fluids and Lugol's solution. After a day on this therapy clinical status markedly improved. Hematology-Oncology services consulted and patient started on chemotherapy with EMACO (etoposide, methotrexate, actinomycin D, cyclosphosphamide and vincristine). After few days on chemotherapy patient now with normal thyroid hormones levels and normal HCG levels. Antithyroid meds already discontinued.

Choriocarcinoma
This case represented a rare cause of thyrotoxicosis secondary to a metastatic choriocarcinoma. The malignant choriocarcinoma, occurs in 1 in 70,000 pregnancies and only 2% have clinical hyperthyroidism. It is important to include trophoblastic tumors in the differential diagnosis of thyrotoxicosis to avoid untoward consequences and provide rapid treatment.
Iodine Uptake & Metabolism Thursday Poster Basic
Whilst radioiodine ablation is an effective therapy for many patients with thyroid cancer, a subset of patients are incapable of accumulating the amount of iodide-131 required for treatment, due to low sodium iodide symporter (NIS) activity. Previous work has identified that the overexpression of pituitary tumor transforming gene (PTTG) binding factor (PBF) in thyroid cells leads to the redistribution of NIS from the plasma membrane into intracellular vesicles, thereby reducing radioiodine uptake. With radioiodine being proposed as a potential treatment for breast carcinomas, where PBF has been reported to be overexpressed, it is important to discern the relationship between PBF and NIS in breast cancer cell-lines.
Immunofluorescent microscopy was used to image MCF-7 and T47D cells to evaluate subcellular localisation of transfected NIS-MYC and PBF-HA. NIS activity was assessed in MCF-7 and MDA-MB-231 cells by measuring the uptake of Iodine-125.
Immunofluorescent microscopy revealed co-localisation between NIS and PBF in transfected MCF-7 and T47D cells, with increased intracellular staining for NIS compared to cells transfected with NIS alone. We have recently identified PBF as a tyrosine phosphorylated protein, with phosphorylation at residue Y174 critical to NIS regulation in thyroid cells. Importantly, phosphorylated PBF co-localised at the plasma membrane with NIS in T47D breast cells. In preliminary functional studies MCF-7 cells, PBF repressed radioiodine uptake in cells that had been transfected with NIS (Fold change=0.12), as well as those treated with the NIS-inducing reagents all-trans retinoic acid (ATRA) and dexamethasone (Fold Change=0.38). PBF also significantly repressed iodide uptake in MDA-MB-231 cells transfected with NIS (fold change=0.75, p<0.05).
Taken together, these data suggest that PBF can alter the subcellular location of NIS and thereby reduce the ability of breast carcinoma cell-lines to take up iodide, consistent with those findings previously reported in thyroid cells.
Iodine Uptake & Metabolism Thursday Poster Clinical
To fight obesity, low carbohydrate diets are popular. In the Paleolithic type diet (PD) (stone age diet) two of the largest iodine sources, table salt and dairy products, are excluded and the risk of iodine deficiency (ID) is evident. This study aimed for the first time to evaluate iodine status in subjects on PD compared to subjects on a diet according to the Nordic nutrition recommendations (NNR).
This is a two-year prospective randomised trial in healthy postmenopausal overweight women that were recruited for a dietary weight reduction program and were randomized to either PD (n=35) or NNR (n=35) diets. Median 24-hour urinary iodine concentration (24-UIC), 24-hour urinary iodine excretion (24-UIE) during three days and thyroid hormone levels were evaluated at baseline and after 6- and 24 months. The urine sampling was monitored by para-aminobenzoic acid (PABA), the salt intake by urinary sodium (U-Na) and dietary habits were registered.
From similar baseline levels (24-UIC 72 μg/L, 24-UIE 134 μg/L), the levels decreased after 6 months in PD group to 36 μg/L (p<0.001) and 77 μg (p<0.001) in 24-UIC and 24-UIE, respectively, whereas levels in the NNR group were held constant. The median TSH at 24 months was higher than at baseline in both groups, p<0.05. FT3 decreased in the PD group after 6 months and was lower than on the NNR diet p<0.05.

24-hour urinary iodine excretion (24-UIE) at baseline, 6 and 24 months after intervention with a paleolithic diet (PD) or a diet according to Nordic nutrition recommendations (NNR).
A paleolithic diet for two years resulted in iodine levels in accordance with mild to moderate ID and iodine supplementation is recommended.
Thyroid Cancer Thursday Poster Basic
Whilst the majority of differentiated thyroid cancers (DTC) have oncogenic mutations, a significant minority may be driven by the over-expression of proto-oncogenes. PTTG and PBF are proto-oncogenes which are induced in DTC, elicit tumours in xenograft models and interact in vitro, where PBF shuttles PTTG into the nucleus. However, the relative contributions of each gene to DTC has not been delineated.
We constructed a bi-transgenic murine model over-expressing both PBF and PTTG specifically in the thyroid gland, and characterised it in comparison to age and sex matched single transgenic (PTTG-Tg, PBF-Tg) and wild-type (WT) mice. A total of 68 WT, 98 PBF-Tg, 25 PTTG-Tg and 23 bi-transgenic mice were assessed.
No significant difference in thyroid weight was observed between male and female mice within each of the 4 genotypes. However, there was a significant 2.7-fold increase in thyroid weight in bi-transgenic mice compared to WT (p<0.001) at 6 weeks of age. PBF-Tg thyroid weight was 1.7-fold higher than WT mice (p<0.001), whereas PTTG thyroid weights were similar to WT (0.95-fold; p=0.18). Interestingly, bi-transgenic thyroids were 1.6-fold heavier than PBF-Tg thyroids (p<0.001). Enlarged thyroid growth in bi-transgenic mice was accompanied by significant hyperplasia and macrofollicular lesions. As oncogenic expression of PTTG is known to induce genetic instability (GI), we determined GI levels through FISSR-PCR in primary thyroid cultures of each genotype. Compared with WT (arbitrary GI Index=0%), PBF-Tg mice had a GI Index of 19.8±1.8%; PTTG-Tg mice of 7.6±1.6%; and bi-transgenic mice of 37.9±2.7%. Examination of a panel of 83 DNA repair genes to understand which genetic changes might underlie these differences showed that expression of 9 genes were significantly down-regulated >1.5-fold in bi-transgenic thyrocytes compared to PBF-Tg, including Gadd45a (2.3-fold, p=0.006), Brca1 (2.1-fold, p=0.003) and Chek1 (2.4-fold, p=0.01).
Together, our data reveal a complex interplay between PTTG and PBF in vivo; the bi-transgenic thyroid phenotype is closer to that of PBF-Tg mice than PTTG-Tg mice, but reveals increased goitre size, and heightened genetic instability than either single transgenic model alone.
Thyroid Cancer Thursday Poster Basic
The antitumoral activity of two new “pyrazolo[3,4-d]pyrimidine” compounds (CLM29 and CLM24), which inhibit several targets (including EGFR, VEGFR and the RET tyrosine kinase and have an anti-angiogenic effect), have been studied in primary anaplastic thyroid cancer (ATC) cells.
We tested the antiproliferative effect of these new compounds in ATC cells obtained from patients with recurrence of the tumor at the time of reoperation. In the in vitro experiments different concentrations of CLM29 and CLM24 (1, 10, 30, 50 μM) were used.
After treatment with CLM29, proliferation assays in ATC cells showed a significant reduction of proliferation, respect to the control (expressed as 100%), that was by 80% with CLM29 5 μM, 50% with CLM29 10 μM, and 32% with CLM29 50 μM. In ATC cells CLM24 also induced a slight but significant reduction of proliferation that was 97% with 30 μM, and 78% with 50 μM. The percentage of apoptotic cells in in vitro experiments with ATC cells was increased by CLM29 and CLM24, dose-dependently (p<0.001). In 3/9 of ATCs used for in vitro experiments the V600EBRAF mutation was observed. The results obtained about the inhibition of proliferation by CLM29 and CLM24 in ATC from tumors with V600EBRAF were similar to those from tumors without BRAF mutation. CLM29 inhibited migration (p<0.001) and invasion (p<0.001) of ATC cells, while CLM24 had no significant effect.
In conclusion, the antitumoral activity of these two new “pyrazolo[3,4-d]pyrimidine” compounds (CLM29, CLM24) in in vitro experiments in ATC has been shown, independently from the presence of the BRAF mutation, opening the way to a future clinical evaluation.
Thyroid Cancer Thursday Poster Basic
Metastasis is a multistep process responsible for the vast majority of endocrine cancer cell deaths. The initial stage of metastasis involves the invasion of tumour cells into the adjacent tissue. We have previously identified PBF to be upregulated in differentiated thyroid cancer, and recently PBF expression has been correlated with distant thyroid cancer metastasis at diagnosis. Further, PBF potently induces breast cancer cell invasion in vitro and our recent in vivo data demonstrate that colorectal tumours with higher PBF protein expression demonstrate increased vascular invasion.
Boyden chamber invasion assays were used to determine if PBF regulates thyroid cell invasion. To gain insight into the pathway in which PBF induces cell invasion we used two different approaches. 1) IP-MS was employed to discover PBF binding partners. 2) As epithelial cells undergo an epithelial to mesenchymal transition (EMT) to facilitate invasion we performed focused SABiosciences cDNA arrays housing 84 genes of central importance to EMT.
We now show that PBF significantly promotes thyroid cell invasion in vitro in SW1736 cells (1.3-fold compared to vector only (VO), P<0.01). Further, our IP-MS approach identified the cortical actin binding protein, cortactin, as an interacting partner of PBF. This interaction was confirmed using co-immunoprecipitation assays, which also found that mutation of residue F at position 177 to A within the C-terminal sorting signal of PBF disrupts this interaction. Cortactin has a central role in invasion as it promotes cell migration; we therefore examined whether the interaction between cortactin and PBF controls cell migration. Wound healing assays in MDA-MB-231 cells revealed that GFP-tagged PBF cells migrated significantly further than GFP-VO cells (VO=115.3 μm, PBF=143.0 μm, P<0.01). Finally, cDNA arrays revealed that PBF significantly regulates four genes (DSP, JAG1, PDGFRB and TCF3) of central importance to EMT in SW1736 thyroid cancer cells (P<0.05).
Taken together these data suggest that PBF may promote thyroid cell invasion by 2 independent mechanisms; 1) PBF binds to cortactin and regulates migration, and 2) PBF regulates the expression of genes involved in EMT.
Thyroid Cancer Thursday Poster Basic
Mutations in BRAF kinase are widely observed in PTC and activate downstream kinases along the MAPK pathway, resulting in functional dependence upon this cascade. While many patients respond to treatment with the BRAF inhibitor vemurafenib, responses are incomplete and patients inevitably progress. The mechanism of acquired resistance is not completely understood, nor is it clear which drug should be started after progression. The 3:1 (female:male) gender disparity and prevalence of PTC in women of childbearing age suggest estrogen receptors, ERα and GPR30, as potential facilitators in this resistance. Moreover, EGFR is a putative target of GPR30 and its increased activation has been correlated with increased BRAF inhibitor resistance in colon cancer. This study begins to investigate whether activated estrogen receptors potentiate/induce acquired resistance to inhibitors of mutated BRAF through adaptations in cell surface receptor tyrosine kinases and the MAPK and PI3-K pathways, as well as the role of estrogen receptors in the observed gender disparity.
Western blots were used to analyze receptor expression in cell lines were treated with 2μM vemurafenib and/or 10 nM Estradiol. Tissue arrays were imaged and analyzed for receptor expression using a Vectra automated multispectral imaging system.
Our data show that ERα and GPR30 are indeed expressed in the PTC cell line BCPAP, which harbors the BRAF V600E mutation, and were both significantly upregulated in PTC lymph node metastasis tissue cores compared to normal thyroid tissue. Although ERα levels were relatively lower in the BCPAP line than the highly aggressive breast cancer cell line MCF7, levels of EGFR and GPR30 were five and fifteen times higher in BCPAP cells, respectively. Estradiol has been shown to increase proliferative and metastatic phenotypes in this PTC line. Our experiments show increased levels of activated AKT and MAPK, as well as EGFR in BCPAP cells following estrogen treatment.
These results indicate the potential for activated estrogen receptors to promote acquired resistance to BRAF inhibitors. Further study of this potential and the molecular mechanism behind the activation of the MAPK and PI3-K via ERα, GPR30, and EGFR is warranted.
Thyroid Cancer Thursday Poster Basic
Thyroglobulin (Tg), is mandatory to monitor efficacy of thyroid gland surgical and Radio-Iodine ablation in patients with Differentiated Thyroid Cancer (DTC). Successful treatment (by removing the unique source of Tg) is currently assessed by undetectable Tg in the serum. The aim of our study was to evaluate the analytical and clinical performances of the new sensitive Tg seric immuno-assay developed on Kryptor Compact Plus instrument (Thermo Fisher Scientific).
Kryptor hTg sensitive assay is using TRACE methodology (Time-Resolved Amplified Cryptate Emission), with 3 anti-Tg monoclonal antibodies labeled with Lumi4 (cryptate of Terbium) and one anti-Tg polyclonal antibody labeled with Cyanin5.5, allowing the detection of each fluorophore separately or associated in the same antigen-antibody complex.
Analytical performances of Kryptor hTg sensitive assay showed total coefficients of variation (CV) of 8% and 5% for Tg levels of 0.97 μg/L and 54.7 μg/L respectively and a Functional Assay Sensitivity (FAS) of 0.14 μg/L Tg. Kryptor hTg sensitive assay was compared to Access 2nd generation Tg (Beckman) in 131 samples from 97 patients with DTC, either on LT4 treatment (n=69 samples) or under TSH stimulation (n=62 samples). The Tg levels varied from undetectable to 363 μg/L and to 370 μg/L on Kryptor and Access respectively. The regression equation in the direct measuring range was y=0.84x+0.07, where y and x are the Tg levels measured on Kryptor and Access respectively. With a cut-off corresponding to the FAS of each assay for patients under LT4 treatment (i.e. 0.14 μg/L for Kryptor and 0.1 μg/L for Access), and a cut-off of 1μg/L Tg for patients under TSH stimulation, the percentage of concordant results was 87%. To the exception of one patient with an unusual Tg response to TSH stimulation, the discrepant results (n=17), i.e. Tg higher than the cut-off by one method and lower than the cut-off by the other method, showed Tg levels slightly elevated over the cut-off.
In conclusion, Kryptor hTg sensitive assay is suitable for the follow-up of patients with DTC as all the results in DTC patients (except in one) were either correctly classified or slightly above the cut-off value whatever the method.
Thyroid Cancer Thursday Poster Basic
Smoking is a major risk factor for cancer development and is strongly related to 90% of lung cancers. In contrast, epidemiological studies demonstrate that cigarette smoking is associated with reduced risk of thyroid cancer. It has been demonstrated that cigarette tobacco smoke metabolites cause cell injury and dysfunction by enhancing oxidative stress and inflammation. We hypothesize that thyroid and lung carcinoma cell growth and proliferation are differentially stimulated by metabolites from cigarette smoking.
Primary cell cultures from papillary thyroid cancer, adjacent normal thyroid tissue (from the same patient), lung adenocarcinoma and adjacent normal lung tissue (from the same patient) were incubated in conditioned F-medium with Y compound (ROCK inhibitor) using the “Georgetown Method”. All cells were incubated with 1% human serum obtained from a smoker (SMK), a second hand smoker (SHS), and a non-smoker (non-SMK) for 24, 48, and 96 hours, respectively. Images of cells were taken and cell numbers were counted at each time interval. The study was repeated using different subjects at each round. Smoking levels were detected using serum cotinine as a biomarker for smoke exposure measured by tandem mass spectrometry (LC/MS/MS).
Thyroid cancer cells did not demonstrate a dose response to the different serum, but did grow less in the presence of serum from SMK and SHS relative to non-SMK. Normal thyroid cells had the highest cell proliferation when incubated with serum from non-SMK and the least with serum from SMK. In comparison, a dramatic increase in lung cancer proliferation, of 300%-700% was detected when cells were incubated in the presence of serum from SMK. A dose response pattern was noted in the presence of serum from SHS vs. serum from non-SMK. Further, normal lung cells did not show differential response in the presence of each of the serum types.
This study demonstrates that smoking is not associated with thyroid cancer cell growth and is associated in a dose response manner with lung cancer cell proliferation. The different effects of cigarette smoking on lung and thyroid cells growth imply that smoking metabolites play distinct roles in the development of these two types of cancer.
Thyroid Cancer Thursday Poster Translational
Detectable circulating tumor cells (CTCs) have been associated with poor prognosis in breast, colon and prostate cancers. We have previously reported that ≥5 CTCs per tube can be detected using the Veridex CellSearch system in blood from a subset of patients with metastatic medullary thyroid carcinoma (metMTC) (Michaelis et al EndoSoc 2010). We now evaluate whether elevated CTCs are associated with worse survival in metMTC.
Two CellSave tubes of whole blood were obtained from 18 subjects (M:F 9:9) with metMTC. CTCs were enumerated by the CellSearch system, which identifies CTCs by immunomagnetic cell selection using EpCAM as a capture antigen, followed by fluorescent immunolabeling for detection of epithelial-derived cells that stain positive for cytokeratin and DAPI and negative for the lymphocyte marker CD45. Captured cells are visually confirmed and counted by microscope.
Mean age at diagnosis was 43 yrs and at sampling was 52 yrs; log mean and median calcitonin were 3918 and 3240 ng/mL, respectively. Metastatic disease was noted in liver, lungs, and bones in 89%, 72% and 67% of patients, respectively. 8 patients were being treated with TKI therapies, and another 7 had undergone previous treatment. 6/18 patients had ≥5 CTCs per tube detected by CellSearch. With a median follow-up of 24.5 months after sampling, 9 patients had died, including 5/6 of those with ≥5 CTCs per tube compared with 4/12 for those with <5 CTCs. Calcitonin doubling times did not significantly differ between those who died and those alive at last follow-up. Median survival was 13 months for those with ≥5 CTCs, and had not been reached for those with <5 CTCs. Kaplan-Meier analysis demonstrated significantly shorter survival for those with ≥5 CTCs (Fig 1; P=0.024). The hazard ratio for mortality of patients with ≥5 CTCs compared with <5 CTCs was 4.05 (P=0.042).
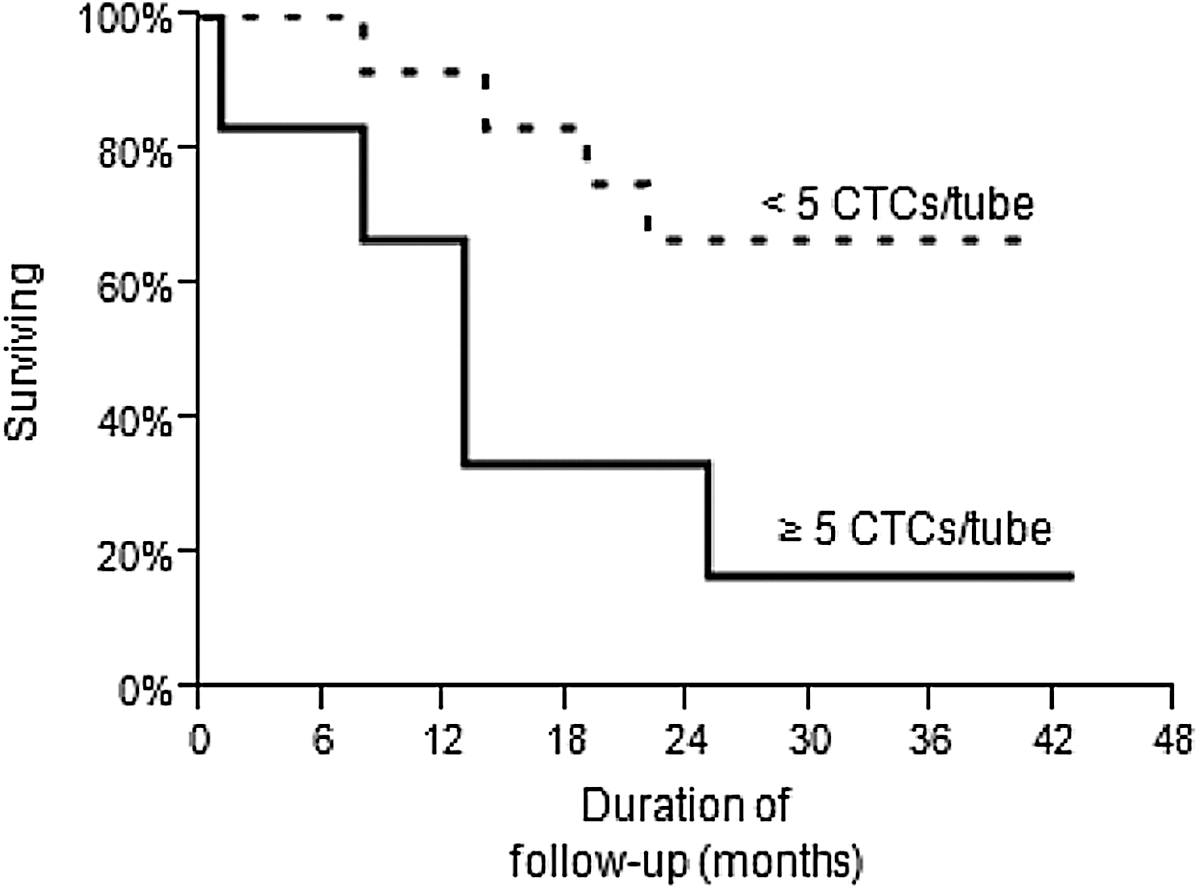
The presence of ≥5 CTCs per tube detected by CellSearch in a single blood specimen from patients with metMTC is associated with worse survival and may be more predictive than calcitonin doubling time. Larger cohorts are required to validate this observation, and to determine if sequential changes in CTCs are predictive of outcomes with subsequent treatment.
Thyroid Cancer Thursday Poster Translational
An impact of CTL on PTC outcome has been long advocated but this matter is still controversial. Moreover, there is increasing evidence that the balance between the cytotoxic and the regulatory components of the lymphocytic infiltration (LI) may affect the tumor-specific immune response. The purpose of this study was to evaluate the prognostic value of CTL in a retrospective cohort of PTC patients and to characterize the LI and the lymphocytic subpopulations.
We assessed 375 PTC patients, aged 45.2±16.4 years, treated with thyroidectomy and radioiodine remnant ablation, with a mean follow-up of 6.28±3.86 years. In a subgroup of patients (n=100), tissue sections were reviewed for the presence of CTL and lymphocytes within and/or surrounding tumor (TAL); lymphocytic subsets were characterized by immunohistochemistry.
Seventy-five/375 patients (20%) had a histological diagnosis of CLT and were more frequently women (90.7% vs 69.7, p=<0.001) with a tendency to be low risk (according to ATA criteria) compared to those with no CTL. At the last follow-up, PTC patients with CTL showed a significantly better outcome compared to those with no CTL, even considering only female patients (cure rate: 92.4% vs 79.3%, p=0.009), low (cure rate: 100% vs 89.8%, p=0.039) or high risk patients (cure rate: 82.9% vs 66.3%, p=0.043). Data from LI characterization are available for 43/100 patients: PTC patients with CTL (n=14) compared to those with TAL (n=21) tend to have more often tumors with intra-thyroidal extension and less aggressive histological variant. Foxp3+ lymphocytes progressively increased from outside the tumor to the intra-tumoral LI in PTC patients with TAL while they showed an opposite trend in PTC patients with CTL.
Our data suggest that concurrent CTL has a protective effect on PTC outcome and that the imbalance between cytotoxic and regulatory T lymphocytes in the intra-tumoral TAL may affect the tumor-specific immune response favoring a more aggressive behavior of cancer.
Thyroid Cancer Thursday Poster Translational
Foxp3+ regulatory T cells (Tregs) are increased in peripheral blood and intra-thyroid lesion of thyroid cancer. These Tregs facilitate the growth and invasion of thyroid cancer. Recently, there are increasing publications showing that Foxp3 can also express in cancer cells but its function remains inconsistent. Very limited information is available on Foxp3 expression in thyroid cancer cells. The activity or/and expression of PPARγ is down-regulated in thyroid cancer and the activation of PPARγ can result in the arrest of thyroid cancer growth. The relationship between Foxp3 and PPARγ has not been reported.
Human thyroid cancer cells and north thyroid cells were cultured to examine the express Fox3 at mRNA and protein level by real-time PCR and Western blot respectively. siRNA was used to inhibit the Fox3 expression. Cell proliferation, migration and apoptosis were examined to determine the cell function. PPARγ expression and activity were determined.
We demonstrated that Foxp3 expression was higher in thyroid cancer cells than in normal thyrocytes. Foxp3 inhibition by its shRNA decreased cell proliferation and migration, but increased cell apoptosis, suggesting a positive role of Foxp3 in thyroid cancer growth. Interestingly, Foxp3 inhibition led to the elevation of PPARγ expression and activity. In addition, Foxp3 inhibition downregulated the expression of NF-κB subunit p65 and cyclin D1 but upregulated caspase-3 levels. These molecular changes are in line with Foxp3 shRNA-mediated alteration of cell functions.
Our study demonstrates that thyroid cancer cells express a high level of functional Foxp3 and that the inhibition of this Foxp3 suppresses the proliferation and migration but promotes apoptosis in thyroid cancer cells likely via inhibiting PPARγ but promoting NF-κB and cyclin D1. The findings suggest that targeting Foxp3 in thyroid cancer cells may offer a novel therapeutic option for human thyroid cancer.
Thyroid Cancer Thursday Poster Translational
TP53 gene exerts a major role in the negative control of cell proliferation and in controlling signaling cascades important in DNA repair and apoptosis. It has been proposed that functional p53 protein is involved in the induction of anti-tumor CD4+ cytotoxic-T-cell activity against carcinoma cells. We aimed to investigate the clinical pathological role of p53 and immune cell markers in Differentiated Thyroid Cancer (DTC) and their utility as diagnostic and prognostic markers.
We used the ACIS-III system to evaluate p53 and immune cell markers including tumor associated macrophages (TAM); CD68 and tumor infiltrating lymphocytes (TIL) subsets such as CD3, CD4, CD8 and CD20 in 206 thyroid carcinomas, 105 benign nodules and 18 normal tissues. In addition, TP53 was sequenced in 78 out of 164 patients with papillary thyroid carcinoma.
Among the thyroid cancer patients, 85% evolved free of disease after 53.8±41 months of follow-up. P53 expression was observed more frequently in malignant than in benign lesions (p<0.0001) and helped discriminate follicular patterned lesions. In addition, p53 expression was more frequent in smaller tumors (p=0.0015), presenting as solitary nodules (p=0.0286), with thyroiditis (p=0.0486) and without metastasis at diagnosis (p=0.0201). We observed that TAM was present in 89.6% of P53 positive and 71.4% of P53 negative tumors (p=0.002). We did not -find any association between P53 expression and infiltration of CD3+TIL. A marginal association was found between P53 expression and infiltration of CD4+TIL (p=0.051). Interestingly, while 61.7% of P53 positive tumors presented infiltration of CD8+TIL, CD8+TIL was found in only 25.6% of P53 negative tumors (p<0.001). A Kaplan-Meier survival curve did not confirm p53 as an outcome independent determinant and there was no correlation, neither between p53 protein expression and TP53 mutational status, nor between TP53 and features of tumor aggressiveness.
In conclusion, we suggest that p53 and immune cells profile analysis by IHC might be useful in the differential diagnosis of thyroid lesions and may help characterize less aggressive cases that do not need hard-line management.
Thyroid Cancer Thursday Poster Clinical
Thyroid cancer is the fastest growing solid malignancy in the U.S. It is unclear if this is a true increase or reflects improved surveillance and diagnostic techniques. If due to increased surveillance, then incidence should vary with access to healthcare.
County-based thyroid cancer incidence for 2009 was obtained from the NCI state cancer profiles database. County-specific insurance coverage rates and median household income were obtained from the U.S. Census Bureau, Current Population Survey, 2009–2012. Correlation coefficients were calculated to evaluate the relationship between cancer incidence, insurance rates, and median household income.
Data was available on 1282 counties in 48 states. Incidence of thyroid cancer ranged from 3.9 to 39.7. The wealthiest counties with the highest insurance coverage had the highest incidence. There was a positive correlation coefficient between cancer incidence and insurance rates (0.27, p<0.001), as well as median income (0.17, p<0.001). Cancer incidence was more affected by insurance rates than median income. Each unit increase in insurance rate correlated to a 0.2 increase in thyroid cancer incidence (p<0.001). When considered by state, 6/8 states with the highest incidence are contiguous in the Northeast while 7/8 states with the lowest incidence are contiguous in the Southeast.
Thyroid cancer rates are greater in wealthier counties with higher rates of insurance coverage, suggesting that increasing thyroid cancer rates are in part due to increased surveillance. Other environmental factors also may contribute to geographic variance.
Thyroid Cancer Thursday Poster Clinical
The vast majority of patients with well differentiated thyroid cancer (WDTC) will have excellent outcomes, with only a select few at high risk of death from disease. None of the existing staging systems for WDTC however are capable of accurately predicting outcome for an individual patient. There is therefore a great need for an accurate, individualized method for predicting outcome, both for patient counselling and for selection of therapy in the growing number of patients presenting with WDTC. The aim of this study was to produce a nomogram to predict disease specific survival for individual patients with WDTC.
1810 consecutive patients treated surgically for WDTC between 1986–2005 were included in this retrospective analysis. Accurate clinical, histological, therapeutic, and outcomes data were collected for all patients. Multivariable Cox proportional hazards regression was used to model the association between predictors and the outcomes. Model reduction was performed using the stepdown method to eliminate predictors with less predictive ability from the final models with the purpose of simplifying the nomogram for widespread application. Concordance index was calculated for disease specific survival with bootstrap correction of overfit bias.
1298 patients (71%) were female with a mean age of 47 years (s.d.16 y). Mean tumor dimension was 2 cm (s.d. 1.5 cm). 315 (17%) had microscopic and 206 (11%) had macroscopic extra thyroid extension. 625 had no neck dissection (35%), 580 had benign nodes excised (32%) and 605 had positive nodal disease excised (33%). 53 patients (3%) presented with distant metastatic disease (M1). With a median follow up of 78 months (range 0–320 months), 55 patients died of disease. The 10 year DSS was 96%. Age, tumor dimension and M stage were independently predictive of outcome. A nomogram based on these factors was able to predict DSS with very high accuracy (concordance index of 0.96).

We have designed a nomogram which is highly accurate at predicting the risk of disease specific survival in individual patients with WDTC.
Thyroid Cancer Thursday Poster Clinical
Familial-non-medullary thyroid cancer (FNMTC) is defined as when 2 or more first degree relatives are affected and is thought to have an autosomal dominant pattern of inheritance. However, there has been no study investigating the mode of inheritance in FNMTC by prospectively ascertaining disease status. The aim of this study was to determine the inheritance pattern(s) of FNMTC.
Kindreds with 2 or more first-degree relatives affected with papillary thyroid cancer were prospectively enrolled and screened for thyroid cancer/nodule. The modes of inheritance were deduced from pedigree analysis.
Nineteen kindreds with 204 family members were enrolled in a prospective screening clinical protocol. 63 of the 204 patients had a thyroidectomy for a thyroid nodule: 3 had benign pathology, 84% (48/57) had papillary thyroid cancer, and 16% (9/57) had follicular variant papillary thyroid cancer. 13 of 19 families (68.4%) had a parent-offspring relationship and 60.5% (26/43) of the offspring generation was affected. The prevalence of thyroid cancer in the offspring generation was not different by the total number of affected members per family. Pedigree analysis suggested autosomal dominant inheritance with or without reduced penetrance in 13 families, autosomal recessive inheritance in 4 families and a possible X-linked inheritance in one family. When considering all family members with a thyroid neoplasm (benign/malignant) on screening ultrasound in the parent and offspring generation, the mode of inheritance was consistent with an autosomal dominant pattern in 15 of 19 families.
In FNMTC, the mode of inheritance is variable with most kindred showing an autosomal dominant pattern of inheritance. Our findings demonstrate that a complete pedigree analysis with screening ultrasound of unaffected family members should be performed to ascertain the pattern of inheritance and for counseling at-risk family members.
Thyroid Cancer Thursday Poster Clinical
While thyroid and parathyroid surgeries were initially performed using local anesthetic techniques, the advent of safe general anesthesia (GA) resulted in the majority of surgeons performing these procedures under GA. However, recent studies have evaluated the return to locoregional techniques, claiming similar results to resections performed in the traditional manner. The purpose of this study was to evaluate the intra-operative metrics and post-operative outcomes of these two approaches.
ACS-NSQIP data from 2005–2010 were queried for patients undergoing thyroid and parathyroid surgery. Of these, 1,771 patients received locoregional anesthesia (RA) with the remainder receiving GA. After patient demographics and pre-operative risk factors were obtained, data were evaluated for the effect of GA vs RA on outcomes of operative time, anesthesia time, unplanned return to OR, and time to discharge.
Patients who received RA had less EtOH and tobacco use, but were otherwise equivalent. No significant differences were noted in post-operative complications between the two forms of anesthesia. Operative time was significantly shorter with RA vs GA (112 minutes [95%CI 109–116]) vs (162 [95%CI 162–163]). Anesthesia time was also shorter with RA (71 minutes [95%CI 68–74]) vs (111 minutes [95%CI 111–112]). Time to discharge was significantly shorter, with 82.15% of RA patients leaving on day 0 and 15.67% on POD #1 vs 18.27% of GA patients leaving on day 0 and 69.71% on POD #1 (p<.0001). Upon stratification by CPT code, these differences remained statistically significant for the majority of procedures performed under RA, primarily thyroid lobectomy, total thyroidectomy, parathyroid exploration, and parathyroid re-exploration.
It remains for future studies to determine whether or not same-day neck surgeries are safe in regards to post-op hematoma and airway compromise concerns. RA is non-inferior to GA upon evaluation of thyroid and parathyroid complications recorded in the ACS-NSQIP database, and results in shorter OR and anesthesia times as well as earlier discharge. This, in addition to the reduced cost of RA over GA, may result in significant cost savings to healthcare systems.
Thyroid Cancer Thursday Poster Clinical
Thyroid cancer (TC) incidence has increased dramatically over the last decades in most developed countries. There is an ongoing discussion whether this is a result of an increased detection rate or if unknown factors contribute. The aim of this study was to analyze TC-epidemiology over 10 years in a long-time iodine-sufficient, well-defined geographic population of 1,5 million inhabitants in Western Sweden.
The National Cancer Registry (NCR) is mandatory in Sweden and covers over 98% of all malignancies. In a population-based registry for clinically detected TC in Western Sweden, 716 consecutive patients (male 198; female 518) were included 2001–2010. Their median age was 52 years (range 6–95). Compared with the NCR 95,3% of all cases diagnosed in the Western region were reported to the register without selection bias. Changes in age, sex, tumor size, stage and type were analyzed over time. Previous studies have shown that the population has an iodine intake well within the WHO-recommended limits.
The female TC incidence rose from 5 to over 9 cases/100 000 inhabitans during the 10 year period whereas the male incidence was stable around 2,5 cases/100 000. Tumor size, proportion with node metastases and distribution of tumor types did not change over time. 27% of the tumors were <1 cm at diagnosis. 45% had node metastases. 75% of the tumors were papillary.
The female incidence of papillary TC is getting higher in the Western region of Sweden. The distribution of tumor sizes was stable and the proportion of small tumors (<10 mm) was unchanged during the 10 year period. Preliminary data from 2011 and 2012 indicate continuous increase among females. Female dominance and unchanged tumor size indicate that other causative factors, than just better detection, are likely to explain the increasing incidence. This will be further studied in detail.
Thyroid Cancer Thursday Poster Clinical
Basal serum thyroglobulin assessed using an ultrasensitive assay (Basal-Tg) has been proposed as an alternative to TSH-stimulated thyroglobulin (Stim-Tg) measurement in the follow-up of patients with papillary thyroid carcinoma (PTC). We aimed to examine the relationship between Basal-Tg and Stim-Tg in patients treated for PTC, and the optimal Basal-Tg that predicts a Stim-Tg≥1μg/L and ≥5μg/L.
We retrospectively analyzed 166 pairs of Basal-Tg and Stim-Tg measurements, performed within a 6-month interval of one another, among 144 patients with a variety of PTC recurrence risks. All patients underwent total thyroidectomy with therapeutic central neck dissection if clinically indicated. Fifty eight (41%) patients received radioactive iodine therapy. Basal-Tg was measured using a second-generation Beckman ACCESS immuno-chemiluminometric assay. Stim-Tg was assessed during TSH stimulation by one of three methods, all of which achieved a TSH>25 mIU/L. All patients had negative anti-thyroglobulin autoantibodies. Pearson correlation was used to assess the relationship between Basal-Tg and Stim-Tg measurements. Area under the curve (AUC) and optimal thresholds for Basal-Tg were determined by receiver operating characteristic (ROC) analysis.
There was a strong, positive correlation between Basal-Tg and Stim-Tg (r(166)=0.93, p<0.001). The line of best fit was modelled by [Stim-Tg]=11.1[Basal-Tg] - 0.6, both measured in μg/L. A Stim-Tg≥1μg/L and ≥5μg/L was present in 68 (41%) and 12 (7%) observations, respectively. The AUC for Basal-Tg in identifying a Stim-Tg≥1μg/L and ≥5μg/L was 0.87 and 0.90, respectively, suggesting good discrimination. The optimal Basal-Tg value for identifying a Stim-Tg≥1μg/L was 0.20μg/L (sensitivity 77%, specificity 87%) and for a Stim-Tg≥5μg/L was 0.6μg/L (sensitivity 58%, specificity 94%).
Basal-Tg and Stim-Tg have a strong positive correlation. A Basal-Tg of 0.2μg/L and 0.6μg/L were the optimal values for identifying a of Stim-Tg≥1μg/L and ≥5μg/L, respectively. Incremental increase in Basal-Tg between 0.2μg/L and 0.6μg/L may require additional investigation with Stim-Tg and neck ultrasound to assess for PTC recurrence.
Thyroid Cancer Thursday Poster Clinical
Thyroid cancer continues to increase rapidly in incidence, and approximately 5% of non-medullary thyroid carcinomas are familial or hereditary. But, the clinicopathologic features and genetic basis of familial non-medullary thyroid carcinoma (FNMTC) are poorly understood. The Familial And Hereditary Non-medullary Thyroid carcinOMa (FAHNTOM) study is aimed to identify the clinicopathologic features, genetic and environmental factors of FNMTC.
Methods: The FAHNTOM study is designed as a prospective multicenter cohort study. A case of FNMTC was defined as a patient with the following two criteria: a well-differentiated follicular origin thyroid cancer and at least one first-degree relative with a well-differentiated epithelial origin thyroid cancer. After an informed consent is obtained from each subject, patients who are scheduled for thyroid surgery and their family members will be interviewed to get the pedigrees and questionnaires about lifestyle and environmental factors. Medical records, blood and tissue samples will be collected from patients and blood samples will be taken from family members who will be screened on a regular basis with high resolution neck ultrasound. The existing group of a large case-control study will be used as a control group for statistical analysis. The blood and tissue samples will be tested to find genetic predispositions for FNMTC. The results of ultrasound in family members will be analyzed to determine the screening strategy of FNMTC.
From November 2012 to May 2013, a total of 63 subjects (patients: 43, unaffected family members: 19, affected family member: 1) have participated in this study. The clinicopathologic features of patients were analyzed. In comparison with the sporadic cases, there was a significant difference in vascular invasion between the two groups (p=0.038).
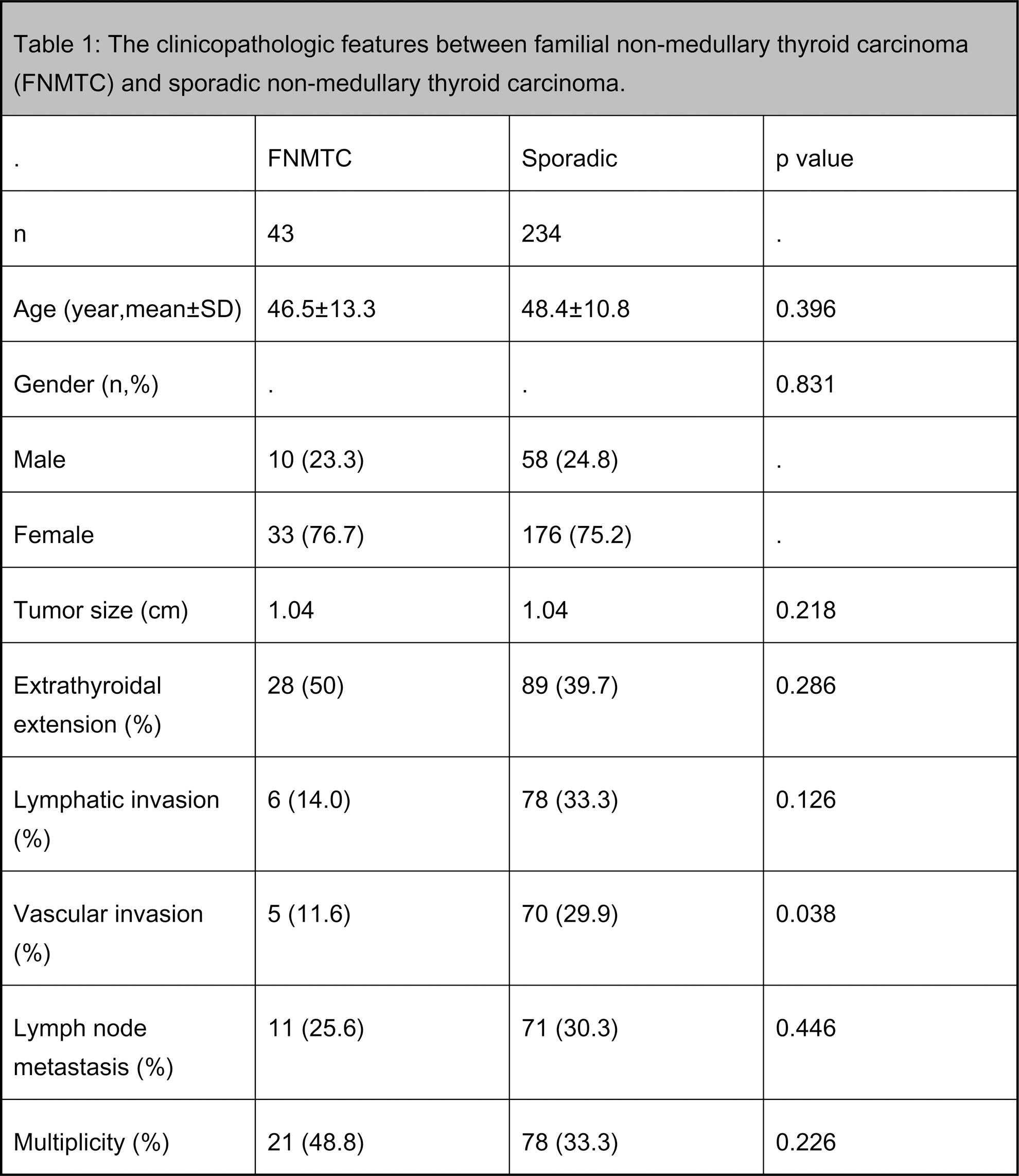
FNMTC is a rare disease entity of thyroid cancer and multi-constitutional long-term studies are needed to comprehend the disease. The FAHNTOM study is focused on this specific group of thyroid cancer patients which are radically increasing in South Korea. The results from this study are expected to be utilized for the clinical practice and research of FNMTC.
Thyroid Cancer Thursday Poster Clinical
Fine needle aspiration biopsy (FNAB) is the gold standard method in the characterization of thyroid nodules We aimed to evaluate the diagnostic efficacy of ultrasound-guided thyroid fine needle aspiration biopsy of larger thyroid nodules.
Thyroid ultrasonography, FNAB and histopathological data of a total of 371 patients subjected to surgery because of nodular thyroid disease between 2006 and 2011 were retrospectively examined.
We evaluated 407 nodules of 371 patients in this study. Mean age was 50,9±13,4 and mean TSH level was 1,6 [1.3–1.9] mIU/L. We grouped nodules by size; group A nodules (n=43) were smaller than 1 cm, group B nodules (n=234) were between 1–2.9 cm and group C nodules (n=130) were 3 cm or greater in diameter. Non-diagnostic cytology was present 23.3% in group A, 5.9% in group B and 7.7% in group C nodules. In group A; sensitivity, specificity, positive predictive value (PPV) of FNAB was 87.9%, 71.4%, and 87.9%, respectively. In group B sensitivity, specificity, PPV of FNAB was 65%, 79.6% and 78.9% respectively. In group C sensitivity was 55.5%, specificity was 80.9% and PPV was 52.6%.
This is the first study which shows that the sensitivity of USG guided FNAB decreases in greater nodules. This finding must be evaluated in larger series.
Thyroid Cancer Thursday Poster Clinical
In the accident of Chernobyl nuclear reactor, the contamination of milk with 131I, for which prompt countermeasures were lacking, resulted in large doses to the thyroids. This led to the increase of childhood thyroid cancer. Although thyroidal 131I measurements and reconstructions were extensively performed, the dose relationship had not been confirmed until 2011. In the accident of Fukushima Nuclear Power Stations on March 11, 2011, the residents within 20 km radius of NPSs were instructed to move before the evening of next day and the instruction of food control (<200 Bq/kg of 131I for drinking water and milk) was issued on the 6th day and of the distribution restrictions of contaminated food on the 10th day.
The measurements of thyroidal 131I were performed from March 26 to March 30, 2011, using a NaI (TI) scintillation survey meter in 1080 children under the age of 15 in evacuation areas. Thyroidal 131I were also measured using NaI scintillation spectrometer or using whole body counter in March, 2011. The program to survey thyroids of all 360,000 children in Fukushima Prefecture by ultrasonography started from 2011 by the requests from psychological and social demands.
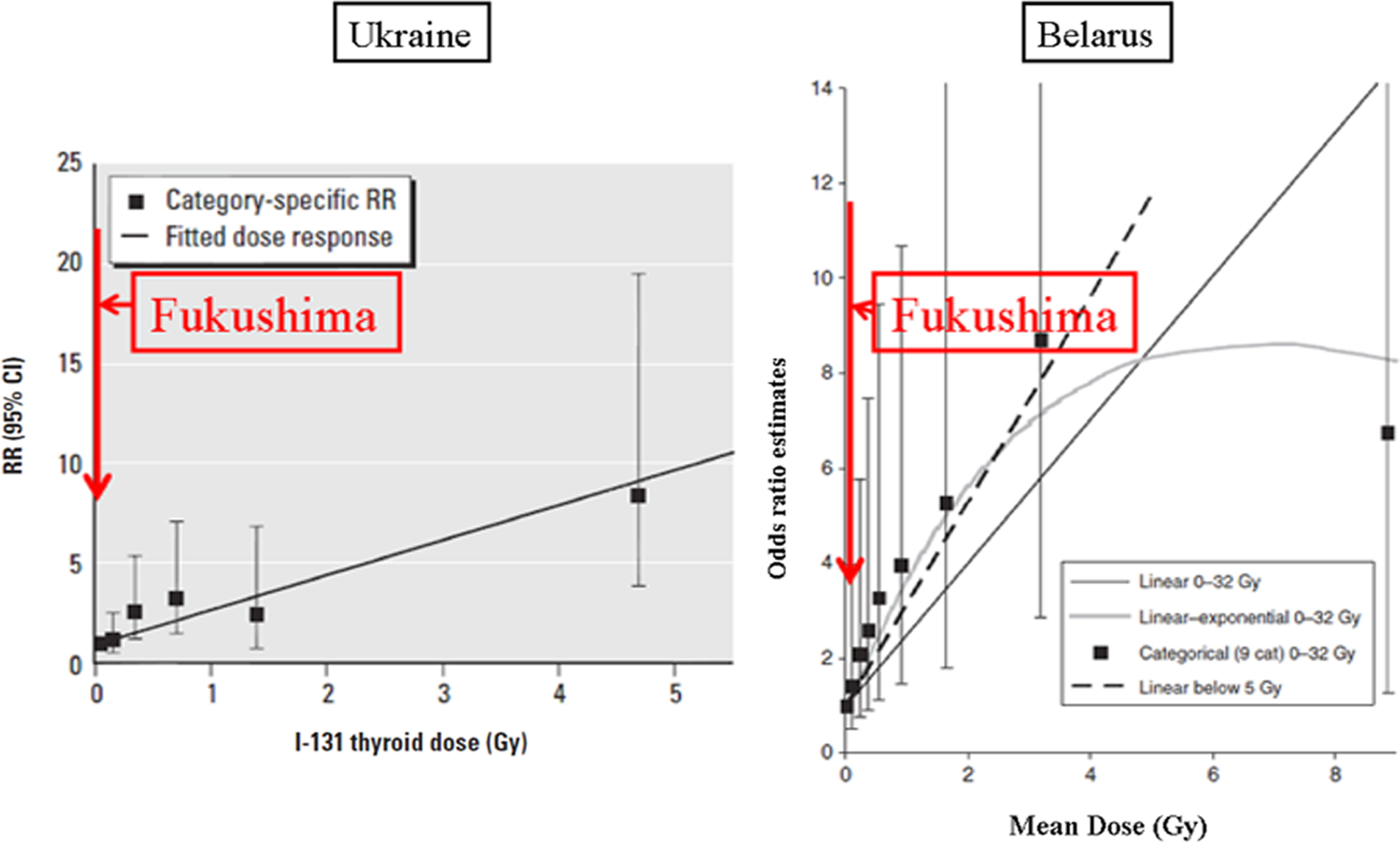
Thyroid Radiation Doses in Fukushima, Ukraine and Belarus in Dose-response Relationship between Thyroid Cancer and I-131.
No children showed values greater than 50 mSv (Intervention level). Comparison of thyroidal 131I among Fukushima, Ukraine and Belarus is shown in the figure. However, according to the information on the website (5/6/2013), 174,976 children were examined; nodules were found in 1.15% (0.51%>5 mm), and malignancy was suspected in 29 children. Among them, 13 were operated and 12 (69/million) were confirmed as papillary carcinoma.
The incidence of childhood carcinoma is reported to be one/million in many countries, and the maximum incidence in Chernobyl accident is 40/million in 1995 in Belarus. The countermeasure for thyroid carcinoma is the biggest issue in not only health consequences in the Fukushima accident, but also in the general thyroidology.
Thyroid Cancer Thursday Poster Clinical
The management of medullary thyroid cancer (MTC) after resection remains complex, with multiple variables affecting risk of recurrence. We introduce a dynamic postoperative risk stratification tool for MTC recurrence, based on patient, tumor and treatment characteristics.
After institutional review board approval, 124 MTC patients who were treated entirely at Memorial Sloan-Kettering Cancer Center between 1986–2010 were identified. Immediate postoperative risk groups were defined as low, intermediate, and high based upon extent of extrathyroidal extension, presence of regional or distant metastases and preoperative calcitonin level. Response to therapy categories were then defined as excellent, acceptable and poor based upon 6 month calcitonin level and presence of radiographic structural disease. Overall risk groups based upon the immediate postoperative risk and the response to therapy category were then defined.
The median age was 55 years (range: 6–88). Median follow-up was 66 months (range: 1–229). In the immediate postoperative risk groups, the 5-year risk of structural recurrence for low, intermediate, and high risk groups was 5.9%, 24.9%, and 67.8% respectively (p<0.001). In the overall risk groups, the 5-year risk of structural recurrence for low, intermediate, and high risk groups was 3.2%, 24.0%, and 45.9% (p<0.001). Low risk patients with poor responses to therapy had increased recurrence risk from 5.9% to 24.9%, while high risk patients with excellent responses to therapy reduced their recurrence risk from 67.8% to 24.9%.
A clinically useful dynamic risk stratification tool to predict risk of recurrence in MTC patients over time is introduced. Its prognostic value may augment patient counseling on prognosis, help determine the frequency and extent of follow-up investigations, and aid decision-making for adjuvant treatment.
Thyroid Cancer Thursday Poster Clinical
Cervical ultrasound(US) is a standard part of the preoperative evaluation of patients with thyroid cancer. The ability of US to identify nodal disease in the central neck is debated which has lead to the utilization of prophylactic central dissection in order to prevent early disease recurrence.
Retrospective analysis of a prospective database of all clinically N0 well differentiated cancer patients. Patients undergoing lymph node (LN) dissection at time of thyroidectomy were excluded, as were patients without documented US evaluation of the neck. Patient demographics and out comes were reviewed, and patients were categorized based on who performed the thyroid US (a single thyroid surgeon vs. non-surgeon sonographer). Recurrence was defined as the need for additional radioactive iodine treatments or subsequent positive pathology on biopsy or exploration.
From 2005 to 2012, 177 patients were assessed with US prior surgery. 48 patients had surgeon performed US in clinic, compared to 129 patients with non-surgeon performed US. Groups were equivalent in age, gender, operative procedure, tumor size, and tumor characteristics. Surgeon US group had LN assessment documented more frequently (69% vs. 20%, p<0.01). While equivalent rates of papillary and hurthle cell carcinoma where in both groups, the surgeon performed US group had a higher incidence of follicular carcinoma (p<0.01). Treatment and dosing with radioactive iodine were equivalent. Radioactive iodine uptake following ablation was significantly lower in surgeon performed US (p<0.05). Recurrence rates were significantly higher in the non-surgeon US group in comparison to the surgeon US group (11% vs 0%, p=0.01, Figure 1). Median time to recurrence was 1 year. However, mean follow up was longer in the non-surgeon US group (24±2.3 months vs. 40±2.3, p<0.01).
US examination of the thyroid should include a routine evaluation of the cervical LN stations. Performance of an US by a sonographer specializing in thyroid cancer ensures optimum assessment and correctly identifies patients as N0 which may eliminate the need for prophylactic LN dissection and not increase the risk of early recurrence.
Thyroid Cancer Thursday Poster Clinical
The impact of preoperative neck US on management of the lateral neck in patients with WDTC is unclear. The objective of this study was to assess the impact of preop neck US on the rate of lateral neck dissection and postop Response to Therapy (RTT).
An IRB approved retrospective review of 892 patients from an institutional database of WDTC between Jan 1 2009 to Dec 31 2010 was carried out. Patients with palpable neck disease, distant metastases, less than total thyroidectomy, no postoperative thyroglobulin (Tg), no postoperative US and positive Tg antibodies were excluded leaving 468 patients available for analysis. Patients were divided into those who had preoperative neck US (241 patients) and those that did not (227 patients). Patient and tumor characteristics were compared using the Chi square test. The primary endpoint was RTT as defined by postoperative US and Tg level.
There were no significant difference in age, histology type, T stage, postoperative RAI dose, AJCC stage, ATA risk or duration of follow up between the 2 groups. Patients with preoperative neck US had more Lateral neck dissection (LND) compared to patients without preoperative Neck US (24(10%) vs 9(4%); p=0.006). In patients having neck dissection, there was no significant difference in the positive or total number of lymph nodes resected between the 2 groups. Importantly, those receiving a preoperative neck US had better RTT (more likely to be NED, less likely to have biochemical or structural incomplete response) than those without preoperative neck US (p=0.003).
Preoperative neck US detects more lateral neck disease, facilitates lateral neck dissection resulting in better Response to Therapy.
Withdrawn
Thyroid Cancer Thursday Poster Clinical
Fibroblast growth factor receptor 4 (FGFR4) is associated with development and prognosis in some cancers. The FGFR4 Gly388Arg polymorphism is a prognostic factor in many cancers, but this significance in thyroid cancer is unclear. This study investigated the relationship of the FGFR4 Gly388Arg polymorphism with clinical, pathological and molecular parameters including BRAFV600E mutation, and evaluated the prognostic outcome in papillary thyroid cancer (PTC).
FGFR4 Gly388Arg polymorphism was evaluated in 247 consecutive patients with PTC by polymerase chain reaction-restriction fragment length polymorphism, along with examination of clinical, pathological, and molecular parameters including BRAFV600E mutation and expression of biological tumor markers. Clinical outcome indicating cancer recurrence/persistence was also evaluated in a subgroup of study subjects.
Gender and age distribution, cancer characteristics such as tumor size, extrathyroid extension, multiplicity, lymph node metastasis, expression of biological tumor markers, and the frequency of BRAFV600E mutation were not different between three FGFR4 genotypes (Gly/Gly388, Gly/Arg388, and Arg/Arg388). However, the FGFR4 Gly/Gly388 genotype was associated with extrathyroid extension (P=0.045) in patients with PTC-BRAFV600E. Tumor recurrence of PTC was more frequent in the Gly/Gly388 group than in other FGFR4 genotypes (P=0.043). Univariate analysis of disease-free survival using the Kaplan-Meier estimation showed that FGFR4 Gly/Gly388 genotype had more likelihood of tumor recurrence (4/25) than the Gly/Arg388 and Arg/Arg388 groups (1/41), but this is not statistically significant (P=0.12).
The FGFR4 Gly388Arg polymorphism might have no dominant effects on cancer progression and prognosis in PTC.
Thyroid Cancer Thursday Poster Clinical
ATA guidelines recommend measurement of thyroglobulin level (Tg) in the wash out of lymph node FNA for the diagnosis of metastatic thyroid cancer. This series compares aspiration cytology to Tg in the needle wash out for the diagnosis of metastatic thyroid cancer in a community FNA clinic.
Patients with a tissue diagnosis of papillary thyroid carcinoma, and sonographically abnormal lymph nodes with negative cytologic on-site assessment for metastasis were included. Needles were rinsed in 1 ml of normal saline, and Tg measured by the Siemens chemiluminescent method. Tg test is positive if >1.0 ng/mL in athyroid patients and >36 ng/mL with thyroid gland. All biopsies and cytologic evaluations were done by one cytopathologist with 12 years experience in FNA and education in neck ultrasound. Sensitivity, specificity, PPV and NPV were calculated for cytology and Tg using histology as the gold standard for discordant cases.
39 lymph nodes from 31 patients were analyzed. 38 nodes from 30 patients had concordant results in final cytology and Tg (35 negatives and 3 positives). One node had negative cytology but positive Tg (1.6 ng/mL); this node was negative for metastasis on excision. For cytology, sensitivity, specificity, PPV and NPV was 100%. For Tg, sensitivity=100%, specificity=97.2%, PPV=75% and NPV=100%.
An increase in sensitivity for metastatic thyroid carcinoma may not be seen in all settings by adding Tg level measurement to cytology in lymph node FNA. Practice settings such as experience of the aspirator and availability of on site assessment may weigh heavily on the baseline sensitivity of aspiration cytology, and thus in the benefits obtained by adding Tg testing. Sensitivity and NPV was identical for both tests in this series, although the selection bias could reduce Tg false negatives which would have lowered Tg sensitivity. As with any test, Tg false positives have been described before, and thus its effect in the specificity and PPV for detection of metastasis must be considered. The use of a 1.7 ng/mL cutoff proposed by some authors for the chemiluminescent method would result in identical performance for both tests in this series.
Thyroid Cancer Thursday Poster Clinical
Follicular neoplasm (Bethesda IV cytology) requires thyroid lobectomy for diagnosis. Approximately 15–30% of cases are ultimately malignant, often requiring reoperative completion thyroidectomy. The use of intraoperative frozen section in these cases is controversial. We sought to reassess whether intraoperative frozen section (FS) reduces the need for reoperative thyroidectomy.
A retrospective chart review of patients with follicular neoplasm on fine needle aspiration (FNA) from 2003–2012 was performed. It is our practice to offer thyroid lobectomy with FS for these patients; if FS was suspicious, total thyroidectomy was performed instead. FS suspicious for papillary thyroid carcinoma (PTC) was based on nuclear features (nuclear grooves/atypia, pseudonuclear inclusions) and for follicular thyroid carcinoma (FTC) was based on capsular/vascular invasion.
A total of 148 patients with follicular neoplasm on FNA were identified, of which 79 underwent FS. Fifteen had suspicious FS with 12 having malignancy on final pathology, for a positive predictive value of 80%. Nine showed features suspicious for PTC, of which 8 had PTC. Six showed features suspicious for FTC, of which 4 had malignancy on final pathology. Of the 64 patients with unremarkable FS, 49 had benign final pathology, for a negative predictive value of 77%. Twelve (19%) patients required reoperation. Seven of 19 patients (37%) with malignancy avoided reoperation due to FS. Risk of malignancy with follicular neoplasm diagnosis was 34% (51/148), while risk of malignancy with follicular neoplasm and suspicious FS was 80%.
Risk of malignancy with follicular neoplasm and suspicious frozen section is 80%. Frozen section may avoid reoperative completion thyroidectomy in up to a third of patients.
Thyroid Cancer Thursday Poster Clinical
The diagnosis and treatment of differentiated thyroid cancer (DTC) is associated with good prognosis. However, quality of life can be affected by treatments and long term side effects. Our study evaluates the quality of life of Puerto Rican patients with a diagnosis of DTC.
Patients with diagnosis of DTC were identified at the General Endocrinology Clinics at the University Hospital of Puerto Rico. Medical chart was reviewed to obtain demographic and clinical data, thyroid function tests, surgeries and other treatments received. A validated Spanish version of the University Of Washington Quality Of Life Questionnaire (QOL) was administered to each patient. The questionnaire evaluates the domains of pain, appearance, activity, recreation, swallowing, chewing, speech, shoulder, taste, saliva, mood, anxiety and other global questions. The association between QOL scores and variables of interest, such as treatment modalities and age at diagnosis, were evaluated using the Mann-Whitney test.
A total of 75 patients with DTC participated. Mean age of the group was 51.54±13.3 years; 84.0% were female. Papillary thyroid cancer was diagnosed in 96.0% of them, 66.7% underwent total thyroidectomy and 32.0% had total thyroidectomy with lymph node dissection. Of those who underwent treatment with radioiodine, 60.6% received <150 mCi of therapy, while 21.2% received >150 mCi of radioiodine therapy. A total of 82.7% of the patients reported that their health was the same or better than it was before treatment. The mean composite score was 82.3, meaning an overall little effect on QOL. Patients diagnosed with DTC after 45 years of age reported a significantly better score on the pain domain (p<0.05) when compared with those patients diagnosed earlier. Patient who received >150 mCi of radioiodine had a tendency toward a worse score on the same domain (p=0.05).
This group of Puerto Rican patients with DTC reported an overall little change on their QOL. However, patient who received >150 mCi of radioiodine and those diagnosed on or before 45 years of age, showed lower scores on the pain domain than their counterparts. Future treatment strategies must include periodic QOL evaluations and long-term side effect of therapy in order to tailor therapy in this growing population of patients.
Thyroid Cancer Thursday Poster Clinical
There has been controversy of the lobectomy for well differentiated thyroid cancer (WDTC). Current guidelines recommend total thyroidectomy for the cancer over 1 cm, despite previous report suggesting that the lobectomy provides similar excellent outcomes. The purpose of our study is to report our experience of WDTC treated by thyroid lobectomy.
We retrospectively analyzed 284 patients with WDTC treated by thyroid lobectomy at department of Surgery in Chosun University Hospital from January 2002 to December 2010. Overall survival (OS) and disease-free survival (DFS) were determined by the Kaplan-Meier method. Factors predictive of recurrence by univariate and multivariate analysis were determined using the χ2 test and Cox proportional hazard model respectively.
With a mean follow-up of 60.4 months, OS and RFS for all patients were 97.9% and 96.5% respectively. No patient died due to WDTC. Univariate analysis showed statistically significant differences in recurrence by tumor size (p=0.013) and presence of invasion (p=0.039). However, Multivariate analysis showed no significant difference in local recurrence.
Patients with WDTC confined to one lobe can be safely treated by lobectomy.
Thyroid Cancer Thursday Poster Clinical
Pathology subspecialty practice is still in infancy in Kuwait. It started few years back after a group of local pathologists did their training in North America. The aim of this study: 1) describe the most common problems in thyroid pathology experienced by general pathologists. 2) Determine discrepancy in thyroid pathology diagnoses after reviewing by subspecialized pathologist.
The archive materials of the author were reviewed. The cases were divided into two groups. Group I: cases were sent for the author before issuing a report or a provisional report was issued and awaiting the consultation opinion. Group II: cases were the final reports issued and sent for the Cancer Center for review and reviewing pathologist doubting the diagnosis; or a review was requested by a clinician.
Seventy three cases were identified in the archives concerned with thyroid pathology. 48 cases (65.7%) were included in group I and 25 in group II. All cases in group I referred by pathologists being the Cancer Center had the highest number of referral (77%). Twenty three (92%) cases in group II were referred by pathologists and 2 by clinicians. Among all referred cases follicular patterned thyroid nodules was the most common causes of referral seen in 64 (87.6%) followed by undifferentiated carcinoma seen in 3 (4%) of the cases. In group I, 22 cases provided with provisional diagnoses; 12 (54.5%) were changed after revision. In group II, (12/25) the diagnoses were changed after revision of the cases, (50%) had significant implication on management or prognosis.
In conclusion, 1) Follicular patterned thyroid nodules is the most challenging problem in thyroid pathology. 2) High percentage of change in diagnoses after revision mostly due to unawareness of nuclear morphology of papillary carcinoma.
Thyroid Cancer Thursday Poster Clinical
The objective of the present study is to evaluate the rise in TSH levels and the quality of life of patients after Recombinant human thyrotropin (rhTSH) administration for the treatment and follow-up of papillary thyroid cancer, without the presence of hypothyroidism or thyroid hormone withdrawal.
Prospective, longitudinal and comparative study. Two groups were compared; G1: patients without hypothyroidism and administration of rhTSH. G2: patients with 4 weeks hypothyroidism and thyroid hormone withdrawal. Studied variables: levels of TSH before and after the administration of rhTSH and 4 weeks of hypothyroidism, quality of life, as well as the presence of cold intolerance, dry skin, palpebral oedema, lower extremity oedema, constipation, sleep, weight gain, physical activity incapacity, loss of memory and other side effects. The statistical analysis was made by means of chi square and Fisher and Yates exact probability with level of significance of p=0.05.
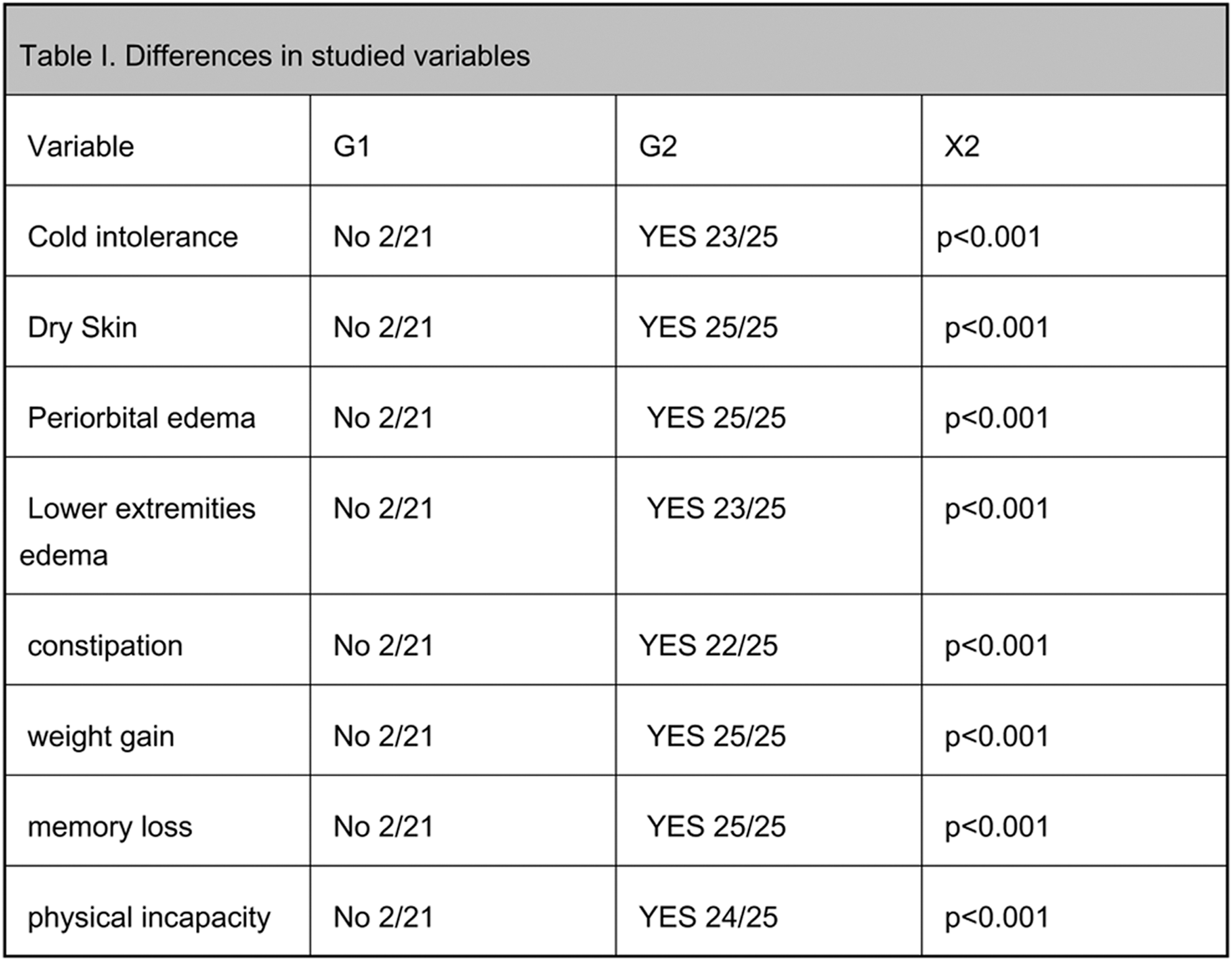
Elevation in TSH levels above 30U/mL in G1 (72 hours after rhTSH administration) and G2 (after 4 weeks of thyroid hormone withdrawal).
G1 (n=21) and G2 (n=25) in both groups the TSH rose above 30 mU/ml and the average elevation for each group was not statistically different (p=0.098). The evaluation of the quality of life had a statistical difference (p<0.001) in favour of G1. All other variables also had statistically significant differences (p<0.001) again in favour of G1. One G1 patient felt slightly nauseous. The administration of recombinant human thyrotropin offers adequate levels of TSH elevation without altering the quality of life.
Thyroid Cancer Thursday Poster Clinical
We are presenting a case of follicular carcinoma of the thyroid with metastasis to the rib 57 yo woman with past history of mediastinal lymphoma treated with chemotherapy and radiation was referred to Endocrinology clinic for newly diagnosed metastatic follicular thyroid cancer. A left thyroidectomy was done 10 years ago due to a large nodule that displaced the trachea. The lesion was benign and right lobe of thyroid was normal. Pathology reports were not available. 7 years ago an incidental enlarging right paraspinal mass was discovered. Due to pain and discomfort a CT scan of chest was obtained and a left 9th rib mass was discovered incidentally. CT guided core biopsy showed metastatic follicular cancer of the thyroid. Bone scan showed no evidence of metastasis. She underwent completion thyroidectomy and excision of both masses. Pathology showed incidental 1 mm papillary carcinoma of thyroid, the rib mass measured 7 cm and consistent with metastatic follicular carcinoma of thyroid with negative margins, and the paraspinal mass consistent with lipoma with calcification and necrosis. She received 201 mCi of iodine-131 after recombinant human TSH (rh-TSH) stimulation. The total body scan post treatment showed intense activity in the neck but no evidence of distant metastatic disease. Her levothyroxine dose was adjusted accordingly.
The serum thyroglobulin(Tg) trended from 3999 ng/mL to less than 0.2 ng/mL without anti-Tg antibodies after the surgery and RAI therapy. Table above includes lab values.
We are presenting a case of follicular carcinoma of the thyroid with metastasis to the rib. There are few cases reported and it is found to be an unusual presentation. The incidence of follicular carcinoma presenting with metastatic disease of bone is 7–20%. We suspect her initial nodule was not benign thyroid tissue rather follicular carcinoma in addition. This patient had many risk factors associated with thyroid cancer and would have been benefited from aggressive management modalities.
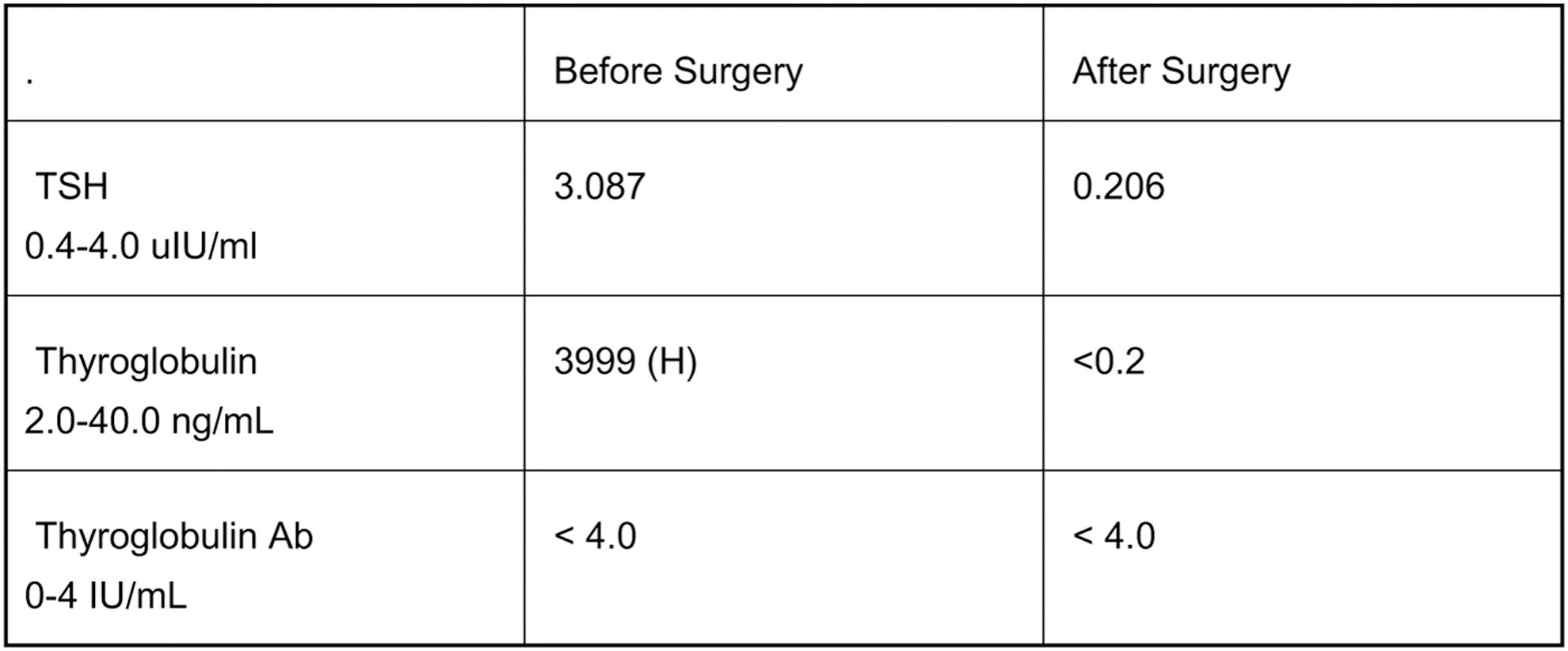
Withdrawn
Thyroid & Development Thursday Poster Clinical
Currently the main stream practice for postoperative care following a thyroidectomy has been on an inpatient basis. Due to the abundant advancements in surgical techniques, these procedures have shifted from the traditional 23 hour observation setting to same day surgery procedures. The purpose of this study was to compare the outcomes of same day surgery and 23 hour observation thyroidectomies encompassing patients with similar morbidity scores.
We performed a retrospective comparison between 100 consecutive patients that underwent outpatient thyroid surgery from June 2008 to May 2013 and 100 patients that underwent thyroid surgery and held post operatively for 23 hour observation. All patients met predetermined morbidity scores based on the Charlson index score. Clinical variables including patient demographics, body mass index (BMI), and surgical outcomes were obtained and analyzed. Principle outcome measures were thyroid volume, length of operation, length of hospital stay, incidence of complications, and estimated blood loss (EBL). Clinical characteristics of patients and operative data were compared between the groups using Student t-test, and the Chi-square test.
Of the two hundred patients undergoing thyroid surgery; 100 were accomplished on an outpatient basis, and 100 under a 23 hour observation status. The outpatient and observation groups were similar in BMI (29 vs. 30, P=.288), operating room time (180.6 vs. 191.2, P=.152), and thyroid volume (40.3 vs. 40.4, P=.99). The postoperative complications including temporary hoarseness, hematoma, wound cellulitis, seroma, and paresthesia stay did not statistically differ between groups.
In a select patient population with a similar Charlson index score of 3 or less, same day thyroid surgeries has yielded favorable experiences. Same day thyroid surgery can be accomplished in a safe and effective manner in a high volume academic setting with excellent results.
Thyroid Hormone Action Thursday Poster Basic
Thyroid disorders compromise the integrity of brain tissues, such as hippocampus and parietal cortex, influencing behavior and process of learning and memory. The deiodinase type III (D3) prevents activation of T4 converting it into reverse T3 which are considered inactive form of the hormone. D3 is increased in critically ill patients, primarily in tissues with hypoxic ischemic injury. During the status epilepticus there is a high release of catecholamines, which can cause several changes, including metabolic acidosis entailed by respiratory failure. Cerebral hypoxia and ischemia also appear to be key to the of self-regulated interruption of seizures. A failure of this inhibition can increase the extension of status epileptics. Following this reasoning we evaluated the effects of epilepsy on D3 expression and the local reduction of T3 in brain tissue. We also evaluated the levels of neuroglobin, an intracellular hemoprotein which has a strong protective role against oxidative stress and is increased during hypoxia.
We studied rats with epilepsy induced by pilocarpine and quantified the expression of D3 in the hippocampal regions, using the method of Immunohistochemistry and Western Blot. A group of rats stayed for 3 hours in status epileticus and then was killed to remove the hippocampus (acute group). Another set of rats was killed two months after the induction of the epilepsy for remove the hippocampus (chronic group).
D3 expression was dramatically increased in acute and chronic epilepsy in hippocampus in CA3, CA1, Dentate Gyrus and Hilo. Also, the neuroglobin levels were significant higher in the epileptic animals, showing that during epilepsy the brain is in a hipoxic state.
Our data shows that epilepsy leds to a hipoxia and an increased expression of D3 in the hippocampus in both acute and in chronic state. The higher D3 activity could be a neuroprotective effect. Also, it is possible to correlate the consequences of epilepsy to a local reduction of the of thyroid hormone in this disease.
Thyroid Hormone Action Thursday Poster Basic
Adult-onset hypothyroidism causes emotional and cognitive alterations. These are paralleled by alterations in the cell population dynamics of the hippocampus, which involve an increase in the expression of markers of DNA damage and apoptosis. It has been recently shown that some fatty acids are able to modify the cell population dynamics in different regions of the nervous system. Particularly, the dietary supplementation with n-3 polyunsaturated fatty acids (ω-3 PUFAs) attenuates certain symptoms of neuropathological disorders such as autism, depression, anxiety, and Alzheimer disease, by an effect that involves the stimulation of cell proliferation and glutamatergic synapse formation in regions such as the hippocampus.
In this study we evaluated the ability of the dietary supplementation with ω-3 PUFAs to prevent the effects of hypothyroidism on the hippocampal cell population. We induced hypothyroidism to a group of rats by treating them with methimazole for 4 weeks. A second group received supplementation with ω-3 PUFAs (350±0.75 mg/kg/day) along with the antithyroid treatment.
Open-field behavior tests showed that hypothyroid rats have reduced motivation for exploration and a reduced ability to modify their behavior by experience (i.e., learning), and that both traits are prevented by supplementation with PUFAs. Immunodetection of marker proteins showed that PUFAs do not change the population dynamics of hippocampal cells in normal conditions, but reduce the expression of p53, associated with DNA damage, in hypothyroid animals. The expression of markers of cell arrest (p21) or apoptosis (Bax/Bcl-2) was not modified.
These results suggest that the administration of ω-3 PUFAs exerts partial neuroprotection against the effects of hypothyroidism in cell populations of the hippocampus. Work supported by SIP-20131071. A. B.-C. is fellow of PIFI-IPN.
Thyroid Hormone Action Thursday Poster Basic
Subclinical hypothyroidism is a common diagnosis in children as well as in adults. Subclinical hypothyroidism is known to be a risk factor for arteriosclerosis. Alterations of blood lipids as well as markers for inflammation and hemostasis were shown in adult patients. In children data on this topic are rare. Calibrated automated thrombography visualizes the entire process of thrombin generation, and is the only overall function test of coagulation that is sensitive to hypercoagulable states. Lagtime, time to peak, peak, endogenous thrombin potential, start tail and velocity index are parameters of thrombin generation. Aim of this study was to analyze the correlation between thyroid function and thrombin generation.
31 children (16 females) with a median age of 8.2 years (range 1.4–17.9) and a suspected subclinical hypothyroidism underwent a thyroid function test (TRH-stimulation test) and had simultaneously determined factor II and thrombin generation.
Median basal TSH was 4.7 U/ml (range 1.0–22.9). We found a significant correlation between TSH and factor II (p<0.05). Moreover, we found a significant correlation between lagtime and fT3 (p<0.05) and between velocity index and fT3 (p<0.05). We found no correlation between thyroid function and other parameters of thrombin generation.
Our data show that there is a correlation between thyroid function and thrombin generation in children with subclinical hypothyroidism and that impaired thyoid function could lead to a hypercoagulable state in children.
Thyroid Hormone Action Thursday Poster Clinical
Developmental hip dysplasia is a significant musculoskeletal pathology with health and cost implications at both the individual and societal level. There are several well-known risk factors associated with developmental hip dysplasia, however, the potential role of thyroid hormones is unclear. Graves' disease is the most common cause of autoimmune hyperthyroidism in pregnancy, and uncontrolled Graves' disease is associated with miscarriages, pregnancy-induced hypertension, prematurity, low birth weight, intrauterine growth restriction, stillbirth, thyroid storm, and maternal congestive heart failure. Triiodothyronine and thyroxine have been shown to be important regulators of early bone and muscular development. It has been hypothesized that excess amounts of thyroid hormone early in pregnancy is a risk factor for developmental hip dysplasia. Data is limited to a single retrospective cohort study by Ishikawa in 2008 which concluded that there was an association between developmental dysplasia of the hip and first-trimester maternal hyperthyroidism. Since Ishikawa's initial report, there have been no other studies evaluating the relationship between maternal hyperthyroidism and developmental dysplasia of the hip.
In this case report, we describe the complication of developmental dysplasia of the hip in the child of a pregnant woman who presents in the second trimester with new onset uncontrolled Graves' disease.
As thyroid hormones are important regulators of early bone and muscular development, we postulate that untreated maternal Graves' disease may be a risk factor for development of neonatal hip dysplasia.
Children of mothers with untreated hyperthyroidism during pregnancy should be monitored for developmental hip dysplasia to prevent long-term complications requiring costly corrective measures. Further studies should be performed to assess whether the incidence of developmental hip dysplasia is increased in the infants of mothers with uncontrolled Graves' disease during pregnancy.
POSTER 68. Table

Thyroid Hormone Metabolism & Regulation Thursday Poster Basic
Iodine is essential for thyroid hormones (THs) synthesis and an important regulator of thyroid function. Maternal THs are important in promoting normal placental and fetal development. Adequate maternal iodine intake is required for the THs synthesis. The drastic consequences of iodine deficiency during pregnancy are well described; however, the effects of iodide excess during this period are still controversy. Therefore, this study aimed to investigate the consequences of iodide excess exposure during pregnancy (P) and lactation (L) periods on thyroid function of rat dams.
Female Wistar rats were treated with iodide excess (5X, 50X and 500X the physiological dose) in drinking water throughout P+L. After these treatments, body weight, heart weight and the number of pups were evaluated. Thyroid genes expression was evaluated by Real-Time PCR and Western Blotting. D1 activity was evaluated in the kidney and liver.
All treatment doses reduced body and heart weight of rat dams in comparison to control group. Iodine treatment decreased the number of pups, and the most striking result was observed in the higher dose of treatment, that led to an increased number of stillbirth. Iodine excess reduced the expression of NIS, Tg, TPO and TSHR in a dose-dependent manner. D1 activity was also reduced after iodine treatment.
Our study strongly suggests that THs production is impaired in rat dams exposed to iodine excess during P+L, since the expression of proteins involved in THs synthesis were reduced after iodine treatment. Moreover, the reduced activity of D1 suggests that THs peripheral metabolism was also impaired by the treatment. Thus, iodine excess seems to lead to central and peripheral hypothyroidism in rat dams, which may have serious consequences in the development of their offspring, as shown by the increased number of stillbirth in the higher dose of iodine treatment. Finally, iodine excess may be as harmful as iodine deficiency to intrauterine and neonatal development.
Thyroid Hormone Metabolism & Regulation Thursday Poster Clinical
Hypothyroidism and obesity are prevalent conditions in the U.S. The use of bariatric surgery to treat obesity has increased substantially in recent years and weight loss can be dramatic. It is unknown what effect various methods of bariatric surgery have on thyroid hormone replacement in the setting of primary hypothyroidism. This is particularly true of gastric bypass (Roux-en-Y) procedures which may alter intestinal absorption of LT4. This study utilizes data from one academic medical center to determine whether bariatric surgery for weight loss impacts thyroid hormone requirements in adults with primary hypothyroidism.
The University of Texas Southwestern Research Data Warehouse was utilized to identify individuals who had undergone bariatric surgery at the institution between 4/1/05 and 12/1/12 and had a diagnosis of hypothyroidism at the time of surgery. Individuals were included if they were taking LT4 for thyroid hormone supplementation and had serum TSH value within the reference range prior to surgery. Roux-en-Y, gastric sleeve and gastric banding procedures performed either openly or laparoscopically were included. Exclusion criteria were central (secondary) hypothyroidism, use of medications known to cause disturbances in thyroid function, and use of any thyroid hormone replacement other than LT4 during the study period. Doses of LT4 preoperatively were compared to doses 0–6, 6–12, 12–24 and 24–36 months postoperatively.
We included 40 patients (24 with gastric banding, 12 with Roux-en-Y and 4 with sleeve gastrectomy surgery). Of the 12 patients with Roux-en-Y procedures, 3 (25%) required a reduction in LT4 within the first 6 months of surgery and 4 (36.4%) within the first year. No significant dose changes were observed in the gastric banding and sleeve gastrectomy groups.
Our data suggests that a significant proportion of individuals undergoing bariatric surgery with Roux-en-Y procedures may require a reduction in dose of LT4 soon after surgery. Clinicians should be aware of this possibility and measurement of thyroid function tests with appropriate dose adjustment should occur within the first 6 months of gastric bypass surgery.
Thyroid Hormone Metabolism & Regulation Thursday Poster Clinical
It has been reported that the presence of thyroid antibodies or TSH above 2.5 μU/mL in the first trimester affects outcomes of pregnancy.
Objective: To assess the effects of autoantibodies and TSH levels on pregnancy outcomes.
Methods: We measured TSH and antithyroid antibodies in 967 consecutive singleton pregnant women at their first visits to Seibo Catholic Hospital in 2011. Pregnancy outcomes in relation to TSH or antibody levels were examined.
Mean gestational age at the examination was 10.6 weeks. TSH levels were above 2.5 μU/mL in 53 women (5.5%), and 64 women (6.6%) were positive for antithyroid antibodies. In 20.3% of the antibody-positive and 4.4% of the antibody-negative women had TSH levels above 2.5 μU/mL (p<0.01). The frequencies of miscarriage in women with antibody-positive versus antibody- negative and women with TSH above 2.5 μU/mL versus women with 2.5 μU/mL or below were 5.9% versus 3.4% (p=0.42), and 4.9% versus 3.6% (p=0.67), respectively. However, there was a positive correlation between the frequencies of miscarriage and TSH levels (r=0.72), and the frequency in women with TSH 3.0 or above was 13.6%. The frequencies of previous miscarriage were not affected the presence of antibodies nor TSH levels. Forty-three percent of antibody-positive women had previous successful delivery, which was not inferior to antibody-negative women (43%). The frequencies of preterm birth in antibody-positive and -negative women were 2.3% and 3.1%, respectively. No preterm birth was found in women with TSH above 2.5 μU/mL.
No positive association exists between the presence of thyroid antibody and miscarriage or premature delivery. TSH above 2.5 μU/mL not always indicates adverse outcomes of pregnancy. The reason that our data are conflicting to others may be due to the methods to measure TSH and thyroid antibodies, or the small sample size. Furtherr investigations with larger sample size will be necessary.
Thyroid Hormone Metabolism & Regulation Thursday Poster Clinical
Serum thyrotropin (TSH) levels of the elderly are often above the upper normal range even when the patients show no clinical symptoms of hypothyroidism. Over the past two decades, the upper TSH reference limit has declined from 10 mIU/L to 2.5–3.5 mIU/L. This decrease is due to several factors, namely improved sensitivity and specificity of monoclonal antibody-based immunometric TSH assays, exclusion of individuals with subclinical autoimmune thyroid disease from the reference population, and the elimination of high values that are due to cross-reactivity problems with other glycoproteins. The controversy surrounding the lowering of the TSH upper reference limit is that it may lead to the unnecessary treatment of healthy individuals. Indeed, serum TSH 3.0–4.5 may be an early indicator of hypothyroidism; however, an upper reference interval of 2.5–3.0 mIU/L would yield a 300–400% increase in the number of patients who are clinically not in need of LT4 treatment; overtreatment may cause serious health problems, including adverse cardiovascular effects. Objective: To determine if higher TSH with increased age is due to the increased presence of biologically inactive isoforms of TSH.
In order to selectively control for elevated TSH, we obtained 148 serum samples of patients from 6/2012-1/2013 at the Georgetown University Hospital. Inclusion criteria were only serum samples with TSH concentrations greater than 5 uIU/mL. Patient ages ranged between 21–99 y. TPOAb and TgAb were measure by ELISA. Thyrotropin receptor (TSHR) antibodies were measured using the TSH-Binding Inhibiting Immunoglobulin (TBII) immunoassay.
72% of the subjects were females; 80% older than 70 years. 17/148 (11.5%) subjects were positive for TPOAb. 7/148 (0.5%) subjects were TgAb positive. 21/148 (0.14%) were positive for TSHRAb and 19/148 (12.8%) were positive for TSI.
Since most of the subjects were not positive for the antibodies the high TSH will be tested for inactive TSH isoforms that are measured in the laboratory test but may not be representative of a clinical condition such as hypothyroidism. We are currently comparing these TSH forms with other TSH types known to be less biologically active.
Thyroid Imaging Thursday Poster Clinical
After the Fukushima Daiichi Nuclear Power Plant accident (nuclear plant accident) following the Great East Japan Earthquake on March 11, 2011, there has been concern about an increase in the incidence of childhood thyroid cancer because of internal exposure to radioactive iodine. In Fukushima prefecture, thyroid ultrasonography(US) has been performed as a screening test for thyroid cancer, and there have been many clinical findings and concern about the influence of the accident. Herein, we report the findings in 2753 children screened by thyroid US at Ito hospital in Tokyo over the last 10 years using a screening method similar to that now used in Fukushima prefecture.
A total of 2753 children aged 15 years or younger visited ito hospital from Jan 2003 to Aug 2012, (boys: 518; girls: 2235; average age:12.0 years). These children were screened by thyroidal US and the incidence of nodules was evaluated.
The findings were as follows; 1) no obvious nodules: 1471 (53.4%); 2) cysts: 994 (36.1%); 3) solid nodules: 227 (8.2%); 4) neoplastic lesions (confirmed by pathological examination): 43 (1.6%); 5) aberrant thymus: 13 (0.5%); 6) suppurative thyroiditis: 5 (1.8%). In addition, we compared the results obtained with the use of the 12 MHz digital linear probe(DLP) introduced in our hospital in 2010 and those obtained with the previously findings. The corresponding results before/after the introduction of this probe were as follows: any US findings 671 (40.7%)/651 (54.2%). These findings demonstrate the significant advantage, in terms of the detection ability, of the 12 MHz DLP (p<0.0001: χ2 test). In a study where 670 subjects without any palpable goiter or nodules were examined using the 12 MHz DLP, we obtained the following results: 1) 200; 2) 435; 3) 30; 5) 5. The corresponding results by age (2–5 years/6–10/11–15): 63/185/422 subjects were as follows: 1) 42/60/98; 2) 19/111/205; 3) 1/10/19. Furthermore, our study revealed no significant difference in the incidence of nodules between before and after the nuclear plant accident.
Our study indicated that thyroid US revealed many clinical findings in the child cohort that could not be detected by blood tests or palpation. This could probably be attributable to the improved precision of the test instrument.
Thyroid Imaging Thursday Poster Clinical
Ultrasound is essential for the management of thyroid and parathyroid diseases. We sought to determine the level of training in ultrasound technique and the utilization of surgeon-performed ultrasound (SPUS) among endocrine surgeons.
American Association of Endocrine Surgeons members and recent endocrine surgery fellows were sent a survey requesting information on current practice profile, training background, SPUS utilization and practice impact.
The survey was completed by 36% (173/481) of recipients. Half of respondents have been in practice <10 yrs. 73% reported that thyroid and parathyroid surgery comprised the majority of their practice, and 75% practice at academic teaching hospitals. 60% have completed an endocrine surgery fellowship, and 58% performed ultrasound during fellowship. Only 18% had ultrasound exposure during residency. Of fellowship trained respondents, 31% did not learn biopsy techniques, and 60% did not practice SPUS in the operating room. Currently, 65% of respondents employ SPUS. 66% complete SPUS in more than half of initial patient consults, 70% perform US-guided thyroid and lymph node biopsies, and 39% perform their own lymph node mapping prior to neck dissection. Only 22% use SPUS for long-term surveillance of their thyroid cancer patients. Of the surgeons performing adrenal/pancreatic surgery, 50% employ intra-op SPUS. Over 50% felt that SPUS altered surgical decision making “sometimes” and 31% “most of the time”. The following were cited as primary sources of ultrasound education: an endocrine surgeon (34%), formal ultrasound course (35%), radiologist (9%), and self (7%). Support for “rich ultrasound exposure” was nearly universal, and 64% of respondents support mandatory SPUS training during fellowship. Although 76% felt “very” or “extremely” comfortable with SPUS interpretation, 43% would still obtain a radiology-performed ultrasound. The majority (53%) rated SPUS as “indispensable”.
Ultrasound is employed by a growing number of endocrine surgeons, and most deem it necessary for clinical practice. The level of training and versatility of usage are disparate. The incorporation of formal SPUS education into endocrine surgery fellowship training would be advantageous.
Thyroid Nodules & Goiter Thursday Poster Translational
Although the BRAF V600E mutation has low sensitivity for cancer in cytologically indeterminate thyroid nodules, its high specificity may help guide a decision to perform a total thyroidectomy instead of lobectomy as the initial operation. Currently, microarray-based molecular evaluation of thyroid nodules provides accurate detection of benign nodule signatures in cytologically ambiguous nodules, but could also address additional clinical questions, such as gene mutation status, in a single combined analysis. Here we present a molecular test for the identification of the V600E mutation in thyroid fine needle aspirates (FNAs) using mRNA to detect downstream gene expression perturbations resulting from the BRAF V600E mutation.
FNAs were obtained from over 200 cytologically indeterminate (across all three Bethesda sub-categories) and malignant nodules. The gene expression of more than 3,000 transcripts was measured by custom microarray for each FNA, and BRAF V600E-positive or negative labels for training and test samples were established using castPCR (Life Technologies). We specified a minimum detection of 5% mutant allele frequency to designate a sample V600E-positive.
These data were then used to select discriminative transcripts and to train a support vector machine classifier. The performance of the classifier was evaluated using both 10-fold cross-validation as well as an independent test set. The overall false positive rate is less than 1% (99.4% specificity, 95% confidence interval (CI) 96.9%-99.9%) while maintaining sensitivity comparable to that of most DNA-based tests (93.3%, 95% CI 77.9%-99.2%).
The classifier was able to accurately determine the presence or absence of the BRAF V600E mutation in FNAs using changes in gene expression. By capturing the downstream transcriptional effects of that mutation this test is more likely to be robust to potential rescue mutation. Pre-operative knowledge of BRAF gene mutation may reduce the necessity for completion thyroidectomy, intraoperative frozen section review, and in the future, consideration of mutation-targeted chemotherapeutics.
Thyroid Nodules & Goiter Thursday Poster Clinical
The aim of this study is to identify the most common methods in which thyroid nodules are detected and to determine whether or not there is a correlation between the mode of discovery and the rate of malignancy.
The study comprised of a retrospective medical record review of 495 consecutive patients referred to our clinic for thyroid nodule evaluation during the year 2012. Patients were evaluated by one of two ECNU-certified thyroidologists and ATA nodule guidelines were followed in determining the need for FNA.
Of the 495 patients,122 (24.6%) had their nodules discovered on physical exam, 75 (15.2%) were noted by the patients themselves and 298 (60.2%) were found on incidental imaging (see Table 1). Subsequently, 292 patients required FNA and a total of 395 nodules were biopsied. 25 nodules, in 25 patients, were found to be malignant after surgical resection. This represents an overall cancer rate of 5.1%. Of these, 7 (28%) were discovered by patient detection, 3 (12%) were found on physical exam and the remainder, 15 (60%), were discovered on incidental imaging (see Table 2). Accordingly, malignant nodules found on patient detection had a malignancy rate of 9.3%, with those found on incidental imaging of 5.1% and physical exam of 2.5% (see Table 3).
The majority of nodules discovered were via incidental imaging, most frequently on US for abnormal TFTs/symptoms and to a lesser extent, CT. Physical exam remains a common mode of detection, second to incidental imaging but more frequent than patient discovery. The nodules discovered by patient detection had the highest rate of malignancy, followed by those found on incidental imaging and then physical exam. Upon a closer look at the rate of malignancy by mode of detection, the nodules found on PET scan had the highest rate of malignancy, trailed by carotid Doppler and then patient detection. In our study, nodules detected on physical exam were least likely to be malignant. To further solidify our findings, we plan to combine our data with two other sites in order to determine if there is a consistent trend in the method of detection and rate of malignancy.

Thyroid Nodules & Goiter Thursday Poster Clinical
The malignancy rate of nodules categorized as FLUS (Bethesda III) has traditionally been estimated at 5–15%, lower than the 15–30% rate for follicular neoplasm (FN; Bethesda IV). Therefore, a repeated fine needle aspiration (FNA) has been recommended for FLUS; in contrast, surgical resection has been recommended for FN. We hypothesize that the probabilities of malignancy in FLUS and FN are similar.
Of 2106 patients undergoing FNA at a tertiary care center between 2010–2013, 203 (9.6%) had Bethesda III cytopathology; 125 (5.9%), Bethesda IV. The risk of malignancy was determined from 127 nodules with available surgical pathology. A multivariable regression model was used to identify clinical and nodule factors associated with malignancy: age, gender, nodule size, and suspicious sonographic features.
The malignancy rate in FLUS nodules was 21% (12/56); in FN, 32% (23/71) (p=.24). There were 4/108 (3.7%) patients with incidental microcarcinomas. Nodules were more likely to be malignant in patients <45 (OR 2.4, p=.04) or if ultrasound revealed microcalcifications (OR 3.6, p=.007). An indeterminate nodule with microcalcifications in a patient <45 was at 7.4-fold escalated risk of malignancy. Patient gender, nodule size, and other ultrasound features (irregularity, vascularity, echogenicity) were not significantly associated with malignancy.
This study supports emerging literature that the rate of malignancy in Bethesda III nodules is higher than initially estimated, and is comparable to Bethesda IV nodules. The risk of malignancy in indeterminate nodules was highest in younger patients with microcalcifications, but was not associated with nodule size. Because malignancy rates are similar in Bethesda category III and IV nodules, we advocate managing these lesions similarly. These findings may have relevance in the era of emerging molecular assays for indeterminate thyroid nodules.
Thyroid Nodules & Goiter Thursday Poster Clinical
The Afirma® Gene Expression Classifier (AGEC) has been shown to identify benign thyroid nodules among those classified as cytologically indeterminate with a negative predictive value of 94%-95%. This test therefore has the potential of avoiding unnecessary surgery on cytologically indeterminate nodules that ultimately are found to be benign. A recent report suggests that the rate of surgery on indeterminate nodules can be decreased from 74% to 7.6% by the use of the AGEC. This study was undertaken to determine if this observation is reproducible.
The medical records of all patients evaluated by the authors for a thyroid nodule from 9/1/2012 to 6/15/2013 were reviewed. 32 patients were identified in whom an FNA was performed by the authors and submitted for AGEC analysis (FNA Group). 9 patients in this group and 7 additional patients with a suspicious AGEC prior to referral underwent thyroidectomy (Surgery Group). In all patients in both groups, FNA cytology was interpreted as indeterminate (Bethesda Category 3 or 4) by cytopathologists within our institution
In the FNA Group AGEC was interpreted as benign in 13 patients (41%) and suspicious in 19 patients (59%). 9 of these 19 patients have undergone surgery and 6 were found to have papillary thyroid cancer (PTC). Of the additional 7 patients in the Surgery Group, 3 had PTC. A total of 9 patients (56%) in the Surgery Group had PTC. (Figure 1)
This study confirms that patients with a suspicious AGEC have a high likelihood of having PTC and should undergo surgery. Because patients with benign AGEC did not undergo surgery, we cannot draw any conclusions about its negative predictive value. However, the number of patients with a benign AGEC (41%) is substantially less than reported elsewhere. This may be due to inter-institutional differences in the risk of malignancy in each of the Bethesda cytological categories. There may also be a referral bias in patients referred to a surgical group. The potential benefit of the AGEC in avoiding surgery on benign nodules may be less than anticipated.

Thyroid Nodules & Goiter Thursday Poster Clinical
The definition of cervical mediastinal goiter (CMG) is based on variable criteria leading to a considerable variation in the reported incidence (from 0.2 to 45%). The incidence of peri- and post-operative complications when it is present is higher than that in thyroidectomy for cervical goiter. The aim of this study was to evaluate the preoperative risk factors associated with post-operative complications.
From 2000 to 2012, 142 (8.5%; 98 women and 44 men; mean age of 58 years; range: 35–78) of the 1690 patients who underwent total thyroidectomy had a CMG, defined as a goiter that was totally or partially located in the mediastinum when the patient was in the operating position, with an edge at least 3 cm below the sternal manubrium. We retrospectively evaluated the following parameters; sex, age, histology, pre- and retro-vascular position, recurrence, extension beyond the carena compared to surgical time, and the number of post-operative complications.
All but two procedures were terminated via cervicotomy, where partial sternotomies were required. No perioperative mortality was observed. Results of the statistical analysis (Student t test, Fisher's exact test) indicated an association between recurrence, extension beyond the carena with surgical time and post-operative complications.
Total thyroidectomy is the procedure to perform in CMG even if the incidence of complications is higher than for cervical goiters. The major risk factors associated with post-operative complications are recurrence and extension beyond the carena. In the presence of these factors, greater care should be used.
Thyroid Nodules & Goiter Thursday Poster Case Report
Parathyroid cysts are rare, and less than 300 cases have been reported in literature. They are often confused with thyroid nodules and goiter both during physical examination and during ultrasound imaging of the neck. Most parathyroid cysts have sizes ranging from 3–5 cm in size with few measuring over 10 cm in size. Even though parathyroid cysts have been reported with size over 10–15 cm, we found no reports of drainage of over 100 ml of fluid from the parathyroid cyst. We report a case of giant non-functioning right inferior parathyroid cyst measuring over 9 cm in size with retrosternal extension which drained 195 ml of fluid on 2 aspirations.
A 50 year old lady was referred for goiter with progressive dysphagia. She had noticed a swelling in the front of her neck for 6 years which gradually increased in size. Ultrasound examination revealed a 9 cm cyst in the region of the right lobe of the thyroid replacing the rest of the thyroid gland to the left.
Fine needle aspiration revealed clear fluid of 180 ml in the first aspiration and 15 ml of hemorrhagic fluid in the subsequent aspiration. Parathormone assay showed a level of 153 picogram/ml in the cystic fluid with normal serum parathormone level. Cytopathology reports of the fluid showed macrophages with no epithelial cells.
1. Parathyroid cysts are most often located in the neck. Most are non-functional and present as a neck mass or are found incidentally during imaging or neck surgeries. 2. A parathyroid cyst should be suspected in a patient who has a cystic mass that usually yields water-clear fluid on aspiration. 3. Aspiration of the cyst fluid and confirmation of elevated parathormone concentrations in the cyst fluid is diagnostic. 4. Aspiration of cyst fluid may be curative for non-functioning parathyroid cyts in most patients.
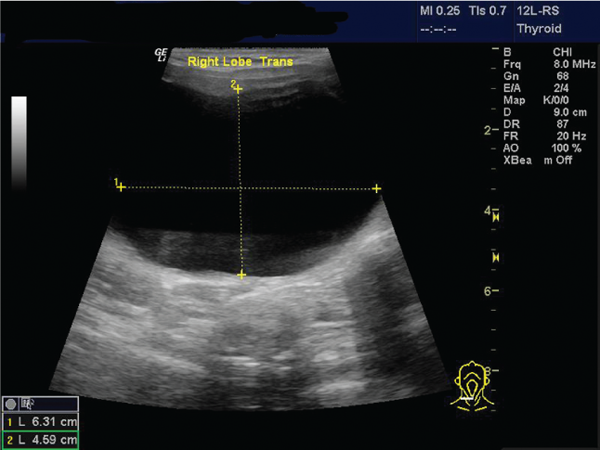
Autoimmunity Thursday Poster Case Report
Introduction: Graves' disease, characterized by autoantibodies to the thyroid stimulating hormone receptor, accounts for the majority of cases of hyperthyroidism. Pretibial myxedema, known as Graves' dermopathy, occurs in less than 5% of patients with Graves' and almost always takes place within the first year of diagnosis or treatment of hyperthyroidism.
Methods: A 52 year-old African American woman, with a 20 pack-year smoking history, developed Pretibial myxedema 28 years after Graves' hyperthyroidism was treated, initially with Methimazole, followed by thyroidectomy and finally successfully with radioactive Iodine.
Physical examination revealed non-pitting scaly thickening, induration, hyperpigmentation, tingling and numbness of the skin on her legs. In addition, prominent bilateral exophthalmos and acropachy were present. Patient laboratory values were: TSH 0.94 mlU/L (reference range 0.4–4.5 mlU/L and TSI 578% (<140%). T3 uptake, total T4 and free T4 were within normal limits. Treatment with topical steroids under occlusive dressings was unsuccessful.
Discussion: Pretibial myxedema, as a result of the accumulation of glycosaminoglycan (GAGs) such as hyaluronic acid and chondroitin sulfate secreted by fibroblasts in the dermis, happens in up to 4.3% of patients with history of thyrotoxicosis and usually develops within one year of diagnosis of hyperthyroidism. Ophthalmopathy almost always precedes dermopathy and acropachy. Topical steroids are the first line treatment of pretibial myxedema. Other options include high potency clobetasol ointment with oral pentoxifylline, intralesional steroid injections, octreotide, systemic steroids and cytotoxic therapy with various degrees of success.
Conclusions: This appears to be the only documented case of the development of thyroid dermopathy outside of the commonly reported time frame following the diagnosis and treatment of Graves' hyperthyroidism.

Graves' dermopathy
Disorders of Thyroid Function Thursday Poster Case Report
Hyperthyroidism can occur in 0.1–0.2% of pregnant women, with Graves' disease as the most common cause. Rarely, gestational trophoblastic disease can cause hyperthyroidism and even result to thyroid storm. We report here a case of multiparous woman admitted due to vaginal bleeding from partial molar pregnancy, and who later developed thyroid storm after total abdominal hysterectomy with bilateral salphingo-oophorectomy (TAHBSO).
A 40-year old Filipina, G15P9 (9059), admitted due to vaginal bleeding, nausea and vomiting. The pregnancy test was positive and the ultrasound of the pelvis revealed an enlarged uterus with multiple grape-like masses within, no fetal echo or gestation sac. She underwent emergency TAHBSO due to sudden profuse vaginal bleeding. Post-operatively, she developed fever, tachycardia, shortness of breath and hypertension. There was no palpable thyroid mass on examination. Her FT4 and B-HCG were elevated and her TSH was suppressed. Thyroid storm was considered with a Burch and Wartofsky score of 55. High dose propylthiouracil, propranolol and hydrocortisone were started.
Thyroid storm resolved after 2–3 days of medications. The PTU was shifted to methimazole which was discontinued after 2 weeks. B-HCG decreased to near normal 2 weeks after the surgery. Methotrexate therapy was given to prevent gestational trophoblastic neoplasia.
Thyroid storm arising from partial molar pregnancy is a very rare event. Treatment is, however, similar with hyperthyroidism arising from primary thyroid diseases. On the other hand, definite treatment of molar pregnancy is surgical removal of the mass and prophylactic chemotherapy to prevent the development of neoplasia.
Withdrawn
Thyroid Cancer Thursday Poster Case Report
The ultimobranchial bodies contribute to thyroid development. The majority of this contribution consists of calcitonin-producing C-cells, however, embryologic remnants known as solid cell nests, consist of cells that display nuclear membrane irregularities mimicking nuclear features of papillary carcinoma. While ultimobranchial body remnants may have some link to the histogenesis of rare thyroid tumors including mucoepidermoid carcinoma, primary neoplasms of these structures have not been described.
A 64-year-old woman with a history of colon carcinoma was found to have an elevated CEA level. A PET/CT scan localized a nodule in the right thyroid. There was no previous exposure to ionizing radiation or family history of thyroid cancer. Laboratory testing showed a normal TSH and free T4. Fine needle biopsy was reported as suspicious for papillary carcinoma. The patient underwent total thyroidectomy.
The thyroid contained a 1.0×0.9×0.6 cm nodule in the right lobe. On histological examination, this lesion consisted of polygonal-to-elongated cells with centrally located, oval nuclei; they displayed variable nuclear membrane irregularities with squamoid features lacking intercellular bridges. The lesion was positive for p63, mCEA (focal), TTF-1 (SPT-24), CK7 and CK19, and was negative for HBME-1, thyroglobulin, chromogranin-A and calcitonin. These features are consistent with an ultimobranchial body remnant tumor and are not characteristic of other known thyroid neoplasms. The remainder of the thyroid exhibited fibrosing thyroiditis with multiple smaller solid cell nest proliferations consistent with ultimobranchial body rest hyperplasia.
To our knowledge, neoplastic proliferations of ultimobranchial body remnants have not been described. This index case suggests that ultimobranchial body remnant tumors do occur and should be added to the spectrum of proliferative lesions of thyroid that can mimic papillary carcinoma.
Thyroid Cancer Thursday Poster Case Report
A 47 y/o Caucasian female presented for initial care for thyroid cancer without any family history of any malignancy or personal history of head & neck radiation exposure. Her thyroid cancer history is as follows: 1996: Papillary thyroid cancer (PTC) after FNA of self-palpable nodule. Underwent total thyroidectomy at outside facility. Pathology reported 2.5 cm PTC in R thyroid lobe & an additional 0.3 cm focus on the same side. Focus of adenocarcinoma was noted outside the thyroid in an area suspicious for vascular invasion but did not involve the inked margin of resection. A 1 cm focus of PTC was in the L thyroid lobe 1999: Underwent excision of a palpable neck nodule. Pathology showed a 2.4 cm paratracheal granulation & hypertrophic scar in the R thyroid bed 2008: Negative PET scan with no suspicious area in the neck, chest, abdomen, & pelvis Patient recalled having medullary thyroid cancer but no available records indicated such. Starting in 2009, calcitonin serologies were checked. TG, TG antibody, calcitonin, & CEA have been undetectable & negative Additional past medical history was significant for: 2002: Underwent colectomy, cholecystectomy, and partial hepatectomy for metastatic rectal cancer & multiple polyps due to familial adenomatous polyposis (FAP) 2004: Diagnosed with CML, on Imatinib & recent BCR/ABL PCR quantitative fusion transcripts undetectable 2008: Desmoid tumor of the abdomen resected We reviewed original slides from 1996 which demonstrated grooved nuclei & intranuclear cytoplasmic inclusions without psamomma bodies with extension to the desmoplastic stroma with areas of cribriform pattern.
Association between PTC and FAP has been noted since 1949 when Crail reported its first case. FAP associated PTC did not become a distinct type of PTC until Harach et. al first described its histopathology in 1994. Genetic disruption in APC gene and gain in RET proto-oncogene with activation of RET/PTC1 isoform lead to development of FAP associated thyroid neoplasm. While there is a 1–2% lifetime risk of FAP-associated thyroid cancer, there should be low index of suspicion and dedicated annual thyroid exam by experienced thyroidologist is recommended in appropriate clinical context.
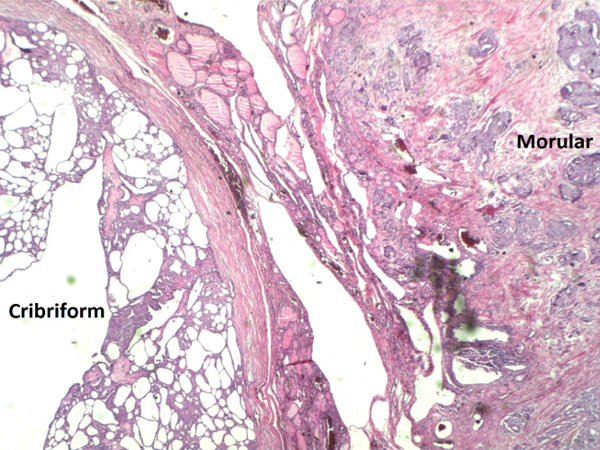
Low power photomicrograph of cribriform morular pattern.
Thyroid Cancer Thursday Poster Case Report
No effective systemic chemotherapy exists for radio resistant aggressive metastatic thyroid cancer and patients are still treated with surgery and suppressive levothyroxine therapy. Molecular targeted therapies have shown promising response in phase 2 trials. We report a case where combination therapy with Sorafenib and Valproic acid for two weeks resulted in stable disease and progression free survival of 25 months.
85 year old male diagnosed with Stage IV papillary thyroid cancer, T4a, N1, M1 disease in Sep 2010 is status post total thyroidectomy and RAI ablation therapy in Nov 2010. Post therapy scan showed extensive activity in the remnant thyroid bed. His thyroglobulin levels were 137 with negative antibodies. A PET/CT scan in Jan 2011 revealed FDG avid tumor in the thyroid bed invading tracheal lumen with metastasis in the paratracheal, mediastinal and bilateral hilar lymph nodes. He went to M.D. Anderson Cancer Center, Houston in January 2011 where he underwent valproic acid and Sorafenib treatment. Unfortunately, after 2 weeks of treatment, he developed hand/foot syndrome and stopped chemotherapy. In March 2011, unstimulated thyroglobulin was 52. In May 2012, thyroglobulin was 8.8 and repeat CT scan of the thorax revealed stable mediastinal and bilateral hilar lymph nodes. Most recent thyroglobulin in May 2013 was 15. He is currently on levothyroxine 150 mcg daily.
In our patient progression free survival was 25 months with stabilization of the disease process. Thyroglobulin levels improved significantly and continue to remain low even 2 years after therapy.
Combination of Valproic acid which is a class 1 selective histone deacetylase inhibitor and Sorafenib which blocks the B-Raf pathway for treating aggressive thyroid cancer is still experimental. Also, does this combination therapy improve the radioiodine avidity of the tumor and can patients be treated with RAI therapy subsequently remains to be seen.
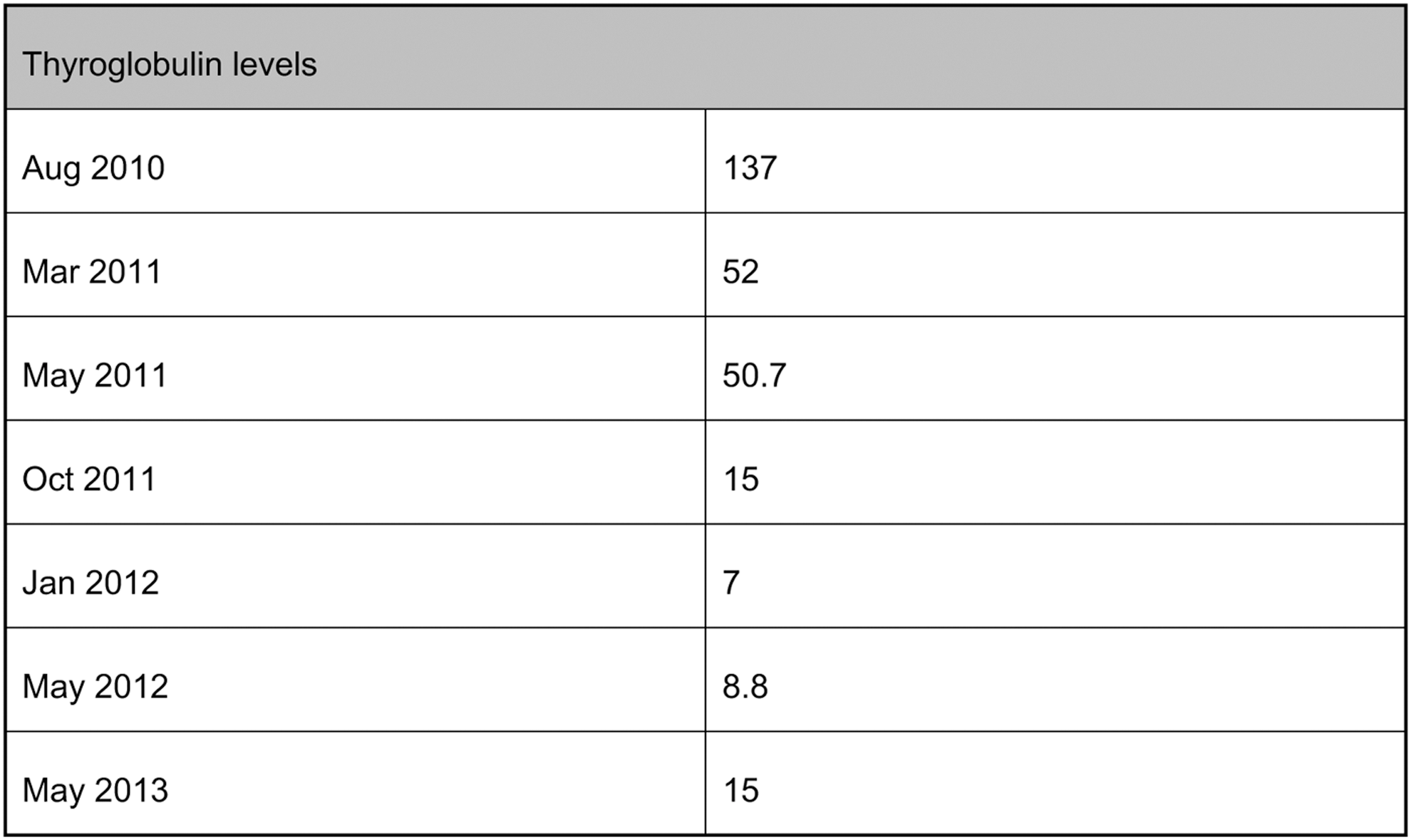
Thyroid Cancer Thursday Poster Case Report
Objective: Report the case of a 39 y/o woman who presented with recurrence of a papillary thyroid microcarcinoma (PTMC); and to review current management recommendations and treatment dilemmas.
Case Presentation: 39 y/o female on therapy for hypothyroidism, referred for evaluation of multinodular goiter. Thyroid nodules were suspicious for papillary thyroid carcinoma (PTC) on FNA biopsy. Patient underwent total thyroidectomy and pathology report of specimen confirmed the diagnosis of PTC, multifocal, with the largest tumor measuring 0.8 cm without capsular invasion, margins free of tumor and lymph nodes (LN) negative for metastasis. I131 radioiodine ablation (RAI) therapy was given and TSH suppression therapy was started. WBS post therapy and one year after therapy were negative for residual tumor or metastases. Neck ultrasound (US) performed 8 months after surgery was unremarkable. A follow up US (16 months post-surgery) showed hypoechoic nodular regions at thyroid bed. Patient underwent surgical resection with central neck dissection after FNA of the 3 mm nodule at right thyroid bed showed recurrent PTC. Final pathology report was positive for LN metastases bilaterally. Follow up WBS was negative for residual neck thyroid tissue or metastatic disease. Multiple LN were found once more in a follow up US. This patient has consistent positive anti-thyroglobulin antibodies titers; quantitative thyroglobulin levels are not reliable.
Discussion: Recurrence is an unusual complication of PTMC. It is unusual to find cancer in FNA biopsy of LN not identified on WBS. Currently there is controversy about the use of RAI therapy in low-risk patients with PTMC, with recent recommendations favoring observation. However, some of these cancers, such as this one, present with aggressive behavior. At this moment risk factors associated with aggressive behavior have not been well defined and a consensus about post-surgical management has not been established.
Conclusion: Recurrence is a rare complication of PTMC. Accurate US imaging for long-term follow up is essential especially in patients with metastasis not identified on WBS studies. It is important to identify risk factors associated with aggressive behavior in PTMC.
Thyroid Hormone Action Thursday Poster Case Report
Resistance to thyroid hormone (RTH) is an inherited condition characterized by decreased but variable target tissue responsiveness to thyroid hormone. More than hundred different mutations of the thyroid hormone receptor β (THRβ) gene that can cause RTH have been reported to date. Typical hormone findings in RTH are elevated serum free T4 and free T3 levels with normal or slightly increased serum thyrotropin concentrations. The majority of patients are euthyroid with a generalized form of RTH and a minority of them have thyrotoxic features consistent with a less pronounced resistance at the peripheral tissue level. RTH is also associated with increased risk for autoimmune thyroid disease.
We report a new family with RTH and symptoms of hyperthyroidism. The proposita, a 23-year-old female presented with palpitations, anxiety, heat intolerance and difficulty gaining weight. Her thyroid tests showed freeT4 of 2.6 ng/dL (0.8–1.6), freeT3 of 539 pg/dL (249–405), and unsuppressed TSH of 1.6 mcIU/mL (0.3–4.7). Her mother reports having the same symptoms in the past when she was diagnosed with Graves disease and treated with propylthiouracil and then total thyroidectomy. The mother is now asymptomatic and maintained with high dose thyroid hormone. Maternal grandfather and uncle was also diagnosed with Graves disease and the uncle was treated for Graves disease with radioactive iodine ablation. The patient and her mother insist on radioactive iodine treatment for her condition. The patient has negative antibodies for autoimmune thyroid disease.
The patient and her mother were found to have a known mutation in the THRβ gene that is a nonsynonymous single nucleotide polymorphism where adenosine 1025 is replaced by thymidine. This results in the substitution of the normal Proline 247 with a Leucine. Being in the T3-binding domain of the THRβ gene, it reduces its affinity to 30% that of the normal receptor.
The patient was reassured and treated with beta blocker and they were counseled against RAI or surgery. RTH was frequently misdiagnosed and treated as Graves Disease. However, these disorders can coexist, and the concurrent presence of both disorders in a patient can present diagnostic challenge.
Thyroid Nodules & Goiter Thursday Poster Case Report
Cervical schwannomas are common but rarely present as a thyroid nodule. We report here a lesion in a multinodular goiter yielding spindle cells on fine needle aspiration (FNA).
A 60 year old woman with history of a goiter for 13 years noticed a significant increase in size of the goiter over a 3 years period and dysphagia for 1 year. She denied symptoms of hypo or hyperthyroidism. Thyroid was nodular and enlarged with retro-sternal extension. TSH=0.31 IU/dl (n: 0.34–5.6 IU/dl), TT4=10.4 mcg/dl (n: 6.1–12.2 mcg/dl).
Ultrasound guided FNA of a 4 cm hypoechoic left lobe nodule yielded cohesive spindle cells in a background of lymphocytes. On computed tomography, the thyroid was diffusely enlarged and heterogeneous. The left lobe extended to the retropharyngeal space and appeared to extend to the anterior mediastinum. The trachea was deviated to right side but remained patent. Differential diagnoses on FNA included schwannoma, melanoma, medullary (MTC) and anaplastic thyroid cancer. Immunohistochemistry was positive for S - 100 suggesting neural crest origin of the lesion. Negative staining for calcitonin, CEA, thyroglobulin, TTF1, melan A and HMB45 excluded melanoma, MTC and well differentiated thyroid cancer. Core biopsy of left lobe mass was consistent with a schwannoma. On MRI the left lobe mass was hyperintense on T2 weighted images and distinct from the thyroid. The mass extended from the skull base to the mediastinum. Intraoperatively the mass was found to be adherent to pharynx and esophagus but resectable. A subtotal thyroidectomy for multinodular goiter was performed. Resection of the intrathoracic component of the mass was deferred for future VATS. Based on operative findings, the most likely origin of the schwannoma was the pharyngeal nerve plexus. On histopathology, the schwannoma displayed spindle cells in whorls with Antoni A and B areas. The thyroid gland was diagnosed as a benign multinodular goiter.
In the evaluation of a nodular goiter with an atypical presentation, pathology arising from other structures in neck, including nerve structures should be considered in the differential diagnosis. In addition to cytology and pathology, multimodal imaging may yield helpful clues.
Friday, October 18, 2013
Autoimmunity Friday Oral Basic 5:10 PM
The TSH receptor (TSHR) has 7 transmembrane (TM) helices responsible for G protein activation. It has become clear that TM3 and TM6 form an “ionic lock” which is known to stabilize receptors in an inactive state and thus prevent major signaling initiation. Four mutations within TM3 have been reported to induce hyperthyroidism at residues 485, 501, 505 and 512 and are presumed to break the “ionic lock” releasing a signaling cascade.
Our high throughput screening (HTS) of 50,000 small molecules revealed 2 highly active compounds (437 and 438) which initiate TSHR signaling in nanomolar concentrations as evidenced by cyclic AMP generation. Molecular docking studies of these compounds revealed their binding to residues 505 (438) and 501 (437) in TM3 further confirming the concept of TM3 “hot spots” for receptor activation acting in an allosteric manner. We also know that TSHR activation follows engagement of all classes of G protein leading to thyrocyte growth and development.
To further examine the ability of these small molecules to activate G proteins we used CHO-TSHR cells transfected with bioluminescent reporter vectors with a cAMP response element (CRE-RE), a serum response element (SRE-RE), a nuclear factor of activated T-cell response element (NFAT-RE) or a mutant form of serum response factor (SRF-RE) incorporated upstream of a destabilized luciferase construct that can quantitatively measure activation of Gsα, Gβγ, Gαq and Gα12 (see Figure above). The ability of these constructs to engage the different G proteins was confirmed using TSH ligand which initiated luciferase activity tagged to activation of Gsα, Gα12 and Gαq in a dose-dependent manner. We saw no control activation of Gβγ with TSH. The small molecule agonists, which bind to the intra-helical region of TM3, when tested at 10 uM, showed activation of Gsα, Gαq and Gα12 and Gβγ with engagement of residue 501 more than with engagement of residue 505.
Differential activation of these different signaling pathways of the TSHR indicates that the TSHR response to ionic lock release may be highly variable.
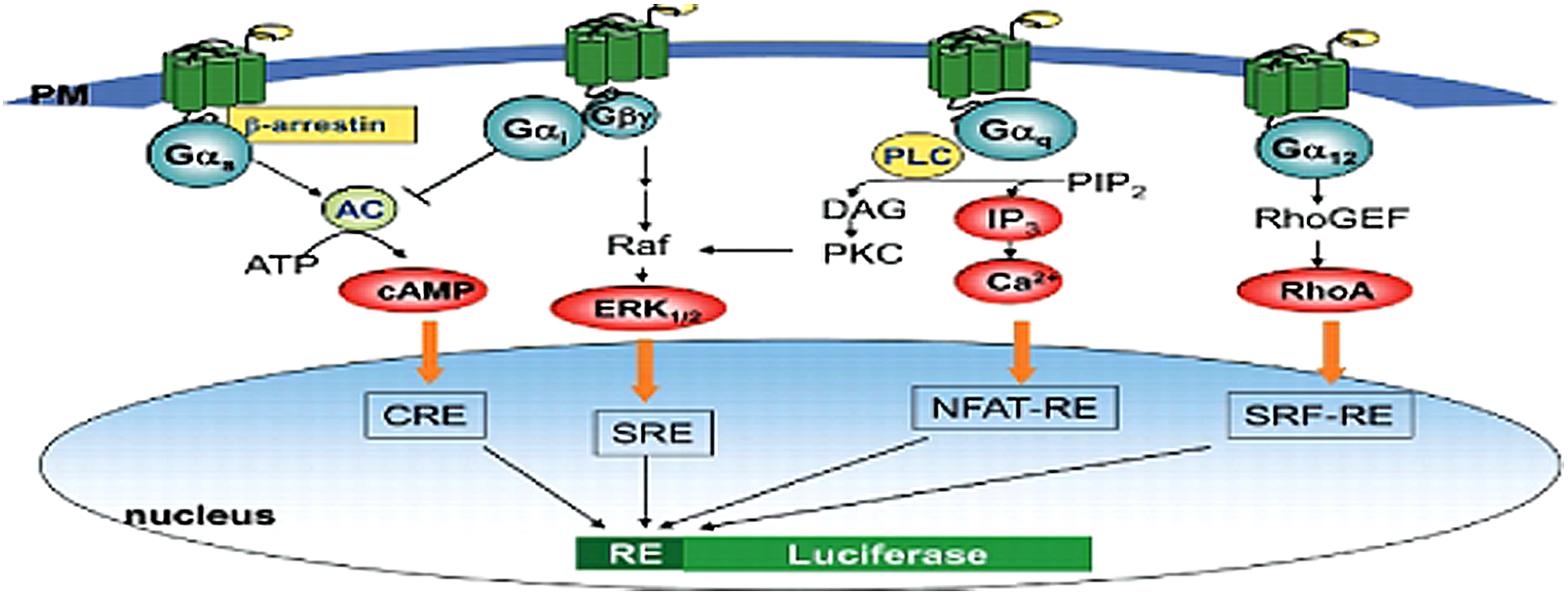
Schematic diagram showing major GPCR signaling pathways (adapted from Current Chemical Genomics, 2010, 484–91).
Autoimmunity Friday Oral Translational 5:25 PM
Graves' ophthalmopathy (GO) is an autoimmune disease of the orbital adipose tissue and extraocular muscles in which circulating thyrotropin receptor (TSHR) autoantibodies activate the receptor on orbital fibroblasts. Recent evidence suggests that ligation of the insulin-like growth factor-1 receptor (IGF-1R), perhaps by locally produced IGF-1, might also activate signaling in these cells leading to the development of GO orbital pathology. In order to better understand how these receptors might interact in this process, we silenced IGF-1R and studied signaling induced by M22, a monoclonal TSHR antibody, TSH or IGF-1 and also investigated the impact of these ligands on receptor expression.
Orbital fibroblasts from patients with GO (n=9) were subjected to IGF-1R silencing using Qiagen GeneSolution siRNA method. Untreated, control siRNA-treated and silenced cells were incubated for 30 minutes with M22 (100 ng/mL), bovine TSH (10 U/L), IGF-1 (10 nM) or IL-6 (10 ng/mL). TSHR and IGF-1R mRNA were measured using RT-PCR. pAkt and cAMP production were assessed using ELISA kits.
IGF-1R was silenced in cultures by 26.5% on average while TSHR expression was not impacted. Silencing decreased M22, TSH and IGF-1-stimulated cAMP production (34.6%; p=0.014, 26.8%; p=0.003 and 28.8%; p=0.004, respectively) relative to control siRNA cultures. Similarly, M22 and IGF-1-stimulated Akt phosphorylation was reduced (28%; p=0.008 and 45.2%; p=0.004, respectively) in IGF-1R silenced cultures. Treatment of cells with M22, TSH or IGF-1 increased both IGF-1R mRNA (1.4 fold; p=0.03, 1.7 fold; p<0.001 and 1.3 fold; p=0.003, respectively) and TSHR mRNA expression (2.6 fold; p=0.005, 2.3 fold; p=0.008 and 2.2 fold; p=0.001, respectively). IL-6 treatment increased only TSHR expression (1.8 fold; p=0.047).
These results suggest that TSHR and IGF-1R cross-communication may play a role in GO pathogenesis. Whether the receptors are transactivated and/or their signaling networks integrated awaits further study.
Autoimmunity Friday Oral Translational 5:40 PM
Persons with positive thyroid peroxidase antibodies (TPOAbs) have an increased risk of developing autoimmune thyroid disease (AITD), including Hashimoto's hypothyroidism and Graves' hyperthyroidism. The genetic basis of TPOAbs and AITD remains largely unknown and neither is it known why only part of the TPOAb-positive persons develops AITD. We therefore performed a genome wide association study for TPOAbs.
The effects of 2.5 million polymorphisms on the risk of TPOAb-positivity and TPOAb levels were studied in 18,300 persons from 11 populations, and replicated in 9,000 persons from 5 independent populations (significance threshold: P<5×10−8). We subsequently studied the effects of these significant polymorphisms on the risk of hypo- and hyperthyroidism. These effects were also studied in 859 pregnant women, as thyroid hormone metabolism significantly changes during pregnancy.
Significant associations were detected at TPO, ATXN2, and BACH2 for TPOAb-positivity, and at TPO, MAGI3, and KALRN for TPOAb levels (all P<5×10−8). The MAGI3 and BACH2 polymorphisms were associated with an increased risk of hypothyroidism (OR=1.57, P=1.9×10−3 and OR=1.37, P=0.05), and Graves' hyperthyroidism (OR=1.37, P=1.2×10−7 and OR=1.25, P=6.2×10−5). A lower risk of suppressed TSH levels (OR=0.82, P=0.01) was found for the KALRN polymorphism. No associations with hypo- or hyperthyroidism were found for the TPO and ATXN2 polymorphisms. In pregnant women, carriage of multiple risk alleles was associated with an increased risk of TPOAb-positivity, but none were associated with hypo- or hyperthyroidism.
We identified five novel genetic loci associated with TPOAbs, and found that in non-pregnant populations the MAGI3, BACH2 and KALRN polymorphisms were also associated with thyroid disease. In contrast, the TPO and ATXN2 polymorphisms were not associated with thyroid disease. These data provide insight into the genetic basis of AITD and as to why only part of the TPOAb-positive persons develops clinical thyroid disease.
Thyroid Hormone Metabolism & Regulation Friday Oral Basic 5:55 PM
The global D2 KO mouse (D2KO) exhibits increased tolerance to glucose and, when on a high fat diet, exhibits liver steatosis and resistance to diet-induced obesity. D2KO animals also exhibit a lower exchange respiratory ratio (RQ) reflecting accelerated fatty acid oxidation, a difference that is dissipated by acclimatization to thermoneutrality.
To define the specific role played by D2 in brown adipose tissue (BAT), we created a mouse with adipose-specific disruption of D2 (FAT-D2KO) by crossing the flox-D2 mouse with the AP2-Cre mouse.
FAT-D2KO animals are grossly normal and systemically euthyroid, but exhibit a ∼65% decrease only in BAT D2 activity. FAT-D2KO have normal BAT UCP1 mRNA (1±0.23 vs. 0.87±0.28; n=12) and defend core temperature normally when at 4°C for 12 h. Despite similar VO2 (5.2±0.7 vs. 5.1±0.4 mlO2/h•g BW), FAT-D2KO have elevated RQ (0.77±0.02 vs. 0.82±0.02; n=4–6; p<0.01; experiment repeated 3x), reflecting accelerated rate of glucose oxidation. In fact, FAT-D2KO animals have increased expression of GLUT4 in BAT (1±0.16 vs. 1.27±0.38; n=12; p<0.05) and in clearance of plasma glucose (34.7±5.7 vs. 25.9±0.84 mg/dl•min, n=12–15; p<0.05) after insulin injection. FAT-D2KO animals have similar body composition by DEXA but are more susceptible to diet-induced obesity caused by high fat diet, gaining more body weight (44.7±0.56 vs. 51.1±1.7 g/day; n=6; p<0.05) and body fat (13.2±3.5 vs. 19.2±5.0% fat) when compared to littermate controls; FAT-D2KO animals never developed liver steatosis. Notably, the metabolic phenotype of the FAT-D2KO mouse was dissipated by acclimatization at thermoneutrality, a condition that minimizes BAT activity.
In conclusion, the metabolic phenotype attributable to a selective D2 inactivation in BAT includes accelerated rate of glucose oxidation (and decrease fat oxidation), what probably explains the greater susceptibility to diet induced obesity.
Thyroid Hormone Metabolism & Regulation Friday Oral Basic 6:10 PM
TSH activates the TSH receptor (TSHR), a member of the family of seven-transmembrane spanning receptors (7TMRs), thereby stimulating the function of thyroid follicular cells leading to biosynthesis of thyroid hormones. Recent studies have demonstrated that the metabolic effects induced by 7TMRs are not entirely a consequence of signaling mediated through G-proteins. β-Arrestins, in addition to their 7TMR desensitizing actions, also serve as multifunctional scaffolding proteins for activation of several, G-protein-independent signal transduction pathways. There are two isoforms, β-arrestin 1 and 2, that have some overlapping and some distinct functions. TSHR has been found to activate/phosphorylate the mitogen-activated protein kinases, ERK1/2, p38α, and Akt. To our knowledge, this is the first report describing β-arrestin mediation of these pathways in TSHR signaling.
TSHR binding to β-arrestins was measured with the PathHunter™ β-Arrestin Assay (DiscoveRx). Phosphorylation of protein kinases was detected with ELISAs. To determine the role of β-arrestin 1 and 2 in TSHR signaling, we knocked down both β-arrestins individually with siRNA.
We showed that the activated human TSHR can bind to and translocate both β-arrestin 1 and 2. We confirmed that TSHR activation leads to phosphorylation of ERK1/2, p38α and Akt in HEK cells that stably express the TSHR, but also in primary cultures of human thyrocytes, suggesting that these pathways are important in thyroid physiology. We showed that phosphorylation of ERK1/2, p38α and Akt is mediated in part by β-arrestins. For TSHR activation of ERK1/2 and Akt, β-arrestin 1 activates and β-arrestin 2 inhibits phosphorylation whereas for p38α, β-arrestin 1 activates but β-arrestin 2 appears to have no effect.
We have shown that β-arrestin 1 is required for TSHR-mediated phosphorylation of Akt, p38α and ERK1/2 and, therefore, β-arrestin 1 in part mediates TSHR-signaling. β-arrestin 2 inhibits TSHR signaling consistent with its role in desensitization of TSHR. Future studies will address the physiological role of β-arrestin 1-mediated pathways in thyrocytes, but also in extrathyroidal tissue, e.g. in orbital fibroblasts from patients with Graves' disease and in bone cells.
Thyroid Hormone Action Friday Oral Basic 6:25 PM
It has been shown previously that triiodothyronine (T3) acts on posttranscriptional steps of beta TSH synthesis and reduces the TSH secretion when acutely administered to thyroidectomized rats. In this study we investigated whether these effects on posttranscriptional steps of beta TSH also occur in TalphaT1 cells, a tumor thyrotrophic cell line, independently of gene transcription, as well as, the possible repercussions of T3 on TSH secretion in primary culture of anterior pituitary cells.
TalphaT1 cells were seeded on matrigel-coated plates in two groups: Control (C), cultured in medium containing 10% FBS and Hypothyroid (H), cultured in medium containing 10% FBS depleted of thyroid hormones by treatment with AG1X-8 resin for 48 h. After this, 5,6-dichloro-1-β-D-ribobenzimidazole (DRB - 50 mM) was administered for 2 h to inhibit the gene transcription, followed by the T3-treatment in the doses of 10 nM or 0.1 nM for 30 min or 0.1 μM for 4 h. Total RNA and the polysomes fraction were extracted for the investigation of Tshb and Cga mRNA by RT/qPCR and the degree of adenylation by RACE-PAT assay, respectively. Primary anterior pituitary cells were isolated and cultured with FBS treated with charcoal (Basal) in the presence or absence of T3 (10 nM) for 30 min.
The results obtained with TalphaT1 cells showed that T3 rapidly reduced the total content of Tshb and Cga mRNAs, and the reduction was maintained only for Tshb mRNA after DRB treatment. Moreover, it was shown that the T3 (0.1 nM) specifically decreased the poly(A) tail length of Tshb mRNA and the content of mRNA of both subunits associated with ribosome, which indicates that the translational rate of TSH synthesis was reduced. In parallel, T3 increased the content of TSHB and CGA (alpha subunit) in intracellular extracts of primary anterior pituitary cells while the amount of TSH in extracellular media was reduced.
These results led us to the conclusion that T3 down-regulates TSH synthesis and secretion in several posttranscriptional steps, characterizing novel actions of T3 on its own regulatory axis.
Thyroid Cancer Friday Oral Clinical 5:10 PM
The limited efficacy of cytotoxic chemotherapy (chemo) has led to a paradigm shift in the treatment of advanced differentiated thyroid cancer (DTC). Practice guidelines recommend sorafenib (SOR) as one potential treatment of progressive DTC. The rare subpopulation of patients with poorly differentiated thyroid carcinoma (PDC) has not been independently studied. Thus, we sought to describe the outcomes of PDC patients treated with SOR.
After IRB approval, pathologically confirmed adult PDC patients treated with 1st line SOR were reviewed retrospectively. We used patients on 1st line cytotoxic chemo as a comparator arm. All cases were reviewed and diagnosed by a head and neck pathologist as PDC. Overall survival (OS) after starting systemic therapy, progression free survival (PFS) and overall best response data (as determined by RECIST 1.1) were gathered. The radiologist was blinded to treatment assignment.
From 1994 to 2012, 48 patients were treated with either SOR (n=23) or cytotoxic chemo (n=25). Five patients were excluded (2 SOR and 3 chemo) due to missing data (2), neoadjuvant chemo (1), anaplastic cancer at metastatic site (1) and concomitant unrelated cancer (1). Baseline demographics were similar between the SOR and chemo groups, including time from diagnosis to treatment and sites of metastatic disease. Median OS in SOR treated patients was 34 months vs. 9 months in chemo treated (p=0.026, figure 1a). Best response in SOR: 3/13 (23%) partial responses (PR), 8/13 (62%) stable disease (SD) and 2/13 (15%) progressive disease (PD). Best response in chemo: 1/8 (12.5%) PR, 4/8 (50%) SD, 3/8 (37.5%) PD (figure 1b). PFS to 1st line treatment was significantly longer in the SOR cohort (median 9 vs.3 months, p<0.01).
This is the first study to describe the efficacy of SOR in the subpopulation of PDC patients. Although this is a small cohort, 85% of patients derived clinical benefit (PR+SD) from SOR, similar to the published data in DTC. Acknowledging that a selection bias may be present, we conclude that PDC patients should receive 1st line SOR as it does not appear inferior to chemo.

Thyroid Cancer Friday Oral Clinical 5:25 PM
SOR is a common 1st line therapy in advanced DTC. Phase 3 results showed a progression free survival (PFS) advantage of 5 months in TKI naive patients. However, responses are not durable and toxicity remains a problem. Median overall survival (mOS) has not been reached. Furthermore, there is no data on OS and efficacy of salvage TKIs after 1st line SOR failure.
This is a retrospective review of DTC patients who received 1st line SOR only (group 1) or with subsequent salvage TKI treatment (group 2). The end points were to assess mOS in all patients treated with 1st line SOR, to compare mOS in group 1 and group 2, and to assess PFS and response rate with 1st line SOR and 2nd TKI. RECIST v1.1 was used to determine best response.
We included 60 metastatic, RAI refractory DTC patients: median age at diagnosis 54, 52% male, 63% papillary, 30% follicular, 7% poorly differentiated carcinoma; 97% lung and 35% bone metastases at the time of SOR start. Group 1 and group 2 included 35 and 25 patients, respectively and were well balanced. 2nd TKI included sunitinib (10), pazopanib (4), cabozantinib (4), lenvantinib (4), vemurafenib (3). The mOS of all 60 SOR-treated patients was 41 months. The mOS was significantly longer with salvage TKI compared to SOR alone (63 vs 24 months, p=0.013) (Figure 1). In group 2, 17 patients were evaluable for response. Two patients had toxicity with SOR leading to drug discontinuation before restaging. Best response with 1st line SOR: partial response (PR) 1/15 (7%), stable disease (SD) 11/15 (73%), progressive disease (PD) 3/15 (20%) and 2nd TKI: PR 7/17 (41%), SD 10/17 (59%). All 3 patients with PD on SOR achieved PR on 2nd TKI (>55% reduction). 2 patients who stopped SOR due to toxicity tolerated and responded to a 2nd TKI (1 SD, 1 PR). The median PFS was 10 months with 1st line SOR and 12 months with 2nd TKI.
The mOS of TKI naive DTC patients treated with SOR is 3.5 years. Although not directly comparable, patients able to receive salvage TKIs following SOR failure appear to extend their mOS from 2 to 5 years. Importantly, SOR failure did not predict response to salvage TKIs despite similar mechanisms of action. The current standard should be to offer salvage targeted therapy to these patients.
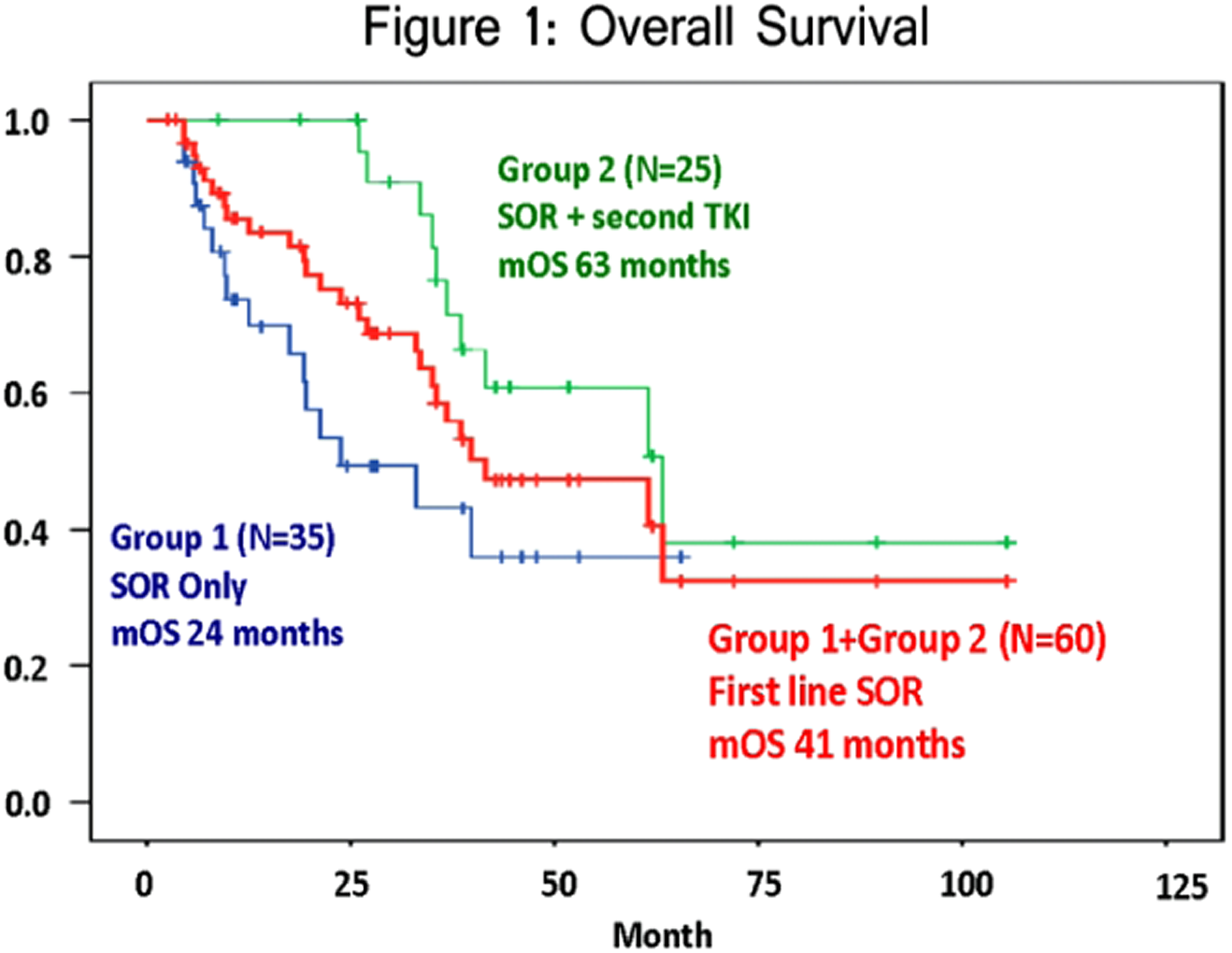
Thyroid Cancer Friday Oral Clinical 5:40 PM
ATA guidelines advise against routine use of postoperative radioactive iodine (RAI) for very low-risk papillary thyroid cancer (PTC), defined as subcentimeter intrathyroidal tumors. Patterns of RAI administration for low-risk PTC vary dramatically across the US, for unclear reasons. We analyzed the association between regional access to healthcare and the pattern of RAI use for very low risk PTC.
We analyzed 13,401 cases of very low risk (defined as ≤1 cm intrathyroidal N0 M0) classical PTC undergoing total thyroidectomy in 337 US counties (1983–2009), in the SEER 18 cancer registry. Aggressive variants of PTC were excluded. County-level access to healthcare was estimated from 8 socioeconomic factors: percentage of county population uninsured, poor, unemployed, white collar employed, non-English speaking, high school educated, college educated, and mean family income. The association between access to care and the probability of RAI use for very low risk PTC was examined using weighted-least squares regression.
During the study period, 32.9% of very low risk PTC patients received postoperative RAI. This proportion was stable between 1990 and 2009, hovering between 30–36%. The proportion was similar (27.9%) when limited to unifocal very low risk PTC. Counties were ranked by socioeconomic factors, and RAI use was more common in the lowest decile, compared to the highest decile (42.0% vs 29.8%, p=.04). The 8 socioeconomic factors together explained 16.7% of the variability in county-level use of RAI for very low risk PTC (r=.41, p<.001). Counties with higher use of RAI had significantly lower levels of income, education and white collar employment, and higher levels of uninsured, non-English speaking, and poor persons.
In the US, RAI is overutilized in very low risk PTC patients, with over 30% of these patients receiving RAI. Levels of access to healthcare are strongly associated with the probability of RAI treatment. Overuse is most frequent in counties with poorer access to healthcare. This association is likely to be multifactorial, possibly attributable to diminished access to experienced specialists resulting in more widespread use of RAI in very low risk patients.
Thyroid Cancer Friday Oral Translational 5:55 PM
Cystic papillary thyroid cancer (cPTC) is a type of well-differentiated PTC exhibiting classical histopathological features, but different morphological properties due to its common presentation as mural nodule in thyroid cystic mass. The diagnosis of cPTC is challenged, because the fine needle aspiration biopsy usually reveals sufficient volume of cystic fluid, but insufficient amount of representative follicular cells resulting in low-informative cytological reports. The aim of this study was to identify potential diagnostic markers for discrimination between cPTC and benign cystic thyroid neoplasms.
We identified 121 patients who were surgically treated for cystic thyroid neoplasms and the cystic fluid from these cases was collected from post-operative specimens. A 14 cases (7 cPTC, 7 cystic benign thyroid lesions) were selected for proteomics profiling by liquid chromatography tandem mass spectrometry (LC MS/MS). The depletion was performed to remove highly-abundant proteins. The depleted samples were digested, labeled by iTRAQ reagents and pooled into one tube, underwent isoelectric focusing. LC MS /MS was performed on a hybrid LTQ-Orbitrap Velos mass spectrometer. The obtained data was searched by Sequest under the software platform Proteome Discoverer, followed by uni- and multivariate statistical analyses. Immunohistochemistry (IHC) was performed to evaluate the immunoexpression of selected proteins.
Out of all 1581 identified proteins, 841 contained labels in both iTRAQ pools. Of these, 87 proteins were differently expressed in cPTC as compared to control samples by Student's t-test, whereas multivariate OPLS model revealed 41 proteins (p<0.05). Of these, annexin A3 (ANXA3), S100A13, carboxymethylenebutenolidase (CMBL), cytokeratin 19 (CK-19) were selected for evaluation by IHC. ANXA3, S100A13, CMBL showed overexpression in both controls and cPTCs, whereas CK-19 was up-regulated in cPTC only (p<0.05).
To our knowledge this is the first extensive catalogue of the protein content in fluid from the thyroid cystic neoplasms. An overexpression of CK-19 in cPTC fluid supports its possible role as a preoperative diagnostic marker. Additional experiments are needed to validate LC MS/MS and IHC findings.
Thyroid Cancer Friday Oral Clinical 6:10 PM
The DECISION trial (NCT 00895674) was the first placebo-controlled phase III study of RAI-refractory DTC patients. While sorafenib significantly improved progression-free survival, here we sought to better understand the impact of disease burden and sorafenib therapy on the health-related quality of life (HRQoL) in RAI-refractory DTC patients using validated questionnaires.
A total of 417 patients with RAI-refractory DTC who progressed in the preceding 14 months were randomized 1:1 to sorafenib or placebo; n=207 and 210, respectively. HRQoL was measured using the FACT-G questionnaire, a validated tool tracking the physical, social/family, emotional and functional well-being of cancer patients. General health status was measured using the EQ-5D index questionnaire and visual analogue scale (VAS). Questionnaires were self-administered at baseline and day 1 of every 28-day cycle.
Questionnaire completion during study was 96%. Patients had FACT-G scores at baseline comparable to a normative adult cancer population: placebo 82±14 (mean±SD) and sorafenib 81±15 (with 108 being the maximal score possible). The sorafenib group had a lower score at first assessment (cycle 2, day 1; 76±15), possibly related to side effects of treatment, but remained relatively constant thereafter, while the placebo group remained near baseline. A mixed linear model estimated that the FACT-G score was 3.45 points lower in the sorafenib group (p=0.0006). For the EQ-5D tool (both index and VAS), the pattern was very similar to that seen with the FACT-G. Although statistically significant (p<0.0001 for both), the treatment effect (−0.07 and −6.75, respectively) was of a small magnitude.
Compared to placebo patients, patients in the sorafenib treatment arm had lower on-treatment scores for the FACT-G, EQ-5D Index and EQ-5D VAS. All three group differences were small, suggesting a mild but detectable impact of sorafenib therapy on HRQoL in favor of the placebo arm.
Thyroid Cancer Friday Oral Translational 6:25 PM
The assessment of thyroid nodules is still a common clinical problem. Thyroid fine needle aspiration (FNA) is the standard preoperative tool for diagnosis of thyroid nodules. However, the limitation of this procedure consist in the high rate of indeterminate or suspicious cytological diagnosis which lead to unnecessary surgical intervention. A number of studies have shown that molecular testing of FNA specimens can significantly improve the accuracy of the preoperative FNA diagnosis and the use of molecular marker is now recommended in the American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer. However, there are many molecular markers to test, which can require a large amount of DNA, is time consuming, and expensive.
In this study we evaluated the benefits of next generation sequencing (NGS) for helping diagnosis of FNA samples. We retrospectively analyzed 30 indeterminate or suspicious FNA samples for which surgical resection was performed; histological diagnosis being considered as gold standard. DNA from these 30 samples was obtained either from cell block of from Diff-Quick stained smear and subjected to targeted NGS with the Ampliseq Cancer Hotspot Panel, which allowed us to analyze 2850 known cancer-related mutations.
Mutations in BRAF, NRAS and KRAS that are known to be involved in thyroid cancer biology were detected in malignant FNA samples. None of these mutations were detected in the benign samples. Moreover NGS allowed us to detected in the same experiment other rare and low frequency mutations in p53, AKT1 and STK11.
This study demonstrate that thyroid FNA specimens can be successfully analyzed by NGS. The detection in these specimens of different mutations known to be involved in thyroid carcinoma biology can improve sensitivity of the diagnosis in thyroid FNA samples.
Autoimmunity Friday Poster Translational
Graves disease (GD) is rare in children and is seldom accompanied with extrathyroidal manifestations. Scarce data are available regarding the role of TSH receptor (TSHR) stimulating autoantibodies (TSAb) in pediatric GD. Thus, in this large multicenter trial, the clinical relevance of TSAb is evaluated in GD children with and without orbitopathy (GO).
TSAb levels were measured with a bioassay that uses a chimeric TSH-R and a CRE-dependent luciferase. TSAb results were expressed as percentage of specimen-to-reference ratio (SRR %). Values ≥140% were considered positive. All samples were also measured for TSHR binding inhibiting immunoglobulins (TBII, automated ECLIA assay). Clinical severity of GO was defined according to the consensus statement and recommendations of the European group on Graves' orbitopathy (EUGOGO).
A total of 372 sera samples were obtained from 156 GD children (124 female, mean age±SD 13.6±4.4 years, 66 children with GD/GO showing proptosis, lid retraction, lid swelling, lid erythema and conjunctivitis), 50 with type 1 diabetes (T1D, 13.69±3.7 yrs.), seven with non-autoimmune hyperthyroidism (NAH, 12±8.2 yrs), five with juvenile arthritis (JA, 14.3±3.4 yrs) and from 50 euthyroid healthy controls (12.4±4.3 yrs.). TSAb and TBII were detected in 240/255 (94%) and 226 (89%) samples, respectively (p<0.001). In 97 untreated children, TSAb and TBII were present in 97 (100%) and 91 (94%) samples, respectively (p<0.001). In line with this, TSAb and TBII were present in 100% and 93% samples of treated children with GD/GO (p<0.001). Also, median TSAb levels were markedly higher in untreated children with GD/GO vs. those with GD, only (SRR% 482 vs. 404, p=0.001). During antithyroid drug treatment, children with GD/GO who became euthyroid still had very high median TSAb levels compared with children with GD, only (SRR% 465 vs. 291, p<0.001). Neither age nor gender had an impact on TSAb values. All controls and children with NAH (SRR% 37±3.8), T1D (46±2.1) and JA (39±1.8) were TSAb and TBII negative.
Serum TSAb levels are a biomarker of disease severity and extrathyroidal manifestations in pediatric GD.
Autoimmunity Friday Poster Clinical
Over the past decade several clinical studies have suggested that selenium supplementation may influence the natural course of autoimmune thyroiditis (AIT). The aim of this randomized, placebo-controlled, prospective study was to evaluate the effect of 2 different doses (80 or 160 μg) of selenomethionine (semet) versus placebo in euthyroid female patients with AIT, in terms of anti-thyroid antibody reduction and thyroid hypoechogenicity improvement, over a period of 12 months.
Sixty patients, aged 21–65 years, were randomly divided in 3 groups according to the treatment modality: 80 μg of semet (80-semet), 160 μg of semet (160-semet) or placebo. AbTPO/AbTg and thyroid hypoechogenicity, by grayscale method, were measured basally and every 3 months. Serum selenium, CXCL9 and CXCL11 levels were evaluated basally and every 6 months.
Preliminary data are available at 3 month-follow-up and in a subgroup of patients at 6 months. Compared to basal values: AbTPO levels were slightly increased in the placebo group, while they were unchanged in the 2 semet groups; AbTg levels decreased in the 160-semet group (from a median of 181.5 U/ml to 102.5 U/ml, p=0.02) at 3 months and showed a further decrease (−9.75%) at 6 months while they did not show any change in the placebo and 80-semet groups; there was no change in thyroid function and grayscale value in any of the 3 groups. No side effects were reported.
Both 80 and 160 μg semet supplementations are well tolerated and may prevent as soon as 3 months, an increase of AbTPO levels in euthyroid AIT patients; 160 μg dose was also able to reduce AbTg values compared to basal levels at 3 months and even more at 6 months. On the other side thyroid function and hypoechogenicity were not affected by 6 month-semet supplementation. The optimal semet dose and duration of supplementation needs to be ascertained over the remaining study follow-up.
Autoimmunity Friday Poster Clinical
The aim of this study was to evaluate the relationships between lipid-carbohydrate metabolism parameters and thyroid hormones and autoantibodies and carotid intima-media thickness (CIMT) in children and adolescents with autoimmun thyroiditis (AIT) during the follow up.
We examined 60 patients with the diagnosis of AIT aged range between 9–19 years (10 male, 50 female), based on examination of autoantibodies (anti-TPO and anti-Thyroglobulin) and thyroid ultrasonography (USG). Oral glucose tolerance test (OGTT) was performed to all patients. Hepatic steatosis and CIMT using B-Mode USG, and lipid profile were evaluated in all patients. All procedures were performed to patients during the follow-up. Body mass index (BMI) was calculated as a kg/m2. Insulin sensitivity was evaluated by homeostasis model assessment (HOMA-IR).
Mean duration of diagnosis was 24.76±22.38 months. Frequency of overweight and obesity were 22.4%. Hepatic steatosis is only present in 3.2% of the patients. BMISDS at the diagnosis, insulin levels at 30th minute and totally insulin levels in OGTT were higher in overweight and obese children and adolescents with AIT compared with non-obese subjects with AIT (p=0.003, 0.026 and 0.04, respectively). In these patients, anti-TPO levels was lower in overweight and obese subjects compared with non-obese subjects (p=0.031). Thyroid stimulating hormone (TSH) and FT4 levels were significantly changed during follow-up (p<0.05, paired sample test). The Pearson correlation coefficient indicated that anti-TPO level at the time diagnosis was positively correlated with HOMA-IR (r=0,37 p=0.008).
Overweight and obesity are common among children and adolescents with AIT. Elevated insulin levels are highly prevalent in overweight and obese children and adolescents with AIT. Insulin sensitivity may be related with anti-TPO levels at time of diagnosis.
Disorders of Thyroid Function Friday Poster Clinical
To analyze the pregnancy outcomes among women with Graves' disease after radioactive iodine therapy and evaluate the influence on the fertility as well as the health status of their births.
We followed a total of 102 female patients who suffered from Graves' disease and kept on the treatment, recorded their pregnancy outcomes during 2009∼2012. Among the pregnant women were classified into two groups: receiving 131I therapy before pregnancy and receiving ATD treatment. During the pregnant period, we monitored closely about the thyroid function to adjust the drug dose and then recorded the health condition of the newborns also the cases about termination of pregnancy. Medication compliance, delivery mode, baby gender and weight were statistically analyzed.
Among the 102 cases, there were 86 women with drug pregnancy and the other 16 without medication during pregnancy; 97 normal deliveries and 5 abortions; 90 term deliveries and 7 premature births; 50 baby boys and 47 baby girls; 86 normal weight babies and 11 abnormal weight babies. The 131I treatment group compared with the ATD treatment group, medication compliance, delivery mode, baby gender and weight were similarity and the difference was not significant.
Women of reproductive age with Graves' disease can choose to pregnant after 131I therapy for at least 6 months later. People can achieve the purpose of giving a good birth as long as their thyroid function kept checking routinely before and during pregnancy period and at the same time rational drugs used to control or maintain the thyroid function normally.
Disorders of Thyroid Function Friday Poster Clinical
Hypoparathyroidism is a rare endocrine disorder caused by insufficient or absent parathyroid hormone, leading to hypocalcemia and hyperphosphatemia. The PARADOX study aimed to quantify clinical, social, and economic impacts of hypoparathyroidism from the affected patients' (pts) perspective.
Pts aged ≥18 y and diagnosed with hypoparathyroidism ≥6 months ago completed a 30 min self-reported, web-based survey.
374 US adults (mean age, 49 y; women, 85%; mean disease duration, 13 y; severe disease, 31%) completed the study. Pts reported visiting a mean of 6 physicians before and after diagnosis. Nearly half of the pts (48%) strongly agreed to feeling mismanaged at diagnosis, and 79% strongly agreed that most physicians do not understand hypoparathyroidism. Pts visited their current managing physician (endocrinologist, 72%; primary care physician, 21%) a mean of 4 times/y. The majority strongly agreed that they felt unprepared to manage the condition at diagnosis (56%), that controlling their hypoparathyroidism is harder than expected (60%), and that they were concerned about long-term complications of their current medications (75%). Despite current management regimens, 72% experienced >10 symptoms in the preceding 12 months, for a mean of 13 hours/d. Physical symptoms reported by >75% of pts were fatigue (82%), muscle pain/cramping (78%), and paresthesia (76%). Comorbidities were experienced by 259 pts (69%), the most frequent being cardiac arrhythmias (66%) and kidney stones (36%). Hospital or emergency room visits because of hypoparathyroidism were reported by 79% of pts. In addition, 45% reported significant interference with daily life, 85% reported an inability to perform some household activities, and 20% experienced a disease-associated change in employment status.
To our knowledge, this is the largest and most comprehensive study conducted to assess the impact of disease in pts with hypoparathyroidism. Despite the current standard of treatment (oral calcium and active vitamin D), pts with hypoparathyroidism have a high burden of illness and experience a broad spectrum of symptoms, with multifaceted effects on their lives.
Disorders of Thyroid Function Friday Poster Clinical
Thyroid hypofunction may adversely affect pregnancy outcomes. Recommendations for thyroid function testing and management of subclinical hypothyroidism and hypothyroxinemia in pregnancy are not in agreement. We aimed to determine current practice patterns among thyroidologists who care for pregnant women to understand how guidelines are being implemented.
An anonymous multiple-choice survey was distributed at the 2012 ATA meeting. Respondents were asked whether or not to test for thyroid dysfunction or treat hypothyroidism/hypothyroxinemia given different clinical scenarios. Responses were compared across different provider demographics using ANOVA.
There were 151 survey respondents. 91% were endocrinologists and 40% had been in practice ≥20 yr. 40% of respondents saw 1–10 pregnant women annually, 34% saw 11–40, and 16% saw >40. 75% had read the 2011 ATA thyroid in pregnancy guidelines and 68% had read the 2012 Endocrine Society guidelines. 74% advocated for and 18% against universal TSH screening in pregnancy; 8% were unsure. 100% advocated thyroid testing in pregnant women with hypothyroid symptoms or family history of Graves' disease and 99% advocated testing in those with goiter. 46% recommended thyroid hormone treatment for a TPOAb negative pregnant woman with TSH 3.5 mU/L; 86% would treat this patient if she were TPOAb positive. 97% would treat for a TSH of ≥8.0 mU/L in pregnancy. 26% would treat isolated maternal hypothyroxinemia in a TPOAb negative woman, and 51% would treat if the woman were TPOAb positive. Provider demographics did not predict survey responses.
Most thyroidologists surveyed favored universal thyroid function testing in pregnancy. Thresholds for treatment of mild maternal hypothyroidism were variable. There was no correlation between provider demographics and survey responses.
Disorders of Thyroid Function Friday Poster Clinical
We sought to determine the prevalence of post-surgical hypothyroidism in patients undergoing thyroid lobectomy for benign disease, and to identify the appropriate time interval in TSH surveillance.
Patients who underwent lobectomy between 01/2005 and 12/2011 were identified; pertinent data were obtained through a retrospective review of the electronic medical record system.
Three hundred and seventeen patients underwent thyroid lobectomy for benign disease. As per surgeon preference, 131 patients (41%) were placed on prophylactic levothyroxine (LT4) immediately after surgery. The remaining 186 patients were followed for a median of three years and were placed on LT4 when their TSH levels were elevated beyond the normal range. Using Kaplan Meier analysis, the prevalence of new onset hypothyroidism was 14% by 6 weeks, 32% by six months, and 40% by one year. Fifty-nine patients were on LT4 at one year postoperatively, only an additional 6% (n=6) developed hypothyroidism after that. Neither preoperative TSH levels (p=0.09) nor evidence of chronic lymphocytic thyroiditis (p=0.2) were significant predictors for development of hypothyroidism. For patients not placed on LT4 (n=54) during the study period, 45% had final postoperative TSH levels that were at least one point above their preoperative levels, and 18% had final TSH levels that were >3.5 (normal 0.45–5.5 mIU/L). In comparison, only 15% of the patients who were placed on LT4 prophylactically had final TSH levels that were one point above their preoperative levels, and only 9% had levels that were >3.5 mIU/L.
With longer follow up, the prevalence of post-surgical hypothyroidism may be higher than previously reported. This is especially true when taken into account the patients who exhibited “relative hypothyroidism” but were never placed on LT4 because their TSH levels were within the “normal range”. This study suggests that patients with “relative hypothyroidism” may have benefited from LT4 therapy. Furthermore, we recommend checking TSH levels at more frequent intervals within the first year after surgery to ensure that hypothyroidism can be treated promptly.
Disorders of Thyroid Function Friday Poster Clinical
Thyroid hormones are well known to regulate metabolic parameters in the physiologic state. We were interested in exploring the relationship that the hypothyroid state has on the occurrence of the metabolic syndrome and on the metabolic parameters of the metabolic syndrome.
Methods: This is a retrospective case control study to compare the prevalence of the metabolic syndrome between euthyroid and hypothyroid subjects. We analyzed 149 subjects in total, 39 euthyroid and 110 hypothyroid subjects. Metabolic Syndrome was defined as per ATPIII criteria. All data were collected through chart review. Statistical analysis was performed by the Chi-square test and logistic regression analysis.
Results: The euthyroid and hypothyroid groups were found to be similar in terms of demographic variables including age, gender, smoking status, alcohol consumption. We found that 28.2% of the euthyroid and 51.8% of hypothyroid subjects had the metabolic syndrome. Statistical analysis revealed an Odd's ratio of 2.6 (CI 1.5 to 5.7) with a P-Value of 0.01. The groups did not significantly differ in the prevalence of any single component of the metabolic syndrome, namely glucose tolerance, blood pressure, body mass index, HDL cholesterol or triglyceride levels, though a uniform trend of increased prevalence among the hypothyroid group was seen. Subset analysis revealed a higher mean TSH among those with the metabolic syndrome as compared to those without, in both the euthyroid and hypothyroid groups.
Conclusion: Our study suggests that hypothyroid subjects are at about 2 to 5 fold increased risk for metabolic syndrome independent of age, gender, smoking status and alcohol intake. This may contribute to the association of ischemic heart disease and hypothyroidism. Further research is needed to evaluate the timing and the cost-effectiveness of routine screening of hypothyroid patients for the metabolic syndrome, the effect of thyroid hormone replacement on the metabolic parameters and the target TSH level in hypothyroid individuals with metabolic syndrome.
Disorders of Thyroid Function Friday Poster Clinical
The key role of an intact gastric acid secretion for subsequent intestinal T4 absorption is supported by biochemical and clinical evidence. Characteristic of several gastric disorders is an increased gastric pH. To note, softgel thyroxine preparation showed a better dissolution profile than T4 tablets under increased medium pH, in vitro. Thus, in patients with gastric disorders, softgel capsules of T4 may help to improve the therapeutic efficacy. Our study was aimed at comparing softgel and tablet T4 requirement in these patients.
Patients enrolled had gastric-related T4 malabsorption, were in long-lasting T4 tablets treatment (same brand) and showed a stable serum TSH (>2 yrs). All patients had been advised and agreed to take oral thyroxine under fasting conditions, waiting at least one hour before eating. Patients bearing additional conditions known to interfere with thyroxine treatment were excluded from the study. A total of 36 patients met these criteria, but only 30 of them (28 F/2 M; median age=51 years; median T4 dose=2.05 μg/kg/day) completed the study. In these patients T4 treatment was switched from the tablet to a lower dose of the softgel T4 capsules (median T4 dose=1.77 μg /kg/day; −16%; p=0.0082). Assessment of FT4 and serum TSH was carried out before (0 time) and after 3,6,12 and 18 months from the treatment switch.
In the whole sample, a slight increase in mean serum TSH has been observed after 3 months of treatment, with no change in FT4 levels. However, once subdivided according with a tertile distribution, two clearly different groups appeared. In more than 2/3 of patients (responders n=21), despite the reduced dose of T4, mean TSH values after 3 months were similar and so remained until the end of the study (p=0.6491). In the remaining patients (non responders n=9), TSH levels were significantly higher than baseline values after 3 months (0.47 vs 4.05 mU/l) and at each time point (ANOVA p<0.0001). To note, in 4 of them we have detected additional intestinal disorders. Again, no significant FT4 variations were observed throughout the study.
The use of softgel capsules, as compared with T4 tablet preparation, helps in optimizing the dose of T4 in most of patients with gastric disorders.
Disorders of Thyroid Function Friday Poster Clinical
William Ord coined the term Myxoedema in 1878 following Sir William Gull, who in 1873, described the cretinoid state presenting in adult women. George Murray treated hypothyroidism with extracts of sheep thyroid extract in 1891, and for the next 80+ years, treatment with natural desiccated thyroid (NDT) was standard of care therapy for hypothyroidism. However, by 1978, leading British endocrinologists felt compelled to warn against its use, leading to a dramatic decline in the amount of prescriptions of NDT. What prompted this paradigm shift away from NDT to alternative medications such as levothyroxine? This presentation proposes that NDT is a victim of the 'Tomato Effect' (as coined by James S. Goodwin), in which a highly efficacious therapy is ignored or rejected “because it does not make sense” in the light of accepted theories of disease mechanism and drug action.
Through an extensive literature review, the case will be made that three seminal events caused a paradigm shift away from glandular therapy to synthetic thyroxine. These events are: special patent protection (and profit-making potential) lasting over 50 years for synthetic thyroid; the introduction and acceptance of thyrotropin (TSH) as the criteria to diagnose hypothyroidism (as opposed to history and physical exam findings); and the misuse of NDT in combination with digitalis, diuretics, amphetamines, and other unclearly labeled pills (but brightly colored with various food dyes) as part of weight-reduction treatment plans for patients, many of them who were not overweight nor obese, merely because the physicians were able to dispense these pills at great profit. The use of these “Rainbow Pills” caused dozens of deaths in otherwise healthy persons, led to the labeling changes on all thyroid medications, and relegated the use of NDT to rogue physicians outside the mainstream.
Data will be presented showing the benefits and risks of NDT in the treatment of selected patients with hypothyroidism on symptom improvement and patient satisfaction, as well as protocols of how to mitigate potential adverse effects.
NDT is an underutilized therapy with a favorable benefit-to-risk ratio. A reappraisal of the use of NDT is warranted.
Disorders of Thyroid Function Friday Poster Clinical
A 49-YO F was admitted because of 2 months Hx of diarrhea, and 30-kg weight loss. On exam, she had SVT with HR 190.
We started her on methimazole, propranolol. Initial work up showed significant PTH-independent Hypercalcemia. Her corrected calcium was 12.6 (8.2–10.4 mg/dl). PTH was <5 (10 to 65 pg/mL). TFT showed Free T4 of 3.94 (0.8–1.9 NG/Dl), Free T3 9.0 (2.3–4.20 PG/ML), and TSH of 0.01. In addition, she had severe prolonged hypomagnesemia, her lowest magnesium was 0.8 (1.1–1.3 mEq/L). Work up for hypercalcemia showed suppressed PTH, low 25 OH vit D 12 (30.0–74.0 ng/mL), normal PTH- related peptide (<4.0 pmol/L), negative CXR for lung masses; CT chest, abdomen and pelvis were negative for cancer. Serum and urine PEP were negative. urinary calcium and magnesium were high suggesting renal loss.
While mild hypercalcemia has been reported with thyrotoxicosis, severe hypercalcemia is usually due malignancy. In situations in which thyrotoxicosis is the cause of hypercalcemia, the serum calcium level rarely exceeds 12 mg/dL and is usually asymptomatic. Hypercalcemia in thyrotoxicosis is presumably because of increased bone turnover. Our patient had severe hypomagnesemia, which were mainly due to GI loss; however, coexisting hypercalcemia can exacerbate hypomagnesemia since calcium and magnesium seem to compete for transport in the thick ascending limb of the loop of Henle. The increased filtered calcium load in hypercalcemic states will deliver more calcium to the loop of Henle; the ensuing rise in calcium re-absorption will diminish that of magnesium. Of note, our patient had microcytic anemia, which is a rare finding in thyrotoxicosis. Previous studies showed hypercellular marrow may indicate that erythropoiesis is enhanced due to hyperthyroidism, but in the same time it is ineffective, hence the finding of anemia with low MCV.
This report highlights the need for physicians to be alert regarding these rare manifestations of thyrotoxicosis including severe hypercalcemia, severe hypomagnesemia and microcytic hypochromic anemia.
Iodine Uptake & Metabolism Friday Poster Basic
Recent studies have demonstrated the presence of the chloride channel 5 (ClCN5), a voltage-gated chloride channel protein abundantly expressed in the kidney, at the apical membrane of mouse thyrocytes. The Clcn5-knockout mice display a phenotype reminiscent of Pendred's syndrome. These mice develop a goiter under conditions of normal dietary iodine intake and show decreased iodide organification when compared to wild-type mice. Another study has shown an increase in ClCN5 mRNA expression in the thyroid of a patient with Pendred syndrome. Currently, the role of ClCN5 in apical iodide efflux and iodide organification remains unclear.
In order to address the question whether ClCN5 mediates iodide efflux, we have performed functional analyses in non-polarized TSA-201 cells (a clone of human embryonic kidney 293 cells). TSA cells were transiently transfected with the human wild type sodium-iodide symporter (NIS), pendrin (PDS/SLC26A4), and ClCN5 cDNAs independently or simultaneously. In addition, we determined ClCN5 mRNA expression in rat thyroid (PCCl3) cells in the absence and the presence of iodide by extracting total RNA from the cells and subsequently analyzing it by real-time PCR.
Functional analyses demonstrate that cells co-transfected with NIS and PDS/SLC26A4, as well as NIS and ClCN5 show a decrease (2.8-fold and 1.6-fold, respectively) in the intracellular iodide content compared to transfection with NIS alone. Co-transfection of NIS with PDS/SLC26A4 and ClCN5 result in a decrease of intracellular iodide (3.2-fold), indicating a partially additive effect of PDS and ClCN5 on iodide efflux. Real-time PCR results show that ClCN5 mRNA expression significantly increases following a 30-minute treatment with 1 mM sodium iodide.
In conclusion, these results suggest that ClCN5 can mediate iodide efflux either by acting as an alternative iodide channel or by regulating pendrin's expression and/or function in vitro. Whether ClCN5 has a physiological role in mediating iodide efflux in thyrocytes remains uncertain.
Iodine Uptake & Metabolism Friday Poster Clinical
Marine algae (seaweeds) provide the bulk of atmospheric gaseous iodine. This can influence cloud formation but is also available for human ingestion by respiration. Conventional wisdom suggests that iodine intake in coastal regions exceeds that in inland areas. This study aimed to establish if living near the sea in a seaweed abundant environment, and therefore exposed to gaseous I2 ingestion by respiration, may confer advantages in terms of iodine intake. This may have relevance in countries such as Ireland and the UK where only 5% (approximately) of table salt sold is iodine supplemented and where urinary iodine excretion (UI) measurements continue to suggest borderline iodine deficiency.
Atmospheric I2 was measured by gas chromatography-mass spectrometry (GC-MS). Iodine intake was assessed by measuring (UI) using Sandell Kolthoff colorimetry. Urine samples were obtained from populations (N=192) living in coastal areas, including those residing beside a seaweed hot spot, and inland areas of Ireland.
Atmospheric I2 was greatest over the seaweed mass (Median 186: range 110–301PPT) compared to inland values of 15–18PPT. The median UI of 133 μg /L in the seaweed rich coastal area was significantly greater than in the coastal area lesser seaweed abundance (71 μg /L) or in the inland area (58 μg /L). The most striking differences were in the proportion of higher (>150 μg /L) individual UI values which reached 39.4% in the seaweed rich coastal area compared to 3.6% and 2.3% in the other study areas.
Thus the abundance of seaweed rather simply living near the sea may influence iodine intake. It is postulated that the relative absence of iodine deficiency recorded near seaweed hotspots may be the result of atmospheric iodine compensation for inadequate dietary intake in areas such as Ireland where iodine intake is traditionally low.
Thyroid Cancer Friday Poster Basic
10% to 25% of fine needle aspiration biopsies (FNAs) of thyroid nodules are either suspicious for follicular neoplasm or atypical (indeterminate cytology) requiring surgical resection for definitive diagnosis. The novel Gene Expression Classifier (GEC) performed on FNAs of thyroid nodules, preoperatively reclassifies these nodules as high probability of being benign (GEC-B) or suspicious for malignancy (GEC-S). We aimed to assess the clinical validity and utility of GEC testing in our institution.
We conducted a 12-month retrospective study involving 1,238 FNAs from thyroid nodules. 94 nodules were sent for GEC analysis. FNAs suspicious for follicular neoplasm or atypical (indeterminate cytology) were named indeterminate. Information regarding demographic characteristics, nodule size and final recommendations by one of our endocrinologists was retrospectively collected. We reviewed surgical and pathology reports from patients who underwent surgery. Ultrasound follow up was recommended in those with GEC-B, whereas surgery was recommended in those with GEC-S.
94 GEC reports were reviewed. 10 were unsatisfactory and 4 were excluded due to questionable indications. Of the remainder 80 nodules that were indeterminate by FNA: 33 (41%) were GEC-B and ultrasound follow up was recommended. 47 (59%) were GEC-S and surgery was recommended. Of the GEC-S, 36 (76%) underwent surgical resection. Malignancy was confirmed in 55% (n=20) of patients (16 papillary thyroid cancers, 2 follicular carcinomas, 1 both papillary and follicular carcinoma and 1 poorly differentiated carcinoma). 44% (n=16) of the GEC-S nodules were benign by final pathology.
This is the largest single center report assessing the clinical utility of GEC testing for suspicious for follicular neoplasm and atypical FNA biopsies of thyroid nodules. Our experience with GEC finds a slightly lower than previously reported rate of GEC-B samples (41% vs. 53%; p<0.01) and a higher rate of GEC-S samples (59% vs. 38%; p<0.01). GEC testing correctly identified a malignancy in just 55% of the GEC-S nodules.
Thyroid Cancer Friday Poster Basic
Thyroid cancer is the most common endocrine malignancy, and many patients with metastatic differentiated thyroid cancer (DTC), poorly differentiated thyroid cancer, and anaplastic thyroid cancer (ATC) fail to respond to conventional therapies, resulting in morbidity and mortality. Further therapeutic targets are needed for these patients. We recently reported that peroxisome proliferator-activated receptor gamma (PPARγ) is highly expressed in ATC and confers an aggressive phenotype when overexpressed in DTC cells.
shRNA-mediated gene silencing, microarray, Western blot (WB) analysis, immunohistochemistry (IHC), genetic overexpression, proliferation and glucose uptake assays, orthotopic thyroid cancer mouse model.
Using microarray analysis, we show that TXNIP, which encodes thioredoxin interacting protein, is highly upregulated when PPARγ is depleted from ATC HTh74 cells using specific shRNA. TXNIP is a tumor suppressor in other cell types which, in addition to its role in modulation of cellular redox state, also functions to inhibit glucose uptake, restrict cell cycle progression, and promote a pro-apoptotic environment. TXNIP and PPARγ exhibit reciprocal expression patterns in DTC and ATC cell lines. DTC cell lines and patient tumors exhibit high TXNIP expression in contrast to low or absent expression in ATC cell lines and tumors as assessed by WB and IHC. Overexpression of TXNIP using a genetic approach decreases the growth of HTh74 cells by 37% compared to vector controls (p<0.01) and inhibits glucose uptake in the ATC cell lines HTh74 and T238 (by 28% and 35%, with p=0.0010 and <0.0001, respectively). Importantly, TXNIP overexpression in T238 cells results in attenuated tumor growth in an orthotopic thyroid cancer mouse model (mean tumor volumes±SD: 97 mm3±68 and 27 mm3±26 for vector and TXNIP overexpression, respectively, p=0.0117).
TXNIP is highly expressed in DTC, however, its expression is downregulated in ATC. Exogenous overexpression of TXNIP in ATC cells slows cell growth, inhibits glucose uptake, and attenuates in vivo tumor growth. These studies underscore the potential of TXNIP as an important tumor suppressor in the transition from differentiated to advanced thyroid cancer.
Thyroid Cancer Friday Poster Basic
Molecular testing of routinely available thyroid nodule fine needle aspiration (FNA) material has many advantages. Although it can be performed with air dried smears, this material results in highly fragmented RNA. In contrast, liquid based FNA material allows efficient and easy RNA extraction. We therefore analyzed the remaining CytoLyt FNA material for BRAF and RAS point mutations and RET/PTC and PAX8/PPARG rearrangements.
Thyroid FNAs were classified according to TBS after routine cytologic examination, typically of a single ThinPrep slide. The remaining material (suspended in CytoLyt) from all available cases was used for blinded analysis of BRAF, NRAS, HRAS, KRAS point mutations and RET/PTC and PAX8/PPARG rearrangements by high resolution melting PCR and pyrosequencing.
A total of 597 consecutive cases were collected and stored at 8°C for up to 6 months. Molecular analysis of the remaining material was possible for 391 cases (65%). Higher volumes of remaining material (>2 ml) were associated with higher diagnostic success rates (23% vs. 79%, p<0.001, chi-squared test). Mutations and rearrangements were detected in 10 of 87 cases (11.5%) of atypia of undetermined significance (AUS), 11 of 33 (33%) suspicious cases, 24 of 51 (47.1%) malignant cases, 2 of 28 (7.1%) follicular neoplasms, 20 of 216 (9.3%) benign cases, and 4 of 163 (2.5%) non-diagnostic (molecular analysis possible for 103 of 163 (63.2%)) samples. Compared to histology (available for 211 samples), cytology and molecular analysis increased sensitivity, specificity, PPV, and NPV compared to cytology alone to 86.7% versus 73.6%, 98.1% versus 95.7%, 98.7% versus 94.4%, and 81.5% versus 78.8%, respectively, considering 13 mutation-positive but histologically benign cases as true positives.
Mutational analysis is feasible on residual ThinPrep material and has the advantage of not requiring additional FNA procedures or dedicated passes, special preservation, or storage. Its reflex use can be valuable in the pre-operative determination of the extent of surgery for mutation-positive cases, help to clarify 12% of AUS cases, decrease the rate of false negatives for benign cases, and allow molecular diagnostics for 63.2% of the non-diagnostic samples.
Thyroid Cancer Friday Poster Basic
Our aim was to examine the mutational profile of non-anaplastic thyroid carcinoma that died of disease (NTCD) and correlate with clinical characteristics and outcome.
39 patients with NTCD were treated with primary surgery at MSKCC from 1986 to 2009. Formalin fixed paraffin-embedded tissue was available on 33 patients; 25 had poorly differentiated, 7 differentiated thyroid carcinoma and 1 Hurthle cell carcinoma. Mass spectrometry-based genotyping was used to interrogate hot spot point mutations in the most common thyroid oncogenes: BRAF, RET, NRAS, HRAS, KRAS, PIK3CA, AKT1. In addition, common fusions of RET and PAX8/PPARγ were assessed by RT-PCR. Mutational profile was correlated with clinical characteristics by χ2test and outcome by the Kaplan Meier method.
Of 33 patients, 17(52%) were female and 31(91%) over 45 years of age. All patients had surgery with adjuvant RAI in 26(79%), adjuvant RAI+radiotherapy in 2(6%) and adjuvant RAI+chemoradiotherapy in 1(3%). 30(91%) patients had pT3/4 tumors, 28(85%) had extrathyroidal extension (ETE) and 19(58%) pN+. 85% of patients had driver mutations: 15 BRAF (46%), 9 RAS (27%), 2 BRAF/PIK3CA (6%), 1 PIK3CA (3%) and 1 had RET/PTC rearrangement (3%). 15% were wild type (wt) with no identifiable driver mutation or gene rearrangement. All patients developed distant metastases, 19(58%) at presentation and 14(42%) during follow up. Distant metastases were pulmonary alone in 11(33%), extrapulmonary in 2(6%) and mixed in 20(61%). Distant disease caused death in 26 (79%) patients: 11 BRAF+, 9 RAS+, 1 PIK3CA, 1 RET/PTC and 4 wt. Locoregional disease caused death in 4 (12%) patients (3 BRAF and 1 PIK3CA) while combined locoregional and distant disease caused death in 3 (9%) patients (1 BRAF, 1 BRAF/PIK3CA and 1 wt).
Majority of NTCD patients die of distant metastases. BRAF and RAS are the main driver mutations in these tumors. BRAF is the main driver mutation in NTCD tumors where locoregional disease is the cause of death.
Thyroid Cancer Friday Poster Basic
Thyroid cancer appears as papillary thyroid carcinoma (PTC) in about 80–90% cases and resulted by RET fusion with 12 other genes leading to 13 different oncofusions. Amongst; RET/PTC3 (RET fusion with ELE1) is the most metastatic type occurring in 20–30% PTC cases.
Initially a stable cell line was established of mouse fibroblasts by plasmid containing RET/PTC3 junction oncogene; named as RP3 cells. An efficient siRNA RET/PTC3 and an effective dose were selected on significant gene (RT-qPCR) and protein (Western blot) inhibitions. In vitro siRNA RET/PTC3 effects were tested on RP3 cell viability (MTT), proliferation (CFSE), invasion/migration in matrigel (IncuCyte), apoptosis (FACS, IncuCyte, WB), RET/PTC3 gene (RT-qPCR) and protein (WB) expressions. siRNA RET/PTC3-SQ bio-conjugate was synthesized, corresponding nanoparticles were prepared and tested for their effects on in vitro gene (RT-qPCR) and protein (Western blot) silencing. In vivo tumour growth inhibition and gene and protein silencing efficiency were later assessed as well, on administration in nude mice via intravenous route (cumulative dose=2.5 mg/kg).
In vitro siRNA RET/PTC3 was found to significantly inhibit cell viability, proliferation, invasion/migration, RET/PTC3 gene and protein expressions compared to siRNA control and siRNA RET/PTC1 at 24 h, 48 h and 72 h post-transfection incubations. Although it was not found to increase apoptosis in RP3 cells (Annexin/PI, IncuCyte) but an increased caspase-3 expression was found by Western blot at 24 h and 48 h post-transfection. In vivo, the RP3 cells were found to be tumorigenic in nude mice compared to mother NIH/3T3 cells. In vivo NPs were found efficient in significant (p<0.001) tumour growth, gene and protein inhibitions.
Although these NPs were not found efficient in gene and protein inhibitions in vitro but could be accepted as an efficient in vivo cancer therapy and hence guide towards further pharmacological studies intended for in vivo applications. This work was supported by ANR “P2N Nanosqualonc”.
Thyroid Cancer Friday Poster Translational
Cancer-associated fibroblast (CAF) plays an important role in the progression of multiple cancers, but its roles in thyroid cancer have not been investigated.
We first treated fibroblasts isolated from normal thyroid with K1 cell derived conditioned media (CM) to identify papillary thyroid cancer (PTC) CAF specific marker. Furthermore, we performed α-SMA immunostaining in 108 consecutive thyroid nodule patients, including 54 PTC, 21 follicular thyroid cancer, 6 anaplastic thyroid cancer, 11 follicular adenoma (FA) and 15 multinodular goiter. Subsequently we compared the tumor promoting effects of fibroblast derived from PTC (CAF and normal adjacent fibroblast (NAF)) and benign thyroid lesion by co-culture model and a co-implantation xenograft model mixing k1 cell with PTC derived CAF or NAF. Finally, we profiled the cytokines mediating the tumor promoting effects of fibroblast.
We found α-SMA as the only elevated marker for papillary thyroid cancer (PTC). Immunostaining showed significantly higher density of α-SMA+ fibroblasts in all follicular thyroid lesions comparing with normal thyroid. Interestingly, α-SMA+ staining was positively correlated with tumor size (P=0.046), local invasive behavior (P=0.0008) and higher TNM stage of PTC patients (P=0.0006). By in vitro co-culture model, we found that although all fibroblasts promoted K1/TPC1 proliferation and inhibited apoptosis, fibroblast from benign lesion inhibited tumor cell invasion. Surprisingly, while PTC derived fibroblasts all promoted invasion, NAF showed stronger effects. In a co-implantation xenograft model mixing k1 cell line with primary PTC derived CAF or NAF, we found mice bearing NAF had earlier tumorigenesis (P=0.0002) and larger tumor volume (P<0.0001) as well as higher rate of liver metastasis (27.27% vs. 16.67%) compared to CAF bearing mice. Finally, by applying cytokine antibody array for CM of both CAF and NAF, high level of IL-6, GRO, MCP-1 was observed in both CAF and NAF derived CM, with NAF even higher. For NAF, higher level of RANTES and GRO were observed.
Our findings provided evidence that fibroblasts with different derivations play different roles in mediating thyroid cancer growth and progression.
Thyroid Cancer Friday Poster Translational
Detecting methylated DNA from peripheral blood (PB) of patients with malignant tumors have been reported for screening and prognostication of tumor. This study aimed to verify methylation status of PTEN and RASSF1A gene in peripheral blood mono-nucleated cell (PBMC) of patients with papillary thyroid carcinoma (PTC) and analyze its correlation with clinicopathologic factors.
Eighty three patients who underwent thyroidectomy due to PTC and 41 age/sex matched healthy individuals were enrolled. PB had been collected, genomic DNA was extracted from PBMC and methylation-specific polymerase chain reaction (MS-PCR) of PTEN and RASSF1A was done. The outcomes were compared with clinicopathologic factors.
Sixty patients out of 83 (72.3%) could be identified of methylation of PTEN. PTEN methylated group showed larger tumor size (p=0.030). RASSF1A methylation was identified in 80.7% (67/83) and unmethylated group was inversely correlated with LN metastasis (p=0.017). Additionally, methylated DNA was observed in PBMC from age/sex matched healthy individuals (PTEN 14.6%, RASSF1A 9.8%).
PTEN and RASSF1A could be identified from PB of both patients with thyroid cancer and healthy controls, which showed relatively high success rate. PTEN methylated group showed larger tumor size and RASSF1A methylated group showed inverse correlation with lymph node metastasis.
Thyroid Cancer Friday Poster Translational
C-met is frequently expressed at very high levels in papillary thyroid carcinomas (PTC) and the concurrent overexpression of the downstream molecule STAT3 suggest a major functional role of HGF/c-met/STAT3 signaling pathway in PTC. STAT3 may act as a negative regulator of tumor growth in thyroid cancer. C-Met is a tyrosine kinase receptor, which is encoded by the proto-oncogene c-met. This protein stimulates cell proliferation, motility, morphogenesis, invasion and metastasis of tumor cells. The aim of this study is to evaluate STAT3 and c-Met immunostaining clinical utility as markers of thyroid nodules malignancy and prognoses.
We analyzed 119 thyroid tissues including 79 benign hyperplasic goiters and 40 thyroid carcinomas (35 papillary and 5 follicular). All patients were managed according to a same standard protocol and followed for 1–10 years (Mo=5 years). According to their serum Tg levels and image results, they were classified as no evidence-of-disease (24 cases) or persistence of disease/recurrence (14 cases). Representative areas of each primary nodule tissue were selected for construction of a tissue microarray slide that was subjected to immunohistochemistry.
Cytoplasmic expression of STAT3 occurred in all thyroid tissues, including the FC. In addition, nuclear expression was observed in 66% of the goiters and in 34% of carcinomas (p<0.0001, sensitivity 97%, specificity 87%, PPV 93%, NPV 94%), suggesting the protein exerts a tumor suppressor role. However, al FC were negative for STAT3 nuclear staining. C-Met had a cytoplasmic expression in all cancer tissues (100%), but in only 2% of the goiters (p<0.0001, sensitivity 100%, specificity 98%, PPV 97%, NPV 100%). Neither c-Met nor STAT3 were associated with any clinical or pathological characteristic of aggressiveness. These proteins were also not related to patients' outcome.
We conclude that c-Met and STAT3 can be useful in the diagnostic of malignancy in thyroid nodules but do not appear to help define thyroid tumors aggressiveness.
Thyroid Cancer Friday Poster Clinical
In Japan, the treatment for thyroid cancer without distant metastasis (DM) is thyroid lobectomy, with DM is radioactive iodine (RAI) therapy after total thyroidectomy. Cases with DM gather in the specific hospital, because RAI where can be treated is limited. We compare the prognosis of follicular thyroid cancer (FTC) with DM to that without DM.
We analyzed 19 cases with FTC from January, 2005 to December, 2012. The sex comprised 5 men and 14 women. The age was an average of 59.0 years old, median 61 years old, from 28 to 86 years old. The follow-up was from 4 to 96 months, the mean was 40.3 months, and the median was 46 months. DM (+) group was 12 cases (63.2%), and DM (−) group was 7 cases (36.8%).
DM (+) group performed total thyroidectomy in all cases, and RAI in 9 cases that overall status had good. It was 54.5% of 5-year survival rates. DM (−) group performed TSH suppressive therapy after thyroid lobectomy in all cases. It was 5-year disease-free survival rate 100%.
DM (+) group tended to have worse 5-year survival rate than DM (−) group. However, we can expect that prognosis of FTC with DM is prolonged if we provide appropriate treatment. FTC without DM is performed TSH suppressive therapy after thyroid lobectomy, and good prognosis is obtained.
Thyroid Cancer Friday Poster Clinical
The incidence of newly diagnosed thyroid cancer (TC) continues to increase. TC is the most common cancer in adolescents and young adult (AYA) females ages 15–29 and second for ages 30–39. However, little research details the unmet support needs and survivorship concerns of TC patients.
TC patients >15 years of age completed online surveys through the thyroid cancer survivor website. Patients rated the importance of receiving various medical/physical (M/Ph), practical, and emotional/psychological (E/Ps) realms of information during diagnosis and treatment, as well as their recollection of receiving such information. Comparison was made between AYAs and those ≥40 years at diagnosis.
Of 1113 respondents, most were female (88.3%), part Caucasian (92.3%), and treated in academic and private urban settings across the country with eventual total thyroidectomy (95.6%) and radioiodine (RAI) (80.4%). More than 80% of patients rated receiving information about most M/Ph matters very or extremely important and >70% felt similarly about E/Ps concerns. However, few recalled receiving any information besides that surrounding surgery or RAI. AYA respondents were more often female, non-white, Hispanic, married with children, living with a spouse/significant other, unemployed at diagnosis (all p<0.001) and reported more RAI (p=0.005). AYAs placed less importance on many M/Ph and practical matters but not E/Ps ones (Table 1). They less commonly recalled receiving information on recurrence (p=0.038), long-term side effects (p=0.024), coping strategies (p=0.049), support groups (p=0.019), opportunities for meeting other survivors (p=0.009) or help with treatment decisions (p=0.036). Additionally, AYAs reporting receiving significantly less information and care for their E/Ps concerns compared to older patients (16.1% v 22.4%, p=0.016).
Conclusion: TC patients place high importance on receiving information about most aspects of TC treatment and survivorship care. However, these information needs and survivorship concerns are largely unmet, especially among AYAs. Establishing multidisciplinary and survivorship-focused TC care may alleviate some of these unmet information and support needs.
Thyroid Cancer Friday Poster Clinical
Cowden Syndrome (CS) is a dominantly inherited tumor syndrome and is diagnosed either by the presence of germline PTEN gene mutation (mut+) or clinical criteria. Thyroid cancer (TC) has the earliest onset (at age 20–30) and 2nd highest lifetime risk (35%) of CS-associated malignancies. Because CS also includes many common benign diagnoses, it may be difficult to recognize and its prevalence underestimated. Our aim was to evaluate the prevalence of CS when screening is a routine part of initial consultation of patients with thyroid disease.
New patients without a CS diagnosis presenting to thyroid surgery clinic at a tertiary referral center were prospectively screened for CS using International Cowden Consortium (ICC) operational diagnostic criteria. Cleveland Clinic Risk Score to predict PTEN mut+status was calculated. Patients with suspicion of clinical diagnosis or ≥3% risk score were referred to genetics. CS prevalence was determined and correlated to patient's presenting thyroid diagnosis.
65 consecutive patients were screened: 2/19 (10.5%) with benign thyroid disease and 5/46 (10.8%) with TC met ICC criteria for CS diagnosis. PTEN mut+ risk score was ≥3% in 7/19 (36.8%) patients with benign disease and 11/46 (23.9%) with TC. Of 18 (28%) patients eligible for referral to genetics, 9 accepted this recommendation and 5 completed formal consultation to date. Pending test results include PTEN (n=3), BRCA (n=1) and Fragile X/array CGH/ Sotos Syndrome (n=1). Of patients meeting ICC criteria for CS, 43% had risk scores <3%. Thus, screening with risk calculator only would have missed 3 patients satisfying clinical diagnosis.
In this first prospective study of its kind, CS prevalence was 10% among patients with both benign and malignant thyroid disease. We demonstrate that CS can be successfully recognized via thorough medical history and PTEN mutation risk calculation. This screening algorithm may need refinement to address the large number of at-risk patients identified. Given high CS-related lifetime cancer risks and opportunity for cancer prevention, efforts to screen patients for CS appear feasible and advisable.
Thyroid Cancer Friday Poster Clinical
Because death is uncommon in thyroid cancer patients, the factors important in predicting survival, and especially the unique role of age in cancer prognosis, remain understudied.
To determine prognostic groups for overall survival in thyroid cancer and to assess relative effects of prognostic factors, we evaluated overall survival in 131,484 well-differentiated thyroid cancer patients who were affiliated with the National Cancer Database between 1998 and 2005. Multivariable analyses were performed using survival trees, random forest, and Cox proportional hazards regression. Patient, tumor, and treatment variables were included in the analyses.
Using survival trees, we identified five distinct prognostic groups (p<0.0001). The 5-year and 10-year overall survival of each prognostic group was as follows: 99% and 97%, 97% and 91%, 91% and 77%, 80% and 56%, and 53% and 22%. The most important factor in determining survival was age <versus ≥63 years. In patients ≥63 years, only clinical characteristics such as age, distant metastases, and lymph node involvement were important factors in defining the prognostic groups. In contrast, in patients ≤62 years, gender and insurance status also influenced the prognostic groups. Lymph node metastases only affected overall survival in patients age 50–82. With Cox proportional hazards regression, in addition to patient age being an important prognostic indicator, presence of distant metastases [adjusted hazard ratio + 95% confidence interval=3.75 (95% CI 3.45–4.06)] and Medicaid insurance [2.22 (2.00–2.46)] were also important factors in predicting death in thyroid cancer patients.
Age ≥63 is the most important prognostic indicator for thyroid cancer. The age at which lymph node involvement influences outcome, is greater than previously believed. These findings have implications for patient outcome, cancer staging, and treatment.
Thyroid Cancer Friday Poster Clinical
To evaluate the efficacy of radiofrequency ablation (RFA) in the treatment of loco-regional metastatic well-differentiated thyroid carcinoma.
Between March 2008 and October 2011, 35 metastatic thyroid carcinomas (mean diameter, 9.1 mm; range, 4.0–26.0 mm) in 32 patients (25 women, 7 men; mean age, 53.0 years) were treated with RFA. Metastatic thyroid carcinomas were detected by regular ultrasound follow-up examination and were confirmed by biopsy. Patients had fewer than three metastatic tumors (two in 3 patients; one in 29 patients) in the neck and infeasible condition to surgery. Total forty five RFA sessions (average 1.3, range 1–3) were performed. Post-RFA biopsy was performed in 21 carcinomas and 14 carcinomas did the follow-up ultrasonography. Pre- and post-RFA serum thyroglobulin value were evaluated in 26 patients.
On 21 post-RFA ultrasound-guided biopsy, 20 carcinomas were negative for malignancy and RFA session was completed. One of two carcinomas in one patient showed remaining carcinoma on post-RFA biopsy and was surgically removed. After RFA, the mean largest diameter decreased from 9.1 mm (range 4–26 mm) to 1.3 mm (range 0–15.0 mm) with overall 85.7% decrease, as did mean volume, from 394.6 mm3 (range 18.9–4792.0 mm3) to 49.8 mm3 (range 0–1099.6 mm3) with overall 88.6% decrease. At the last follow-up ultrasound examination, thirty one metastatic tumors had completely disappeared (31/33, 93.9%) and two tumors showed decreased volume (volume reduction rate, 84% and 53%) with tiny calcified nodule and hypoechoic nodule with internal hyperechoic dot, respectively. The serum thyroglobulin concentration in 19 of 26 patients showed overall 44.9% decrease (from 11.8 ng/ml to 6.5 ng/ml). Six patients had voice change immediately after RFA. Voice change was spontaneously recovered in 5 patients and was improved after vocal cord medialization in one patient.
Although surgery is the choice of treatment, RFA is minimally invasive effective modality and may have a role in treatment of loco-regional metastatic well-differentiated thyroid carcinoma in patients with infeasible condition to surgery.
Thyroid Cancer Friday Poster Clinical
Postoperative hypocalcemia is a common complication after total thyroidectomy. This study aimed to evaluate clinicopatholgic risk factors and biochemical predictors for the development of hypocalcemic symptoms according to postoperative days (POD) after total thyroidectomy.
Medical records of 988 patients who underwent total thyroidectomy from March 2008 to December 2010 were reviewed. Clinicopathologic characteristics and biochemical data were compared across symptomatic and asymptomatic patients. The optimal cut-off and associated predictive value of each biochemical parameter at each time point was evaluated using receiver operator characteristic (ROC) curves.
Hypocalcemic symptoms developed in 414 patients (41.9%). Age <45 years (p<0.0001), female gender (p<0.0001), and bilateral central compartment node dissection (p=0.031) were independent risk factors for development of hypocalcemic symptoms. Biochemical predictors of hypocalcemic symptom development with the highest positive predictive values (PPV) at each POD were intact parathyroid hormone (iPTH) <4.9 pg/mL (PPV=78.4%) on POD1, iPTH <7.6 pg/mL (PPV=79.9%) on POD2, and iPTH <7.3 pg/mL (PPV=87.2%) on POD3. Biochemical predictors of non-development of hypocalcemic symptoms with the highest negative predictive value (NPV) were iPTH >4.9 pg/mL (NPV=88.0%) on POD1, calcium >7.5 mg/dL (NPV=93.8%) on POD2, and calcium >7.5 mg/dL and phosphate <5.3 mg/dL (NPV=99.0%) on POD3.
Biochemical markers measured on POD 2 and 3 can be applied to more accurately predict hypocalcemic symptoms compared with those at 1 h postoperatively and on POD 1.
Thyroid Cancer Friday Poster Clinical
It has been reported that papillary thyroid microcarcinoma (PTM) is now the most commonly diagnosed endocrine malignancy. It has been estimated that, if approximately 10% of the population of the USA harbors this latent disease, paying just for the FNA biopsy and the thyroidectomy, presently mandated to manage this PTM ‘tsunami’, would bankrupt the American health system! The ATA and ETA Guidelines recommend thyroidectomy and lifelong thyrotropin suppression for papillary thyroid cancers (PTC) of 1 cm or less. By contrast, Ito in Japan has been willing to manage the majority of his PTM patients with observation alone. In the USA, patients with a new diagnosis of PTM are starting to question the dogma of the Guidelines and are willing to be observed or to be treated by less invasive procedures than partial or total thyroidectomy.
After more than two decades of employing ultrasound-guided percutaneous ethanol ablation (UPEA) in controlling nodal metastases in the postoperative necks of 146 personal PTC patients, we felt confident in offering UPEA of cancer foci in the intact thyroid to those patients who have decided against surgical resection of their PTMs. Here we describe our initial experience in the first three patients that we have so treated.
The first patient (M58) had bilateral foci (5 and 9 mm diameter); larger (140 mm3 volume) treated with 0.7 cc; smaller (31 mm3) with 0.65 cc. At 12 months after UPEA, neither PTM had Doppler flow and both were smaller (140 to 83 and 31 to 23 mm3). Second patient (F36) with FDG-positive 7 mm PTM received 1.25 cc, disappeared on PET at 4 months, avascular and smaller (44 to 5 mm3) at 5 months. Third patient (F53) had bilateral foci (10 and 5 mm) treated with total 2.45 cc and at 3 months avascular and smaller (250 to 21; 42 to 25 mm3).
To summarize, we have successfully treated with UPEA five foci of PTM in three intact thyroids. No patient developed a painful thyroiditis and none had hoarseness or hypocalcemia. UPEA was well tolerated as an outpatient procedure under local anesthetic and was substantially cheaper than conventional surgery. We conclude that, for PTM patients who refuse surgery, UPEA may prove to be a long-term superior alternative to observation alone.
Thyroid Cancer Friday Poster Clinical
Papillary thyroid carcinomas(PTC) less than 2 cm in size are believed to be a less aggressive subset of PTC which behave more like benign lesions and are often more conservatively treated. However, it is unclear whether carcinoma no larger than 2.0 cm in diameter can be expected to have a similar favorable clinical behavior as tumors no larger than 1.0 cm. Therefore, to address this question and to characterize the biology and optimal treatment for PTC less than 2 cm, we performed a retrospective chart review.
From October 2001 to March 2013, 670 patients underwent surgery for PTC less than 2 cm. Data from these patients were retrospectively analyzed.
The mean age of these patients was 43.2 years and 91.3% were female. 53.0% of the patients underwent a total or near-total thyroidectomy. Of the 670 patients, 204 (30.4%) had lymph node metastases. The patients present with signs of aggressiveness including multifocality (27.2%), bilaterality (19.7%), capsular invasion (44.9%). Lymph node metastases were associated with tumor size (p<0.0001), capsular invasion (p<0.0001) and bilaterality (p=0.002) but not multifocality, age and sex. With follow-up of up to 138 months, 7 patients had a local recurrence, recurrence rate was 1.0%, and no patients currently have active disease. No patients have died during this period.
In PTC less than 2 cm in size, progressively increasing frequency of signs of tumor aggressiveness including bilaterality, capsular invasion and lymph node metastasis with increasing tumor size.

Thyroid Cancer Friday Poster Clinical
Pediatric patients diagnosed with papillary thyroid cancer (PTC) have a high incidence of regional metastasis. Total thyroidectomy (TTx) with varying extent of lymph node dissection is believed to be the best surgical approach to decrease the risk for repeat surgical procedures. Younger age and the annual volume of thyroid cancer surgeries performed are proposed to be the greatest predictors of post-operative complications, however, there are few studies that have attempted to correlate extent of disease as a potential confounding variable.
Retrospective chart review of all thyroidectomies performed at the Children's Hospital of Philadelphia between January 1, 2009, and March 1, 2013.
Over the time of review, 157 thyroid surgeries were performed on 140 subjects ≤18 years of age; median age was 15 years (IQR 13–17), 108 were females. Nodules and abnormal cervical adenopathy were noted on physical exam in 80 (76.2%) and 17 (16.2%), respectively. Pre-operative ultrasound (US) confirmed abnormal central or lateral lymph nodes in 13 (12.6%). 39 subjects underwent lobectomy and 66 TTx with or without neck dissection. Parathyroid glands were visualized and left in situ in 71 (67.6%) and auto-transplanted in 33 (31.4%) subjects. Post-operative hypocalcemia was observed in 40 (38.9%): 16 (48%) after parathyroid gland reimplantation and 14 (28%) with glands left in situ (p=0.037). Sustained hypoparathyroidism was seen in 12% of subjects with parathyroid gland reimplantation compared to 6.3% of subjects whose glands remained in situ (p=0.027). In subjects with sustained hypoparathyroidism, 13.9% underwent a TTx with central neck dissection and 36.4% had TTx with central and lateral neck dissection. Sustained hypocalcemia was significantly associated with central (N1a) and lateral (N1b) neck metastasis confirmed on final pathology (p=0.025).
The extent of lymphatic involvement and method of parathyroid gland management are strongly associated with post-operative hypoparathyroidism in children with PTC undergoing thyroidectomy.
Thyroid Cancer Friday Poster Clinical
The vessel-sealing (VS) instruments have been shown to decrease operative time (OT) compared to knot-tying in thyroid surgery. The first generation VS instrument (Ethicon CS-14), a shortened version of a laparoscopic instrument designed for vessel ligation with limited dissecting abilities. The second generation instrument (Ethicon Harmonic Focus), designed to mimic a Kelly clamp with both dissecting and ligating functionality. The impact of this new technology on operative efficiency, in particular surgeon to surgeon variability, has not been studied in the literature.
Between 2000–2011, 839 patients underwent total thyroidectomy without nodal dissection by 3 endocrine surgeons at a tertiary medical center. The procedures were done using a first-generation VS device in 53% and a second-generation in 47%. Clinical parameters and VS device (CS-14 versus Focus) were prospectively collected and analyzed using Student's t, Chi-square, univariate and multivariate analyses. Data are expressed as mean±SEM.
There were 675 women and 164 men. The overall OT was 143±1 mins, and incision size 4.8±0.1 cm. The strongest independent predictor of decreased OT was the use of the second-generation VS device that reduced OT for surgeon 1 from 126 to 111 (15 mins less), for surgeon 2 from 169 to 146 (23 mins less), for surgeon 3 from 179 to 153 minutes (26 mins less), p<0.001. In addition to the surgeon (Hazard Ratio: 9.2) and device model (HR: 7.9), other independent predictors of longer OT were younger age (HR: 3.9 min/year), male sex (HR: 6.1), increasing BMI (HR: 3.9 min/kg/m2), increasing specimen weight (HR: 4.1 min/gr), increasing specimen size (HR: 2.3 min/cm), and thyroiditis vs cancer or multi-nodular goiter (HR: 2.2), p<0.05 in univariate analyses. The presence of a resident vs fellow did not affect OT (p=0.119).
The VS device type, surgeon, and specimen weight were most consistent predictors of OT for total thyroidectomy. The results show that all 3 surgeons demonstrated improved operative times using the second-generation VS devices. We feel that, this effect is not due to faster VS times per se, but to improved ergonomics of the devices with grater use as a dissector and fewer instrument exchanges.
Thyroid Cancer Friday Poster Clinical
BRAFV600E mutation is the most common genetic alteration in papillary thyroid carcinoma (PTC). Some studies showed that Hashimoto's thyroiditis (HT) was associated with a higher risk of PTC and coexistence of HT was associated with better prognosis. This study was to determine a correlation between BRAFV600E and presence of HT in patients with PTC and their association with other clinicopathological factors.
We enrolled 399 patients with classical PTC who evaluated BRAFV600E status by using direct-sequencing. HT was defined as pathologically proven lymphocytic thyroiditis and/or positive serum anti-thyroperoxidase antibody.
Total 122 patients (28%) had PTC with coexistent HT. Coexistence of HT was significantly associated with female gender (p=0.04), younger age (p=0.05), and multifocal PTC (p=0.02). BRAFV600E mutation was confirmed in 248 patients (62%). There was a significant correlation between with BRAFV600E status and HT (p=0.004). BRAFV600E was less common in PTC with coexistent HT (51%) as compared to PTC without HT (67%). PTC with BRAFV600E mutation was significantly associated with more extrathyroidal invasion only (p=0.02). There was no significant difference in clinicopathologic parameters according to the coexistence of HT in patients with BRAFV600E mutated PTC.
In this study, we found that BRAFV600E mutation is less frequent in PTC with coexistent HT as compared to PTC without HT.
Thyroid Cancer Friday Poster Clinical
Black thyroid pigmentation is a rare entity. Previous small series suggest an association between black thyroid and thyroid cancer. The aim of this study was to examine this correlation.
A retrospective medical chart review was performed on 924 patients who underwent thyroid surgery at an academic university hospital.
Among 924 patients, 722 (78%) were female, and 202 (22%) were male, 403 (43.6%) were white, and 379 (41%) were African American. Black thyroid was diagnosed in 112 (12.1%) patients. The mean age for patients with black thyroid was 54.3±12.8 versus 51.2±15.7 for patients with non-black thyroid (P=0.05). Incidence of malignancy in black thyroid and non-black thyroid was 55.4% (62/112) and 32.8% (378/812) respectively; p<0.0001). In addition, incidence of papillary thyroid cancer among the black and non-black thyroid was 34.8% (39/112) and 20% (162/812) respectively; p<0.001. Black thyroid was also associated with a higher incidence of micro-carcinoma (76% vs. 59%, p=0.02). Incidence of multi-focal papillary carcinoma in black and non-black thyroid was 39% and 49% respectively (p=0.3).
The current study suggests that the incidence of malignancy is higher in black thyroid compared to non-black thyroid glands. This high risk warrants thorough pathological examination and prophylactic removal of incidentally found black thyroids.
Thyroid Cancer Friday Poster Clinical
Tyrosine kinase inhibitors (TKIs) represent an important therapeutic option for patients with metastatic cancer. Most TKI's inhibit angiogenesis via targeting of the tyrosine kinase domain of the vascular endothelial growth factor receptor (VEGF-R). Inhibition of VEGFR mediated signaling can lead to vascular endothelial cell apoptosis, inhibition of new vessel formation and vasoconstriction. The VEGF signaling pathway however, is a key mediator of angiogenesis in the proliferative phase of wound healing. In preclinical studies, VEGFR targeted therapies have been shown to impair wound healing, but the clinical relevance of this finding is unclear. Thus, how to approach wound healing in patients on TKIs is unclear.
We report 2 patients with progressive, end stage papillary thyroid carcinoma and wounds, who continued on a single investigational TKI.
Case #1: A 64 year-old Japanese-American male initiated TKI 12 days after surgical excision of a 3 cm subcutaneous abdominal wall metastasis. Thirty five days after surgery, the surgical wound dehisced resulting in a 3.3×5×1.5 cm wound, extending through the dermis and subcutaneous tissue with extensive undermining along the margin. Given the advanced stage of his disease and limited alternative options, TKI was continued. The wound was treated with calcium alginate and negative pressure therapy. The wound fully healed after 7 months.
Case #2: A 71 year-old Hispanic diabetic female on TKI therapy for 10 months developed a 1.5×1×0.2 cm open wound on her left shin resulting from cat scratches. She was treated with antibiotics, debridement and monitored by a wound specialist. Her wound healed completely over a 2 year period. During this 2 year period, brief interruptions and dose adjustments of therapy were necessary for unrelated side effects.
Two patients exhibited successful wound healing while continuing on TKI therapy. While caution must be exhibited, all wounds may not represent an absolute contraindication to TKI therapy. Continuation of TKI therapy and aggressive wound therapy supervised by a wound care specialist may be an option. Since both patients were treated with a single investigational TKI, these results may not be generalizable to the TKI class of drugs.
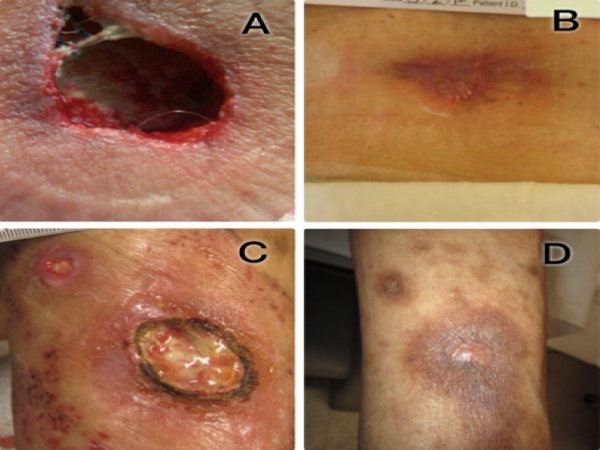
Thyroid Cancer Friday Poster Clinical
The association between thyroid cancer (TC) and Hashimoto's thyroiditis (HT) is currently being further studied to investigate the risk of developing thyroid cancer in patients with HT. BRAF gene mutation has been linked to aggressive TC. The aim of this study was to evaluate the association between TC and HT.
A retrospective case control study involved 943 patients who underwent thyroid surgery at a single North American institution from January 1998 to May 2013. Patients were evaluated for demographic data, malignancy, tumor size, BRAF mutation and lymph node metastasis. Statistical analysis was conducted using Chi-square test and logistic regression. Significance was defined as p<0.05.
There were no differences in patients' demographic, tumor size, focality of the disease and BRAF gene positive mutation between HT and Non-HT. HT has been diagnosed in 217 patients. Patients with HT were more likely to have TC than Non-HT patients (OR 2.12, 95% CI=1.5413–2.9111; p<0.0001). Furthermore, HT patients were less likely to have metastatic lymph nodes than non-HT patients (OR 0.19, 95% CI=0.0721–0.5110; p<0.0001).
HT may be considered a risk factor for developing TC. However, the co-occurrence of TC and HT can have less invasive disease and better prognosis than Non-HT. The association between TC and HT may require full pathological investigations for all HT patients to exclude cancer.
Thyroid Cancer Friday Poster Clinical
Serum Thyroglobulin (Tg), measured by second generation IMAs (functional sensitivity ≤0.10 ng/mL) methods is used as the primary tumor marker for detecting recurrent/persistent DTC, although even very low levels of TgAb interferes causing falsely low/undetectable Tg IMA values. The goal of this study is to evaluate whether thyroidectomy-related Tg release increases or prompts de novo appearance of TgAb postoperatively (<12 weeks).
40 DTC patients (39 PTC/1FTC) with preoperative Tg (RIA)+ TgAb measurements and TgAb detected postoperatively. A post-operative TgAb rise was classified as >110% TgAb above preoperative TgAb, measured between 10 and 100 postoperative days, prior to any radioiodine therapy. TgAb was measured using the Kronus TgAb radioassay (functional sensitivity=0.4 kIU/L; %CV=<10% in the measureable range in runs spanning a year of measurements.
Group 1: In 22/40 (55%) patients with preoperative TgAb detected, TgAb fell to a median of 52% (range 28–88) of preoperative values by a median of 48 (range 20–104) postoperative days. Group 2: 18/40 (45%) patients displayed a rise in TgAb (median 220, range 123–3600%) at a median of 47 (range 10–91) days. 4/18 (22%) of Group 2 patients developed detectable TgAb denovo after surgery that persisted throughout follow-up (1.6, 3.6 and 5.9 years). Group 1 compared with Group 2 tended to have lower preoperative Tg (median 21.8 versus 61.7 ng/mL) and higher TgAb (median 27.2 versus 1.0 kIU/L), respectively. The groups showed no difference in age, TNM, frequency of recurrences, or histologic lymphocytic thyroiditis.
It is not unusual to see a rise or de novo appearance of TgAb in the first 3 months following thyroidectomy with the potential to interfere with Tg IMA measurements. This likely reflects the immune response to antigen (Tg) release secondary to surgical trauma, especially when preoperative TgAb is low or undetectable.
Withdrawn
Thyroid Cancer Friday Poster Clinical
The early detection of metastatic lateral neck lymphnodes (LNL) was evaluated by thyroglobulin (Tg) and neck ultrasonography (NU) in 534 patients with papillary or follicular differentiated thyroid cancer (DTC), and long-term follow-up after I131 and/or surgery.
DTC-patients, previously treated with near-total thyroidectomy and I131 ablation of residual tissue, underwent follow-up by Tg, NU, diagnostic and post-therapy whole body scan (WBS), alone or in combination.
For detecting LNL, TSH-stimulated Tg alone had a diagnostic sensitivity of 85% and a negative predictive value (NPV) of 83%, while NU and diagnostic WBS had a sensitivity of 67% and 80%, and NPV of 66% and 80%, respectively. The combination of Tg with NU or diagnostic WBS increased the sensitivity to 98% and 97%, while NPV to 100% and 97%, respectively. Patients with LNL uptaking radioiodine were treated with I131, among them 51% responded after 4 cycles (median 310 mCi, cumulative dose; 6.7 years median follow-up) with “disappearence of uptake at post-therapy WBS and Tg<1 ng/ml” (complete remission, CR), patients not responder had CR with other treatments in only 14% of cases. Patients with LNL not uptaking or not responder to I131 (7%) were treated with surgery, and subsequent I131 readministration with CR in 26% of cases (5.3 years median follow-up).
Complete remission by I131 in 51% DTC-patients after 4 or less I131 treatments may be permitted by early dection of LNL. Patients not responder/not uptaking I131 can achieve a complete remission in 26% of cases combining surgery and radioiodine retreatment.
Withdrawn
Thyroid Cancer Friday Poster Clinical
Patients in a US public hospital were recently found to present with more advanced differentiated thyroid carcinoma (DTC) than those in an adjacent university hospital. 37% of public hospital patients with DTC were primarily Spanish-speaking. We used focus groups and key informant interviews to examine access to care and knowledge of diagnosis/treatment among Spanish-speaking patients with DTC.
All adult patients treated for DTC between 2000–2011 and who indicated Spanish as their preferred language met inclusion criteria. Focus groups and key informant interviews were conducted in Spanish by trained facilitators, utilizing a phenomenology approach. Discussions focused on diagnosis and treatment of DTC.
16/50 eligible patients participated. While all expressed a preference for Spanish when discussing medical care, no patient found language to be a barrier due to ready availability of interpreting services. All reported unimpeded access to primary care, with community networks serving as an important information source of public health services. The majority of patients presented with a self-reported nodule or symptoms associated with hypo/hyperthyroidism, which prompted further work-up. DTC was discovered incidentally on imaging in a small minority of patients. The majority of patients reported limited to no knowledge of thyroid cancer prior to diagnosis. Although only one patient used alternative medicine as a treatment for thyroid cancer, many expressed a belief in its value as a complementary modality.
Access to care proved unhindered among this patient population, though was contingent on strong community networks and availability of interpreter services. Despite limited patient knowledge, DTC was most commonly diagnosed following presentation with a self-discovered nodule or symptoms of hypo/hyperthyroidism. Beliefs in alternative medicine did not affect timely treatment. These data emphasize the importance of patient education and a culturally sensitive approach to optimize care in this demographic.
Thyroid Cancer Friday Poster Clinical
We conducted a retrospective chart review study of differentiated thyroid cancer patients to examine thyroid bed nodules seen on ultrasonography after total thyroidectomy. Factors that influence the loco regional recurrence were observed and comparison was performed between patients with recurrence and those without cancer recurrence.
From our database, we selected 60 patients with differentiated thyroid cancer that underwent total thyroidectomy, received 131-I therapy (mean dose 229.12 mcui) and had thyroid bed nodules on postoperative surveillance ultrasound. Thyroid bed nodules were studied over a mean of 10.9 years with standard deviation of 5.94. Their ultrasonography features and progression over time was studied. Serum thyroglobulin levels were monitored and determined if the levels remained stable or increased. Comparison was performed between patients who did not have recurrence versus patients who had recurrence and factors for loco-regional recurrence were studied.
Out of 60 patients, 15 patients had cancer recurrence. Increase in the size of thyroid bed nodule was seen in 20% patients and increase in number was seen in 20%. 30.0% of patient had more than twice increase in serum thyroglobulin levels. 60% patients (9 out of 15 patients) in recurrence group had an increase in size of bed nodules as compared to only 6.67% (3 out of 45 patients) in group without recurrence. 60% patients with recurrence had increase in the number of nodules as compared to 6.67% in non-recurrence group. Significant increase in serum thyroglobulin (more than twice) was seen in 80% patients with recurrence (12 out of 15 patients). In non-recurrence group, only 13.33% (6 out of 45) had increase in serum thyroglobulin levels. Patient with recurrence had higher number of suspicious thyroid bed nodules (80%) and neck lymph nodes (15.56%).
Thyroid bed nodules are commonly seen after total thyroidectomy in thyroid cancer patients. Thyroid bed nodules on surveillance ultrasound warrant fine needle aspiration cytology if they significantly increase in size and number, are persistent and associated with suspicious features. Increase in serum thyroglobulin levels more than two fold is worrisome for recurrence.
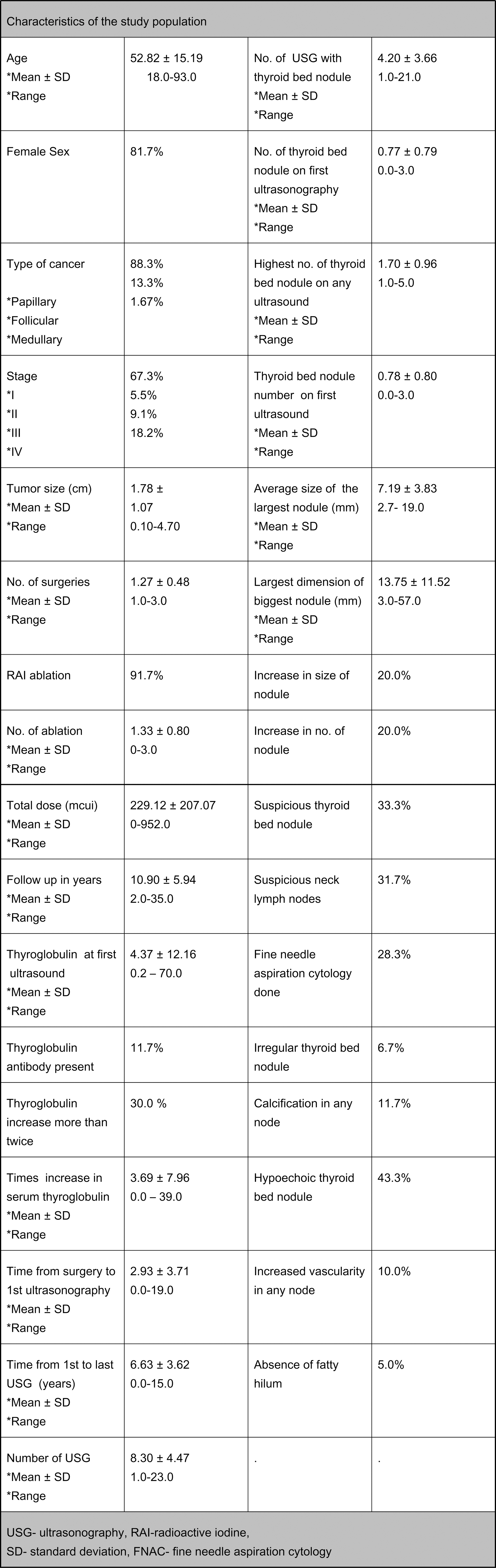
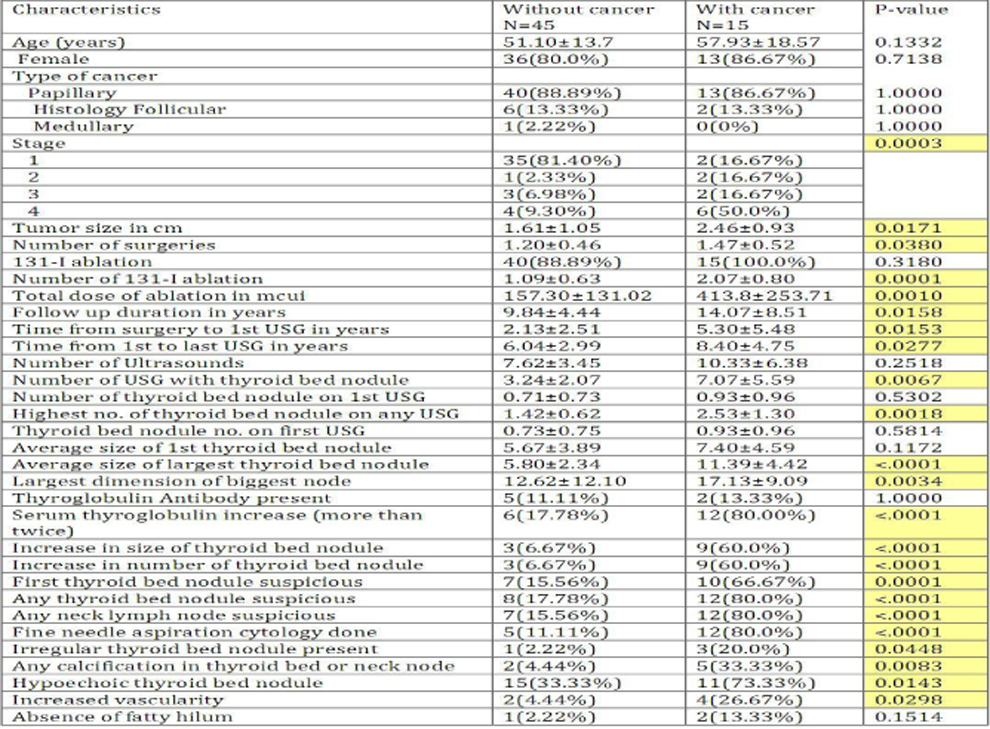
Comparison of patients with cancer and without cancer
Thyroid Cancer Friday Poster Clinical
Fine needle aspiration is one of the most useful initial diagnostic tools in the work-up of thyroid nodules. However, cytology may be indeterminate or equivocal, and BRAF mutation status may be helpful in surgical decision-making. In this study we examine the incidence of BRAF mutations diagnosed in fine needle aspirates from thyroid nodules in a veteran population and its impact on surgical decision making. In addition, we analyze the incidence of BRAF mutations in surgically removed papillary thyroid cancers in this group of patients.
A retrospective review was performed of all thyroid fine needle aspirates performed between January 1, 2011 and December 31, 2012 at the VA West Los Angeles Medical Center. BRAF testing was performed on all aspirates using PCR methodology to search for an oncogenic mutation at V600E in exon 15. The computerized patient record system (CPRS) for the VA West Los Angeles was searched to analyze the subsequent clinical recommendations based on thyroid cytology. BRAF testing was also performed on papillary thyroid carcinoma specimens which were surgically removed.
A total of 190 thyroid nodules were analyzed with fine needle aspiration and BRAF testing during this time period in 170 patients. There were 150 males and 20 females. The mean age was 57 years of age. BRAF mutations were found in the majority of surgically removed papillary carcinomas.
BRAF testing of fine needle aspirates and papillary thyroid cancer specimens is a useful diagnostic tool during work-up and treatment of thyroid nodules. The incidence of BRAF mutations in the majority of papillary thyroid carcinomas is not surprising in this predominantly male and older population and suggests that such cancers should be aggressively treated in this subset of patients.
Thyroid Cancer Friday Poster Clinical
Patients who undergo thyroidectomy due to thyroid cancer often complain weight gain, although they are on suppressive thyroid hormone treatment. The aim of this study is to know whether thyroid cancer patients gain the weight after thyroidectomy and weight change is dependent on estrogen state or use of rhTSH.
We performed a retrospective chart review of subjects receiving medical care at an academic medical center. Two hundred two patients who underwent total thyroidectomy were included. As a control group, patients with thyroid nodule and euthyroidism were matched for age, gender, menopausal status. The weight changes occurring over first one year and thyroid function were assessed.
Mean age was 51±12 years and patients was composed with 38% of premenopausal, 15% perimenopausal women, 37% of postmenopausal women and 20% of men. Patients with thyroid cancer gained 2.2 kg during the first year. It' was not significantly different with control. However, weigh change in perimenopausal and post menopausal women gained more weight than control (P<0.05). Age, baseline body weight and weight gain were not correlated.
Patient who had undergone thyroidectomy gained more weight than their control, especially in peri- and postmenopausal women. Patients in this age should be monitored for their weight carefully.
Thyroid Cancer Friday Poster Clinical
Papillary thyroid carcinoma (PTC) is one of the relatively good-prognosis cancers. However, even if patients with PTC recovered completely once, PTC sometimes recur for years later. This time, we analyzed about the treatments of PTC in our hospital.
Retrospective analysis revealed 123 cases of patients with PTC in a total of 153 cases between April 2005 and March 2013. Statistical data was as follows: age; 14–84 years (median: 59.8), sex; 40 males and 83 females. 26 patients had distant metastasis at first examination, and 38 patients had Hashimoto disease.
Cause-specific survival rate in total was 96.4% at 5 years. 72 patients were recovered completely by one surgery. 10 patients were operated one more because surgery stumps of them were positive, and they all could get complete response. 31 patients have recurrence. Among them, 11 of 31 were recovered completely by reoperation, while the others have recurrence again even if we performed secondary operation. The relapse-free survival rate in total was 69.5% at 5 years. In 11 patients that recovered completely by reoperation, a period until tumor enlargement was an average of 35.3 months. On the other hands, in 20 patients that did NOT recover completely by reoperation, a period until tumor enlargement was an average of 30 months, then they tended to have a short time to recurrence again rather than patients with complete response by reoperation. In 26 patients with distant metastasis, 4 patients were recovered completely because of the complete resection of their distant metastases.
Cause-specific survival rate in total was 96.4% at 5 years, and this is a good prognosis. A prognosis prolongation effect is obtained by reoperation to the patients with recurrence. Further and long-term studies are necessary for the improvement of the treatment outcome in PTC.
Thyroid Cancer Friday Poster Clinical
To report a case of metastatic thyroid cancer in an elderly patient who presented with hip pain.
70 year old female who complained of persistent left sided hip pain during a recent hospitalization for syncope. She had history of DM, HTN and breast cancer s/p lumpectomy and RT in 2003. Initial syncope workup was negative; however she was noted to have an abnormal gait on exam. Hip x-rays were normal. MRI demonstrated a lesion in the proximal Lt femur. Biopsy of the lesion demonstrated Hurthle cell follicular thyroid carcinoma (HCC). Initial thyroglobulin was 23102 ng/dl. Thyroid ultrasound showed a mass within the Lt lobe with no abnormal lymph nodes. She underwent total thyroidectomy and final pathology demonstrated HCC in the Lt lobe and a 0.5 cm papillary carcinoma in the Rt lobe. Post-surgery labs showed thyroglobulin 6330 ng/dl. Low Dose I131 (2 mCi) scan showed small area of uptake in the thyroid bed and no uptake in the Lt femur. Patient was started on levothyroxine. Following administration of recombinant thyrotropin she was given 250 mCi of I131. Post treatment scan showed focal area of uptake in the thyroid bed but no uptake in the Lt femur. She received localized RT to the Lt hip after stabilization with intramedullary rods. The patient was referred to oncology to discuss further treatment options.
HCC represents 3% of thyroid cancers. The clinical course is usually aggressive, especially in elderly patients. Initial presentation in this population commonly includes symptoms related to distant metastases. Our patient presented with hip pain and abnormal gait due to a metastatic lesion. Features such as decreased I131 avidity and late recurrence are associated with poor prognosis. Management of metastatic, I131 resistant HCC is challenging. Palliative external beam RT is recommended by current guidelines. Further modalities of treatment such as tyrosine kinase inhibitors are currently being studied in this population.
Metastatic HCC can present late in the course of the disease with atypical symptoms. Treatment options for this aggressive disease are presently limited. Newer therapeutic modalities including the use of tyrosine kinase inhibitors may prove beneficial in patients with advanced HCC.
Thyroid & Development Friday Poster Clinical
Bilateral neck exploration (BNE) was the traditional gold standard operation for primary hyperparathyroidism (PHP), however, some disadvantages were also existed. Recently, with the development of minimally invasive thyroid surgery, more and more attention was paid to the minimally invasive video-assisted parathyroidectomy (MIVAP). The purpose of this study is to perform a randomized controlled trial to compare the therapeutic effects of BNE and MIVAP.
Between April 2005 and July 2011, 108 patients (52 cases for BNE and 56 cases for MIVAP)with PHP were enrolled in our study. In the MIVAP group, both preoperative localization and intra-operative parathyroid hormone (iPTH) detection were performed to confirm the success resection. While in the BNE group, only tumor size observation and rapid frozen pathology detection were used. Follow-up was performed in 6 weeks, 6 months and 1 year postoperatively.
Cure rates of the two groups have no difference (95% vs 96%, P<0.005). Five patients have been found to have persistent or recurrent HPT (3 in MIVAP and 2 in BNE), and 3 cases was converted to BNE in MIVAP. Patients in the MIVAP group encountered a lower incidence of early severe hypocalcemia compared with patients in the BNE group, also a higher cosmetic satisfaction rate, shorter operative time, less postoperative pain and shorter hospital stay. The values of serum calcium and iPTH during 6 months of follow-up were not difference. There was also no difference for mortality.
MIVAP provides the same cure effect as conventional BNE, with advantages of lower hypocalcemia rate, higher cosmetic satisfaction rate, shorter operative time, less postoperative pain and shorter hospital stay.
Thyroid Hormone Action Friday Poster Basic
T3 is known to positively regulate mitochondrial uncoupling protein1 (UCP1) and deiodinase 2 gene transcription in BAT leading to increased thermogenesis and decreased body weight. Carbohydrate-responsive element-binding protein (ChREBP) is a glucose-responsive transcription factor (TF) that plays an important role in regulating lipogenic and glycolytic genes in white adipocytes.
Adipogenesis was induced in immortalized mouse brown pre-adipocytes using minimal adipogenic media (MAM) containing DMEM, 10% resin-stripped FBS, dexamethasone, indomethacin and insulin for 2 days. T3 was added at a concentration of 10 nM. Cells were analyzed at day 8 after the initial treatment. mRNA levels were measured by Illumina RNA-seq and qRT-PCR. Mitochondrial content was measured by FACS using Mitotracker®. Glucose and lactate were measured in the media after 6–8 days of adipogenesis. ChREBP was silenced using a lentiviral shRNA. TF binding sites were predicted using the Genomatix database.
By adding MAM to BATs, adipogenic markers such as peroxisome proliferator-activated receptor gamma (PPARg), adiponectin, leptin, and UCP1 were induced. Adding T3 to MAM between days 0–2 of adipogenesis resulted in a strong upregulation of UCP1, which correlated with mitochondrial biogenesis and with the cells becoming hypermetabolic (decreased glucose:lactate ratio), but with minimal to no change in PPARg, leptin or adiponectin transcription. In addition, we found the glucose transporter 4 (Glut4) and ChREBP mRNAs to be upregulated by T3. ChREBP, UCP1 and Glut4 have putative T3 receptor and ChREBP binding sites suggesting there is a coordinate adipogenic response between T3 and glucose in BAT. Indeed, in low glucose concentrations, UCP1, fatty acid synthase (Fasn) and Glut4 gene expression were lower than in high glucose and T3 upregulated UCP1 and Glut4 mRNA to higher levels at both glucose concentrations. As predicted, ChREBP shRNA decreased UCP1, Fasn and Glut4 mRNA levels.
We suggest T3 not only regulates UCP1 expression levels and mitochondrial biogenesis, but does so in a coordinated fashion with glucose by regulating ChREBP and Glut4 expression. The coordinated actions of T3 and glucose cause BAT cells to become hypermetabolic.
Thyroid Hormone Action Friday Poster Basic
Thyroid hormone (TH) plays a significant role in the differentiation, growth, and repair of a broad spectrum of tissues. To define the role of TH and the deiodinases in lung development we performed primary culture of human airway epithelium, containing ciliated, basal and goblet cells, in media with varying TH concentration.
Human airway epithelial cells were isolated from trachea and bronchi obtained from organ donors. Cells were harvested and plated onto collagen-coated dishes. When confluent, cells were transferred to a collagen-coated porous support (Transwell, Corning) that separates two chambers filled with standard medium containing 0.05% BSA and 10 nM T3 (∼3.5 nM free T3) for 1 week. The upper chamber was then emptied to expose the apical surface, establishing an air interface. Media conditions were then changed: cells were incubated with either media devoid of T3, 10 nM T3, or 50 nM T3 (∼17.5 nM free T3) for 3 weeks. Cells were harvested at baseline and weekly from each condition. RNA was isolated and cDNA synthesized for gene expression analysis by RT-qPCR.
Total RNA/filter increased from 6.5±0.9 to 12.7±1.2 ug over 4 weeks and was not affected by TH conditions. Ciliated cells were studied via expression of FOXJ1, a ciliated cell-specific transcription factor. In the condition devoid of T3 there was a 161-fold increase in FOXJ1 mRNA levels during the 4 week period. In contrast, addition of T3 to the media reduced this induction to only 62-fold (10 nM T3) or 74-fold (50 nM T3). Relative to 18 s, FOXJ1 expression was higher in cells exposed to the medium devoid of TH versus the 10 nM T3 medium (3.6±1.7 vs. 1.4±0.3, n=5, p<0.05) or 50 nM T3 medium (1.7±0.9, n=5, p<0.05) at 4 weeks. There was no difference in FOXJ1 between the 10 nM and 50 nM T3 conditions. Both D2 and D3 had higher expression in weeks 1–2, and then decreased; their expression was not affected by thyroid status.
TH affects the differentiation of ciliated cells in human airway epithelium. Media devoid of TH promotes greater differentiation of ciliated cells, which is inhibited by addition of 10 nM and 50 nM T3. D2 and D3 are expressed in the human airway epithelium and their role in regulating local TH signaling should be investigated.
Thyroid Hormone Action Friday Poster Clinical
Resistance to thyroid hormone (RTH) is a rare condition characterized by high T4 and T3 concentrations with normal or slightly elevated thyroid stimulating hormone (TSH). The majority of cases are due to mutations in the thyroid hormone receptor beta subunit gene (THRB). To date, 124 mutations have been identified. We report a patient with RTH due to a novel THR mutation.
Evaluation of the patient with a novel mutation of THR.
A 51-year-old man was referred for abnormal thyroid hormone levels and increased levothyroxine (L-T4) requirements. At age 24, the free T4 (FT4) and free T3 (FT3) levels were high with a normal TSH during routine pre-operative testing for ankle surgery. He was asymptomatic and denied having a goiter. He was treated with radioiodine (RAI) for presumed hyperthyroidism. He required up to 450 mcg of L-T4 daily to control symptoms of hypothyroidism. He was on 400 mcg/day of L-T4 at the time of his first evaluation in our clinic in 2012. His TSH was normal 0.82 mIU/L (0.47–4.68) with elevated FT4 3.5 ng/dL (0.7–1.9) and FT3 4.7 pg/mL (2.5–3.9). FT4 measured by direct dialysis was also high at 8.1 ng/dL (0.8–2.7). TSI, anti-TPO and thyroglobulin antibodies were negative. Alpha subunit, TBG, angiotensin-1 converting enzyme, sex hormone binding globulin and ferritin were within normal limits. MRI of the pituitary in 2012 revealed mild heterogeneity of the posterior pituitary with a 3 mm focus of hypoenhancement. Thyroid ultrasound in 2013 showed a small heterogeneous gland consistent with RAI therapy. We suspected RTH and proceeded with genetic testing which revealed a novel sequence change in one copy of the THRB gene. The novel variant Ile250Thr was caused by T to C change at nucleotide position c.749 in exon 8 of the THRB gene. Screening of the first degree relatives with thyroid function tests was recommended.
A novel mutation of the THRB gene was identified. Early recognition of RTH can improve clinical management and prevent iatrogenic morbidity from treatments for misdiagnosed hyperthyroidism.
Thyroid Hormone Metabolism & Regulation Friday Poster Basic
Various aspects of hepatic lipid metabolism are regulated through the actions of nuclear hormone receptors including thyroid hormone receptor beta (TRB). Although this regulation has been targeted in the development of thyromimetic drugs, there is need for an improved understanding of the nature of this regulation. Our studies have used targeted comparisons of metabolic and transcriptional regulation by thyromimetic drugs with the effects of specific agonists of related related nuclear receptors, CAR (NR1I3) and LXRA (NR1H3), to characterize their distinct, but overlapping effects on lipid metabolism.
We have performed focused comparisons of the genome-wide transcriptional and metabolic effects of TRB activation to CAR and LXRA activation in animal and cell culture models. Our functional analyses focused on conserved regulatory targets, including the conserved ApoA1/4/5/C3 gene cluster. We have analyzed the transcriptional regulation and chromatin interaction using chromatin binding assays and functional assays of DNA response elements to test the function of putative regulatory sites and the interaction of these receptors at these sites.
Our results indicate high levels of overlap in gene regulation by drug-induced activation of TRB, as compared to CAR and LXRA, constituting more than 30% of targets and consistent similarity of gene ontological profiles. These results include overlapping transcriptional regulation of genes in the ApoA1/4/5/C3 gene cluster, and detailed analysis found shared binding events within this regions, as well as isolation of functional regulatory elements with overlapping transcriptional responses by TRB and other receptors.
Our studies suggest a functional similarity in the aspects of hepatic lipid metabolism regulation by TRB studied here, shared with other hepatically-expressed nuclear hormone receptors, CAR and LXRA, corresponding to overlapping transcriptional regulation. In the context of the apolipoprotein genomic region studied here, overlapping regulation of target genes corresponded to shared regulation of regulatory elements, suggesting models of cooperative or antagonistic regulation.
Thyroid Hormone Metabolism & Regulation Friday Poster Basic
There has long been a desire to confer BAT-like function upon WAT as a strategy to combat obesity. Numerous recent examples have demonstrated that it is indeed possible to elicit a BAT-like program of adaptive thermogenesis in WAT, although the pharmacological potential of this action is not yet clear.
Here we demonstrate that thyroid hormone receptor (TR) activation by the synthetic agonist GC-1 or T3 induces a program of adaptive thermogenesis and uncoupled respiration in subcutaneous WAT, a process often referred to as ‘beiging’.
TR-mediated beiging is accompanied by supraphysiological thermogenesis and an amelioration of obesity and insulin resistance. Surgical denervation of BAT has no effect on systemic thermogenesis and all thermogenesis is lost in lean mice that possess little subcutaneous WAT, suggesting that the induction of thermogenesis is mediated exclusively by WAT.
These data demonstrate that TR activation can elicit UCP1-mediated thermogenesis in WAT, a previously unrecognized component of TR mediated thermogenesis, and establish the profound pharmacological potential of WAT beiging.
Thyroid Hormone Metabolism & Regulation Friday Poster Clinical
Thyroxine is both a hormone and a drug. The inability to distinguish between the administered drug and the endogenously synthesized hormone thwarted our understanding of dosing requirements in the treatment of hypothyroidism. This issue is magnified during aging when the use of radiolabeled isotopes or ingesting high doses of the hormone are unethical. Using conventional methods of analysis it is impossible to differentiate between the administered drug and endogenous T4. PK studies are conducted to determine drug absorption, distribution, metabolism and excretion for determining the appropriate use of medicines according to patient characteristics (e.g. disease, genotype of drug-metabolizing enzymes). Objective: To determine if LT4 PK changes with increased age, and determine if there are sex differences in LT4 metabolism, changes following thyroidectomy and thyroid cancer.
Thirty men and women ages 21–85 y on daily LT4 treatment were recruited. On the study day each was given its own prescribed dose using a capsule with stable-isotope labeled LT4. Subjects were followed for 14 days and 13C7LT4 was measured using tandem mass spectrometry (LC/MS/MS). LOD 0.02 pmol/mL.
1. CL/F significantly increased with increasing dose (R2=0.26) 2. CL/F increased with increasing weight (R2=0.54) or BMI (R2=0.31). However, dose normalized CL/F is not a function of weight. 3. There is no relationship between CL/F and either age or UI. 4. Median (dose and weight normalized) CL/F is higher in patients without a history of cancer. 5. Median CL/F is higher in non-thyroidectomized patients compared to thyroidectomized patients (0.85 vs. 0.505 L/h).
Females have significantly lower CL/F compared to males. Median and mean CL/F in females are approximately 3 times lower that in males (0.51 vs. 1.54 L/h). This observation is driven by the difference in weight and administered dose between males and females. Median weight in females is 63.6 Kg and median weight in males is 86.7 Kg. Dose and weight normalized CL/F is similar between males and females.
Thyroid Hormone Metabolism & Regulation Friday Poster Clinical
In the last few years a number of studies have found that metformin has a thyrotropin (TSH) lowering effect in patients with type 2 diabetes mellitus (DM2) and this effect disappears after discontinuation of the drug. Initial studies were carried out on hypothyroid patients on levothyroxine treatment. Recent data suggest that metformin effect could be related to the serum TSH level. However this was found only when the TSH level is elevated. The aim of the present study is to evaluate the changes in serum TSH levels in euthyroid DM2 patients on metformin treatment.
A retrospective study was conducted in 7 primary health care centers in northern Spain. The study included 297 euthyroid DM2 patients (120 females). Serum TSH level was tested before the initiation of metformin and the sample was divided into hierarchical clusters (C1 to C4), according to the Euclidean mean of the initial TSH level, which was within the normal range (0.72–4.43 mU/L). A dendogram was performed to decide the number of clusters. After one year of metformin treatment, TSH was tested again. We compared both TSH levels by paired t-tests.
The results are summarized in the table. In the whole sample, post-metformin TSH level was significantly higher than the basal level. However, this trend was observed only in clusters 1 and 2 subgroups (those with lower baseline TSH levels) and was lost in clusters 3 and 4.
Metformin seems to have a “buffer effect” on TSH secretion in euthyroid subjects with the lower-normal TSH level. The mechanism under this result needs to be elucidated.

Thyroid Imaging Friday Poster Clinical
It has been recommended to perform total thyroidectomy on patient with follicular neoplasm >4 cm. Our objective was to identify the impact of size upon malignancy risk in follicular neoplasm.
A total of 87 patients with follicular neoplasm who underwent thyroid surgery were evaluated. The nodule size, FNA cytology results, and final histopathology were documented. All nodules were ≥1 cm and analyzed by size: <3 cm, ≥3 cm and <4 cm, ≥4 cm.
Among 87 patients, the histopathology was malignant in 45 nodule. The malignancy rate in nodules <3 cm and ≥3 cm was 55.3% and 40.9%, respectively (p=0.32). when 4 cm used as a cutoff, the rate in nodules <4 cm and ≥4 cm was 56.1% and 40%, respectively (p=0.08).
Total thyroidectomy should not be offered to patients with follicular neoplasm solely due to large size. Increased thyroid nodule size does not influences malignancy risk in follicular neoplasm. Further multi-institutional study are warranted to examine this association.
Thyroid Imaging Friday Poster Basic
The use of ultrasound (US) has become standard in the evaluation, diagnosis and management of differentiated thyroid cancer (DTC). The majority of thyroid US are performed by radiology, where evaluation of the lateral neck for pathologic lymph nodes is not standard. As many pathologic LN are not palpable, reliance on radiology reports alone can lead to an inadequate operation being performed. The purpose of our study was to determine the impact of clinician performed US (C-US) in performing the correct initial operation for patients with DTC with lateral LN metastases.
Retrospective review of a prospectively maintained database was performed to determine the number of patients who underwent MRND for DTC between 2000 and 2013 at our tertiary referral center. All patients had C-US prior to surgery performed by one of seven endocrine surgeons. We compared our findings with that of the pre-referral imaging studies to determine how many patients would have undergone the wrong initial operation due to missed pathologic lateral LN.
During the study period 137 patients underwent MRND for DTC. Of these, 94 (69%) had pre-referral imaging of the neck (US, CT, MRI). The remainder had our C-US as their initial imaging test. Of those patients with pre-referral imaging, C-US detected non-palpable, cytologically confirmed, pathologic lateral LN not previously identified in 29 (31%). 55 of these patients (59%) had radiologist-performed US (R-US) as part of their pre-referral imaging, and 39 (41%) had other imaging modalities. Of the 55 patients with R-US, 19 (35%) had non-palpable ultrasound-detected pathologic lateral LN detected on C-US, significantly altering the surgical plan.
Absence of C-US would have led to an inadequate initial operation in one third of patients with DTC and lateral neck metastases in our study population, despite pre-referral neck imaging. Awareness of the limitations of R-US is important for clinicians evaluating patients with DTC, and C-US is critical in ensuring patients with DTC get the correct initial operation.
Thyroid Imaging Friday Poster Clinical
In order to test whether the computerized quantification of ultrasonic heterogeneity can aid the diagnosis of thyroid malignancy, we evaluate ultrasound heterogeneity by an objective and quantitative computerized method in a prospective setting.
A total of 347 participants with 404 nodules were evaluated. Among them, 4 nodules were excluded for suspicious aspiration cytology results without pathologic proofs. Among the rest 400 nodules, the diagnosis of 314 nodules was verified by surgical pathology, and the diagnosis of 86 were based on FNA biopsy results There were 271 benign thyroid nodules and 129 malignant thyroid nodules, which included 114 papillary carcinomas. Patient clinical data were collected, and the grading of heterogeneity on conventional gray scale ultrasound images was retrospectively reviewed by a thyroid specialist. Quantification of ultrasound heterogeneity was performed by a proprietary program implemented with methods proposed in this paper. The ultrasound heterogeneity index (HI) was calculated after the cystic component was excluded.
The HI between benign and malignant nodules diagnosed by combined FNA biopsy and surgical pathology results (total number, 400) showed a significant difference (p<0.001, AUC=0.714). Furthermore, we excluded patients without surgical pathology results for further validation, and the HI between benign and malignant nodules confirmed by pathology results (total number, 181) showed a significant difference (p<0.001, AUC=0.748). To learn whether our computer program increased our diagnostic capabilities, we compared HI to ultrasound heterogeneity evaluated by human investigators. In this study, ultrasound heterogeneity(US-H) evaluated by human investigators did not show significant difference between benign and malignant thyroid nodules. The marked heterogeneity of US-H evaluated by human investigators showed higher HI than homogeneous US-H did.
This new computer-aided diagnosis method to evaluate the sonographic heterogeneity of thyroid nodules is an objective and quantitative method. This new computerized heterogeneity index can aid in the diagnosis of thyroid malignancy better than traditional US-H evaluated by human investigator.

Thyroid Imaging Friday Poster Clinical
Some hypothesize that the worldwide increase in thyroid cancer rates is in part due to an increasing number of thyroid neoplasms detected incidentally by imaging done for non-thyroid related reasons. Previous studies have given an incomplete understanding of the incidental rate of thyroid nodule/cancer detection because most have been underpowered or focused only on one imaging modality. We aim to clarify the true clinical rate of thyroid incidentaloma discovery by all common imaging modalities and to describe the rate of workup and treatment of these incidentalomas.
The study cohort was identified by querying a database of all CT, MRI, and PET scans of the head, neck, or chest performed at a tertiary care referral center from January 2010 to December 2012 containing the phrase thyroid. Ultrasound scans for parathyroid disease localization were also included. Patients with known thyroid disease or head and neck cancer were excluded. Medical records were reviewed for demographics, medical history, evaluation by ultrasound, fine needle aspiration, surgical intervention and pathology data.
A total of 56,656 imaging studies comprised the study cohort: 46,438 CTs (82%), 5,361 MRIs (9.5%), 4,377 PET scans (7.8%) and 480 (0.85%) parathyroid localization ultrasounds. 190 thyroid incidentalomas were identified in the radiology reports (0.34% discovery rate). 72 were identified by CT (0.16% discovery rate), 77 by ultrasound (16% discovery rate), 22 by MRI (0.41% discovery rate), and 16 by PET (0.36% discovery rate). Ultimately, an ultrasound exam was done on 176 (93%) of the incidentalomas, and 95 (50%) of them had fine needle aspiration (FNA). Of those with FNA, 35 (36%) had a malignant or indeterminate cytology and all of these underwent surgical intervention. 13 (6.8% of incidentalomas, 0.022% of all imaging studies) were found to have thyroid cancer on final pathology.
Thyroid incidentaloma detection is much lower than previously reported. Less than half of these incidentalomas required diagnostic FNA. The extremely low rate (0.022%) of cancer diagnosis in this study suggests that the incidental detection of thyroid nodules with imaging is not contributing significantly to the rising incidence of thyroid cancer.
Thyroid Imaging Friday Poster Clinical
Thyroid nodules are common, but are rarely malignant. The current gold standard for diagnosis, fine-needle aspiration (FNA) biopsy, yields 10–25% of indeterminate cytology results, leading to patients undergoing thyroidectomy for diagnosis. ESS has been found to differentiate benign from malignant thyroid tissue ex vivo, but this study hypothesized that a smaller ESS probe, capable of in vivo applications would increase the clinical utility of this technology. We assessed the technical potential of a miniature elastic scattering spectroscopy (ESS) probe that was designed to fit into a 23 gauge FNA needle assembly to differentiate benign from malignant thyroid nodules.
We collected data in vivo using the miniaturized ESS probe on patients undergoing ultrasound-guided thyroid biopsy. A standard operating protocol (SOP) was created and refined including cleaning and sterilization, physician tool use, calibration and resterilization. Using pathology as our gold standard, spectra from the miniaturized ESS probe were compared to previous ESS data that was collected ex vivo with a larger optical geometry.
122 patients were enrolled in the in vivo study and analyzed with the ESS spectra taken from 64 patients measures with a large, ex vivo probe. ESS features were comparable between both in vivo and ex vivo probes. Measurement acquisition time for the miniaturized in vivo optical probe was under one second.
An in vivo trial of an invasive miniaturized integrated ESS biopsy probe for discrimination of benign from malignant thyroid nodules is feasible and comparable to larger ex vivo probes. Data could be normalized for analysis, and produced excellent reproducibility. Collection of ESS data during a biopsy would be both practical and reliable. With the development of a disease-specific algorithm, ESS could potentially be used as an in-situ real-time intra-operative diagnostic tool or as a minimally invasive adjunct to conventional FNA cytology.
Thyroid Nodules & Goiter Friday Poster Translational
Fine-needle aspiration biopsy (FNAB) is widely accepted as an effective procedure for diagnosing thyroid nodules. This technique is often done with a 3 or 10 cc syringe. Various studies have analyzed sampling accuracy of FNAB, and have attained a variety of results. This study evaluates the pressure-volume relationship that is generated during a thyroid biopsy in an effort to standardize one more element of the FNAB, and generate more consistent results.
A gas pressure sensor was fitted on a variety of 3 and 10 cc syringes through a leur-lock connection. Static empirical measurements were taken for each syringe size using 3 syringe bodies with 3 trials each. Measurements were taken in cubic centimeter (cc) increments. All readings were recorded at sea level. Empirical measurements were analyzed, and compared against theoretical calculations of pressure and volume.
Empirical measurements were found to be repeatable, and demonstrated a high statistical significance of P<0.001 for both the 3 and 10 cc syringe when compared to theoretical calculations. Standard deviation for each 1 cc increment on both sizes of syringe was less than 0.85 kPa. A volumetric change of 3 cc's produced 79% of the maximum suction attained from fully withdrawing the plunger of a 10 cc syringe.
The results of a FNAB have been found to be operator dependent and in an effort to maximize the diagnostic value, clinicians should be informed of the implications from the volume of aspiration. The data shows that both a 3 and 10 cc syringe is suitable for a FNAB. During a thyroid biopsy a change of 3 cc's, is sufficient for generating enough negative pressure to collect cells. After 3 cc's, increasing the volume of aspiration in the syringe will become increasingly inefficient at changing pressure. Changes in altitude and contents of a nodule will affect the amount of suction necessary to attain cells of diagnostic value. Specific implications cannot be drawn to every circumstance in which a FNAB is required; however the study discovers trends that provide insight, and establish a standard to base a needed change in clinical practice.
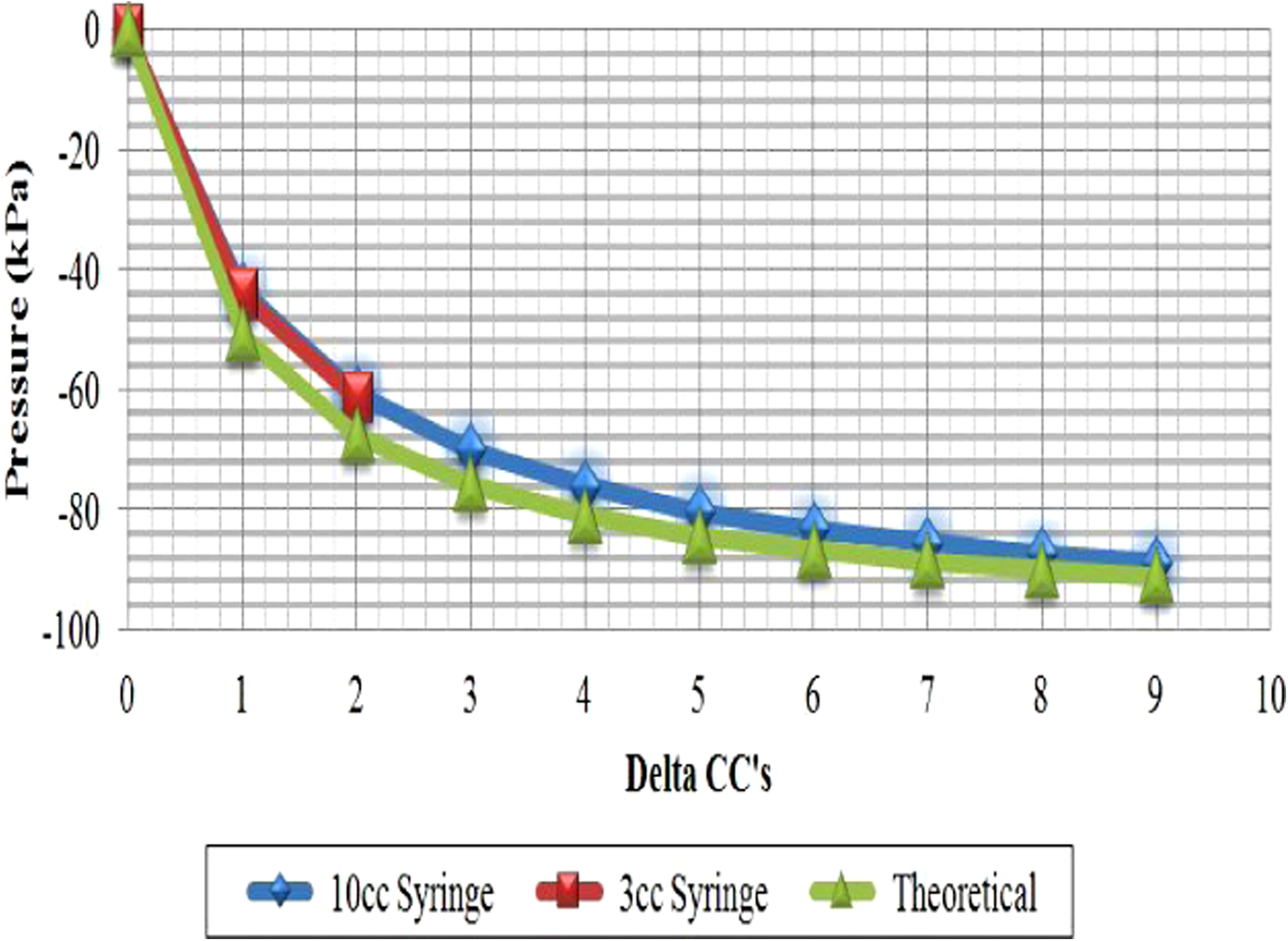
Thyroid Nodules & Goiter Friday Poster Clinical
The Bethesda System of Thyroid cytopathology classification defines Atypia of Uncertain Significance (AUS) as abnormal thyroid biopsy results that cannot be classified into other categories. A repeat biopsy as opposed to surgery is recommended, as estimated malignancy rates are felt to be relatively low. There is now accumulating data on final histopathologic outcomes in AUS. We report 198 thyroid nodules with AUS that were analyzed retrospectively.
2,106 thyroid FNA biopsies done between October 2007 and May 2012 were reviewed. The biopsy results that were reported prior to application of Bethesda System were studied and retrofitted to one of the Bethesda categories. Demographics and clinical outcomes were recorded.
We found that 210/2106 (10%) of the FNA results during the study period were AUS. 12 of these were repeat biopsies of the same nodule. Of 198 nodules that were assessed, 53 were lost to follow up leaving 145 nodules to be further tracked. 28 of the 145 or 19% of the index thyroid nodules diagnosed with AUS turned out to be malignant. 51/198 (26%) of AUS nodules went directly to surgery based upon other clinical factors (radiation, family history of thyroid cancers, patient preference or suspicious features - size, microcalcifications). 26% (13/51) of the nodules in this subgroup were malignant (77% papillary carcinoma, 15% follicular carcinoma, and 8% lymphoma). The Bethesda recommended repeat FNA was done in 105/198 (53%) of nodules with no clinically worrisome features. 44/105 (48%) of repeat FNAs in initially AUS patients confirmed AUS or more worrisome categories. 21/27 (78%) of those with a confirmatory AUS underwent surgery where 6/21 (29%) had papillary thyroid cancer on the nodule under investigation. One of the 5 (20%) nodules initially diagnosed AUS but later reported as benign on rebiopsy was found to be malignant after undergoing surgery for suspicious features.
Following the cytologic diagnosis of AUS, 19% of nodules proved to be malignant. Regardless of the outcome of the second FNA, the repeat FNA strategy results in about the same rate of malignancy detection rate as after a single AUS result. Reconsideration of the repeat FNA strategy to enhance outcomes should be a priority.
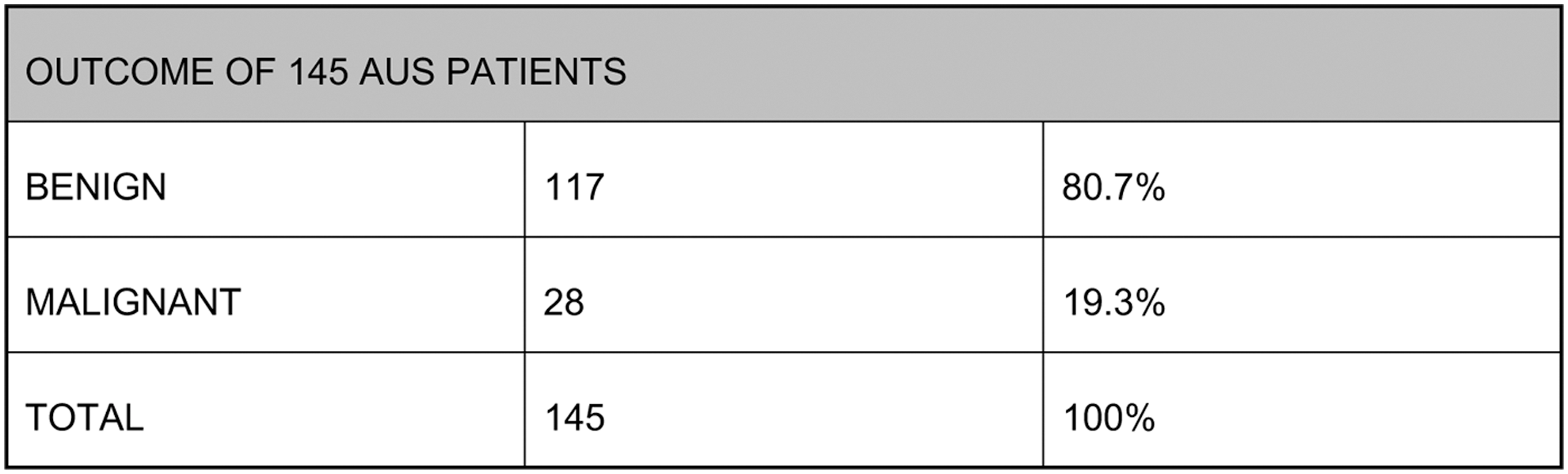
Flowsheet of the biopsied nodules.

Thyroid Nodules & Goiter Friday Poster Clinical
Certain orally ingested compounds and drugs impair the intestinal absorption of tablet levothyroxine (LT4), which is the classic formulation of this hormone. In our country, a novel formulation available is LT4 as oral solution (OS), in which sodium LT4 is solubilized in ethanol and glycerol. Because OS-LT4 lacks a gastric dissolution phase, it is directed faster to the hormone sites of absorption in the upper intestine, thus being less prone to the said impaired absorption. Using serum TSH as a marker of optimal absorption, we tested the hypothesis of better absorption of OS over tablet LT4 in patients with PPI-induced malabsorption of LT4 tablets.
Upon informed consent, 18 adult patients with tablet LT4 malabsorption due to PPI (8 omeprazole, 6 pantoprazole, 4 lansoprazole) were switched to the same daily dose of OS-LT4. Three patients also were taking other drugs known to interfere with LT4 absorption: one patient was taking calcium salts, a second patient was taking ferrous salts, while a third patient was taking both calcium and ferrous salts. Tablet LT4 was taken for replacement purposes (REP, n=9) or TSH-suppressive purposes (SUP, n=9). TSH (in mU/L) was assayed at least twice in each patient, starting from two months after the switch. Data are m±SD, and statistics is based on Wilcoxon and Fisher's exact tests.
Serum TSH was significantly lower under OS compared with tablet both in the REP group (1.69±0.95 vs. 5.10±5.10, P=0.003) and in the SUP group (0.15±0.22 vs. 1.15±1.85, P<0.0001). Moreover, in SUP patients, the number of serum assays with TSH<0.10 mU/L was 25/34 (73.5%) under OS, compared with none under tablet (0/19, P<0.0001).
OS-LT4 is absorbed far better than tablet LT4 in patients who are taking PPI alone or PPI plus other drugs that impair the LT4 intestinal absorption. Because OS-LT4 permits serum TSH to reach target levels, frequent repeated assays of TSH consequent to dose adjustments of tablet LT4 can be avoided.
Thyroid Nodules & Goiter Friday Poster Clinical
Thyroid nodules are common. The current gold standard, fine-needle aspiration biopsy (FNAB), yields 10–25% indeterminate results necessitating thyroidectomy for diagnosis. Elastic scattering spectroscopy (ESS) is a minimally invasive optical-biopsy technique, mediated by a fiberoptic probe that can fit through a 23 gauge needle. We hypothesized that combining a real time diagnostic test with high sensitivity (FNAB) to one with a high specificity (ESS) might increase the clinical utility.
We built a miniaturized ESS-integrated biopsy syringe that can fit through a 23-gauge biopsy needle and assessed the potential of ESS to pre-operatively differentiate benign from malignant thyroid nodules. An IRB approved protocol was conducted on patients undergoing ultrasound-guided FNAB of thyroid nodules. Cells and ESS data were collected from within the thyroid nodule. Post-surgical pathology was our gold standard for indeterminate cytology. Leave-one-out cross-validation was used to obtain performance estimates in the form of sensitivities and specificities.
All patients tolerated the procedure well; additional time to perform ESS measurements required less than 20 seconds. A significantly altered spectrum was noted between solid and cystic portions of the thyroid nodule. Using the real time feedback of ESS, the spectroscopy tool was guided towards solid tissue to collect cells, and yielded an insufficiency rate of 2.5%. A waveform signature could discriminate benign from malignant disease. Preliminary results show a NPV of 0.99, a sensitivity of 0.92 and a specificity of 0.85.
ESS can reduce the number of indeterminate nodules that require surgical treatment. Additionally, this technology can decrease insufficiency rates of FNAB by avoiding microscopic cystic areas that cannot be visualized with ultrasound. Analysis reveals a unique waveform signature that can differentiate solid from cystic fluid and benign vs. malignant thyroid nodules to improve targeting of biopsies. With the collection of further data, an algorithm using cytology and ESS data could potentially be used as an in-situ real time minimally invasive adjunct to conventional FNA cytology to improve diagnosis and prevent unnecessary surgery.
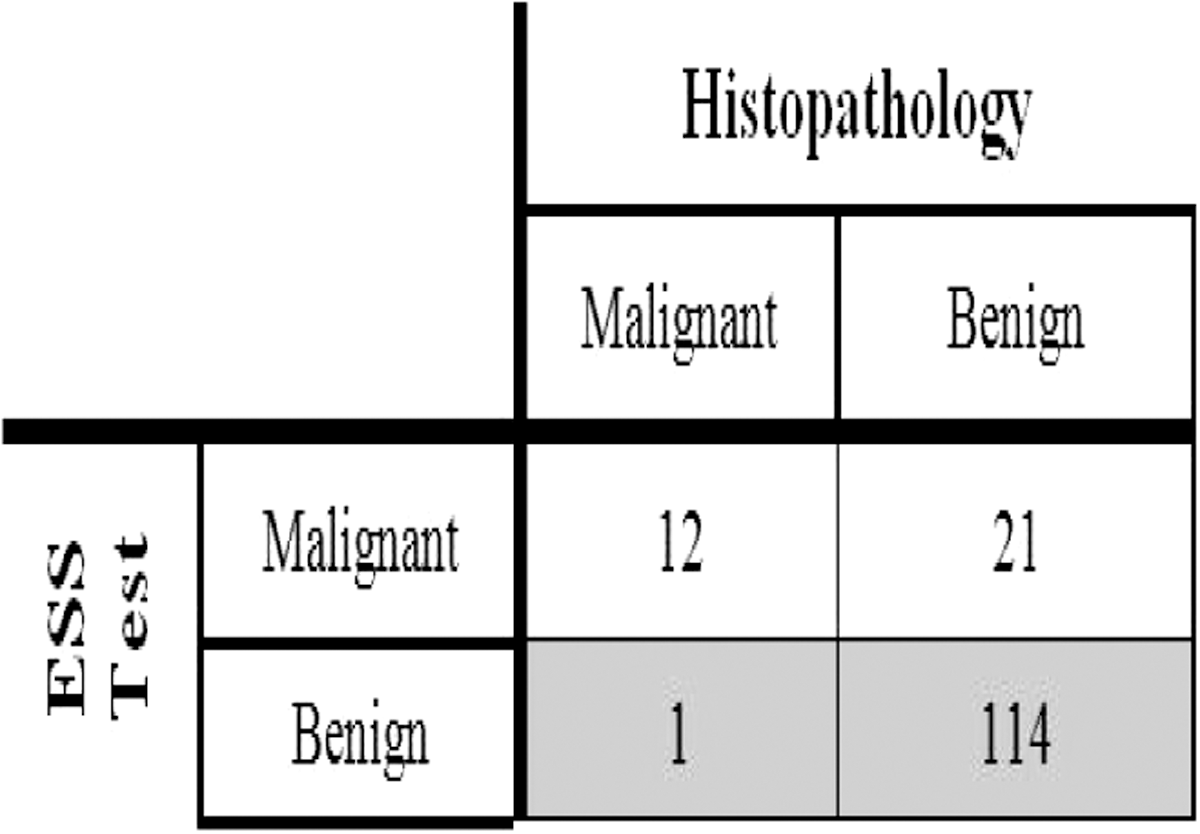
“Leaveone-out” cross-validation done for ESS spectra.
Thyroid Nodules & Goiter Friday Poster Clinical
Reported complication rates following re-operative thyroid surgery vary widely. Local data are increasingly compared with national figures and in the UK will form an integral part of re-validation and surgical unit review. An awareness of local differences in cohort characteristics, particularly in tertiary centers, is vital if accurate direct comparison to national data can be made.
Prospective data for consecutive thyroid operations between January 1993 and January 2013 were collected. All cases of re-operative thyroid surgery were identified and analyzed for patient demographics, surgical indication and complications. Cohort data were compared to national data presented in the British Association of Endocrine and Thyroid Surgeons (BAETS) 2012 national audit report.
A cohort of 1657 patients who underwent thyroid surgery at the Queen Elizabeth Hospital Birmingham, UK were identified, of which, 164 (10%) had re-operative procedures. Comparison with national data showed our cohort to be a significantly younger group with a higher proportion of males (p<0.01). Complications rates within our cohort were significantly higher than national data for transient hypoparathyroidism and transient recurrent laryngeal nerve (RLN) palsy but lower for permanent hypoparathyroidism and permanent RLN palsy (p=0.03). Subgroup analyses showed our re-operative cases to be a significantly older group with higher co-morbidity and a significantly higher rate of haematoma formation (p<0.01). Re-operative cases for initial benign disease also saw a significant increase in the rate of permanent RLN palsy.
An awareness of differences between surgical unit cohort and national data is vital when making direct comparisons, especially in an era where data are freely available for public scrutiny. Much of the difference identified here is likely to be indicative of the case mix of a tertiary center with proportionally more complex and malignant disease. An in depth understanding of surgical unit outcomes in relation to cohort characteristics is vital for successful and accurate comparative analysis.
Thyroid Nodules & Goiter Friday Poster Clinical
Percutaneous Ethanol Injection Treatment (PEIT) has been used over 15 years in selected cases to treat both benign and malignant thyroid lesions. Because levothyroxine suppression therapy has not proven to be very effective in nodules larger than 10 ml in volume, surgery has been the first choice treatment for these lesions. Nonetheless, patients who reject surgery or have a poor surgical prognosis can benefit from PEIT. To the best of our knowledge, no data has been previously published in Mexico for PEIT.
We present the first 7 procedures of PEIT in mexican patients, 5 females and 1 male (2 procedures were done in two different hot nodules in the same female patient) aged between 19 and 75 years of age. 6 were hyper-functioning nodules, 1 was a large (10.89 cc) non-functioning nodule. All patients underwent previous ultrasound guided FNAB, all were reported as class II by the Bethesda Classification. PEIT was done by ultrasound guidance, and 97% ethanol was used in all procedures. The total volume injected was calculated at 1 cc per 1 cc of nodule volume, divided between 3 to 5 sessions.
Of the 6 hyper-functioning nodules, treatment success (defined as normalization of Total T3, T4 and FT4 levels and a TSH level above 0.50) was achieved in 5 and partial success (normalization of Total T3, T4 and FT4 levels but with TSH below 0.5) in 1. All 7 nodules treated showed volume reduction, with and average reduction of 71% (range 50 to 91%). The most common complication was pain and swelling of the injection site that lasted around 36–48 hours, 1 patient suffered a laryngeal spasm that had to be treated with IV steroids and fully reverted in 30 minutes and 1 patient had ethanol extravasation to the ipsilateral ECM muscle.
Our first reports show PEIT to greatly reduce nodule volume and successfully treat the underlying hyperthyroidism in 5 out of 6 cases and partially treat the remaining case.
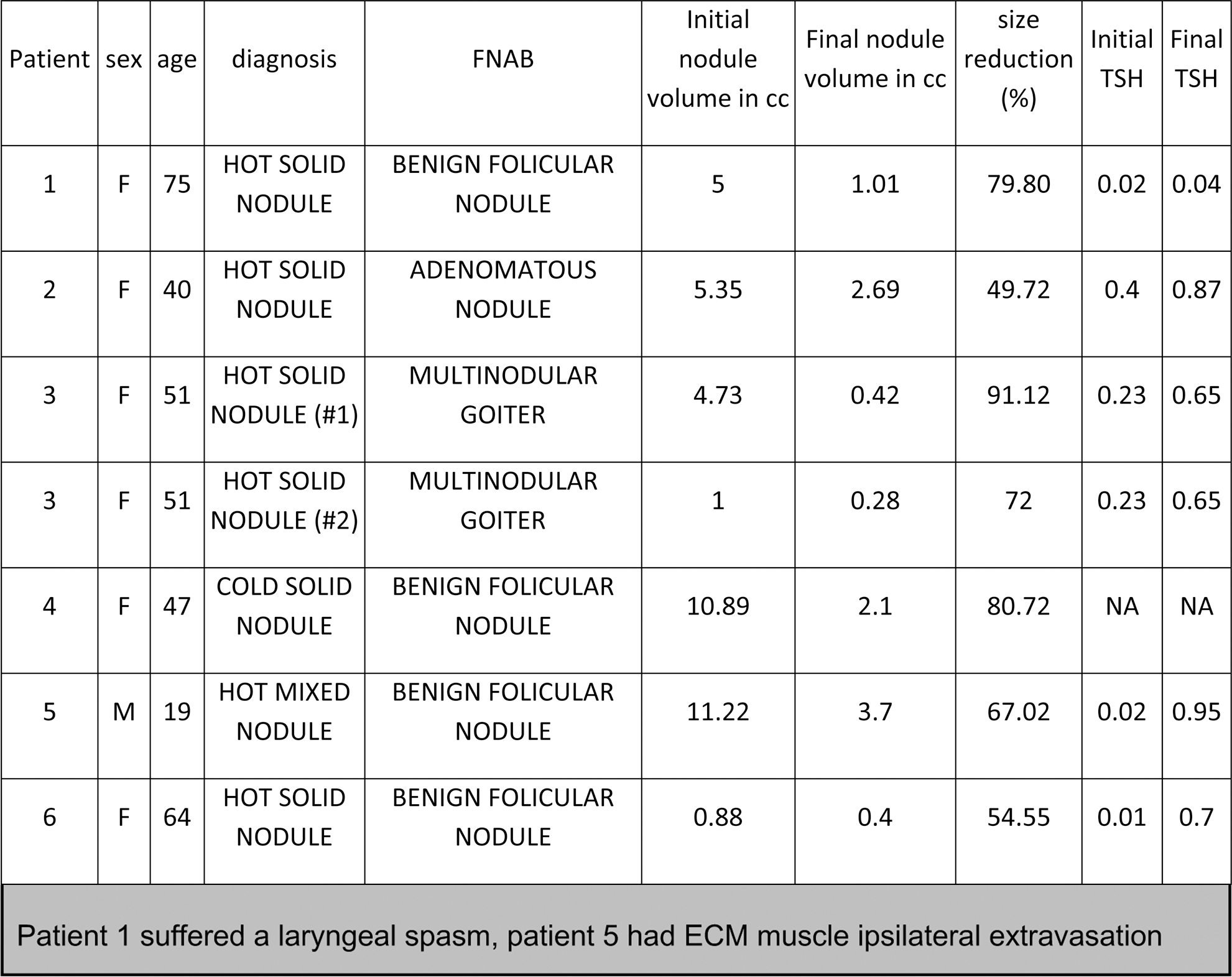
Thyroid Hormone Action Friday Poster Basic
The bioactive thyroid hormone (TH) T3 has pleiotropic effects in early and adult life in vertebrates by binding to the thyroid hormone receptors (TR) in the cell nucleus and promoting or blocking gene transcription. We have shown that another TH, 3,5-diiodothyronine (3,5-T2 or T2), induces the transcription of genes in the same way as T3 in fish, and activates a specific isoform of the TRβ1 different from that activated by T3. These isoforms differ in the presence (long or L-TRβ1) or absence (short or S-TRβ1) of a 9-amino acid insert in the ligand binding domain of the receptor. Results from binding and competition assays show that T2 binds to L-TRβ1 with high affinity and suggest that it may exert its effects through this receptor in fish. T2 has a lower affinity for the human TRβ1, which correlates with the effects reported in mammals.
In order to further understand T2 action mechanism, two approaches were followed. 1) The regulation of T2 signalling pathway was analysed ex-vivo. To this end, organotypic tilapia liver cultures were standardized. Hepatic slices were treated with different concentrations (0.1–100 nM) of T3 and T2 for 24 hours and the expression of the two isoforms of TRβ1 was assessed (qPCR). 2) The protein composition of the transcriptional complex involved in T2+L-TRβ1 mediated gene expression was explored. To this end, two-hybrid assays were conducted to screen tilapia liver cDNA libraries in the presence of 1 μM of T2 and employing L-TRβ1 as a bait.
Our results showed that L-TRβ1 was down-regulated in a dose-dependent manner by T2, while S-TRβ1 expression decreased only with T3 treatment, confirming that each bioactive TH regulates the expression of the TR isoform that mediated their genomic effects. Furthermore, two-hybrid assays identified a specific interaction of T2+L-TRβ1 with the coregulator Jab1.
Together, the present results suggest a different signaling pathway for each bioactive TH in teleosts and allow the proposal that there is an extra level in the cascade of TH signaling in which 3,5-T2 is specifically made and regulated for this purpose. (Acknowlegments: Patricia Villalobos for technical support, grants PAPIIT IN208511 and CONACyT 166357).
Thyroid Nodules & Goiter Friday Poster Case Report
A 42-year-old Nicaraguan woman status-post liver transplant 4 months prior to admission presented with 3 week history of fevers and severe anterior neck pain. She had previously lived in California and Texas. Home meds included tacrolimus, trimethoprim/sulfamethoxazole, lamivudine for donor +hepatitis B, and ganciclovir for donor +CMV. Symptoms persisted despite one week of empiric broad-spectrum antibiotics; endocrinology was consulted for consideration of thyroiditis.
Exam revealed a normotensive female in moderate distress with fever, tachycardia and tachypnea. No exophthalmos. Thyroid exquisitely tender to palpation, diffusely enlarged, smooth, and mobile without distinct mass. Perithyroidal tissue demonstrated bogginess with left cervical lymphadenopathy.
Labs on admission showed leukopenia, normal liver enzymes, TSH 1.68 μIU/ml, free t4 0.93 and T3 77.4 ng/dL. On US thyroid was enlarged and heterogenous without definite nodules. Noncontrast CT showed normal thyroid, bilateral innumerable lung nodules and an ill-defined hepatic hypodensity. Extensive infection workup including BAL, liver biopsy and thyroid FNA was performed; cytology sample was not obtained from the scant serosanguinous aspirate. Empiric voriconazole was initiated with resolution of fever and neck pain within 48 hours. Repeat CT showed improvement in the lung nodules. All cultures were negative save for the thyroid specimen, which was positive for Coccidioides immitis. Antifungal was changed to oral fluconazole with a plan for indefinite therapy; tacrolimus dose was decreased to achieve about half of the prior target while staying within the therapeutic range. The donor's other organ recipients were without infectious symptoms. Two months later she remained clinically well but developed two enlarging, extremely firm, hypoechoic thyroid masses that yielded insufficient cytology sample from FNA; fungal culture was negative.
This is a rare case of infectious thyroiditis due to disseminated coccidiomycosis, most likely from reactivation after initiation of immunosuppressants. This may represent the first case report of thyroid mass formation as a consequence of immune reconstitution syndrome after coccidiomycosis thyroiditis.
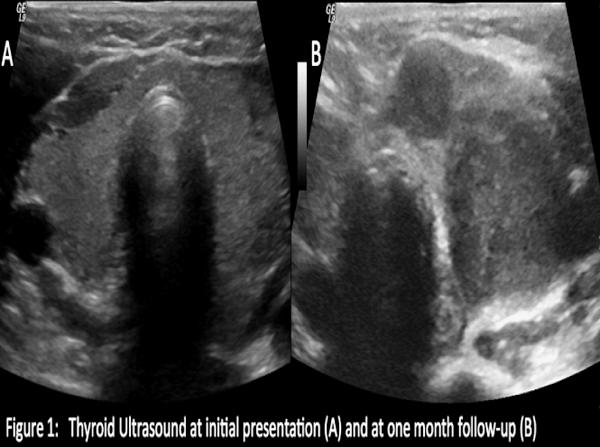
Disorders of Thyroid Function Friday Poster Case Report
A 39 year old female presented with worsening exertional dyspnea and bilateral leg swelling for one month. She reported palpitations, night sweats and weight loss for a year.
Examination showed regular pulse of 113 per minute, blood pressure 142/81 mmHg and oxygen saturation 96%. She had an enlarged thyroid, jugular venous distention, hepatomegaly, fine tremors and bilateral pitting leg edema. Echocardiogram showed left ventricular systolic function of >55% with right atrial enlargement, right ventricular hypertrophy, moderate to severe tricuspid regurgitation and moderate pulmonary hypertension with pulmonary artery systolic pressure (PASP) of 59 mmHg. TSH level was undetectable (<0.010 uIU/ml) with markedly elevated free T4 (>8 ng/dL). Total T3 and free T3 were 532 ng/dL and 22 ng/dL, respectively. Thyroperoxidase antibody was 7121 U/ml and thyroid-stimulating antibody index was 5.6. Thyroid ultrasound showed diffusely enlarged thyroid without discrete nodules. Work-up for secondary causes of pulmonary hypertension was negative. The patient was diagnosed with isolated right heart failure (RHF) and pulmonary hypertension (PH) secondary to Graves disease and started on methimazole, beta blocker and diuretic. She was noted to have significant improvement and was discharged. On 2-week and 1-month follow up, dyspnea has resolved, TSH was still <0.010 but free T4 and T3 improved to 0.93 ng/dl and 6.24 pg/ml, respectively. PASP improved to 41 mmHg after five months.
PH in hyperthyroidism is increasingly being reported. Although the mechanism is uncertain, the reversal of PH following restoration to a euthyroid state supports a causal relationship. PH with isolated RHF is a rare presentation of hyperthyroidism, with only 11 cases we found to date. It is potentially reversible with treatment of hyperthyroidism. Nakchbandi, et al proposed a possible autoimmune phenomenon causing endothelial damage, or excess thyroid hormone increasing the cardiac output and increasing metabolism of vasodilating substances. RHF without PH and vice versa has also been described. Evaluating for hyperthyroidism in patients with RHF and PH is recommended as these may reverse with antithyroid treatment.
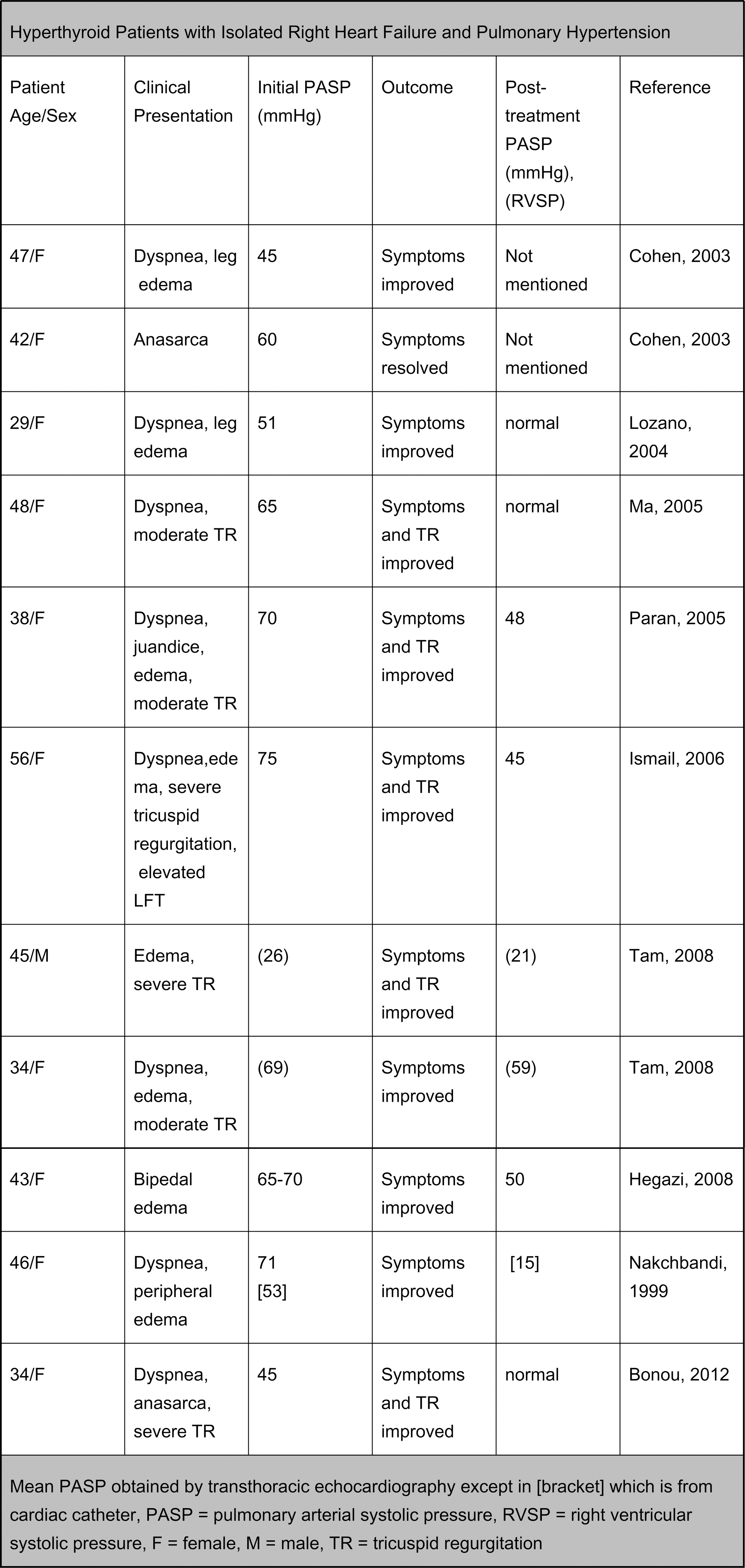
Disorders of Thyroid Function Friday Poster Case Report
Gestational trophoblastic disease (GTD) is a rare complication of pregnancy that may be associated with thyrotoxicosis. Complete mole has the highest incidence of thyrotoxicosis. It affects predominantly younger women and presents with vaginal bleeding most of the time. Hyperthyroidism in hyperemesis gravidarum occurs with greater frequency than in normal pregnancy. We describe a case of hyperthyroidism secondary to molar pregnancy highlighting the rare but important evaluation of hyperthyroidism in women of child-bearing age.
20-year-old woman presented to Emergency Room with history of nausea, weight loss of about 20 lbs in 6 weeks, and intermittent vaginal bleeding. On examination she had sinus tachycardia at 108 bpm and the ultrasound of her enlarged uterus was consistent with molar pregnancy.
Her TSH was <0.07 mIU/mL (0.3–4.2 mIU/mL), freeT4 was 5.59 ng/dL (0.8–2.0 ng/dL), total T3 was 465 ng/dL (40–180 ng/dL) while her HCG was close to 2 million mIU/mL. The patient had dilatation and curettage for evacuation of the mole. She required intubation and had prolonged hospitalization but stabilized and was discharged in good condition. Histopathology of all aborted specimens verified the diagnosis of partial mole including a dystrophic fetus. HCG values decreased to below detection after 12 weeks.
GTD with thyrotoxicosis is a rare clinical scenario but thyroid hyper-stimulation can have sever clinical consequences. The analogy in the structure between human chorionic gonadotropin (hCG) and thyroid stimulating hormone (TSH) can cause their cross-reactivity. Molecular variants of hCG found in molar pregnancies have increased thyrotropic potency. As gestational trophoblastic disease causes a significant rise in HCG levels it may induce secondary hyperthyroidism that requires treatment. As expected, thyrotoxicosis resolves with treatment of GTD and normalization of HCG levels. The development of hyperthyroidism is largely influenced by the level of HCG and usually resolves with treatment of GTD. The consideration of this etiology of hyperthyroidism should be diagnosed early and managed efficaciously before imminent dilattage and curatage is required for definitive management of molar pregnancy.
Disorders of Thyroid Function Friday Poster Case Report
After neonatal screening, hypothyroidism is diagnosed early and it is treated as soon as possible.
We want to report a girl, 17 year old, with thyroid agenesis. She was congenital hypothyroidism ten years ago, but she didn't take any medication for hypothyroidism.
She was mental retarded and dwarf. She has basal ganglia, pineal gland, adrenal gland and vascular calcification.
After neonatal screening program, severe hypothyroidism is almost uncommon. If a child with hypothyroidism don't take treatment long time, multiple calcification and related organ dysfunctions are observed.
Thyroid Cancer Friday Poster Case Report
Salivary glands are exposed to high dose radiation in thyroid radioiodine (I-131) therapy but salivary gland tumors following I-131 ablation is uncommon. We present a case of this rare association.
A 64 year old female with history of metastatic papillary thyroid carcinoma (PTC) underwent total thyroidectomy in February 1989 followed by radioiodine ablation. She initially received her 50 mCi of I-131 in May 1989 but developed recurrence of PTC and then received a second dose 146 mCi of I-131 in 1994. She was given suppressive levothyroxine therapy and her PTC was in remission with negative neck and thyroid ultrasound (US), whole body scan (WBS), and undetectable thyroglobulin (Tg) and anti-Tg Antibody (Ab) levels. In July 2009 she had recurrence of metastatic PTC at level 3 and 4 lymph nodes but she did not receive radioiodine ablation at that time. In 2012, she reported a painful lump around right jaw without associated dry mouth, or dry eye. US guided FNA of right parotid gland initially reported PTC. Subsequently she underwent right parotidectomy; however, pathology revealed mucoepidermoid cancer of parotid gland. This was considered to be potentially related to the cumulative dose of 203 mCi of I-131 she received over 23 years and 10 months.
Beta rays emission from I-131 causes death of thyroid cancer cells and is carcinogenic to the organs that contain sodium-iodide symporters that take-up I-131 such as salivary glands. The development of secondary malignancies after I-131 is associated to be dose-related and the latency period varies between 2 to 24 years in as in this case. Mucoepiermoid cancer of parotid gland has been reported after receiving 100 mCi of I-131 for PTC.
Salivary gland tumor should be included in differential diagnosis of after high dose of I-131 therapy for thyroid cancer.
Thyroid Cancer Friday Poster Case Report
A 19 year old female with familial adenomatous polyposis (FAP) syndrome was found to have a thyroid nodule on routine exam. She denied dysphonia, dysphagia or dyspnea. Her family history is significant for FAP in her father and sister. She does not have a family history of thyroid nodules or cancer. Thyroid ultrasound showed a 1.8 cm right and 1.3 cm left sided thyroid nodules with intranodular vascularity.
Biopsy was performed and cytology revealed papillary thyroid carcinoma (PTC). She underwent a total thyroidectomy and central compartment lymph node dissection. Surgical pathology was consistent with PTC, cribriform-morular variant (Image 1). The tumor was 1.5 cm on the right and 1.2 cm on the left with negative margins bilaterally. Bilateral central compartment nodes were negative for tumor. She was staged as Stage 1, pT1pN0MX.
The relation between familial adenomatous polyposis (FAP) and thyroid carcinoma was first described in 1968. In 1994, Harach et al. demonstrated unique histological features of FAP-associated PTC such as a cribriform pattern. Two types of cribiform-morular variant(CMV) PTC were identified: FAP associated and sporadic. It is commonly seen in young females under 30 years of age and presents either as a thyroid nodule or during screening of FAP patients for thyroid nodules. Unlike the other variants of PTC, up to 75% of FAP-associated CMV and 37% of sporadic CMV were diagnosed as or highly suspected of CMV on cytology. While sporadic forms usually appear as an isolated tumor, the cases associated with FAP are often multifocal due to somatic mutations within the gene. In 25–30% of cases, PTC-CMV might provide the first indicator of an underlying FAP syndrome. PTC-CMV usually shows an indolent character and rarely has extra-thyroidal extension. Total thyroidectomy is recommended but extensive lymph node dissection is not necessary.
This case illustrates the close association of FAP with an uncommon variant of PTC that has an indolent course. Patients diagnosed with CMV should undergo screening for colonic polyps and patients with FAP should be screened for thyroid nodules for early detection of thyroid cancer.

Surgical pathology of right lobe specimen demonstrating papillary, follicular and cribriform-morular (arrow) variants of PTC.
Thyroid Cancer Friday Poster Case Report
Typically the diagnosis of solitary hyper functioning hot nodule in radionuclide imaging can almost always rule out malignancy in a thyroid nodule. We report a case in which such a nodule was found to be Follicular thyroid cancer.
59 year old Hispanic female presented with 12 pound weight loss over six months. 6 cm well-defined, hard nodule was palpable in left thyroid lobe with no cervical lymphadenopathies. No diarrhea/vision problems/heat intolerance/palpitations/compressive symptoms. No FH thyroid problems or exposure to radiation in the past. TSH<0.01 (0.35–5.5 uIU/ml) FT4 (0.89–1.76 ng/dl) consistent with subclinical hyperthyroidism. Ultrasound - 5.8 cm heterogeneous solid mass with few cystic areas and increased vascularity in left lobe. NM scan 12% uptake in 24 hours with hot nodule on the left. FNA- Indeterminate with follicular cells in macro & micro follicular pattern with oncocytic changes. Patient underwent left lobectomy and final pathology came back as Follicular carcinoma (3.8 cm size, No lymphovascular/perineural/extrathyroidal invasion. Hence she underwent subsequent total thyroidectomy for Stage 2 PT2 Nx Mx. Currently is scheduled for RAIA.
Prevalence of thyroid nodules in US is 4–7%. Around 5% are malignant; hence the main goal of evaluating thyroid nodules is differentiation of hyperplasia from true neoplasms. Nuclear imaging helps determine if thyroid nodule is functioning/hot or nonfunctioning /cold. Majority are cold, and about 10% of those are malignant. 5% of all nodules are hot and less than 1%of those are malignant. In our case despite the nodule being hot, final pathology was cancer. Very few such cases have been reported in literature previously.
In conclusion our case underlines the clinical importance of predicting the incidence of malignancy in hot thyroid nodules. FNA should be done in all such nodules so that malignancy is not missed.
Thyroid Cancer Friday Poster Case Report
Thyroid nodules were incidentally discovered in a 34-year-old man on CT neck done to rule out neck injury after a fall. Neck ultrasound confirmed the presence of a 3.6 cm right thyroid nodule with ill-defined borders containing microcalcifications and internal flow. Additional 1.9 cm solid nodule in left thyroid isthmus and 2.7 cm solid nodule with few microcalcifications in inferior left thyroid lobe were also identified. Ultrasound-guided fine needle aspirations of the three nodules were all positive for PTC. No history of radiation exposure, family history of thyroid cancer or thyroid dysfunction was elicited. His initial TSH and free T4 were normal at 1.19 and 0.86 respectively. Thyroid peroxidase and thyroglobulin antibodies were negative. He had history of relapsing-remitting type multiple sclerosis treated with IFNβ 1a for 4 years. He underwent total thyroidectomy with left central and superior mediastinal lymph nodes dissection. Pathology revealed four PTC foci with largest tumor dimension of 3.5 cm involving both left and right thyroid lobes. Seven out of seven lymph nodes were positive for metastasis. Val600Glu (c.1799 T>A) mutation in codon 600 of the BRAF gene was also detected. Immune profiling of ex-vivo aspirated lymphocytes present in the thyroid tumor microenvironment revealed a never described Foxp3-negative immune-regulatory array.
Thyroid autoimmunity and dysfunction are well-known side effects of IFN. Clinical hyperthyroidism, hypothyroidism, presence of thyroid antibodies as well as goiter have been associated with either IFNβ 1a or 1b treatment in one study. However, association of PTC and IFNβ 1a treatment has never been reported. We hypothesize here that treatment with IFNβ 1a immune-modulation may facilitate development of PTC. “Non-classic” regulatory lymphocytes are found in the immune microenvironment of many human conditions spanning from autoimmune diseases to inflammation, infection and cancer. These cells might potentially play a role in promoting/facilitating PTC development.
Thyroid Hormone Action Friday Poster Case Report
Cardiac arrhythmias in thyrotoxicosis are usually seen as sinus tachycardia and atrial fibrillation but conduction abnormalities in the form of heart blocks do occur in rare instances. We present here 4 hyperthyroid patients with complete heart blocks.
This is a case series of 4 patients with hyperthyroidism-induced heart block seen at the Philippine General Hospital.
Cases 1 and 2 are young women diagnosed with Graves' disease who both experienced syncope and were seen to have 3rd degree atrio-ventricular block. Case 3 is a young adult woman who presented with palpitations, fever and shortness of breath. Her 12 lead ECG showed diffuse ST-segment elevation consistent with pericarditis and complete heart block. Case 4 is a young male with enlarged anterior neck mass and hyperthyroid symptoms who was not cleared for thyroidectomy due to 3rd degree AV block.
Conduction problems in hyperthyroidism can be due to overwhelming thyroid hormones per se and contributed by acute infections, use of rate control drugs, electrolyte imbalances, and cardiac anomalies. Resolution of clinical, electrophysiological, and biochemical abnormalities occurred in our patients after achieving euthyroidism.
Thyroid Cancer Friday Poster Case Report
Papillary thyroid carcinomas characteristically behave in a more indolent manner in comparison to most other epithelial cancers, and is touted to have a good prognosis when diagnosed early. However, when neglected, these tumors may prove to be locally invasive and in rare instances, transform into large ulcerating masses.
We report the case of a 54-year-old Filipino man with a twelve-year history of a gradually enlarging left-sided neck mass. He denies having had any hyperthyroid or hypothyroid symptoms and any compressive symptoms. He never sought any medical consult prior to his admission, when he presented at the emergency room with a firm, nodular anterior neck mass measuring approximately 15×12 cms, with multifocal ulcerations and profuse bleeding. Fine needle aspiration biopsies were inconclusive. Neck CT scan revealed a 15.7×15.1×13.4 cm enhancing, soft-tissue mass at the left side of the neck with solid and cystic components and calcifications, extending superiorly at the level of the mandible and inferiorly into the thoracic inlet. Total thyroidectomy was done.
Intraoperatively, the left thyroid lobe, measuring 17×10×7cm was noted to be encasing the left internal jugular vein, while the right thyroid lobe, measuring 4×2×1cm, had multiple small nodules. There was also note of confluent neck nodes. Final histopathology revealed papillary thyroid carcinoma of the left thyroid lobe, with extension into perithyroidal soft tissues and overlying skin and and 15 of the 17 harvested lymph nodes were positive for cancer. The right thyroid lobe was free of malignancy. He is scheduled to undergo radioactive iodine ablation.
The case illustrates the capacity of papillary thyroid cancer for local invasion and capability to achieve immense dimensions - complications that may be circumvented with timely intervention.

Preoperative gross tumor
Thyroid Nodules & Goiter Friday Poster Case Report
Mutation of the phosphatase and tensin homolog (PTEN) tumor suppressor gene leads to PTEN hamartoma tumor syndrome (PHTS) that includes Cowden's syndrome, Bannayan-Ruvalcaba-Riley syndrome (BRRS) and Proteus-like syndromes. Patients with PHTS are at risk for developing thyroid disease, such as multinodular goiter, thyroiditis, papillary and follicular thyroid cancer. We are unaware of any previous report of a patient with BRRS with hyperthyroidism due to Graves' disease.
A 26 year-old man with a history of macrocephaly, mental retardation, lipoma of the skull and freckled penis was diagnosed at age 19 with BRRS, PTEN mutation positive. There were no signs of thyroid disease until he presented with a goiter and symptoms of hyperthyroidism. See table for laboratory data. Thyroid US revealed a markedly enlarged thyroid (right lobe 3.3×2.7×7.7 cm, left lobe 4.9×3.8×8.3 cm) and innumerable solid nodules, with the largest (6 cm) in the left lobe. RAI uptake and scan were not obtained due to his baseline agitation. He started methimazole (MMI) 20 mg/day with a subsequent increase to 30 mg/day. Despite clinical and biochemical improvement over 10 months, the goiter progressively enlarged leading to dysphagia and symptoms of airway obstruction. CT scan of the neck showed a massively enlarged thyroid (right lobe 5.8×4.9×10.1 cm, left lobe 6.4×5.3×10.3 cm) with 50% narrowing of the hypopharynx and right to left deviation of the upper airway. He had a 10-day preparation for thyroidectomy with SSKI, MMI, propranolol and prednisone. Pathology revealed a 219 gm gland (right lobe 6.0×4.0×10.0 cm; left lobe 8.5×5×10.0 cm) with changes of Graves' disease, multiple adenomatoid nodules typical of BRRS, a left lobe 7 cm follicular adenoma and no malignancy.
Our patient is the first documented case of Graves' disease with hyperthyroidism in PTHS. The unusual clinical course of rapid goiter growth in spite of clinical and biochemical improvement may be an exaggerated response of the thyroid to changes in TSH with decreased thyroid hormone feedback on MMI. A potential role of the PTEN mutation in this response remains to be investigated.
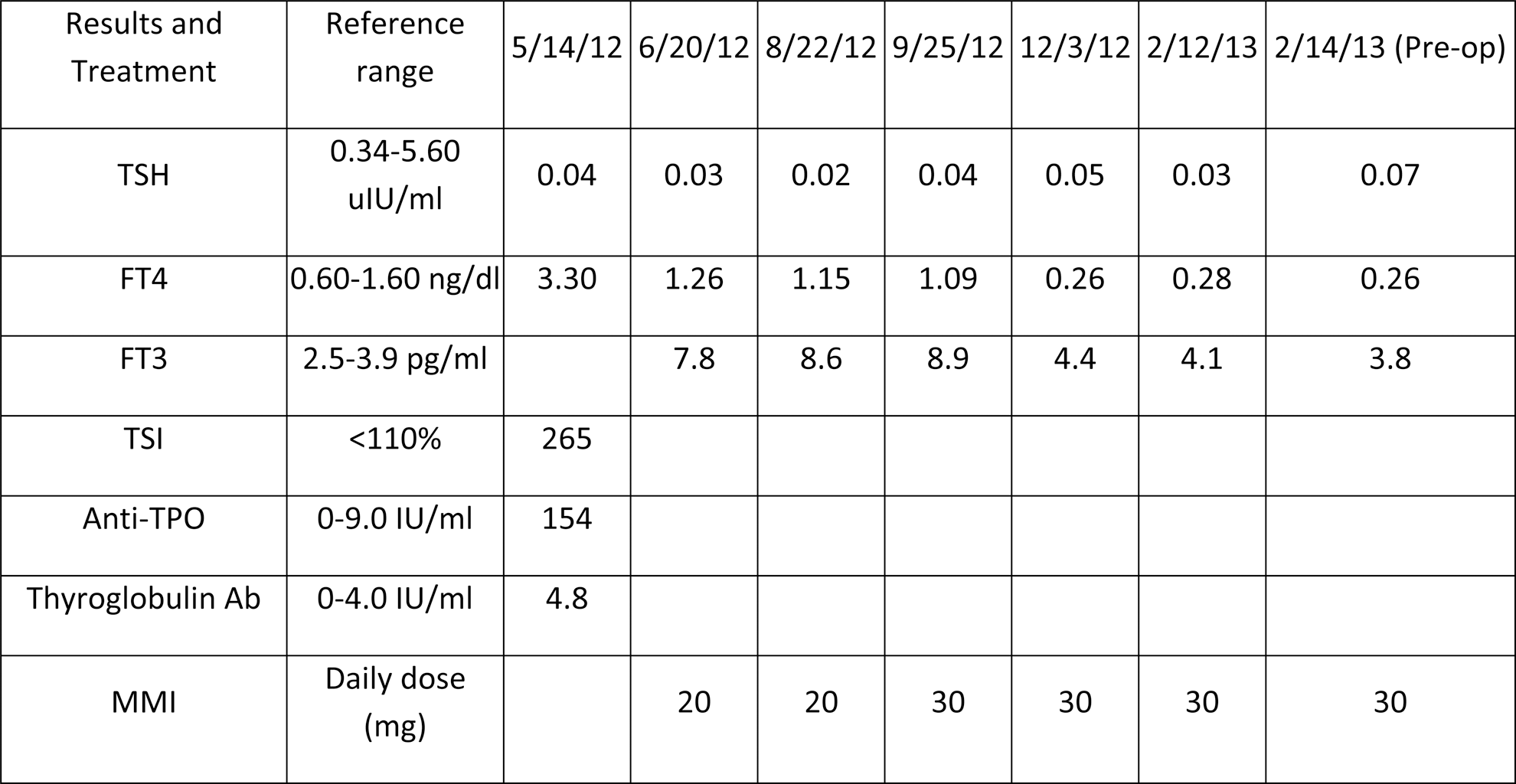
Disorders of Thyroid Function Friday Poster Case Report
It is known that hyperthyroidism can be complicated by atrial fibrillation (AF) and that its treatment may resolve such complication. However the situation becomes more complex when treatment of a preexisting AF is the cause or the aggravation of such condition, particulalrly if using a substance that can affect the thyroid function.
We describe the case of a 69 year-old patient who had suffered from paroxismal AF during the past 4 year, but was in remission following a cardiac ablation and a 2-year treatment with amiodarone. However, 9 months after discontinuing the medication, he started to have repeated attacks of AF. On the 4th episode thyroid test were as follows: FT4: 53 pmol/L (N=11–22), FT3 : 10 pmol/L (N=3.4–6.8), TSH : 0.02 mUi/L (N=0.3–3.5). Anti-TPO and anti-TSH receptor antibodies were negative. 131I uptake was 0.9%. With these results we diagnosed an amiodarone induced thyrotoxicosis type II and started treatment with 40 mg of prednisone per day for a month, tapering gradually every week thereafter. There was a good response with rapid normalization of the thyroid function and remission of AF. However when the prednisone was down to 15 mg/day, both hyperthyroidism and AF recurred. Furthermore the patient did not tolerated the higher doses of prednisone which caused significant lower limb oedema and gain of weight. Therefore we kept him on 20 mg/day. Three months later is 131I uptake was up to 8%. We then treated him with 30 mCi of 131I. Two month later he developed a hypothyroidism and was put on l-thyroxine 0.075 mg/day. The latest tests showed a FT4 of 15.1 and a TSH of 8.96. As for the cardiac arrhythmia, the patient, once euthyroid, had another cardiac ablation and he has been eurhythmic ever since.
Such case illustrates how using amiodarone for the management of AF may complicate its evolution even after it has been discontinued for several months. Awareness and monitoring of thyroid function is mandatory in such situation.
Saturday, October 19, 2013
Thyroid Cancer Saturday Oral Basic 2:20 PM
The MAPK pathway is constitutively active in a majority of papillary and anaplastic thyroid cancers (PTC and ATC). While MAPK-targeted therapies have been encouraging in other tumor types, clinical benefit has been limited in thyroid cancer. Our lab has shown Src is activated in PTC and ATC, and that the growth of a subset of thyroid cancer cells is susceptible to treatment with the Src inhibitors, dasatinib and saracatinib (Schweppe et al 2009; Chan et al 2012). Recently, we identified the MAPK pathway as a potential mediator of resistance in response to Src inhibition in an unbiased genome-wide synthetic lethal screen. We therefore hypothesized that inhibition of Src, using dasatinib or saracatinib, in combination with the MEK1/2 inhibitor, selumetinib, will enhance the anti-tumor effects of either pathway alone.
The effects of Src and MAPK pathway inhibition on thyroid cancer growth and apoptosis were tested in vitro, using the Sulforhodamine B and Caspase 3/7 assays, respectively, and signaling was evaluated by Western blotting. Therapeutic efficacy was tested in vivo using an orthotopic model.
For both the dasatinib + selumetinib and saracatinib + selumetinib combinations, the IC50 values were synergistically reduced 2.6 to 6.4 fold in both BRAF-mutant (BCPAP, SW1736) and RAS-mutant (C643) cell lines. Accordingly, apoptosis was enhanced 3.5 to 8.4 fold for the combinations compared to single agent treatments. As expected, both Src inhibitors effectively inhibited pY416Src and pY861FAK. Interestingly, treatment with dasatinib, but not saracatinib, resulted in a paradoxical increase in ERK phosphorylation, suggesting distinct mechanisms of drug action. We next tested the combinatorial effects of saracatinib (25 mg/kg) and selumetinib (50 mg/kg) in vivo using an orthotopic model. After 4 days of treatment, the combination therapy significantly reduced tumor growth in comparison to selumetinib or saracatinib alone (p=.039). Overall, the combination treatment was similar to selumetinib alone, resulting in a 2.1-fold increase in survival (p=.0076).
Combined Src and MAPK pathway inhibition results in enhanced anti-tumor effects, and may provide a new, more effective therapy for advanced thyroid cancer patients.
Thyroid Cancer Saturday Oral Translational 2:35 PM
VEGFR-targeted kinase inhibitors have emerged as highly promising therapies in radioiodine-refractory metastatic differentiated thyroid cancer. Unfortunately, drug-resistance uniformly develops, limiting therapeutic efficacy.
To assess acquired kinase inhibitor resistance and associated underlying mechanisms, BHP2-7 differentiated (papillary) thyroid cancer cells were subjected to continuous in vitro selection with 18 μM Pazopanib. Acquisition of pazopanib resistance was serially assessed, with the resulting pazopanib-resistant cell line thereafter sub-cloned and characterized.
Stable 2–4 fold in vitro pazopanib resistance developed in response to pazopanib selection associated also with markedly more aggressive in vivo xenograft growth. Selected cells were cross-resistant to sunitinib and to a lesser extent sorafenib, but not to pharmacologic MEK inhibition with GSK1120212. Assessment of effects on ERK phosphorylation in parallel demonstrated the resistant line to have maintained p-ERK relative to the parental cells in response to pazopanib treatment. Genotyping demonstrated acquisition of an activating kRAS codon 13 GGC to GTT (glycine to valine) mutation - consistent with the observed resistance to upstream VEGFR inhibition, yet sensitivity to downstream MEK inhibition.
Selection of thyroid cancer cells with clinically utilized therapeutics can lead to drug resistance and altered in vitro and in vivo xenograft behavior with potential to recapitulate analogous drug resistance observed in patients. This approach has potential to lead to insights into acquired drug resistance that can be subjected to subsequent validation in serially obtained patient samples.
Thyroid Cancer Saturday Oral Basic 2:50 PM
Thyroid cancer stem cells (TCSCs) represent a small percent (1–3%) of a highly invasive and metastatic cell population found in thyroid neoplasms. c-Met and AKT are highly activated and play a key role in stimulating TCSC invasion. CSCs share many genetic traits with cancer cells undergoing epithelial to mesenchymal transition (EMT). The sonic hedgehog (Shh) pathway plays an important role in CSC self-renewal in several tumor types, but its role in stimulating EMT remains controversial. The Shh pathway is highly activated in thyroid neoplasms and plays an important role in tumor cell proliferation. However, whether the Shh pathway and its downstream transcription factor Gli1 can regulate tumor cell invasion through EMT or CSC self-renewal remains unknown.
Two anaplastic (KAT-18 and SW176) and one follicular (WRO82) thyroid tumor cell lines treated with Shh pathway inhibitors or with Shh and Gli1 knockdown or Gli1 overexpression were analyzed for the expression of Snail, E-cadherin, vimentin, and slug by Western blot, for cell motility and invasion in Boyden chambers, and for stem cell self-renewal by thyrosphere formation and the expression of stem cell-related genes (beta-catenin, Sox2, AKT S473, and c-Met tyrosine phosphorylation).
Inhibition of the Shh pathway by HhAntag and GANT61 or by Shh and Gli1 knockdown led to decreased Snail expression but slight increase of E-cadherin expression in all three thyroid tumor cell lines. In contrast, Gli1 overexpression led to increased Snail expression but decreased E-cadherin expression. Both inhibitors had no effect on Slug and vimentin expression. Interestingly, Shh and Gli1 knockdown led to a significant reduction of the chemoinvasive potential of KAT-18 cells. Shh or Gli1 knockdown led to a dramatic decrease of c-Met and AKT phosphorylation and a reduction in the number and size of thyrospheres, whereas Gli1 overexpression led to increased expression of beta-catenin and Sox2 as well as the phosphorylation of AKT and c-Met.
The Shh pathway increases the invasive potential of thyroid tumor cells, largely by inducing CSC self-renewal. Targeting the Shh pathway could be a novel therapeutic strategy to eradicate TCSC-originated tumor metastasis and recurrence.
Thyroid Hormone Action Saturday Oral Basic 3:05 PM
The stem cells governing formation of the intestinal epithelium undergo molecular changes around birth corresponding to the initiation of milk consumption to weaning, a postembryonic developmental time period when thyroid hormone (TH) levels peak. Surprisingly, very few studies have examined mechanisms governing the transition of embryonic into adult intestinal stem cells or the effects of thyroid hormone on stem cell maturation. During Xenopus (X.) laevis metamorphosis, a remodeling of the larval intestinal epithelium occurs which is analogous the postembryonic maturation of the mammalian intestine. Thyroid hormone is critical for the formation of adult epithelium in the intestine for both mammals and amphibians but the tadpole provides an opportunity to examine the molecular mechanisms of TH action independent of maternal influences.
Genome-wide analysis of X. laevis revealed an expressed sequence tag (EST) of an unknown gene was upregulated in the intestinal epithelium during stem cell formation. Rapid amplification of cDNA ends was used to identify the gene and then qPCR, in situ hybridization and immunohistochemical analyses were utilized to analyze its role during intestinal stem cell development.
The EST was determined to be a part of the 3' UTR of the Mxd1 gene that encodes for the Mad protein, a bHLH/Zip transcription factor that competes with cMyc to heterodimerize with Max. Previous studies have shown that Mad/Max dimers inhibit transcription leading to differentiation while cMyc/Max binding induces proliferation. Mad expression was confirmed to be epithelial specific during metamorphosis. In both naturally and TH induced metamorphosing intestines there is strong induction of Mad just prior to cMyc expression and adult stem cell formation. High levels of Mad expression is localized to apoptotic larval cells while cMyc expression is in newly forming adult stem cells.
Our findings suggest TH induced Mad plays a novel role of inducing apoptosis in the maturing intestine, which was further supported by high levels of Mad in other apoptotic tissue. Thus cMyc/Mad balance is likely critical for cell fate determination during TH-dependent postembryonic adult stem cell development.
Disorders of Thyroid Function Saturday Oral Clinical 2:20 PM
Antithyroid drug (ATD) treatment in early pregnancy may be associated with an increased risk of birth defects. A ‘syndrome of malformations’ has been described in relation to Methimazole/Carbimazole (MMI/CMZ), but it has been proposed that also Propylthiouracil (PTU) may be associated with an increased risk of malformations.
We identified all live births in Denmark, 1996–2008, and obtained information on prescriptions of ATD and diagnoses of birth defects from Danish nationwide registers. According to maternal ATD treatment in early pregnancy, children were categorized as exposed to PTU (n=564); MMI/CMZ (n=1,097); MMI/CMZ and PTU (shifted in early pregnancy (n=159)); no ATD (ATD use, but not in pregnancy (n=3,543)); and controls (never ATD or replacement therapy (n=811,730). Multivariate logistic regression was used to estimate adjusted odds ratio (OR) with 95% confidence interval (95% CI) for the risk of birth defects in children exposed vs. controls.
The prevalence of birth defects diagnosed before the age of 2 years was high in children exposed to ATD in early pregnancy (PTU 8.0%, MMI/CMZ 9.1%, MMI/CMZ and PTU 10.1%, no ATD 5.4%, and controls 5.7%, p<0.001). Both MMI/CMZ (adjusted OR 1.66 (95% CI 1.35–2.04)) and PTU (1.41 (1.03–1.92)) were associated with an increased risk of birth defects, and also the group of children born to mothers who had been shifted between MMI/CMZ and PTU in early pregnancy had a high risk (1.82 (1.08–3.07)). Both MMI/CMZ and PTU were associated with malformations of the urinary system and PTU, but not MMI/CMZ, with malformations in the face and neck region (especially sinus, fistula, cyst). Choanal atresia, esophageal atresia, omphalocele, omphalomesenteric duct anomalies and aplasia cutis were common in MMI/CMZ exposed children (these birth defects combined: OR vs. controls 21.8 (13.4–35.4)), but also malformations of the eye and the circulatory system.
Both MMI/CMZ and PTU exposure had teratogenic effects with an excess 2–4 cases of birth defects per 100 live births, but the spectrum of malformations differed. More studies are needed to corroborate results in regard to early pregnancy shift from MMI/CMZ to PTU. New ATD with no teratogenic effects should be developed.
Disorders of Thyroid Function Saturday Oral Clinical 2:35 PM
Thyroid dysfunction is associated with impaired cognitive development in children. Perchlorate decreases thyroidal iodine uptake, thereby potentially reducing thyroid hormone production. Exposure to perchlorate is ubiquitous and it is unclear whether maternal perchlorate exposure negatively affects child neurodevelopment.
We analysed a subset of 487 hypothyroid/hypothyroxinemic women from the CATS Study who had perchlorate levels measured in the first trimester with subsequent IQ assessment of offspring at age 3 years. Logistic regression was undertaken to ascertain if perchlorate levels in the upper third and highest 10% of the population were associated with increased odds of offspring having lower-end IQ (lowest 10%). Analyses were adjusted for recruitment center, maternal age, smoking, maternal thyroid and iodine status, gestational age at urine/blood collection, levothyroxine treatment, gender of offspring and age at psychological testing.
Perchlorate exposure was detectable in all women; median urine perchlorate was 2.58μg/liter (IQR 1.20–5.47); urine iodine levels were low median 72μg/liter IQR (42–156). We observed strong evidence of an association between maternal perchlorate levels in the highest 10% of the population and increased odds of offspring IQ being in the lowest 10% OR=3.14 (95%CI 1.37, 7.12) p=0.006. A greater negative impact was observed with verbal than performance IQ. Analyses were only modestly attenuated after adjusting for maternal thyroid function and iodine status.
We found some evidence of association between high-end maternal perchlorate levels during pregnancy and subsequent adverse cognitive development in offspring in a cohort of women with mild iodine deficiency, and hypothyroidism/hypothyroxinemia during pregnancy. Associations persisted after adjustment for maternal iodine and thyroid status, raising the possibility that there may be a direct action of perchlorate on the fetal thyroid. These results require replication in larger studies in the euthyroid pregnant population.
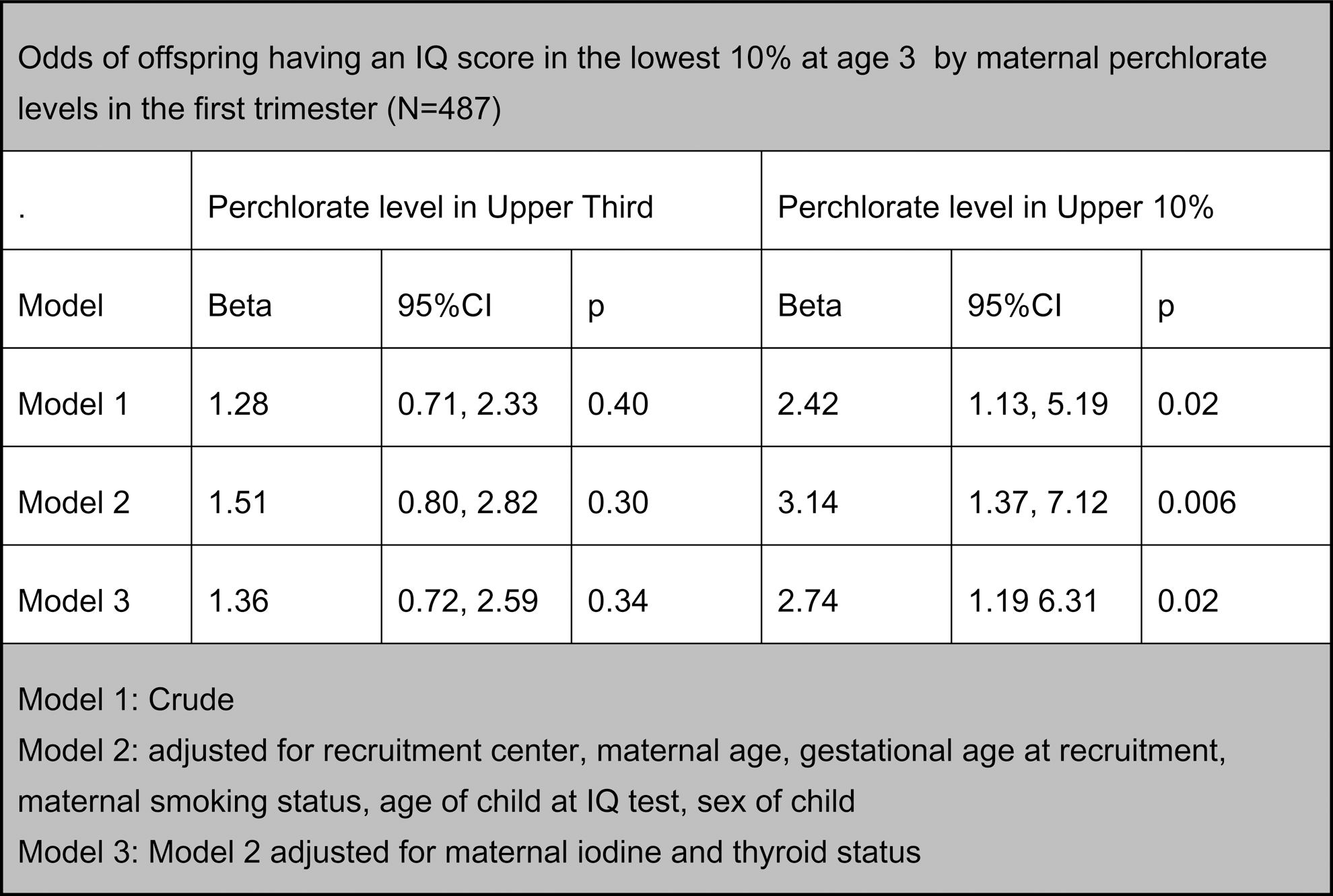
Disorders of Thyroid Function Saturday Oral Clinical 2:50 PM
Surprisingly few studies have examined weight change of hypothyroid patients after levothyroxine (LT4) treatment. We aimed to investigate the relationship between successful treatment of overt hypothyroidism and subsequent weight change.
Using electronic medical records from Boston Medical Center, we performed a retrospective cohort study from 1/1/2003-2/1/2011. We identified patients with newly-diagnosed primary hypothyroidism with initial TSH≥10 mIU/L. We excluded those with post-surgical hypothyroidism, thyroid cancer, history of radioactive iodine or head/neck radiation, congestive heart failure, anorexia nervosa, end-stage renal disease, cirrhosis, pregnancy, or use of prescription weight loss medication. TSH and weight at diagnosis as well as at up to 24 months after initiation of LT4 were collected. Demographic data including age, gender, race, education level, and insurance provider, were ascertained. Weight change was assessed at the first time point of TSH<5 mIU/L after LT4 initiation. Associations between individual predictors and weight change were analyzed by Spearman correlations or Wilcoxon Rank Sum test. Multivariable regression models examined weight change with initial TSH, initial weight, and demographic characteristics as predictors.
A total of 101 patients (mean age 48±15 yr, 71% women) were included. Initial median (range) TSH was 48 mIU/L (10.1–710.5) and weight was 79.6 kg (41.5–167.5). Post-treatment median (range) TSH was 2.3 mIU/L (0.04–5) and weight change at a mean 32±26 weeks was −0.1 kg (−20.6–7.7). 52% of patients lost weight, with mean weight loss 3.8±4.4 kg. In univariate and multivariate analyses, race, education, insurance type, age, initial TSH, time to normalization of TSH, and initial weight were not associated with weight change or weight loss.
LT4 treatment of patients with overt primary hypothyroidism resulted in modest weight loss in only 52% of patients. There were no associations between weight change and gender, race, education level, insurance provider, initial TSH or weight, age, or time to normalization of TSH. Contrary to popular public belief, treatment of overt primary hypothyroidism was not associated with clinically significant weight loss in most patients.
Thyroid Hormone Metabolism & Regulation Saturday Oral Clinical 3:05 PM
Prior thyroid chronobiology research identified a circadian variation in serum TSH and T3, and a circannual rhythm in TSH, T3, and T4. Small sample size and short duration of observation limit the relevance of these findings. By analyzing a data set of TSH, FT4, and FT3 measurements performed in a controlled and calibrated manner over 29 consecutive months, we conducted a more robust analysis of temporal variation in thyroid hormone levels.
The Intermountain Healthcare IRB approved this retrospective study of outpatients (25% males, ages 0–103 years; 75% females, ages 0–105 years). Serum TSH, FT4, and FT3 were measured by Abbott Architect immunoassay with external controls performed daily, Circadian TSH and FT4 values consisted of 205,538 observations; circadian FT3 data were obtained from 58,993 subjects. Monthly TSH and FT4 values were obtained in 164,094 subjects, and monthly FT3 data on 47,667 subjects.
Circadian Rhythms. TSH peaked at 7.5 mIU/L between 2–3 AM and reached a nadir of 3.2 at 10 AM. A 42% rise in FT3 occurred at 3 AM. There was minimal change in TSH between 6 AM and 7 PM. FT4 values were stable over 24 hours. Circannual Rhythms. TSH varied from a minimum of 3.01 in May, 2011 to a maximum of 4.13 in Dec. 2010 (amplitude=37%). FT4 was lowest (1.11 ng/dl) in Dec. 2010 and highest (1.19) in Nov. 2012 (amplitude=7%). FT3 was lowest in Nov. 2010 (2.78 pg/ml) and highest (3.32) in March, 2012 (amplitude=19%). The pattern of TSH rising in November and December, absence of circannual variation in FT3, and the stability of FT4 values were present over a period of 29 months.
TSH rose sharply between 2–3 AM and remained relatively constant between 6 AM and 7 PM. FT3 peaked at 3 AM and was otherwise stable throughout the day. FT4 had no circadian variation. TSH displayed a circannual rhythm with highest values in November-December. FT4 and FT3 did not show an annual periodicity. These data suggest that outpatient TSH levels are stable between 6 AM and 7 PM and TSH reference values vary by month. Further studies need to confirm our finding that the reference range for TSH should take into account month, but not time of day.
Autoimmunity Saturday Poster Basic
Convincing evidences were shown the association of thyroid stimulating hormone receptor (TSHR) with Graves' disease (GD) in the Chinese Han population. The aim of this study was to identify the causal variants for GD in TSHR region by a refining association study.
In total, 1,536 GD patients and 1,516 sex-matched controls were recruited in the first stage, and additional 3,832 GD patients and 3,426 sex-matched controls were recruited in replication stage. Genotyping was performed by Illumina Human 660-Quad BeadChips or TaqMan® SNP Genotyping Assays in Fludigm EP1 platform.
Combing the results of regression analysis for 74 genotyped SNPs and 922 imputed SNPs in the first stage cohort, rs179243 and rs3783949 were the probable susceptibility SNPs associated with GD in TSHR region. Eleven SNPs including rs179243 and rs3783949 in this region were selected for further refining association in the replication study. Finally, rs12101261 and rs179243 as independent GD susceptibility variants were confirmed in the replication and combined population. Meanwhile, we also found that the rate of persistent thyroid stimulating hormone receptor autoantibodies (TRAb) positivity is significantly higher in the GD patients with the susceptible genotypes of rs12101261 or rs179243 than that in the GD patients carrying the protective genotypes after the GD patients treated over one year.
These findings indicated that rs12101261 and rs179243 were the possible causal SNPs to GD susceptibility in TSHR region and could serve as a genetic marker to predict the outcome of TRAb in GD patients.
Autoimmunity Saturday Poster Clinical
The role of thyroid stimulating autoantibodies (TSAb) in the medical therapy of Graves' disease (GD) is still a matter of debate. We hypothesized that serum TSAb levels are clinically useful and predictive in GD.
Hundred consecutive untreated hyperthyroid GD patients received Methimazole (MMI, 2.5–30 mg/day) for 24 weeks. Response vs. non-response to treatment was defined as biochemical euthyroidism at weeks 24 and 36 vs. persistent hyperthyroidism at week 24 and/or relapse at week 36. Serum TSAb levels were measured at baseline, at 4, 8, 12, 24 and 36 weeks after starting MMI with a bioassay that uses a chimeric TSH-R and a CRE-dependent luciferase. TSAb results are expressed as percentage of specimen-to-reference ratio (SRR%). Values ≥140% are considered positive.
Forty two of 98 patients who completed the trial (43%, median age 42 years, 13 smokers, 31%) responded to MMI of whom 19 (45%) had Graves' orbitopathy (GO). In contrast, 56 (57%) were non-responders (43.5 years, 28 smokers, 50% and 36, 64% with GO). At week 0, responders demonstrated marked differences in diluted TSAb titers compared with non-responders (P<0.001). Also, 12 weeks after starting MMI, differences of TSAb levels and MMI dose (both P<0.001) were noted between responders vs. non-responders. At week 24 and compared with baseline, serum TSAb levels decreased markedly in responders (median SRR% 420 vs. 271, Δ−60%, P<0.001) but increased in non-responders (422 vs. 465, Δ+10%). In contrast, serum levels of TSH-R binding inhibiting immunoglobulins (TBII) decreased in non-responders at week 24 (14.9 vs. 9.27 IU/L, Δ−40%, P=0.002). TSAb and TBII levels positively correlated (r=0.66, P<0.001) however TSAB but not TBII values differentiated between GD and GD/GO (P<0.001). Median thyroid volume was 15.85 ml (range 3–35) and 23.5 ml (5–64) in responders and non-responders, respectively (P=0.002). Neither gender nor age had a significant impact on the outcome.
Serum TSAb levels mirror the severity of GD. Their increase during medical treatment is a marker for on-going disease activity. TSAb dilution analysis was additionally predictive. Thus, TSAb levels are a prognostic parameter for GD and reliably predict response to medical therapy.
Autoimmunity Saturday Poster Clinical
Vitamin D role has extended beyond the action on the skeleton, on many more objectives. Among these, an effective action has been demonstrated in immunology field both promoting a positive response of innate immunity against infections and through an immunomodulatory mechanism against autoimmune diseases. At this purpose we have tested the effect of vitamin D supplementation on the level of thyroid antibodies (TAbs): AbTg ( anti-thyroglobulin) and AbTPO (anti-peroxidase) antibodies.
We have performed a randomized double blind study with high dosage of cholecalciferol, 4,500,000 UI, in a group of subjects affected by autoimmune thyroiditis in order to observe the variation of thyroid antibodies (Tg and TPO antibodies) over a period of 9 months following the vitamin D administration. We have considered 28 subjects, with age ranging 24–45 yrs, 20 female and 8 male. All presented high titer of TAbs, typical thyroid hypoechoic echostructure and a normal TSH (normal range 0.3–5 mUI/ml) (Autoimmune thyroiditis type 1 B, eucrine and no goiter, according to Terry Davies classification). Subjects were divided in two groups (16 vitamin D group and 12 placebo). The first one have received a single oral dose of 450.000 UI of cholecalciferol, the second one an oil formulation as placebo, both on bread piece, twice a year (2012) in January and May. They underwent blood sample withdrawn on January, before vitamin D or placebo supplementation and then one, two, three, six and nine months after. We have assayed by immunofluorimetric method both AbTPO and AbTg; by chemiluminescent method (Liaison) 250HD.
The results are shown in table and figure below demonstrating a continuous and significative reduction over time of TAbs after vitamin D, while no differences were shown after placebo administration
The efficacy of vitamin D in autoimmune diseases has been already illustrated in other autoimmune based conditions as diabetes mellitus type I and multiple sclerosis but not yet in the most frequent autoimmune disease like AT. The data we have obtained in this double blind work are very promising; in fact a significant declining of TAbs after vitamin D administration was observed compared to a control group.
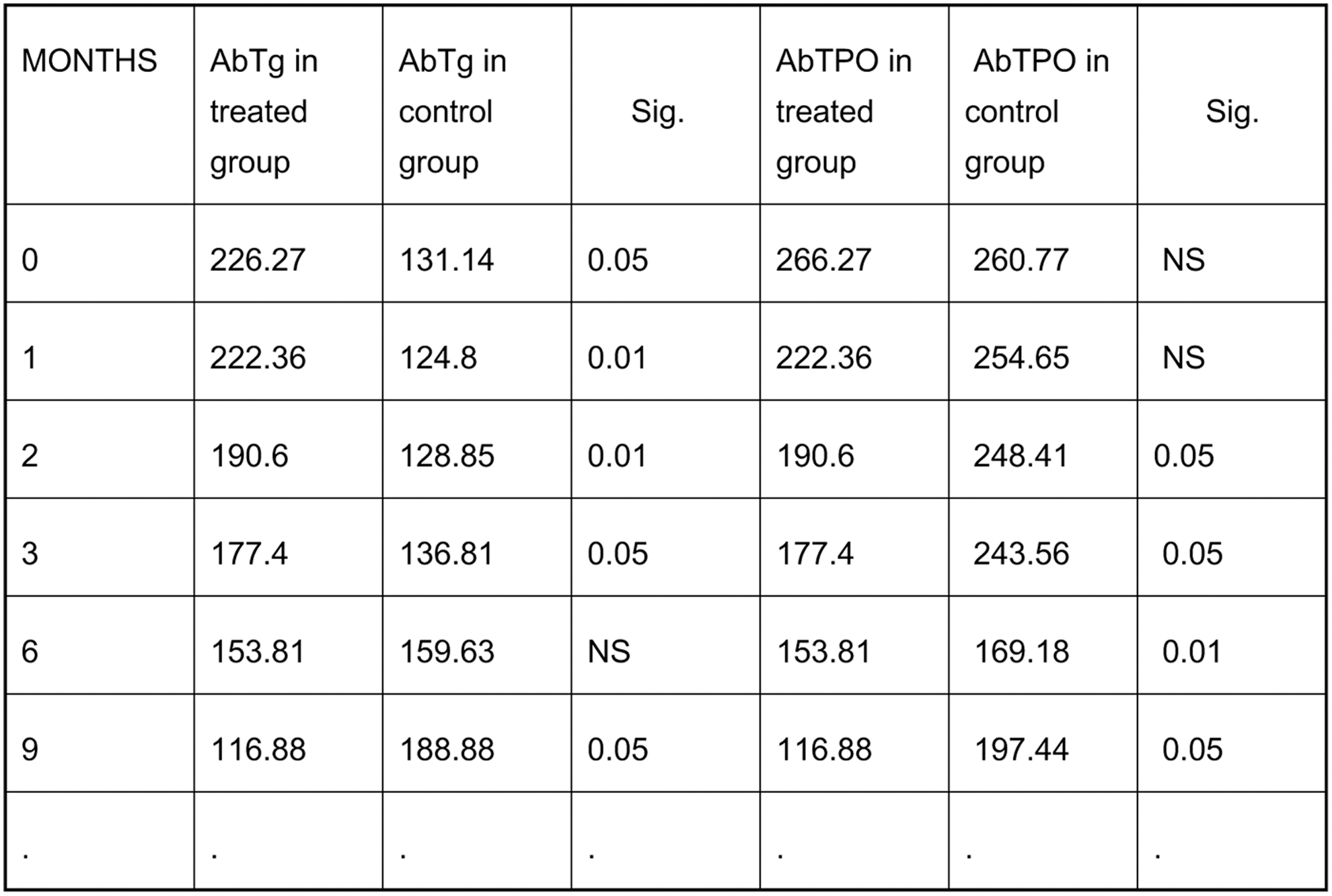

Disorders of Thyroid Function Saturday Poster Clinical
The diagnosis of subclinical hypothyroidism is defined as the presence of an elevated thyroid stimulating hormone (TSH) with a normal free thyroxine (FT4) level. The commonly used direct analogue immunoassays for the measurement of FT4 have been shown to have poor performance at the upper and lower limits of the FT4 reference interval. The purpose of this pilot study was to investigate the percentage of individuals classified as having subclinical hypothyroidism with a standard immunoassay, that actually have low free thyroid hormone levels by mass spectrometry measurements.
Outpatient samples for patients less than sixty years old with elevated TSH values and normal FT4 concentrations as per standard immunoassay methods were collected. Patients' samples were excluded if they had known thyroid disease, were receiving thyroid hormone replacement therapy or other medications that are known to affect FT4 values or cause elevation in TSH values. FT4 and free triiodothyronine (FT3) analyses were performed on these samples using liquid chromatography-tandem mass spectrometry (LC-MS/MS).
Seventy five percent (n=21) of patients had LC-MS/MS FT4 or FT3 or both FT4 and FT3 values below mass spectrometry reference limits. Sixty-one percent (n=17) of patients that would be classified as subclinical hypothyroidism as per immunoassay FT4 measurements had LC-MS/MS FT4 values that were below the mass spectrometry(MS) reference interval. There was poor correlation between immunoassay and LC-MS/MS values for both free thyroid hormones. Pearsons correlation coefficient between IA FT4 and MS FT4 was 0.58 (95% CI 0.27–0.78) and between IA and MS for FT3 was 0.29 (95% CI 0.06–0.52).
Our findings indicate that the direct analogue immunoassay method for FT4 measurement results in a significant proportion of patients being misclassified as having subclinical hypothyroidism.
Disorders of Thyroid Function Saturday Poster Clinical
Persistent or recurrent hyperthyroidism after treatment with radioactive iodine (RAI) is common, and many patients require either additional doses or surgery before they are cured. The purpose of this study was to identify patterns and predictors of failure of RAI in patients with hyperthyroidism.
We conducted a retrospective review of patients treated with RAI from 2007–2010. Failure of RAI was defined as receipt of additional dose(s) and/or total thyroidectomy. Kaplan-Meier disease-free survival estimates were plotted to analyze the timing of failures. Using a Cox proportional hazards model, we conducted univariate analysis to identify factors associated with failure of RAI. A final multivariate model was then constructed with significant (p<0.05) variables from the univariate analysis.
Of the 325 patients analyzed, 74 patients (22.8%) failed initial RAI treatment. 53 (71.6%) received additional RAI, 13 (17.6%) received additional RAI followed by surgery, and the remaining 8 (10.8%) were cured after thyroidectomy. Failures occurred in 25.8, 14.3, and 9.8% of patients with Graves', toxic multinodular goiter, and solitary toxic nodule, respectively. Among the variables significant on univariate analysis were higher initial T3 (HR 1.07, 95% CI 1.0–1.11, p<0.01) and free T4 levels (HR 1.14, 95% CI 1.07–1.21, p<0.01) and lower RAI doses (HR 0.90, 95% CI 0.85–0.95, p<0.01). The percentage of patients who failed decreased in a step-wise fashion as RAI dose increased (Figure 1A). Similarly, the incidence of failure increased as the presenting T3 level increased (Figure 1B). Sensitivity analysis revealed that RAI doses ≥15 mCi were protective against failure while initial T3 and free T4 levels of at least 4.5 pg/mL and 2.3 ng/dL, respectively, were associated with failure. In the final multivariate analysis, higher T4 (HR 1.13, 95% CI 1.02–1.26, p=0.02) and methimazole treatment (HR 2.55, 95% CI 1.22–5.33, p=0.01) were associated with failure.
Laboratory values at presentation can predict which patients with hyperthyroidism are at risk for failing RAI treatment. Higher doses of RAI may prevent the need for repeat RAI in selected patients.
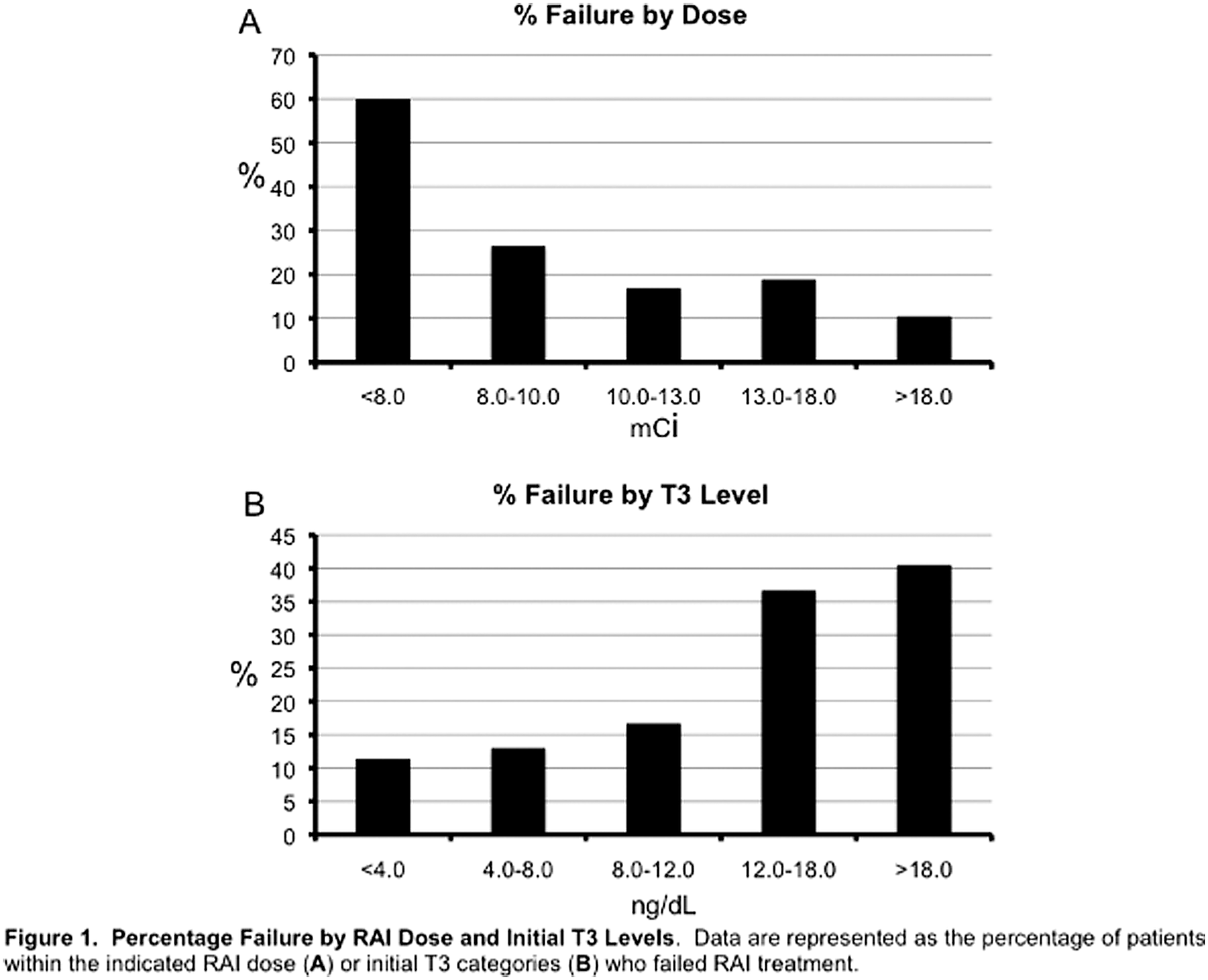
Disorders of Thyroid Function Saturday Poster Clinical
Several studies have suggested an association between subclinical hypothyroidism (SCH) and increased cardiovascular risk. The present study evaluated the presence of subclinical coronary artery disease (CAD) in asymptomatic patients with SCH by measuring the coronary artery calcium score (CACS).
Subjects (103 SCH and 119 euthyroid [EU]), aged 35 to 65 years, with no previous history of CAD were enrolled in a cross-sectional analysis. Criteria for SCH were confirmed normal serum free thyroxine levels with high serum thyrotropin levels (>4.0–10.0 mU/L). Lipid profile, Framingham Risk Score (FRS), and CACS were obtained from all subjects.
Age, gender, body mass index, and frequencies of diabetes, systemic arterial hypertension, hypercholesterolemia, and smoking were similar in both groups. The overall median CACS did not differ between the groups. However, in the subgroup of subjects with intermediate/high FRS, the mean CACS was higher in the SCH compared to the EU group (EU vs. SCH: 38.5±80 vs. 254±554.2; p=0.045). SCH patients with FRS ≥10% had a higher frequency of CACS>100 than EU subjects with similar FRS (EU vs. SCH: 5.9% vs. 43.8%, p=0.01). Serum thyrotropin was positively correlated with CACS in subjects with intermediate/high FRS (rs=0.301, p=0.045).
SCH may be an additional risk factor for CAD in subjects with intermediate/high FRS.
Disorders of Thyroid Function Saturday Poster Clinical
Thyroidectomy is considered a safe procedure, especially in the elective setting. However, there are few large studies exploring the outcome of elective thyroidectomy for benign disease. We undertook the present study to determine factors leading to poor outcomes after elective thyroidectomy for benign disease.
All patients undergoing a partial or complete thyroidectomy (ICD-9 CM 06.2–06.5) in the 2010 Nationwide Inpatient Sample database were selected. Patients were excluded if they were admitted emergently or if they had a diagnosis of thyroid or parathyroid malignancy. Sampled patients were divided into cohorts based on occurrence of total complications. Factors that were significantly different between the cohorts on univariate analysis were used to make multiple logistic regression models.
An estimated 37,129 patients underwent elective thyroidectomy for benign disease in 2010. The overall complication rate was 10.9%, and included bleeding (2.2%), wound complications (1.9%), vocal cord paralysis (1.2%), and hypocalcemia (5.0%). On univariate analysis, history of cardiac disease, diabetes, chronic kidney disease, obesity, race, and primary insurance were associated with increased risk of complications. History of pulmonary disease hospital size, teaching status, and location (rural vs. urban) were not associated with complications. On multivariate analysis, significant predictors of total complications included cardiac disease (OR 1.79, p=0.001) and renal disease (OR 3.07, p<0.001). Renal disease was also associated with increased risk of bleeding (OR 2.5, p=0.002), wound complications (OR 2.17, p=0.02), and hypocalcemia (OR 2.25, p=0.005). Diabetes was associated with risk of vocal cord paralysis (OR 1.68, p=0.041).
Overall, elective thyroidectomy is a safe procedure, with low rates of complications. However, the presence of specific comorbidities is associated with increased risk for certain complications after thyroidectomy. The endocrine surgeon should be aware of these risks when determining which patients are the best candidates for elective thyroidectomy in the setting of benign thyroid disease.
Disorders of Thyroid Function Saturday Poster Clinical
Extent of surgery in Graves' disease remains controversial. The aim of this study is to compare long term outcome and complication between total thyroidectomy (TT) and subtotal thyroidectomy (ST).
Three hundred fifty patients underwent thyroid surgery for Graves' disease in Asan Medical Center from December 1995 to December 2010. There were 80 male and 270 female patients with mean age of 32.8±11.9 years (range, 14∼69). Among them, 254 (72.5%) patients underwent ST and 96 (27.5%) patients underwent TT. Median follow-up period was 61 months (range 5∼201). We investigated the change of postoperative thyroid function after subtotal thyroidectomy and the post-operative complications. In patients who underwent subtotal thyroidectomy, we maintained follow-up for 2 years at least after surgery and checked thyroid function test (TFT).
Transient hypoparathyroidism occurred in 24 patients (24/254, 9.2%) after ST and patients (3/96, 4.5%) after TT (p=0.54). Permanent hypoparathyroidism occurred in 1 patients (1/259, 0.4%) after ST and in no patient after TT. Recurrent laryngeal nerve injury was seen in one patient (1/259, 0.4%) who had ST and in no patient who had TT. When we evaluated serial TFT of the patients who underwent ST (n=209), 13 patients (13/209, 6.2%) showed euthyroid status in early period after surgery. In late period (2 years after surgery), 18 patients (18/209, 8.6%) achieved euthyroid status eventually, while 180 patients (180/209, 86.1%) showed hypothyroidism. Most of the patients with hypothyroidism (164/180, 91.1%) needed the supplement of thyroid hormone. Persistent or recurrent hyperthyroidism occurred in 11 patients (5.3%). After recurrence, 6 patients received radioactive iodine ablation and 5 patients received antithyroid medication. There are no recurrences in patients who underwent TT.
In the present study, Patients who underwent TT showed excellent disease remission, while majority of patients who underwent ST did not maintain normal thyroid function. TT for Graves' disease can be performed safely without increased complication when compared with ST. TT for Graves' disease is a feasible surgical option especially for patients who is retractable to antithyroid medication.
Disorders of Thyroid Function Saturday Poster Clinical
The incidence and types of adverse events after initial antithyroid drug (ATD) therapy during pregnancy have never been reported, nor has whether the incidence of adverse events is as same as among non-pregnant subjects ever been investigated.
We investigated the incidence of adverse events particularly of hepatotoxicity and cutaneous reactions, after initial ATD administration to previously untreated Graves' disease (GD) patients during pregnancy. We reviewed the cases of 90 untreated pregnant women who came to our hospital for the first time and were newly diagnosed with GD during the period between January 1, 1999 and December 31, 2011.
Thiamazole (MMI) was used to treat 40 patients and 51 patients were treated with propylthiouracil (PTU). Adverse events occurred in 21 patients (5/40; 12.5%) treated with MMI, and they consisted of cutaneous reactions in 5 patients. Adverse events occurred in five patients (5/51; .9.8%) treated with PTU, and they consisted of hepatotoxicity in two patients and cutaneous reactions in three patients. No patients experienced serious side effects, such as agranulocytosis or ANCA-related vasculitis. The incidences of adverse events in the pregnant patients in this study were lower than the incidences in non-pregnant GD patients reported in the previous study conducted at our hospital.
The incidences of adverse events after initial ATD treatment during pregnancy were lower than in non-pregnant GD patients. All of the types of adverse events were mild.
Disorders of Thyroid Function Saturday Poster Clinical
Myxedema coma is the extreme presentation of hypothyroidism. Mortality can be as high as 60%. There are very few reports of myxedema coma in developing countries 4 cases of myxedema coma were found in the database of consults of the Endocrinology Service. Important variables were extracted.
Case 1. 55 yo male, with personal history of dyslipidemia, was found with abdominal pain and seizures. The initial GCS was 8/15. The patient had bradycardia (43 bpm) and hyponatremia. TSH was 346 mU/L and FT4 was <0.4 ng/dl. The patient was treated with oral levothyroxine and concomitant infections were treated properly in the ICU. The patient was discharged alive at day 30th.
Case 2. A 48 yo female patient presents hypoglycemia, hypotension and very low sodium (102). A normal TSH was found with low FT4. The patient was also diagnosed with Sheehan syndrome. The patient was placed on treatment with IV hydrocortisone and was discharged alive with levothyroxine and prednisone at day 9th.
Case 3. 71 yo male patient with bipolar disorder presents unconsciousness and was also found with bradycardia, hypotension and TSH of 394 with FT4 of 0.68. Patient was prescribed levothyroxine and discharged alive after ICU support.
Case 4. 61 yo male patient with history of HTN and COPD. Patient was found with Glasgow 9/15, bradycardia, hypotension. TSH was 154 and FT4 was 0.4 Patient received treatment with oral levothyroxine, ICU support, and was treated for a CAP and MSSA bacteremia. The patient was discharged alive at day 88 of hospitalization.
The experience of these 4 cases was presented at a single institution. All patients were discharged alive. Intensive care support is essential in the management of these types of patients and probably is one of the main causes associated with a successful outcome in myxedema coma.
Disorders of Thyroid Function Saturday Poster Clinical
Acquired immune deficiency syndrome (AIDS) is an immune deficiency disease. The etiology of hyperthyroidism can also be immune-related, including thyroid, neoplastic, autoimmune, inflammatory hyperthyroidism and so on. Hyperthyroidism is a rare complication of highly active antimicrobial therapy (HAART) for AIDS. This is the first reported case of hyperthyroidism directly caused by AIDS.
A 29-year-old man who complained of dyspnea and asthenia for 1 month, recurrent fever for more than 20 days, and breathlessness for 1 week was admitted to our hospital. The thyroid function test showed the level of free thyroxine (FT4) was higher than normal and that the level of thyroid-stimulating hormone (TSH) was below normal. He was diagnosed with hyperthyroidism. Additional investigations revealed a low serum albumin level and chest infection, along with diffuse lung fibrosis. Within 1 month, he experienced significant weight loss, no hand tremors, intolerance of heat, and perspiration proneness. We recommended an HIV examination; subsequently, AIDS was diagnosed based on the laboratory parameters.
The patient's hyperthyroidism characteristics were as follows: his status was not typically hypermetabolic, his thyroid hormone level was mildly elevated, the associated antibodies were negative, and his thyroid function was normalized after a short-term treatment with drugs. Additionally, there was a drop in the CD4 cells and an increase in CD8 cells. We cannot explain the mechanism linking hyperthyroidism and AIDS and the elevation of CD8+ cells or the production of thyrotropin receptor antibody (TRAb) stimulated by Th cells. We hypothesize hyperthyroidism in our case may be the consequence of a kind of thyroiditis, which is directly caused by the immune-related disorders of AIDS.
Although hyperthyroidism is rare in patients with AIDS, clinicians should be aware of this potential interaction and should carefully monitor thyroid function in HIV-positive patients.

Iodine Uptake & Metabolism Saturday Poster Basic
The Wolff-Chaikoff effect and its escape phenomenon consist in an acute homeostatic adaptation of the thyroid gland to iodine excess. The molecular mechanisms involved in these effects are only partially elucidated. It is well known that iodide downregulates its own uptake through inhibition of NIS, which contributes to a subsequent decrease of the iodide intracellular concentration. Pendrin has been suggested to be one of the apical transporters of iodide. However, little attention has been given to a possible regulation of pendrin by iodide. We have demonstrated that an excess of iodide rapidly upregulates pendrin mRNA expression in thyroid, through a transcriptional mechanism. We aimed now to investigate if iodide excess could regulate the promoter of the pendrin gene. Moreover, we have investigated the action of different doses of iodide on pendrin protein expression.
Two human fragments upstream of the ATG of the pendrin gene (−4.1 kb and −2.0 kb) were subcloned into the pGL3-basic vector, upstream to a luciferase reporter gene. Rat PCCl3 thyroid cells were transfected, and then treated or not with 10–3 M NaI for 1 hour. For protein analysis, PCCl3 cells were treated with 10–3, 10–5, 10–7 and 10–9 M NaI for 30 min, 1, 24 and 48 hours. Total protein was extracted and the abundance of pendrin was evaluated by Western Blot.
Iodide treatment had no effect on the studied regions of the SLC26A4/PDS promoter, suggesting that the previously demonstrated increased mRNA may be regulated by an effect outside the promoter. Protein expression was significantly increased when cells were exposed to 10–3 M of NaI for 24 hours. The lower doses did not have an evident effect on pendrin protein expression suggesting that the observed regulation of pendrin by iodide is dose-dependent.
The present data demonstrate that only high doses of iodide are capable to upregulating pendrin protein expression. This is consistent with the fact that the Wolff-Chaikoff effect requires a high intra-cellular concentration of iodide. This upregulation may be associated with increased iodide efflux and could contribute to the mechanisms protecting thyroid cells against excessive intracellular iodide concentrations.
Iodine Uptake & Metabolism Saturday Poster Clinical
Obesity has been associated with certain nutritional deficiencies. It is unclear if excess weight affects urine iodine (UI) levels, and if mildly elevated TSH noted in some obese patients is related to UI.
We examined NHANES data (2007–10) for potential effects of BMI, fasting & dairy intake on UI levels, and whether any of these factors affects thyroid functions. As noted in NHANES publications, UI was measured via mass spectrometry and thyroid functions via immunoenzymatic assays. We used pairwise comparisons to compare median UI among the 3 weight groups and adjusted chi-square for proportions.
The age groups analyzed were 6–11, 12–19, and 20–29 yr old (yo), with 1440, 1485, and 1101 subjects, and fasting samples in 20.7%, 50.7%, and 47.9%, in the respective groups. No difference in dairy consumption among normal (NL), overweight (OW) or obese (OB) within the 6–11 and 12–19 yo, though 81.3% vs 60.3% in the respective ages listed dairy consumption as “very often” (p<0.0001). Fasting vs non-fasting UI (μg/L) in NL were lower (p≤0.001) in 6–11 yo (167 vs 259) and in 12–19 yo (118 vs 188); fasting levels were also lower in the OW (p≤0.02), but not in the OB group. In adults, only the OB had lower fasting levels, 132 vs 167 (p=0.04). UI in both 12–19 and 20–29 yo were higher in OB vs NL subjects (p<0.01) and iodine deficiency rates were lower in OB vs NL (Table). Logistic regression model for risk of UI<100 in 6–19 yo reveals higher risk (2.9 fold) in non-Hispanic Blacks vs Hispanic and White, and increasing age (p<0.0001); higher risk (1.9 fold) in those consuming dairy rarely vs “very often”, and NL vs OB. Both weight group and UI did not associate with TSH, T4 or T3. UI or weight status in 12–29 yo did not affect the likelihood of having a TSH>4.5 uIU/mL.
Except in the obese, iodine deficiency is less common in 6–11 vs 12–19 year olds, in part due to higher dairy intake in the younger group. In 12–29 yo, iodine deficiency is higher in the normal weight vs obese group. The physiologic significance of lower fasting UI, more noticeable in children and adolescents of normal weight, is unclear. Non-fasting spot urine should be collected when using the WHO criteria for the diagnosis of iodine deficiency.
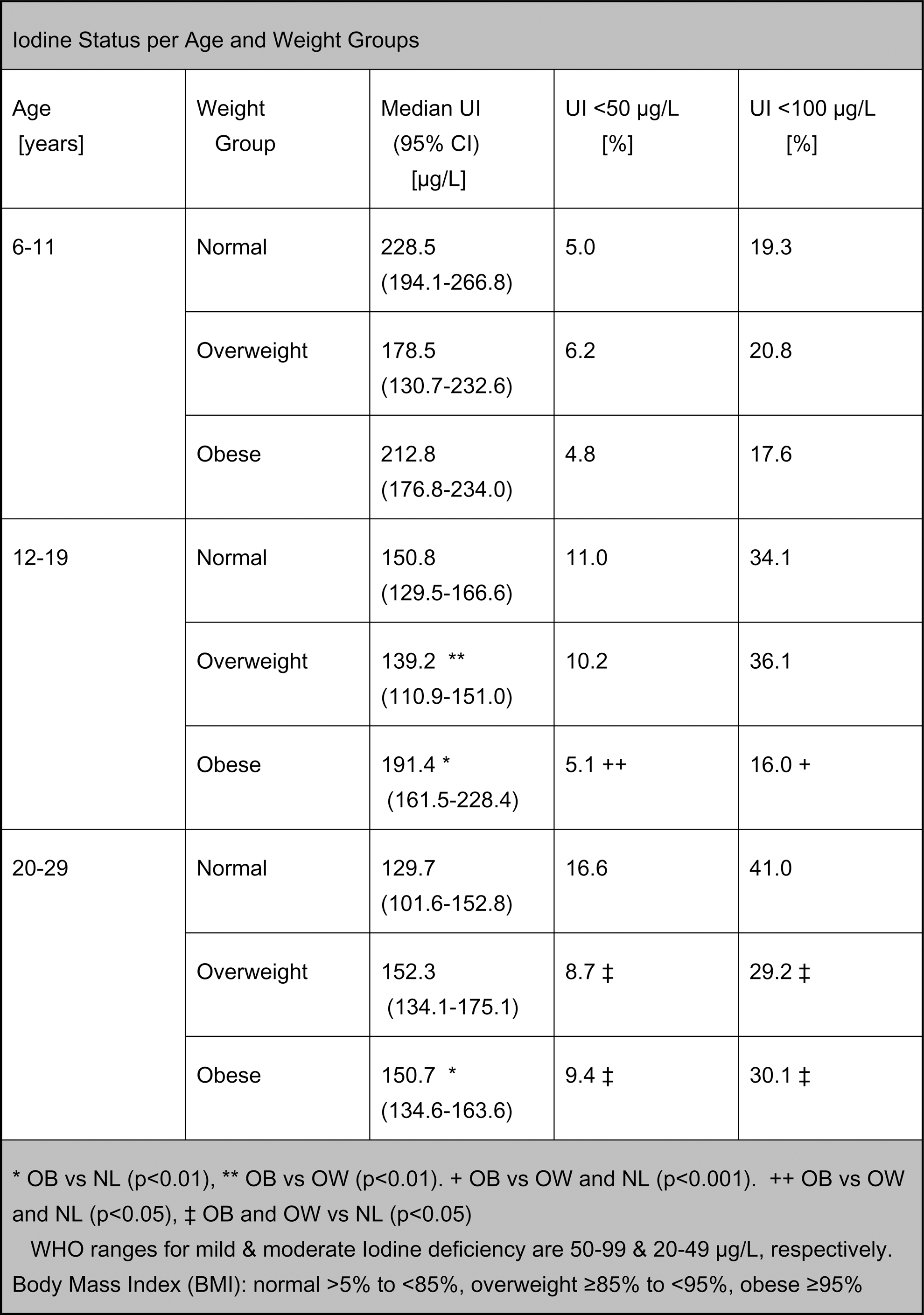
Withdrawn
Thyroid Cancer Saturday Poster Basic
New therapeutic strategies are needed for patients with advanced thyroid cancer who do not respond to current therapies. The Src family kinases (SFKs) are multifunctional nonreceptor tyrosine kinases that are key regulators of growth, survival, migration, and invasion, yet how these pro-tumorigenic processes are regulated in thyroid cancer is currently not clear. Our lab was the first to show that the Src substrate, Focal Adhesion Kinase (FAK), is phosphorylated on a subset of papillary thyroid cancer patient tumor samples, and we further showed that the growth and invasion of thyroid cancer cells is sensitive to Src inhibition (Schweppe et al 2009; Chan et al 2012).
Here, we show that Src is a key regulator of global phospho-tyrosine signaling. We therefore examined potential upstream receptor tyrosine kinase targets, and focused on the role of c-Met, which plays important role in thyroid cancer, and has been shown to be upstream and downstream of Src in other cancers.
For these studies, we show that c-Met is phosphorylated at tyrosine residues 1234/1235 in the absence of supplement ligand, HGF, in the majority thyroid cancer cell lines tested (C643, TPC1, SW1736, and BCPAP, not K1). Src inhibition with saracatinib reduced phospho-Met levels in a dose-dependent manner in the four cancer cell lines, indicating that c-Met is a downstream target of Src. Treatment with HGF further increased phosphorylation of c-Met, and overcame the inhibitory effects of saracatinib on phospho-Met. Interestingly, HGF-dependent activation of c-Met did not activate Src or FAK, indicating that Src and FAK are not downstream of c-Met. Furthermore, treatment with a selective c-Met kinase inhibitor, PHA665752, inhibited both basal and HGF-stimulated phosphorylation of c-Met, but did not affect phosphorylation of Src or FAK. Finally, inhibition of c-Met with PHA665752 showed limited effects on thyroid cancer growth, while shRNA knockdown of c-Met blocked anchorage-independent growth.
Taken together, our data indicate that c-Met is likely an effector protein of Src through an upstream signaling mechanism, and that c-Met, along with Src, could be a relevant therapeutic option for thyroid cancer.
Thyroid Cancer Saturday Poster Basic
The most prevalent genetic alterations in papillary thyroid carcinoma (PTC) include point mutations in BRAF and RAS and RET rearrangements (RET/PTC), affecting MAPK signaling pathway activation. BRAF mutation (BRAFV600E) is found in 35–70% of PTC and is frequently associated with tumor aggressiveness. The aim of this study was to compare transcription profiles of PTC according to the presence and frequency of BRAFV600E alleles and to identify molecular pathways deregulated in PTC carrying the alteration.
Sixty-one PTC and 13 surrounding normal thyroid tissues (SNT) were evaluated by oligoarrays using Sure Print G3 8×60K slides (Agilent Technologies). BRAF mutation were verified and quantified by pyrosequencing. Cases were stratified into three categories according to BRAFV600E allele frequency: negative/low (0–10%, n=21), intermediate (10–30%, n=21) and high (>30%, n=19). Unsupervised and supervised analyses (multi-group SAM) were performed. Canonical pathway analysis was generated through IPA software (Ingenuity® Systems). Ten transcripts were further assessed by RT-qPCR in 70 PTC and 15 SNT by taqman assays (Applied Biosystems).
The unsupervised hierarchical clustering revealed a total separation of normal samples and three clusters comprising all tumors, associated with BRAFV600E allele frequency (Fisher exact test, P<0.001). One-hundred and five genes were identified by supervised analysis (FDR 0%) and neuregulin signaling was identified as the major canonical pathway altered. All genes were confirmed by RT-qPCR as being differentially expressed in BRAFV600E tumors (one way ANOVA, P<0.01) and correlated with percentage of altered alleles (Pearson correlation test, P<0.01). Down-regulation of ELMO1, HGD, TFF3 and ZMAT4 and up-regulation of ERBB3, GGCT, NOD1, PDLIM4, PROS1 and RIMS2 was also observed comparing BRAFV600E PTC against the matched SNT (paired t test, P<0.001).
A distinct expression profile was observed according to the percentage of BRAF mutated alleles, with a predicted activation of the neuregulin signaling pathway. These findings provide additional information of potential therapeutic targets in treatment of advanced BRAFV600E harboring PTC.
Thyroid Cancer Saturday Poster Basic
Anaplastic thyroid carcinoma (ATC) is a highly aggressive undifferentiated carcinoma with a mortality rate near 100%. This high mortality rate is due to a multiplicity of genomic abnormalities resulting in the lack of effective therapeutic options. In order to find and apply effective targeted therapies, new molecular targets need to be discovered. Our lab has previously identified that the upregulation of RhoB is therapeutically beneficial in ATC and can serve as a molecular target.
For studying RhoB and its epigenetic regulation, HDAC inhibitors and HDAC shRNAs are used to examine the downstream effects of upregulated RhoB.
RhoB is repressed by HDAC1 and, for the first time, we identify HDAC6 as another repressor of RhoB. Both HDAC1 and HDAC6 are overexpressed in ATC and we find that RhoB has divergent downstream targets depending upon which HDAC is inhibited. When HDAC1 is inhibited by romidepsin or by shRNA, RhoB upregulates p21 leading to cytostasis. However, HDAC6 inhibition by belinostat, vorinostat, or shRNA leads to RhoB mediated upregulation of BIM resulting in apoptosis. Interestingly, these divergent pathways can be flipped between the two, through the bilateral regulation of RhoB. When p21 is silenced, romidepsin can now induce apoptosis through RhoB–>BIM. When BIM is silenced, the effects of belinostat and vorinostat now shift to RhoB–>p21 leading to cytostasis. The combination of these HDAC inhibitors with paclitaxel also yields divergent results. Belinostat and vorinostat in combination with paclitaxel results in synergy and this can be reversed when BIM is silenced. Romidepsin in combination with paclitaxel has no synergy, but when p21 is silenced, synergy is invoked.
Thus, to attain optimal therapeutic benefit, drugs that alter RhoB to favor BIM induced apoptosis should be employed. This study shows that the combination of either belinostat or vorinostat with paclitaxel may prove to be an effective therapeutic option in ATC patients by removing the repression of RhoB by HDAC6 and then adding paclitaxel.
Withdrawn
Thyroid Cancer Saturday Poster Basic
The association of special AT-rich binding protein 1 (SATB1) with a poor prognosis in various cancers has been reported. However, this association is controversial. We previously demonstrated immunohistochemical detection of SATB1 was independent of thyroid cancer differentiation. In this presentation, we further demonstrate expression pattern of SATB1 in well differentiated thyroid cancer.
SATB1 expression was immunohistochemically investigated in 35 papillary, 1 follicular, 6 poorly differentiated, and 2 anaplastic thyroid cancers.
SATB1 expression was observed in none of 2 anaplastic, 1 of 6 poorly differentiated, and 9 of 36 well-differentiated thyroid cancers. SATB1 expression was not significantly associated with any high-risk group-related clinicopathologic factors in well-differentiated thyroid cancer. Survival was not associated with SATB1 expression. In a case of diffuse sclerosing variant type of papillary carcinoma, SATB1 expression was observed in area of squamous metaplasia, but not in area of papillary carcinoma.
SATB1 expression is independent of thyroid cancer differentiation as well as high-risk-related factors of aggressiveness of thyroid cancer. SATB1 expression in a portion rather than papillary carcinoma may be associated with aggressiveness.
Thyroid Cancer Saturday Poster Translational
Anaplastic Thyroid Carcinomas (ATC) are aggressive, undifferentiated tumors for which there currently is no cure. Although ATC accounts for a mere 1.7 percent of all thyroid cancers in the United States, it is disproportionately responsible for a large fraction of thyroid cancer related deaths. Patients diagnosed with ATC have grim prognoses, with a median survival rate of 5 months. ATC not only is resistant to traditional radio and chemotherapeutics, but targeted applications as well. Furthermore, due to its highly invasive nature, surgical resection is often not an option. Clearly, new therapies for ATC are sorely needed. Stearoyl-CoA Desaturase 1 (SCD1) is a fatty acid metabolism enzyme whose expression has been implicated in pro-tumor survival of several subsets of cancer.
SCD1 expression patterns were examined in patient samples of normal thyroid, follicular adenoma (FA), papillary thyroid carcinoma (PTC), high grade follicular thyroid carcinoma (FTC), and ATC via quantitative real-time PCR as well as by immunohistochemistry. Activity of the SCD1 inhibitor A939572 was tested in representative patient derived cell lines.
SCD1 demonstrates high levels of expression in papillary thyroid carcinoma (PTC), high grade follicular thyroid carcinoma (FTC), and ATC. Application of an SCD1 inhibitor (A939572) surprisingly yielded strong anti-tumor proliferation and induction of apoptosis specifically in ATC cell lines, but had little to no activity among the other subtypes of thyroid carcinomas. In addition, A939572 induced the endoplasmic reticulum (ER) stress pathway, leading to endoplasmic reticulum associated degradation (ERAD) activation- a proteasome mediated survival response to ER stress. Sequential application of a proteasome inhibitor with A939572 led to synergistic anti-tumor activity in ATC cell lines.
We propose that administration of an SCD1 inhibitor concomitantly with a proteasome inhibitor is a novel course of treatment that may provide a clinical benefit for patients presenting with ATC.
Thyroid Cancer Saturday Poster Translational
Viruses are estimated to cause 15 to 20 percent of all cancers in humans but the mechanisms of latent infection and carcinogenesis vary depending on the particular virus, target cells, and host factors. Herpes viruses, such as Human Simplex Virus type 2 (HSV-2), Epstein - Barr virus (EBV), Cytomegalovirus (CMV) and Human Herpes Virus type 8 (HHV-8) have been associated with human malignancies and also with thyroid autoimmunity. HSV-2, EBV and CMV have already been found in autoimmune thyroid disease and EBV has been found in nasopharyngeal and breast cancer. HHV-8 is the etiologic agent of Kaposi's sarcoma, and both EBV and HHV-8 are considered oncogenic. We aimed to analyze the presence of HSV-2, EBV, CMV and HHV-8 in thyroid nodules.
Serum and thyroid specimens were prospectively collected from 97 thyroid nodule patients including 59 papillary thyroid cancers (PTC), 01 follicular thyroid cancer (FTC), 07 follicular adenomas and 31 goiters. There were 84 females and 14 males, aged 44±16 years. We used an ELISA assay to screen for antibody-positive patients and a real-time quantitative PCR (qPCR) technique to analyze thyroid tissues viral load.
All tissue samples were negative for HSV-2, CMV and HHV-8. However, we detected EBV DNA in 14 (15%) nodules including 10 (71%) PTCs and 4 (29%) goiters. All EBV-positive PTC samples were of classic histology and pTNM-1. Although the viral load was higher in malignant (544±1500 copies/ug) than in benign (292±365 copies/ug) nodules, this difference was not significant (p=0,1406). We did not find any association between the presence of EBV or its viral load and any clinical or pathological feature.
The presence of high EBV copy numbers in thyroid tissue, especially in PTC cases, suggest that this virus may play a role in the development of thyroid nodules and perhaps in thyroid malignancy.
Thyroid Cancer Saturday Poster Translational
We have shown that genetic profiling can be used to differentiate benign from malignant thyroid nodules, but there is heterogeneity in finding biologic relevance for these markers. In this study we sought to address this limitation.
We examined whole-genome miRNA expression in benign (n=20) and malignant (n=20) thyroid specimens and then used the thyroid cancer cell line TPC transfected with antimiR7, premiR7 and negative control scramble oligonucleotides to modulate the level of microRNA7. qRT-PCR<proliferation, invasion and apoptosis assays were performed to assess the biologic significance.
We found 43 miRNAs to be differentially expressed (P<0.05) with the majority being down-regulated in cancer. We found that either restoring the levels of mir-7 (a miRNA that is commonly downregulated in malignancy) in human thyroid cancer cell line TPC, we could inhibit proliferation and invasion while increasing apoptosis.
These data indicate that microRNA profiles can differentiate benign from malignant thyroid nodules, and that mir-7 may play a role not only as a marker but as a promotor of carcinogenesis.
Thyroid Cancer Saturday Poster Translational
Tumor-induced immunosuppression facilitates thyroid cancer progression by inhibiting host anti-tumor immune responses. Numerous mechanisms of tumor-immune tolerance have been described, including the recruitment of suppressor cells like tumor-associated macrophages (TAMs). Immune dysfunction in thyroid cancer is poorly understood, but likely correlates with more aggressive disease and recurrence. This study aims to evaluate the presence of TAMs and other immune cells in papillary thyroid cancer (PTC) patient specimens with respect to established clinical predictors of poor prognosis, including age, local invasion, and lymph node metastasis.
PTC tumor specimens and corresponding patient clinical data were obtained from the University of Southern California Tissue Bank with IRB-approval. Formalin-fixed paraffin embedded tumor tissue sections and controls were stained by H&E and immune cell markers, including CD68 to identify tumor-infiltrating macrophages. Stained sections were scored by a blinded pathologist for positive cells at the invading tumor margin and intratumorally, (5 HPF/specimen). Tumors specimens were stratified as having either low (<10) or high (>10) CD68+ staining cells/HPF.
Thirty-two tissue specimens were analyzed. All were classical PTC. Median age was 49 years (range 22–75). Patients were <45 years old in 10/31 (32%) of cases. Lymph node metastases were present in 19/31 (61%). Tumor specimens from patients older than 45 years had significantly more TAMs [13/21 with >10 CD68+ cells/HPF, (62%)] than tumors isolated from younger patients [2/11 with >10 CD68+ cells/HPF, (19%)](p<0.05). Tumors from older patients demonstrated significant deficits in intratumoral immune effector populations compared with tumors from younger patients.
Tumor-host immune interactions in PTC correlate with established clinical predictors of poor prognosis, such as age >45 years. These data suggest that distinct immune contexts may underlie the more aggressive disease and more frequent treatment failures observed in older PTC patients. Immunotherapeutic approaches may be of particular benefit in this subset of patients.
Thyroid Cancer Saturday Poster Translational
Well-differentiated thyroid cancer (WDTC) invading the aerodigestive tract is a rare entity whose surgical treatment remains challenging and oncologic outcomes poorer than non-invasive forms of this cancer. Information about extent of therapy, oncologic outcomes and functional results is under-reported. This study characterizes the oncologic outcomes and functional performance after curative surgery for WDTC invading the aerodigestive tract. We examine these typically under-reported aspects, and also, uniquely, describe the functional outcomes of therapy related to diet, speech, pain and quality of life.
A single institution retrospective review of 69 patients over a 9-year period who presented with WDTC invasion of the larynx, trachea and/or esophagus and underwent organ-preserving surgical resection.
Aerodigestive tract invasion occurred both initially (n=19, 27%) and as persistent or recurrent disease (n=50, 73%). Organ-preserving laryngo-tracheal resection was performed in 34 patients (47%) and esophageal wall resection in 39 (57%), achieving complete tumor excision with negative margins (R0) in 62%. While there was no perioperative mortality, procedure-related surgical morbidity included recurrent laryngeal nerve paresis (41%), tracheostomy dependence (28%), and permanent hypoparathyroidism (49%). Functional outcomes, however, revealed that nearly 70% of patients ate a regular diet, 59% had normal speech and the majority (63%) had normal activities of daily living. Overall survival at 3 and 5 years for the entire cohort was 79% and 71%, respectively. At the same timepoints, disease-free survival was 62% and 46%, respectively, with local/regional failure observed in only 9 (13%) cases.
Invasion of the aerodigestive tract characterizes a rare but particularly aggressive form of thyroid cancer. While overall and disease-free survival is lower compared to non-invasive WDTC, local disease control is achievable with good to excellent preservation of quality of life, supporting a strategy of appropriately aggressive, individually tailored surgery.
Thyroid Cancer Saturday Poster
The V600E BRAF mutation in papillary thyroid cancer (PTC) has been associated with aggressive clinicopathologic features. Our study evaluates the prevalence and clinicopathologic features of the BRAF mutation in both micro and macro PTC.
From August 2011 to December 2012, a prospective database was collected on 109 patients with PTC undergoing total thyroidectomy. BRAF mutation status was determined by a polymerase chain reaction (PCR) amplifying the codon 600 region. Associations between BRAF mutation status and clinicopathologic features were analyzed using Chi-square analysis and Fisher's exact test.
192 primary cancers in 109 patients were examined for the pathologic features and BRAF mutation. The BRAF mutation was present in 72% of all patients. The presence of BRAF mutation was not significantly associated with age, gender, tumor size, or extrathyroidal extension. Overall, 41% of the patients in this study presented with PTC<1 cm in size (microPTC). Presence of BRAF mutation was similar in both microPTC and in patients with larger tumors (75% vs. 71%, respectively, p=NS). Capsular invasion, extrathyroidal extension, and the presence of positive margins were more common in tumors >1 cm, irrespective of BRAF status (Table 1). Only extrathyroidal extension was significantly greater in tumors >1 cm (p=0.02). Cervical lymph node metastases were more common in patients with tumors >1 cm, and in those with BRAF positive status. The highest rates of extrathyroidal extension and positive margins were found in BRAF (−) tumors >1 cm (p=NS), while the highest rates of lymph node metastases and capsular invasion were found in BRAF (+) tumors >1 cm in size (p=0.04).
The presence of BRAF mutation is similar in both micro and macro PTC. BRAF (+) tumors >1 cm have the highest rate of capsular invasion and lymph node metastases. BRAF (+) microPTC have the same rate of capsular invasion and lymph node metastases as BRAF (−) tumors >1 cm. The role of BRAF mutation as a prognostic indicator in microPTC remains unclear.
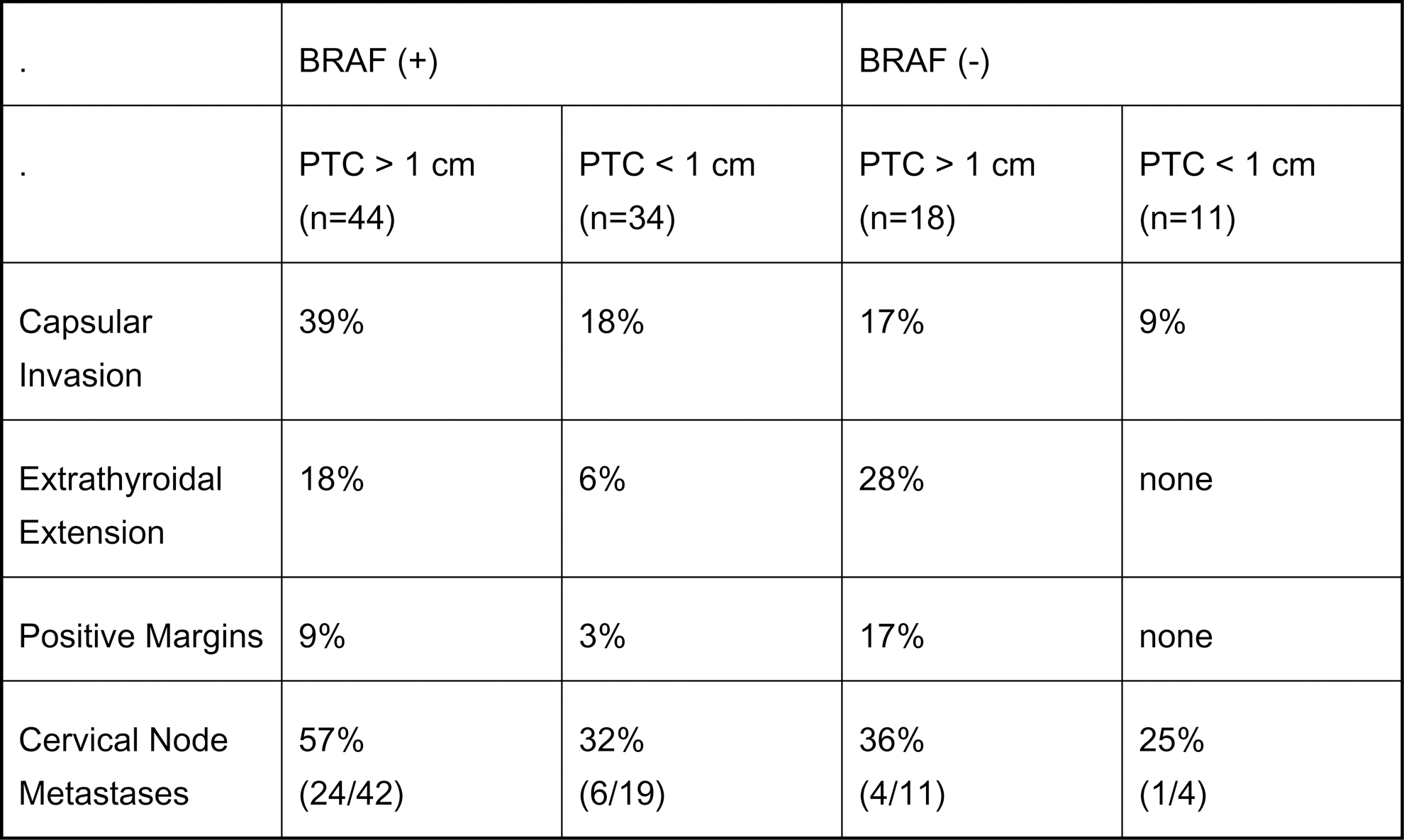
Thyroid Cancer Saturday Poster Clinical
An optimal dose of I-131 for successful ablation remains controversial in patients with differentiated thyroid carcinoma. The aim of this study is to compare the ablation success rate and recurrence rate of two different therapeutic doses, 3,700 MBq (100 mCi) and 5,550 MBq (150 mCi) in patients with papillary thyroid cancer (PTC) without distant metastasis.
We enrolled 275 patients who underwent I-131 ablation with either 3,700 MBq or 5,550 MBq after total thyroidectomy for PTC. All the enrolled patients underwent I-123 whole body scan (DxWBS), serum measurements of thyroglobulin (Tg) and neck ultrasonography (US) for evaluation of ablation results about 6 months after ablation. Patients with distant metastasis were excluded. The ablation success and recurrence rates were compared between the two doses. For appropriate comparison, preablation Tg was normalized by stratification into 3 groups, <1 ng/ml (Group A), ≥1 ng/ml and <10 ng/ml (Group B), and ≥10 ng/ml (Group C).
The ablation success rates were not significantly different between 3,700 MBq and 5,550 MBq in each Tg group (86.6% and 81.6%, p=0.494 in Group A; 75.0% and 65.1%, p=0.213 in Group B; 60.0% and 43.5%, p=0.502 in Group C, for 3,700 MBq and 5,550 MBq, respectively). Also, recurrence rates were not significantly different between the two doses in patients who were further followed up after ablation success (6.9% vs. 4.2% for 3,700 MBq and 5,550 MBq, respectively, p=0.453).
The therapeutic response to 3,700 MBq and 5,550 MBq of I-131 was similar to each other in papillary thyroid cancer without distant metastasis when analyzed within each Tg group. In PTC patients without distant metastasis, 3,700 MBq can be used instead of 5,550 MBq with less radiation exposure to patients and comparable therapeutic efficacy.
Thyroid Cancer Saturday Poster Clinical
The surgical management of inferior parathyroids during central neck dissection (CND) in papillary thyroid carcinoma (PTC) remains controversial. Most surgeons preserve inferior parathyroids in situ. Autotransplantation is not routinely performed unless devascularization occurs. This study aimed to compare routine autotransplantaion of inferior parathyroids with preservation in situ.
A total of 525 patients with PTC(pN1) underwent total thyroidectomy (TT) and bilateral CND with/without lateral neck dissection at West China Hospital of Sichuan University from February 2008 to February 2011. Among these patients, 7 had no statement of parathyroids, 9 had one or two superior parathyroids autotransplantation, 4 had no inferior parathyroids found intraoperatively. These patients were excluded. A total of 505 cases (109 males and 396 females) were analyzed retrospectively in this study.
All patients had central neck lymph node (CNLN) metastases including 323 ipsilateral and 182 bilateral. Of these, 290 were pT1-2N1 and 215 pT3-4N1. Three hundred and thirty-five patients underwent inferior parathyroids autotransplantation (autotransplantation group). Inferior parathyroids were preserved in situ among 170 patients (preservation group). Postoperative transient hypoparathyroidism rate was 20.3% (68/335) versus 24.7% (42/170) respectively (P=0.257). Permanent hypoparathyroidism rate was 2.09% (7/335) versus 5.88% (10/170) respectively (p=0.026). Mean numbers of resected CNLN were 9.05±2.800 (4–15) (autotransplantation group) versus 7.71±1.544 (5–11) (preservation group) (p=0.000). CNLN recurrence rate was 0.298% (1/335) versus 3.52% (6/170) respectively (p=0.003). Mean follow-up time was 42.51±6.76 months (23–60 m) (autotransplantation group) versus 42.98±5.01 months (24–61 m) (preservation group) (p=0.425).
Routine inferior parathyroids autotransplantation in CND of PTC (pN1) is better for prevention of permanent hypoparathyroidism and for thorough dissection of CNLN. Consequently, CNLN recurrence is reduced. Further study enrolling more patients with long-term follow-up is needed to support this conclusion.
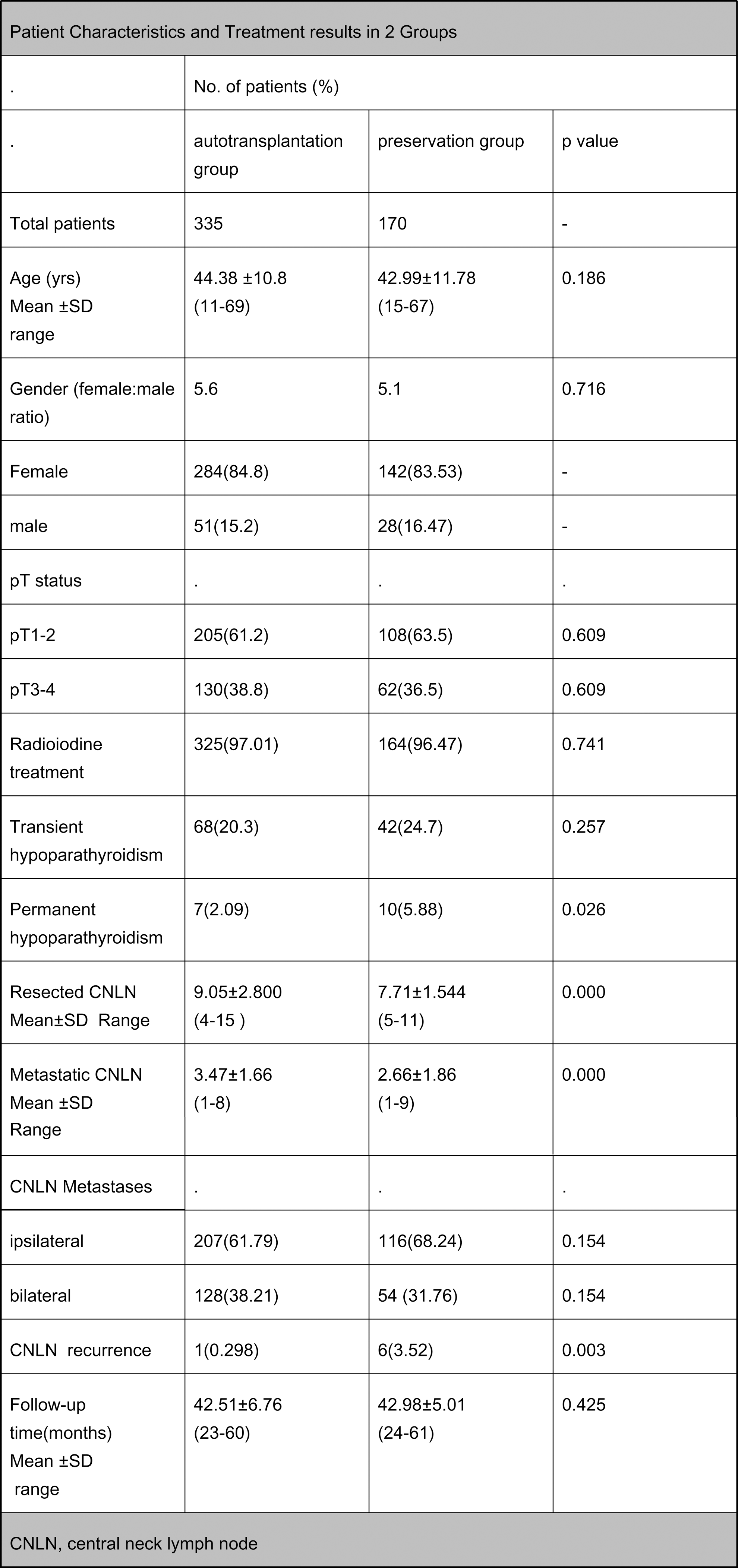
Thyroid Cancer Saturday Poster Clinical
The 2009 ATA Guidelines recommend TMN AJCC/UICC staging and risk assessment to predict risk for death and persistence/recurrence. They also propose reserving I 131 for higher risk advanced disease and selectively in lower stage disease, and considering molecular testing in the management of patients with indeterminate FNA cytology. However, what therapeutic measures should be taken when patients are BRAF+ remains unclear. In this study, we attempt to clarify the utility of BRAF mutation in managing the pre-op patient.
This is a prospective study examining surgical outcomes on 40 consecutive patients with indeterminate cytopathology between 2/11 and 3/13. Molecular testing was performed on neoplasm (26), suspicious for PTC(S) (4) or diagnostic for PTC (10) FNAs using Asuragen miRInform® or Ameripath Mutation Tests for BRAF V600E, RAS, RET/PTC and PAX8/PPAR-gamma mutations. Central lymph node dissection (CLND) was recommended for surgical candidates and performed by skilled community surgeons as a prophylactic measure to remove possible microscopic disease.
Of the 40 specimens (19 malignant/21 benign), 8 were BRAF V600E+ (2/4 suspicious, 6/10 PTC). 4 cases were RAS+ (4 neoplasms: FTC, FV-PTC, thyroid lymphoma and benign histology). CLND was extended to 19 patients (BRAF+, RAS+, S, PTC, and 1 other), CLND resulted in <2% complication rate, including transient recurrent laryngeal nerve paresis (<1 w) and transient hypoparathyroidism (<6 w). In BRAF+ group, nodal disease was detected in 4/8 and multifocal disease in 7/8 patients. None received I 131 ablation. To date, all patients, including 8 BRAF+ patients, have stimulated Tg <3 ng/ml and undetectable suppressed Tg with no signs of structural disease.
This study shows that selecting patients who are BRAF V600E+ for CLND performed by skilled surgeons with low complication rates may prevent persistence and render safer treatment alternatives, including no I 131 for residual metastasis that may likely be non-iodine avid.
Thyroid Cancer Saturday Poster Clinical
Management of patients with thyroglobulin (TG) positive/scan negative thyroid cancer remains challenging. ATA guidelines recommend potential use of empiric 131I therapy and various scanning modalities, but no standard for managing such cases exists. We surveyed American Thyroid Association members to assess current practice in management of patients with TG positive / scan negative disease.
Members participated in a web-based survey of six case scenarios of TG elevations but iodine scan negativity.
288 ATA members (80%M; 20%F) participated. Patient age, gender, and basal and stimulated TG varied between the cases. Respondents were asked their opinion regarding empiric 131I therapy use including 131I dosage, use, and duration of low iodine diet, T4 withdrawal or rhTSH, and utilization of additional imaging (neck US or PET/CT) and reconsideration of 131I therapy. Between 16–51% recommended initial use of empiric 131I for the various scenarios. The majority chose a 131I dose between 75–150 mCi and 73% employed a low iodine diet for ≥2 weeks. Preference between T4 withdrawal versus rhTSH was evenly split. Greater than 98% obtained a neck ultrasound if empiric 131I was not given. 52–89% would proceed to PET/CT if ultrasound was negative. Only 44% used rhTSH stimulation in PET scan preparation. 131I use was more common with stimulated TG significantly >10 ng/ml. 131I therapy was slightly more likely with PET positive (56%) than PET negative status (45%). Respondents were split regarding empiric 131I if basal and stimulated TG increased ≥150% over 2 years. Providers in North America less commonly utilized 131I treatment than those from other areas. In the face of TG assay interference, the majority did not recommend 131I therapy.
Empiric 131I therapy is still commonly utilized for cases of TG positive / scan negative disease. Neck ultrasound is frequently used to further evaluate such cases as is 18FDG-PET/CT, albeit somewhat less so. Use of 131I therapy correlated with degree of TG elevation, being slightly more common with PET positive versus PET negative status and is less commonly used by providers within North America.
Thyroid Cancer Saturday Poster Clinical
Due to its rarity and ambiguous classification, Hurthle cell cancer (HCC) has been subject to controversy with respect to natural course, optimal treatment and follow-up. Recent studies suggest that HCC is more likely to metastasize into the neck soft tissue and to distant sites rather than to cervical nodes, is less iodine avid and displays a more aggressive behavior compared to other differentiated thyroid cancers.
Utilizing Mayo Clinic Cancer Registry we identified 188 consecutive HCC cases evaluated and treated between 2001 and 2011, aiming to identify risk factors for poor prognosis and assess optimal follow up.
Of 188 patients, 87 had clinically persistent or recurrent disease, none of which were HCC minimally invasive histology. Eighty-eight local recurrences were noted in 50 patients, 35 in thyroid bed, 28 in neck soft tissue and 27 in cervical lymph nodes. Distant disease was diagnosed in 77 patients, located in lung (54), osseous (23), mediastinum (13), liver (4), brain (3) adrenal glands and skin (2 each), pancreas, kidney and pleura (1 each). Sensitive thyroglobulin levels generally correlated with tumor burden with the notable exception of 4 patients who had distant metastases and undetectable Tg (<0.1 ng/mL) and negative neck US therefore were missed with basic surveillance methods. Pulmonary metastases were best identified by CT (98% sensitivity) and were generally iodine resistant, with RAI scan being positive in only 9% of cases. MRI, CT and PET were equally sensitive in diagnosing osseous metastases (100%) with RAI scan sensitivity of 50%. Multivariate analysis identified age >60 years, tumor size >4 cm, T3-4, N1, M1 status and MACIS score ≥6 as significant (p<0.05) risk factors for disease related death. 5-year estimated cumulative incidence of disease-related death was 76% in patients with distant metastases, compared to 7% in those with loco-regional disease.
Our study indicates that HCC has a more aggressive clinical behavior and a distinct metastatic mechanism therefore would benefit from individualized management guidelines. Initial histological diagnosis should be confirmed by an experienced endocrine pathologist. RAI scan has a very low sensitivity in detecting distant disease.

Thyroid Cancer Saturday Poster Clinical
Thyroid hormone withdrawal (THW) is required for a postoperative radioiodine adjuvant therapy or diagnostic radioiodine whole body scan in patients with differentiated thyroid cancers. Acute thyroid hormone deficiency following THW often results in a transient abnormality of lipid profiles. We aimed to clarify the clinical factors influencing the post-THW dyslipidemia that has not been fully elucidated.
A total of 61 patients with papillary thyroid cancers who underwent postoperative 1.1 GBq 131-I remnant ablation and lipid profiling after a 3-week THW were included in the study. The patient demographics and various biochemical parameters measured before and after the surgery and during postoperative follow-up periods were retrospectively analyzed.
While the mean total cholesterol level after THW was significantly higher than the preoperative baseline level (249.1±58.0 mg/dL vs. 194.8±39.8 mg/dL, P<0.001), lipid profiles returned to the baseline level at a follow-up visit after a levothyroxine re-administration. Total cholesterol level after THW was correlated with the level of the preoperative baseline total cholesterol and a preoperative body mass index (BMI). Other parameters such as age, gender, or elevated TSH level after THW showed no correlation with a total cholesterol level following THW. The overweight patient group (BMI≥23 kg/m2) had a greater post-THW total cholesterol level (260.8±61.2 mg/dL vs. 226.1±43.8 mg/dL, P=0.015) and LDL-C level (178.5±55.6 mg/dL vs. 146.1±36.3 mg/dL, P=0.025) compared to the normal weight patient group, although there is no difference in the baseline total cholesterol level between the two groups. BMI was found to be an independent determining factor of post-THW total cholesterol level along with the preoperative baseline total cholesterol level and an elevated TSH level following THW through a multiple logistic analyses.
BMI is an independent factor determining the post-THW serum total cholesterol level in thyroidectomized patients. Therefore, overweight patients who underwent total thyroidectomy may be more susceptible to the adverse metabolic effects of thyroid hormone deficiency.
Thyroid Cancer Saturday Poster Clinical
Recombinant human thyroid stimulating hormone (rhTSH) has been approved by the FDA since December 2007 for preparation of thyroid remnant ablation with radioactive iodine (RAI) in low risk patients with well differentiated thyroid cancer and no evidence of metastatic disease following total or near total thyroidectomy. There is currently insufficient data on the safety & efficacy of rhTSH preparation for RAI treatment of thyroid cancer patients with nodal metastatic disease diagnosed at the time of thyroidectomy.
A retrospective analysis was performed on 108 consecutive patients with histopathologically-confirmed nodal metastatic differentiated thyroid cancer following thyroidectomy, treated with initial RAI by our institution between January 1, 2000 & December 31, 2007. Within this selected group, 31 and 42 patients were prepared for initial and all subsequent RAI treatments exclusively by thyroid hormone withdrawal (“withdrawal”) & rhTSH protocols respectively, with a requirement of at least three years local follow-up or death related to thyroid cancer. Short and long term clinical outcome & treatment responses were compared.
There were no significant differences between the baseline patient characteristics of the two groups with the exception of two negative prognostic risk factors - male gender & age ≥45 years - which were both more prevalent in the rhTSH group (P=0.05 for both parameters). The mean follow-up was significantly longer for the withdrawal group than for the rhTSH group (8.6 versus 6.8 years; P=0.01). There was no significant difference in the final clinical outcome assessment of the rhTSH and withdrawal groups. The response to initial treatment - classified as either excellent, acceptable or inappropriate - was significantly better for the rhTSH group (57%, 21% and 21%, respectively) than for the withdrawal group (39%, 13% and 48%; P=0.05). The rhTSH group also received significantly fewer additional doses of RAI than the withdrawal group (P=0.03).
The findings suggest that in patients who present with nodal-positive differentiated thyroid cancer, preparation for radioactive iodine therapy with rhTSH is a safe & efficacious alternative to thyroid hormone withdrawal protocol.
Thyroid Cancer Saturday Poster Clinical
Follicular variant of papillary thyroid cancer (FVPTC) is a common PTC type which exhibits considerable clinical and pathologic heterogeneity. Both FVPTC and follicular thyroid carcinoma (FTC) are difficult to diagnose by fine needle aspiration biopsy (FNAB). When FNAB cytology is indeterminate, molecular panel testing (MT) including PAX8/PPARγ rearrangement markers has augmented clinical management. PAX8/PPARγ rearrangements are known to be a common event in follicular thyroid carcinomas, and the outcome for patients with this rearrangement remains not well understood.
Over a 5.5 year period in a high-volume program, we prospectively performed PAX8/PPARγ testing in preoperative FNAB from all cytologically malignant or indeterminate thyroid nodules (Bethesda categories of FLUS/AUS, HCN, FN, or suspicious) and on histologic cancers when MT was not preoperatively performed. Pathology slides on all surgically removed nodules were examined. The clinical records of all patients with nodules positive PAX8/PPARγ results were reviewed.
Among 16 patients with PAX8/PPARγ positive thyroid nodules, there were 10 (63%) women and age ranged from 13–66 years. Cytologic diagnosis was benign (1), FLUS/AUS (2), FN (7), HCN (4), and suspicious (2); none were cytologically malignant. On final pathology, all PAX8/PPARγ positive nodules diagnosed by FNAB were found to be malignant. Among them, 75% (12/16) were FVPTC, 2 were FTC, one was oncocytic FTC, and one was solid variant of PTC. All PAX8/PPARγ FVPTCs were encapsulated (12/12), with frequent capsular (5/12) or vascular (3/12) invasion and a high rate of concurrent papillary microcarcinoma (4/12). No PAX8/PPARγ FVPTC lymph node metastasis or recurrence was present in short-term follow-up.
In this series, PAX8/PPARγ rearrangement found in indeterminate cytology nodules had a 100% predictive value for differentiated thyroid cancer, and was much more predictive of PTC, particularly of FVPTC (75%), rather than FTC (19%). PAX8/PPARγ thyroid carcinomas are encapsulated with frequent vascular and/or capsular invasion, and clinical indolence on short-term follow-up.
Thyroid Cancer Saturday Poster Clinical
We have previously reported on the selective use of radioiodine remnant ablation (RRA) in low-risk papillary thyroid carcinoma (PTC) patients using a post-surgical TSH-stimulated serum thyrogloubulin (Stim-Tg) biomarker. A decreae in Stim-Tg after RRA is well establish, however, little is known about the natural trend of Stim-Tg measurements in PTC patients not treated with RRA therapy. Herein, we provide the first report on the natural history of post-surgical serial Stim-Tg measurements among low-risk PTC patients not receiving RRA, followed prospectively for more than 5 years.
We prospectively analyzed serial Stim-Tg measurements among a cohort of 95 consecutive low-risk PTC patients who did not receive RRA. All patients underwent total thyroidectomy, with a minority receiving concurrent central neck dissection if clinically indicated. Low-risk was defined as PTC confined to the thyroid gland or level VI lymph nodes. Patients were selected to avoid RRA based on an initial 3-month post-surgical Stim-Tg <5μg/L (previously published as the Stim-Tg Protocol). Linear regression modelling was used to assess the trend in serial Stim-Tg measurements as a function time—from surgery to a median of 5.2 years of follow-up. Decreasing, unchanged, and increasing Stim-Tg was defined as an annual Stim-Tg change of <−0.5μg/L, >−0.5 to <0.5μg/L, and >0.5μg/L, respectively.
Sixty (63.2%) patients had an initial Stim-Tg that was undetectable (<1μg/L). Of those, serial Stim-Tg remained unchanged in 54 (90%) patients and increased in 6 (10%) patients. For the remaining 35 (36.8%) patients with an initial Stim-Tg that was detectable (≥1μg/L), serial Stim-Tg was found to decrease, remain unchanged, and increase in 15(43%), 18(51%) and 2(6%) patients, respectively. The maximum absolute value of Stim-Tg for patients with an increasing Stim-Tg trend remained ≤4μg/L, with no ultrasonographic or histologic evidence of PTC recurrence.
Post-surgical Stim-Tg decreases or remains unchanged in most low-risk PTC patients who do not receive RRA. These observations suggest that the decrease in Stim-Tg often attributed to RRA, may also occur post-surgically in the absence of RRA.
Thyroid & Development Saturday Poster Clinical
Recurrent Laryngeal Nerves' (RLN) extralayngeal bifurcation into anterior and posterior branches has been well described in the literature. Presence of branching conveys an increased risk of nerve injury during thyroid surgery. Little is known about gender and racial variations in RLN extralaryngeal branching. We hypothesized that variations exist, and analyzed intraoperative neuromonitoring (IONM) data for patients who underwent thyroid surgery.
A retrospective review of a prospectively collected database identified all patients who underwent thyroid or parathyroid surgery with IONM in a four year period by a single surgeon in an academic North American institution. Details of nerve dissection and monitoring were recorded.
We identified 467 patients in which 689 RLNs were at risk. Three hundred eighty-four patients were female (82.5%) and 210(45.5%) were African American (AA). Overall, 261 RLN (37.9%) had an extralaryngeal bifurcation at 10.45±0.53 mm from cricothyroid membrane (CTM). Motor fibers were present in 100% of the anterior and 3 of the posterior extralaryngeal RLN branches (1.2%). In males, 52 of 127 RLNs (40.9%) bifurcated. Of the 562 RLNs in female patients, 209 RLN (37.2%) bifurcated (p=0.43). RLNs in males bifurcated at the average distance of 8.55±0.76 mm from CTM versus 10.93±0.61 mm in women (p=0.016). In AA patients, 133 of 315 nerves (42.2%) at risk bifurcated. In the 222 Caucasians, 121 of the 346 RLNs (35.0%) bifurcated (p=0.056). AAs' RLNs bifurcated at the average distance 9.86±0.51 mm from CTM compared to 10.69±0.79 mm in Caucasians (p=0.38).
Our study demonstrates gender is not associated with a statistically significant difference in RLN bifurcation; however, males have RLN's whose bifurcation is closer to the CTM. AA patients also have no statistically significant difference in the rate of RLN bifurcation when compared to their counterparts; however, the trend suggests increased prevalence of bifurcation (in AA's). Further investigation is warranted.
Withdrawn
Thyroid Cancer Saturday Poster Clinical
Obesity is associated with a number of medical comorbidities and is considered a risk factor for surgical complications. However, the impact of obesity on the safety of minimally invasive video-assisted thyroidectomy (MIVAT) has not been well-defined. We sought to determine the relationship between obesity and the risk of complications in patients undergoing MIVAT.
A prospectively maintained database of all thyroid surgeries performed from January 2006 through June 2012 was queried and all cases of MIVAT were identified. Patients were stratified into 3 body mass index (BMI) groups according to the National Institutes of Health classification for obesity: normal (BMI≤24.9 kg/m2), overweight (BMI 25 to 29.9 kg/m2) and obese (BMI≥30 kg/m2). The total number of complications was compared among the three groups.
There were 238 MIVATs performed on 228 patients. The mean overall BMI for the study population was 25.5 kg/m2. There were 124 procedures (52%) in the normal group, 78 procedures (33%) in the overweight group and 36 procedures (15%) in the obese group. Complications included one case of cellulitis (0.4%), 6 cases of temporary hypocalcemia (2%) and 6 cases of transient recurrent laryngeal nerve (RLN) weakness (2%). No patients suffered permanent hypocalcemia or a permanent RLN injury. There were 9 complications in the normal group (7.3%), 4 complications in the overweight group (5.1%), and no complications in the obese group. Due to the low number of complications in this series, the overweight and obese groups were combined into a high BMI group for further analysis. Statistical analysis using simple logistic regression models revealed that there was no significant difference in the number of complications in patients with a high BMI compared with patients with a normal BMI (OR=0.45, CI:0.13–1.55, p=0.2).
Overweight and obese patients undergoing MIVAT in this series were not at an increased risk for surgical complications. The MIVAT procedure may be considered safe in patients with a high BMI.
Thyroid Cancer Saturday Poster Clinical
We investigated if post-total thyroidectomy urinary iodine concentration (UIC) in patients undergoing CECT is comparable to those not undergoing CECT and if patients with intact thyroid have higher UIC after CECT.
This prospective study consisted of patients undergoing surgery for thyroid and non-thyroid diseases. Patients were divided in 4 groups consisting of 31 each. Group I- Differentiated thyroid carcinoma (DTC) patients undergoing preoperative CECT, Group II- DTC patients not undergoing CECT, Group III- Benign goiter patients undergoing CECT, Group IV- Patients with non-thyroidal diseases undergoing CECT. CECT was performed using either Omnipaque or Ultravist. A minimum of 3 spot urine samples were collected from each patient: 1- Basal sample (prior to CECT), 2- Sample at the time of discharge (5–10th post-operative day) and, 3- Follow-up sample (about 6 weeks after surgery). UIC was measured by method based on the Sandell-Koltoff reaction. Time intervals from the day of CECT to surgery, surgery to collection of sample at discharge; and follow-up were noted for each patient. Results are expressed as medians for UIC (μg/L) and time intervals. Statistical analysis was done on SPSS version 10. Non- parametric tests were used to test the difference among groups.
Duration from CECT to surgery, surgery to discharge; and surgery to follow-up was 2, 5 and 42 days respectively for the whole cohort. Interval form CECT to surgery was significantly shorter in Group IV as compared to Group I (2 vs 5 days, p=.022). Interval from surgery to discharge was significantly shorter in Group II (4 days) than other groups (p=.006). However, the follow- up interval was comparable among the groups (p=.51). There was no significant difference in basal (p=.22) and follow-up (p=.38) UIC among the Groups (I- 284& 223, II- 258& 250, III- 269 & 304, IV- 179 & 408). However, UIC at the time of discharge differ significantly (p=.018); Group I (855), III (757), and IV (671) had higher UIC as compared to Group II (285). 74 and 48% in Group I and II respectively were off thyroxine (30 days) at the time of collection of follow-up samples.
CECT using non-lipophilic contrast does not result in long-term iodine retention.
Thyroid Cancer Saturday Poster Clinical
Thyroid cancer (TC) spinal metastases (SMs) are associated with reduced quality of life and increased mortality, thus, their early recognition and treatment are essential. The goal was to analyze TC-SMs to predict type-specific clinical behavior to optimize follow-up and treatment plans for TC patients.
174 FTC-SMs (n=120) and PTC-SMs (n=54) patients treated at MedStar Washington Hospital Center (n=31) and collected from the literature (n=143) were analyzed.
66% FTC patients were female, males predominated in PTC (55%) (p<0.02). SMs were more often initial manifestations of FTC (as compared to being diagnosed after FTC) (41% vs 24%); PTC-SMs were commonly diagnosed after TC diagnosis (76% vs 59%) (p<0.05). Solid organ involvement in FTC-SMs manifested TC was less common than in FTC-SM developed after TC diagnosis (34% vs 67%) (p<0.05). FTC-SMs developed within 82+34 (0–372) months and PTC-SMs within 35+17 (0–144) months (p<0.01) from TC diagnosis with PTC-SMs being diagnosed more frequently as synchronous (63% vs 36% in FTC) and FTC-SMs as metachronous metastases (64% vs 37% in PTC) (p<0.01). 28% of FTC and 37% of PTC had only SMs as distant metastases. Multilevel FTC-SMs compared to solitary FTC-SMs were associated with other bone non-spinal (82% vs 30%) and solitary organ metastases (65% vs 41%) (p<0.01) with no correlation in PTC-SMs. FTC-SMs presented as neural compression (72% vs 36%); PTC-SMs were asymptomatic (38% vs 5%) (p<0.01). FTC-SMs were more often I-131-avid (p<0.01) and required spinal surgery more frequently (72% vs 55%) (p<0.05) compared to PTC.
FTC-SMs and PTC-SMs typically have distinct presentations and behavior, should be categorized separately for treatment and follow-up. FTC-SMs represent the most favorable group for treatment. SMs may occur up to 372 months after TC diagnosis which emphasizes the need for long term monitoring. A significant portion of TC patients have isolated SMs without evidence of additional distant metastases.
Thyroid Cancer Saturday Poster Clinical
Indications for performing a central neck dissection (CND) in patients with well-differentiated thyroid cancer (WDTC) are unclear. In addition, how lymph node (LN) metastases should factor into the decision-making process for administration of adjuvant radioactive iodine (RAI) also remains unclear. Our objectives were to assess indications for performing CND and explore variability of LN retrieval across centers and amongst surgeons in the province of Alberta and to identify factors that predict the use of adjuvant RAI in this population. The study design was a province-wide cross-sectional analysis.
A prospectively collected provincial synoptic operative report identified 594 patients who underwent total thyroidectomy for WDTC +/− CND. Demographics, peri-operative and pathologic factors were analyzed.
Between 2009–2012, 18 surgeons performed 425 CND's, 313 unilateral and 112 bilateral. 224 CND were prophylactic (no clinically apparent lymph node metastases). Conventional risk factors such as age, tumor size, and suspicion of extra-thyroidal extension were not predictors of performing a CND. Presence of positive lymphadenopathy prior to surgery was the only significant indication for performing CND. Positive LN's were retrieved in 39% of prophylactic CND, and thus 39% of patients were upstaged from clinical N0 to pathologic N1a stage as a result of performing a CND. Amongst all peri-operative predictors of receiving RAI, presence of LN metastases was the strongest predictor [OR=5.9(3.7–9.5)], while tumor size was a modest predictor [OR=1.8(1.5–2.1)]. Traditional risk factors for more aggressive WDTC such as age and evidence of extrathyroidal extension did not predict use of adjuvant RAI.
In this provincial cohort, conventional risk factors were not identified as indications for performing a CND, implying that this decision was surgeon-specific. Prophylactic CND upstaged 39% of patients from cN0 to pN1a, and as such these patients were six times more likely to receive adjuvant RAI. By contrast, conventional risk factors were not predictors of receiving adjuvant RAI. A unified approach to performing a CND and administering RAI among specialists in Alberta is lacking.

Thyroid Cancer Saturday Poster Clinical
Vemurafenib, a selective BRAF inhibitor, appears to have promising clinical activity. Recently reported results of 3 patients with PTC harboring BRAF mutations treated with vemurafenib in phase I trial showed that 1 patient had a confirmed partial response (PR) and 2 patients had stable disease (SD).
This is a case series of BRAF V600E positive PTC patients treated outside a clinical trial with vemurafenib. Best response was evaluated using RECIST v1.1 (PR>30% reduction, progression >20% increase in sum of target lesions, and SD any percent change between +19% and −29%). Minor response (MR) was defined as 10–29% tumor size reduction. All images were reviewed by a radiologist. Adverse events (AEs) were evaluated using CTCAE v.4.0.
15 patients receiving vemurafenib were identified, of which 12 were evaluable. All patients had BRAF V600E positivity by DNA testing. Median age at diagnosis was 62 years, 3 patients had poorly differentiated carcinoma, 11/12 patients had stage IV disease at diagnosis. All patients had RAI non avid disease. At the time of vemurafenib start, site of distant metastases included lung in 75% and bone in 40%. Figure 1 shows best response: PR 3/12 (25%), SD 9/12 (75%; of which 5/9 had MR). Updated response data and progression free survival will be presented at the meeting. Median time on treatment was 20 weeks (5–44). 11 patients are still on treatment at the time of this analysis. Vemurafenib starting dose was 960 mg twice daily. Drug hold and dose reduction was needed in 75% and 50% of patients, respectively. Most common AEs: skin rash (50%), anorexia (50%), fatigue (50%), diarrhea (42%), photosensitivity (42%), verrucous keratosis (42%), weight loss (25%), arthralgias (25%), hand foot syndrome (25%) and hair loss (25%). 2 patients had biopsy proven squamous cell carcinoma. 1 patient developed uveitis. Grade 3 AEs: photosensitivity (2 patients) and hand foot syndrome (1 patient). Grade 4 AEs: elevated lipase (1 patient).
In patients with advanced metastatic PTC harboring the V600E BRAF mutation, vemurafenib may be an effective and well-tolerated treatment strategy.
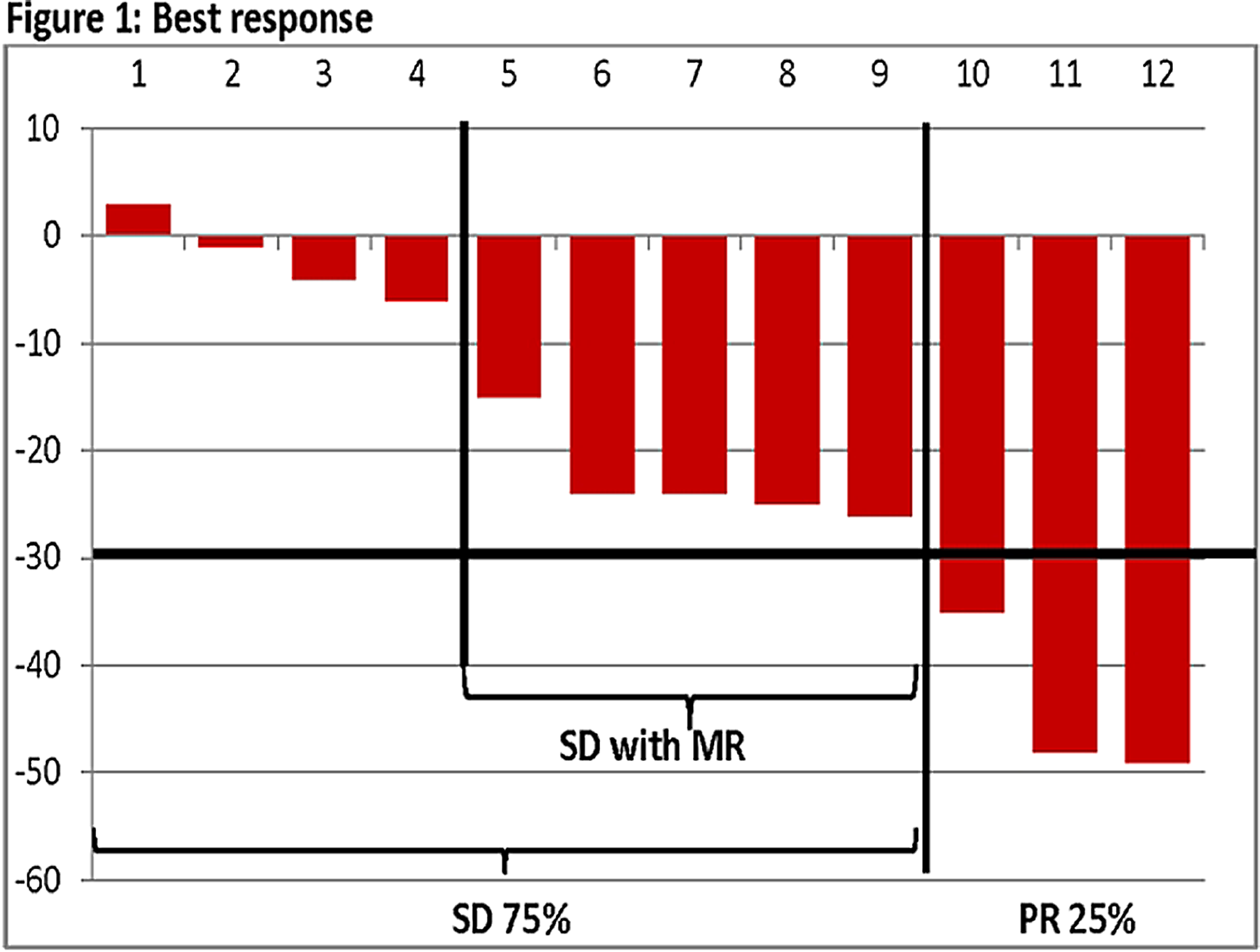
Thyroid Cancer Saturday Poster Clinical
Ideal surgical management of lymph nodes in patients with well-differentiated thyroid carcinoma (WDTC) is still subject of controversy. Given the inherent risks and unknown benefits, routine prophylactic central compartment neck dissection (CCND) is litigious. Sentinel lymph node biopsy (SLNB) has recently been shown to be an accurate predictive tool of locoregional disease. In this study we aim to determine the effect of the dominant nodule size on the rate of metastasis to the sentinel lymph node. As a second goal, we wish to find an association between the total number of nodules and SLNB outcome.
In this retrospective study, SLNB using 1% methylene blue dye was performed in 285 patients undergoing thyroidectomy and CCND for WDTC. Ultrasound reports were reviewed to determine the size of the dominant nodule and the number of nodules. According to the latter, patients were classified with either solitary nodule, solitary nodule with micronodules, or multiple nodules.
Patients were divided into two groups: 245 with negative SLNBs and 40 with positive SLNBs. No statistically significant difference was found between the two groups when looking at age (p=0.461) and gender (p=0.181). The mean dominant nodule size in the positive SLN group was significantly lower than the negative SLN group (2.3 vs 2.9 cm, respectively; p=0.008). Using logistic regression we found that each augmentation of 1.0 cm in nodule's size diminishes the risk of a positive SLNB by 41% (OR=0.587; 95%CI[0.410; 0.840]). SLNB outcomes were not found to be significantly associated to the number of nodules (p=0.521).
According to our results, there is a direct correlation between the size of the dominant nodule and SLNB outcome, such as the rate of malignancy decreases with the nodule's size. Furthermore, SLNB outcome is independant of the total number of thyroid nodules.
Thyroid Cancer Saturday Poster Clinical
The role of intraoperative frozen section(FS) in thyroidectomy has controversy. Intraoperative FS was used to decide the extent of surgery in cases of non-diagnostic preoperative cytology. The aim of this study was to investigate the association of combined of thyroiditis and diagnostic accuracy of FS.
From January 2012 to May 2013, 840 patients underwent thyroid operation in National Medical Center. Fourteen cases of recurred thyroid cancer and 20 cases of completion thyroidectomy were excluded because FS is not necessary for determining extent of surgery. FS and permanent pathology of 806 cases reviewed retrospectively. Non-diagnostic frozen section included ‘no tumor’, thyroiditis, atypia. FS was performed by endocrine surgeon and interpreted by endocrine pathologist.
FS was non-diagnostic in 18 cases. Six cases were misdiagnosed by pathologist (diagnostic error) and 12 cases were sampled from inappropriate sites by surgeon (sampling error). The present of thyroiditis shows significantly higher rates in sampling error than diagnostic error (67% vs 34%, p<0.05).
The present of thyroiditis is associated with non-diagnostic FS, especially causing sampling errors. We might suggest to take careful considerations on intraoperative FS in patients with thyroiditis.
Thyroid Cancer Saturday Poster Clinical
Background: Rhodiola rosea (RR) is a plant adaptogen commonly used for stress adaptation. Our group previously published RR could be of help ameliorating the stress imposed on the body by the progressive loss of thyroid hormone in patients in whom replacement therapy is withdrawn for 4–6 weeks prior to radioactive iodine imaging for thyroid cancer. Objectives In line with our previous work, we decided to evaluate the potential usefulness of this approach comparing it with current clinical practice (hormone withdrawal [HW] or administration of recombinant thyroid stimulating hormone [rTSH]) by using an economic analysis.
Materials/Methods: The following parameters were estimated from published medical articles: rates of sick-day leave, amount of days off, and costs of rTSH injections. Average labor was downloaded from www.averagesalarysurvey.com. Cost of a month supply of RR was estimated at $ 30. Decision trees were constructed using Insight Tree Private Edition v3.0 software. Rates and costs of complications of each approach were not included in the analysis as it was assumed they would lead to work absence making the final endpoint selected (costs of sick leave days) a fair representation. The analysis was done from the employer's perspective. Because no clinical trials where RR was studied in this scenario were identified, we used these rates to run simulations accounting for use of RR.
Results: Average gains in terms of costs of sick leave days saved were $ 1771.03 for rTSH and $ 3064.49 for the HW. The best scenarios for RR were gains of $3940.25 if RR could reduce to 2 days of work lost (=rTSH option) with a rate of 48% (=HW option), and $ 3872.32 gains if RR could reduce the number of patients going on sick leave to 11% (=rTSH option) even if the duration was 12 d (=HW).
Conclusions: This theoretical evaluation on saving costs from sick day leave suggests supplementing thyroid cancer patients with RR during periods of HW might be a cost-saving alternative. We believe further clinical studies that include economic data analysis are warranted.
Thyroid Cancer Saturday Poster Clinical
Anaplastic thyroid cancer is a rare type of thyroid malignancy accounting for only 1.3% of all thyroid malignancies. It is one of the most aggressive solid tumors to affect humans, with a median survival of 4 months following diagnosis. Despite its rarity, it contributes up to 14–50% of the annual mortality associated with thyroid cancer.
This is a retrospective study of all anaplastic thyroid cancer cases diagnosed by biopsy in the Philippine General Hospital between 2008 and 2013. Clinical presentation, physical findings, diagnostic tests and management received were all documented and described.
A total of 15 patients were identified. Median age at diagnosis was 63. All tumor sizes were at least >6 cm upon diagnosis. All had previous history of thyroid pathology presenting with an average duration of 11 years. Eleven patients (73%) presented with cervical lymphadenopathies upon diagnosis while 7 (47%) showed signs of distant metastases where lungs appeared to be the most common site. More than 70% of patients presented with a rapidly growing (<3 months) fixed hard neck mass leading to airway obstruction as the most common reason for admission at our institution. Only 3 patients (20%) were treated with curative surgery. Majority (80%) received palliative and supportive form of treatment. Only 3 patients (20%) were offered with radiotherapy but none was able to complete the full regimen. Chemotherapy was not offered to any of the patients in the study. Only 2 remaining patients were confirmed to be alive during this study. Median survival for most of the patients was 3 months from the time of admission and diagnosis. Majority (>90%) will die within the first year after diagnosis.
Our experience on anaplastic thyroid cancer showed concordance with the current clinical profile, presentation and prognosis compared with other institutions. Absence of distant metastases and lymph node involvement translated to better survival outcomes while age at diagnosis and tumor size did not affect survival. Curative surgery offers the most effective means to prolong survival. Radiotherapy and chemotherapy in combination with surgery might offer promise in the future.
Thyroid Cancer Saturday Poster Clinical
Inflammation plays a critical role in many aspects of cancer, tumor development, progression and prognosis. Interaction between tumor and host may have significant influence on patient's outcome, but there's still few studies for thyroid carcinoma. Neutrophil-to-lymphocyte ratio (NLR) is emerging as a simple and valid marker of systemic inflammation response, which is inexpensive, easily calculated, and universal available. The aim of this study was to evaluate the relationship between NLR and the prognosis of patients with papillary thyroid cancer.
We included patient who had total thyroidectomy for papillary thyroid carcinoma between 1995–2005 in Asan medical Center. Only typical papillary thyroid carcinoma patients and who had complete blood counts with automated differential counts before surgery were included. Patients were categorized on the basis of NLR into two groups and analyzed clinico-pathological variables and prognosis between these groups. All statistical analyses were performed using program R (project R).
Total 1142 patients were enrolled to this study. At a median follow-up of 48 months, 170 patients showed loco-regional recurrence or distant metastasis. When we performed univariate analysis between two groups stratified by NLR, there was no differences in clinico-pathologic variables. When we compared disease-free survival between two groups stratified by NLR, there was little statistical difference. (p=0.48) After adjusting for risk factors to perform multivariate analysis, N stage (p<0.0001) and extra invasion (p<0.0001), there was no significant difference according to N stage (N0:p=0.86, N1a:p=0.4, N1b:p=0.12) and extra invasion (data not shown).
There was no significant relationship between LNR and papillary thyroid carcinoma in this study, yet, there are several conflicting results about NLR and thyroid carcinoma, it is early to consider NLR as a prognostic predictor of thyroid carcinoma.
Thyroid Cancer Saturday Poster Clinical
Although surgery and radioiodine are the standard curative therapy for papillary thyroid cancer (PTC), management of progressive PTC, such as invading to aerodigestive tract, major vessels and spine, are still discussed. These progressive findings are uncommon but absolutely worsens its prognosis. In this study, we aim to assess our treatment regimens and results for such severe cases.
Investigation of 381 cases of thyroid tumor resections, which were performed at our faculty in recent 13 years (2000–2012), revealed 8 severe cases. We report a detailed clinical history in one severe case and evaluated our managements retrospectively.
The patient was a 67-year-old woman, who was introduced to our hospital as suspicious esophageal cancer. At the first examination, computed tomography (CT) indicated a low-density mass behind the trachea, which measured 35 mm in diameter, and endoscopic survey revealed submucosal tumor with strong erosion. Fine needle aspiration (FNA) cytology showed PTC. At first, tangential tumor excision with shaving technique was executed, but most of tumor remains attaching firmly to the esophagus and trachea. After 13 months follow-up, residues of PTC grew invading the larynx and esophagus. So that, with patients' admission, salvage pharyngolaryngectomy with free jejunum flap reconstruction was performed and radioactiveiodine (RAI) therapy was executed subsequently. After 1.5-year follow-up since last RAI, PTC recurred and invaded to jejunum flap and the cervical vertebrae. Salvage operation with gastric tube reconstruction was executed in combination with intraoperative radiation therapy and photodynamic therapy. As further treatment, RAI still go on subsequently.
The management of invasive thyroid cancer remains controversial. Several studies have shown no significant difference in survival between radical and conservative resection. Although long-term prospective studies are still required, any kind of salvage therapies are still necessary for such progressive cases, based on our experiences.
Thyroid Cancer Saturday Poster Clinical
Metastatic thyroid cancer is rare. Whereas the small cell lung cancer is a prognostic poor type in lung ca., and the 3-year survival rate is around 30% with the 'LD' type which said that it is relatively good of the prognosis. We experienced the very rare case that late-metastasized to only thyroid gland four years later since small cell lung ca. recovered completely once. Because of its localizing, in combined modality therapy, we were in charge of surgery (total thyroidectomy) in our department and were able to examine effects of the preceding chemotherapy.
Thyroid cancer treated in our department by March 31, 2013 from April 1, 1996 was 207 cases and, by the frequency order, was papillary carcinoma 165 (79.7%), follicular ca. 26 (12.6%), undifferentiated ca. 7 (3.4%), metastatic ca. 4 (1.9%), medullary ca. 3 (1.4%), lymphoma 2 (1.0%). Of these, after examining four metastatic carcinoma, about the primary site, kidney (clear cell ca.) was 2 cases, and skin (malignant melanoma) and pulmonary (small cell ca.) were by one case, respectively. We report the clinical course or treatment (chemotherapy and surgery) about metastases to thyroid case of the small cell lung ca. in detail.
The patient had a diagnosis of small cell lung cancer at 59 years old time and was treated with standard procedure and recovered completely and followed up severely afterward. But it became clear on various kinds of testing that the cancer metastasized to thyroid gland approximately four years after initial treatment. We performed total thyroidectomy after 3 course of chemotherapy (CDDP+CPT-11). As a result of having examined the specimen which we resected by surgery, we thought that the preoperative chemotherapy was not effective and changed the regimen to AMR (Amrubicin Hydrochloride), and 6 courses performed afterward.
We experienced the case that very rare small cell lung cancer (LD) metastasized to thyroid gland. PET-CT and tumor marker pro-GRP were particularly useful for a diagnosis. As combined modality therapy, we performed total thyroidectomy in an interval of the chemotherapy. We review a regimen of the adjuvant chemotherapy by evaluating the specimen which we resected by surgery and are following it up severely now.
Thyroid & Development Saturday Poster Clinical
Graves' disease (GD) contains subtypes caused by different major susceptible genes or different variants of one susceptible gene. Here, we investigate whether the PTPN22 is the susceptibility gene of GD in Chinese population and further determine the susceptibility variant of GD in PTPN22.
We conducted an imputation analysis based on our results of the genome wide association study (GWAS) in 1,536 GD patients and 1,516 control subjects. We found that 255 common SNPs on a linkage disequilibrium (LD) block containing PTPN22 were associated with GD (P<0.05). Nine tagSNPs were selected to be further genotyped in a large cohort including 4,368 GD patients and 4,350 matched controls.
There was no significant difference of the nine tagSNPs (P>0.05) in either the genotype distribution or allelic frequencies between patients and controls in the replication study. Although the combined analysis exhibited weak association signal (Pcombined=0.003263 for rs3811021), the FPRP analysis indicated it was most likely a false-positive finding.
Our study did not support an association of common SNPs on PTPN22 LD block with GD in Chinese Han population. It is suggested that GD in different ethnic population probably caused by distinct susceptible gene.
Thyroid Hormone Action Saturday Poster Basic
Mesenchymal stem cells (MSCs) are actively recruited into the tumour stroma, where they differentiate into carcinoma-associated fibroblast (CAF)/pericyte-like cells, thereby forming the tumour's fibrovascular network. There is growing evidence that thyroid hormones T3 and T4 play a critical role in the formation of the stroma by stimulation of angiogenesis, proliferation and inflammation - effects that are mediated through non-genomic mechanisms via the integrin αvβ3. Tetrac, a T4 derivative, is an inhibitor of thyroid hormone action at the integrin site. To improve the understanding of the mechanisms behind MSC differentiation and the effects of thyroid hormones on tumour stroma formation, we examined the effects of T3, T4 and tetrac on MSC biology in vitro.
Here, immortalised human bone marrow derived CD34- MSCs were grown in HCC cell-conditioned medium supplemented with T3 or T4 with or without tetrac for 30 days. Changes in expression levels of genes associated with CAF/pericyte-like differentiation were analysed by quantitative real time PCR.
Most striking changes in gene expression levels were observed for ACTA2, which is associated with neovascularisation, and MMP3, a gene indicative of tissue remodelling and invasion. MSCs treated with tumour cell-conditioned medium alone showed a 30-fold increase in ACTA2 expression and an over 100-fold increase in MMP3 expression compared to untreated cells. Cells treated with a combination of T4 and tetrac showed an additional increase in RNA levels of up to 12-fold for ACTA2 and up to 40-fold for MMP3 compared to cells treated with HCC cell-conditioned medium alone. Treatment with T3 showed comparable effects. Expression levels of other genes such as VEGF and TSP1 were also affected, albeit to a lower extent. So far no inhibitory effect of tetrac on T3/T4-stimulated MSC differentiation was seen.
Our preliminary data suggest that T3 and T4 act on the expression of MSC genes associated with angiogenesis and tissue remodelling/invasion. These studies will increase our understanding of the mechanisms that regulate MSC differentiation as a critical part of tumour stroma formation and for utilisation of MSCs as gene delivery vehicles. AMM and KAS contributed equally.
Thyroid Hormone Action Saturday Poster Basic
Chronic β-adrenergic stimulation (cAMP/PKA/CREB/CRE pathway) induces acquisition of the neuroendocrine phenotype in prostate cancer cells. Neuroendocrine tumors are poorly proliferative but highly invasive. Studies in athymic mice inoculated with LNCaP cells (human prostate cancer line) show that T3 treatment (2.5 μg/day for 6 weeks) prevents the CRE-dependent gene expression associated with tumor progression (VEGF, MMP-9, uPA, and chromogranin A) induced by β-adrenergic activation (isoproterenol [ISO], 200 μg/day) (ATA 2012, Abs A-112). The aims of this study were to assess if T3 prevents acquisition of the neuroendocrine phenotype and if the inhibition of CREB phosphorylation (pCREB) could be involved in this protection.
LNCaP cells were treated for 6 days with vehicle or 50 μM ISO or 10 nM T3 or ISO+T3. Neuroendocrine morphology (number and length of neurite processes) was evaluated by phase-contrast microscopy. Cell migration was measured with a transwell assay, and the pCREB/CREB ratio was determined by immunoblotting.
As expected, ISO alone increased the number and length of neurite processes (60–70%), cell migration (80%), and the p-CREB/CREB ratio (200%) in comparison with the control group. T3 alone did not modify any of these parameters, but in the combined group, neuritic outgrowth and cell migration were prevented. This group (ISO+T3) showed a pCREB/CREB ratio lower than ISO, but higher than T3.
Together, these data suggest that T3 prevents acquisition of the neuroendocrine phenotype induced by β-adrenergic stimulation. The partial reduction of the CREBp/CREB ratio by T3 suggests that more than one mechanism is involved in the inhibition of β-adrenergic signaling.
Thyroid Hormone Action Saturday Poster Basic
During the last decade 3,5-Diiodothyronine (3,5-T2) emerged from a negligible T4 metabolite to a thyroid hormone with its own mode of action distinct from that of the main thyromimetic hormone T3 which controls the hypothalamus-pituitary-thyroid axis. In animal experiments 3,5-T2 rapidly stimulates basal metabolic rate, prevents obesity in rodents on high-fat died and increases oxidation of long-chain fatty acids. These TR-independent direct actions occur devoid of thyrotoxic side effects on the heart or the CNS typically accompanying T3 administration.
A recently developed immunoassay allowed the measurement of 3,5-T2 concentrations in 1000 participants of the Study of Health in Pomerania-TREND (SHIP-TREND) cohort. After the exclusion of participants taking thyroid medications or showing a TSH-level outside the reference range (0.25 – 2.12 mU/l), 685 subjects were included in the descriptive analyses.
The median and mean of the 3,5-T2 serum level was 0.24 nM (1st quartile: 0.2 nM; 3rd quartile: 0.38 nM) and 0.33 nM (standard deviation:±0.26 nM), respectively, indicating a right-skewed distribution. Accordingly, we analyzed the influence of age, sex and smoking by group models, which revealed no difference in sex and smoking but a slight positive trend of increasing serum levels in older age. Based on a classification of 3,5-T2 values into three nearly equivalent in size groups, positive correlations with serum glucose levels became obvious (p=0.01). Moreover, a highly significant positive association with the Waist-to-height ratio was observed (p=0.003). However, the content of subcutaneous as well as visceral fat, measured by whole body MRI, showed no significant associations. Taken together, our findings suggest an relevant role of circulating 3,5-T2 in glucose metabolism as well as body constitution, the latter in sense of fat storage, which is partly in conflict with the outcome of pharmacological interventions in rodent models.
Taken together, our findings suggest a relevant role of circulating 3,5-T2 in human body fat metabolism which is partly in conflict with the outcome of pharmacological interventions in rodent models.
Thyroid Hormone Action Saturday Poster Clinical
Data on the association between subclinical thyroid dysfunction and the risk for fracture are conflicting. Purpose of this study is to summarize prospective evidence about the relationship between subclinical thyroid dysfunction and declined of bone mineral density (BMD) and the risk of fracture.
Systematic review of MEDLINE, EMBASE, CCTR and Chinese Biomedical literature database from 1974 to December 2012. Two views cohort studies in which thyroid function was measured and then followed up patients prospectively to assess fracture or altering of BMD.
Three identified studies involved population-based cohorts the included 32685 participants, subjects included both patients who took thyroid-altering medications and endogenous subclinical thyroid dysfunction, which assess fracture in population. All 3 prospectively studies examined risk associated with subclinical hyperthyroidism, whereas 2 prospectively study examined risk associated with subclinical hypothyroidism. In a fixed-effects model, the Risk Ratio (RR) for subclinical hyperthyroidism for fracture was 1.52 (95% CI, 1.33 to 1.73; P for heterogeneity=0.27). Risk estimates were lower when just higher-quality studies were analysed (RR=1.35, 95% CI 1.12- 1.63); the RR was 1.30 (95% CI, 1.08 to 1.56; P for heterogeneity=0.13) for subclinical hypothyroidism. Whereas, consequence of the only higher-quality study analysed was conflicting (RR=1.36, 95%CI 1.11–1.36). The RR was 1.36 (95%CI 1.11–1.36) for endogenous subclinical hyperthyroidism, 1.66 (95%CI 1.40–1.96) for exogenous subclinical hyperthyroidism, 1.02 (95%CI 0.76–1.38) for endogenous subclinical hypothyroidism and 1.53 (95%CI 1.20–1.94) for exogenous subclinical hypothyroidism.
Despite heterogeneity across studies, data suggest the subclinical hyperthyroidism and subclinical hypothyroidism, which included both endogenous and drug-induced exogenous dysfunction, may be associated with an increase risk for fracture in population, with lower risk estimates when analysis higher-quality studies. The risk was higher in exogenous subclinical thyroid dysfunction than in endogenous subclinical thyroid dysfunction.

Forest plots for Subclinical Hyperthyroidism
Thyroid Hormone Metabolism & Regulation Saturday Poster Basic
Thyroid hormones have an essential role in skeletal development and the maintenance of adult bone structure. Thyroid diseases, e.g. thyrotoxicosis, are known to affect the equilibrium between bone resorption and deposition. Recently, it has been shown that TSH may play a role in bone metabolism and homeostasis but the mechanisms have not yet been fully elucidated.
To study TSH-mediated effects in bone we generated a human osteosarcoma U2OS cell line, which has characteristics of bone precursor cells, stably expressing TSH receptor (TSHR). We used TSH and the small-molecule TSH receptor agonist C2 (NCGC00161870) to test their effects on protein kinase phosphorylation/activation by ELISA and on bone-specific gene expression by qRT-PCR. The PathHunter™ beta-Arrestin Assay (DiscoveRx) was used to show translocation of β-arrestin 1 or 2. siRNA silencing of β-arrestin 1 or 2 was utilized to test their individual role in differentiated gene expression.
We showed that TSH activated the recruitment of β-arrestin 1 and 2 to the TSHR whereas C2 had no effect. TSH up-regulated the osteoblast markers RANKL, osteopontin (OPN), ALPL, IL6, and IL11 while it down-regulated the osteoclast marker TRAP. The C2 effect on TRAP down-regulation was identical to TSH. ALPL and OPN up-regulation by C2 was comparable to that of TSH, but with different kinetics. IL6 and IL11 up-regulation was, at least in part independent of β-arrestins. Importantly, C2 failed to have an effect on RANKL expression. We hypothesized that β-arrestin signaling could be essential for TSH-mediated changes in bone-specific gene expression. We found that up-regulation by TSH of OPN, IL6, IL11, RANKL, and ALPL was impaired by β-arrestin 1 knockdown, but not β-arrestin 2 knockdown.
TSH regulates bone-specific gene expression in U2OS-TSHR cells that directs cells towards an osteoblast and not an osteoclast phenotype. These effects of TSH are mediated in part by β-arrestins, and β-arrestin 1 is the key player.
Thyroid Hormone Metabolism & Regulation Saturday Poster Basic
Thyroid hormone (TH) stimulates the expression and activity of glycolytic and oxidative enzymes, accelerates the metabolism of glucose, which reduces the intracellular glucose concentration and generates a gradient that favors the entry to glucose into the cells. These actions demonstrate the importance of TH in the regulation of glucose homeostasis. Hyperthyroidism increases the glycogenolysis and gluconeogenesis with the consequent development of glucose intolerance, while increases the metabolic rate promoting weight loss, which improves insulin sensitivity. The set of data presented shows that some actions of TH contribute to the maintenance of glucose homeostasis unlike other actions that compromise it. This study aimed to investigate the effect of chronic treatment with T3 on glucose homeostasis in diabetic rats. For this we evaluated: the insulin tolerance test (KITT), blood glucose, and hepatic glucose production.
Adult Male Wistar rats were divided into control, diabetic, and diabetic treated with T3 (1.5 ug/100 g BW) groups for four weeks. Diabetes was induced by injecting the rats intraperitoneally with alloxan monohydrate (150 mg/kg) dissolved in 0.05 mol/L citrate buffer saline solution at a single dose. Animals showing fasting blood glucose levels greater than 250 mg/dl were selected for the study. After treatment, we measured blood glucose, insulin sensitivity by insulin tolerance test (KITT), and hepatic glucose production, which was evaluated by liver perfusion with glycerol or lactate (2 mM).
Diabetic rats treated with T3 showed a reduction of blood glucose and improved insulin sensitivity in relation to the untreated group. Moreover, hepatic glucose production, after liver perfusion with glycerol or lactate, was decreased in diabetic animals treated with T3.
Our results suggest that T3 decreases hepatic glucose output lowering plasma glucose levels thus improving insulin sensitivity. Although the use of T3 as a therapeutic agent is quite unfeasible, identifying the molecular mechanisms by which it acts could lead to the development of specific agonists or antagonists as potential therapeutic agents. Fapesp 2010/18151-7.
Thyroid Hormone Metabolism & Regulation Saturday Poster Clinical
Agranulocytosis is one of the serious adverse effects of antithyroid drug (ATD) and mainly develops within 3 months of continuous ATD intake periods. Agranulocytosis can also develop in patients when ATD is resumed, even though they were previously treated with the same ATD without developing agranulocytosis. However, little is known about agranulocytosis that develops beyond the initial course. We investigated the characteristics of patients who developed agranulocytosis during their second or later course of ATD treatment.
A total of 81 patients were diagnosed with ATD-induced agranulocytosis between 1983 and 2012 at our hospital, of which 14 patients (MMI10, PTU4) that developed agranulocytosis for the first time in the second or later course of ATD treatment were designated the “resumed group”. Thirty five patients (MMI28, PTU 7) that developed the disease during their first uninterrupted course of ATD therapy were designated the “first group”.
The median total duration of ATD therapy until diagnosis of agranulocytosis was 559 (range, 86–1775) days, and the median length of the interval between the final administration in the previous course and the first day of the course in which agranulocytosis was diagnosed was 916.5 (153–8110) days. Interestingly, there were no cases which developed agranulocytosis never developed when treatment with an ATD was resumed after discontinuation period of for less than 5 months. There were no significant differences between the first and the resumed group in the interval between the start of ATD therapy in the course in which agranulocytosis was diagnosed and the diagnosis of agranulocytosis (39 (20–98) days in the first group and 32.5 (21–95) days in the resumed group (N.S.)).
When ATD treatment is resumed using the same drug, especially after a discontinuation period of more than five months, patient follow-up is vital in order to detect risks of developing agranulocytosis regardless of initial or further treatment.
Thyroid Hormone Metabolism & Regulation Saturday Poster Clinical
We assessed predictors of recurrence of Graves' disease(GD) after discontinuing an antithyroid drug (ATD) or potassium iodide (KI).
The subjects were 326 patients who diagnosed new-onset GD from April 2006 to June 2007 and discontinued medical treatment after maintenance dose. The male-female ratio was 1:4.7, and median age was 40 years (range: 9–77). Treatment consisted of methimazole (MMI) in 252 cases, propylthiouracil (PTU) in 49 cases and KI in 25 cases. Of 326 patients, 117 patients experienced a recurrence (group A) and 209 patients were in remission (group B). Age, gender difference, thyroid function, TSH-binding inhibitory immunoglobulin (TBII) and sonographically measured thyroid weight (TW) at the time of first visit and drug discontinuation were analyzed between the two groups. The duration of treatment was 2.08 years (0.1–5.37), and the follow-up period after discontinuation was 3.53±0.92 years.
Age at the first visit was 39 years (12–77) in group A vs. 41 years (9–74) in groupB. Factors at the time of drug discontinuation in group A and group B were as follows; F-T3 3.0 pg/ml (1.7–4.2) vs. 2.9 pg/ml (1.0–4.0), F-T4 1.26 ng/dl (0.64–1.57) vs. 1.26 ng/dl (0.2–1.91), TSH 1.22 μIU/ml (0.01–16.1) vs. 1.36 μIU/ml (0.01–138.6), TBII 1.3 IU/l (0.3–40) vs. 0.9 IU/l (0.3–6.7) and TW 24.7 g (11.9–129.1) vs. 23.0 g (10.0–53). TSH and TBII were significantly different between two groups (both P<0.05). The duration until the dosage was reduced to maintenance dose was 10.5 months (1.25–50.5) in group A vs. 8.2 months (0.9–38.2) in group B, and was significantly longer in the recurrence group. The maintenance dose period was 9.5 months (0.4–25.5) in group A vs. 10.1 months (1.2–39.3) in group B, and the difference was not significant. The recurrence ratio classified by TBII at the time of drug discontinuation was 29% in the group with TBII<1.2 IU/l vs. 47.9% in the group with TBII≧1.2 IU/l. The recurrence ratio classified by TSH at the time of drug discontinuation was 41.2% in the group with TSH<2.0 μIU/ml vs. 25.5% in the group with TSH ≧2.0 μIU/ml.
It suggested that the TBII and TSH values at the time of drug discontinuation would be the predictor of recurrence of Graves' disease.
Thyroid Imaging Saturday Poster Basic
Synchrotron radiation(SR) provides highly collimated and powerful beams with linear polarization and makes it possible to show the internal structures of biological soft tissues with high spatial resolution under low radiation dose and may offer greatly enhanced image quality over conventional imaging techniques. The aims of this study were to estimate the visualization of the human thyroid tissue with SR micro-CT and to compare the results with histopathological examinations.
The normal human thyroid tissue samples were routinely fixed in 10% neutral buffered formalin, processed and embedded in paraffin, and each specimen was cut down to a cylindrical sample with 2 mm diameter and 11 mm height. Experiments were performed at the bending magnet beamline 6D of Pohang Light Source in Pohang Accelerator Laboratory, Korea. The white beam imaging system developed for synchrotron tomography consists of a 1 mm Si attenuator, 100 μm-thick CdWO4 scintillator and a full-frame charge-coupled device camera (CCD camera; Vieworks 2M; United Digital Device, Seoul, Korea). Phase contrast technique was applied. Detector was placed 23 cm downstream from the sample on an optical table which could be rotated in a vertical axis. For tomography 1,000 images were collected at 0.18° increments through 180°. The visual image was magnified using a X20 microscope objective and captured using a digital CCD camera. The pixel size was 0.45 μm. After imaging, the samples were split into many 5 μm thick sections for hematoxylin-eosin staining. Obtained tomography images were compared with corresponding histopathological findings in optical microscopy.
Synchrotron tomography images yielded high contrast from smoothly varying internal structures corresponding to information on actual structures seen at histopathological analysis.
3-dimensional micro-tomography has excellent visualization of subject contrast, together with depth localization, so it is useful for showing 3-dimensional anatomical structures of thyroid gland. This results suggest that tomography with SR has a great potential as a diagnostic tool, and also its clinical and laboratory application is feasible
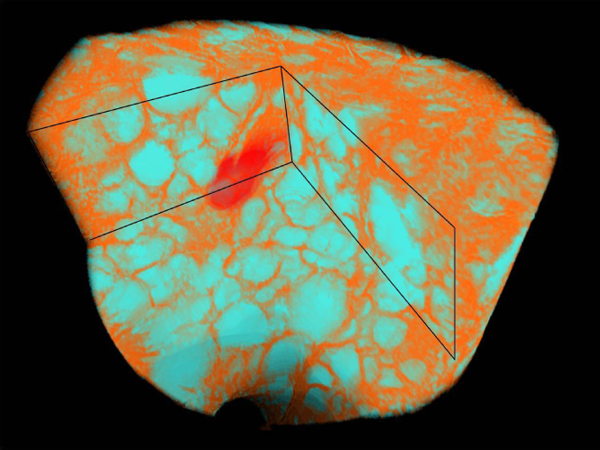
Reconstructed 3-dimensional image of normal thyroid tissues showed variable sized follicles encircled by thin layer of the epithelial lining cells, blood vessels and connective tissues in tomogram.
Thyroid Imaging Saturday Poster Clinical
The purpose of our study is to compare the effectiveness of PLA and RFA procedures in the treatment of benign thyroid nodules discussing indications, techniques, complication and outcomes derived from our experience.
33 patients (24 F; 57±17) with benign thyroid nodules were treated, 13 with PLA and 20 with RF. Nodules were classified as thy2 through two consecutive fine-needle-aspiration(FNA) and selected for their clinical implications due to their volume. All of them presented a solid component of over 80% of its total volume, assessed by pre-treatment US evaluation. Right after the ablation procedure, treated nodules were evaluated with a contrast-enhanced ultrasonographic (CEUS) examination in order to assess the area of necrosis. Then patients were followed-up at 1 week with US, at 1 month with CEUS, at 6 and 12 months with US in order to assess nodule's volume reduction and treatment outcomes.
Reduction in nodules volume after RFA has been found to range 27–53% at 1 month follow-up and 55–84% at 12 months; PLA resulted in a nodule's volume reduction of 25–45% at 1 month and 53- 76% range at 12 months. No significant differences has resulted between the two techniques in terms of nodule's volume reduction. No procedural complications occurred.
RFA and PLA are excellent and safe procedures in the management of benign thyroid nodules. Safety represents the primary treatment prerogative, hence the clinical presentation and the radiologist skills should play an important role in the procedure planning; our experience suggested that the choice between RFA and PLA could be made on the basis of where the nodule is sited and on its morphologic features, preferring RFA for more superficial and irregular-shaped nodules and PLA for deeper and plongeant ones.
Thyroid Imaging Saturday Poster Clinical
Our purpose was to evaluate the safety and effectiveness of a virtual needle tracking system for US-guided percutaneous RFA of benign thyroid nodules(BTN) as compared to standard RFA.
A STARmed (Korea) 18G bipolar RF electrode was used to perform the BTN ablation procedures. A US machine (LOGIQ E9, GE Healthcare) with a low magnetic field generator was used; electromagnetic sensors, calculating their mutual position, were set on the US probe and on the needle bottom (VirtuTRAX, CIVCO); the system shows the expected path of the needle and its tip position. US-guided RFA were made with a in-plane approach on 17 patients (13 F; 54±11) with BTN, randomized in two groups: 10 (group A) were treated with RFA using the Virtual Tracker, 7 (group B) without it. A contrast-enhanced US follow-up was performed after 1 week in order to have a precise assessment of the area of necrosis in each patient.
In all 17 cases a wide area of nodule ablation was safely obtained. The positioning system accurately guided the needle tip inside the target and allowed for a correct treatment of the lesions with RF. A significant increase of the area of necrosis after RFA was found in group A compared to group B (p<0.01). No periprocedural complications occured.
The Virtual tracker allows to easily perform nodules RFA with US-guided approach, providing the clear visualization of the virtual needle tip and shaft, even if the real needle is not visible due to the ablation artifact. The excellent level of safety provided by the Virtual Tracker allows to perform RFA with high confidence achieving a shortening of the learning curve and granting a significant increase in the nodule area of ablation.
Thyroid Imaging Saturday Poster Clinical
Adhesion between recurrent laryngeal nerve (RLN) and thyroid cancer makes it difficult to dissection of RLN during thyroid surgery, so the risk of injury to RLN could be increased. Sometimes preoperative imaging studies could help to predict the relation between RLN and tumor before surgery, but the exact findings are not known. We investigated this study to evaluate ultrasonography (USG) findings related to RLN status and to evaluate effect of duration of surgery related to RLN invasion.
Among the patients underwent thyroid surgery for papillary thyroid cancer (PTC) in Asan Medical Center from July 2012 to April 2013, we included the cases that cancers are close to posterior aspect of thyroid gland or tracheal wall on preoperative USG. We divided these patients to two groups, no abutting group (close to posterior aspect of thyroid gland or tracheal wall, but no evidence of invasion) and abutting or protruding group (having suspicious findings of invasion). We compared the preoperative USG and intraoperative findings between these groups.
42 patients who underwent thyroid surgery for PTC were included. In preoperative USG findings, 11 patients (26.2%) were classified as no abutting group and 31 patients (73.8%) were classified as abutting or protruding group. In intraoperative findings, 14 patients (33.3%) showed adhesion between RLN and thyroid cancer and 28 patients (66.7%) showed no adhesion. Among these patients, 22 patients underwent surgery within 6 months after diagnosis and 20 patients underwent surgery over 6 months after diagnosis. When we compared two groups that were divided by preoperative USG findings, there was no significant difference in tumor size, distance from trachea in preoperative USG, proportion of RLN adhesion. The duration of surgery from diagnosis did not influence to the proportion of RLN adhesion (p=0.66). When we evaluated the patients who had more than 6 months of duration of surgery after diagnosis (n=20), preoperative USG findings had no relation to intraoperative finding of RLN status (p=0.64).
It is difficult to predict adhesion between tumor and RLN only through pre-operative USG. The duration of surgery from diagnosis seems to have little effect on tumor adhesion to RLN.
Thyroid Nodules & Goiter Saturday Poster
Acromegalic patients have a higher prevalence of thyroid disorders, particularly of non-toxic nodular goiter and carcinoma. Studies have reported association between the gland volume and duration or disease activity. Sustained exposure to IGF-1 appears to play an important role in the increased size of the gland and development of cancer in these patients. The thyroid tissue expressed both GH and IGF-1 receptors, establishing possible local autocrine and paracrine actions. The synergistic effect of the interaction TSH/IGF-, is well recognized. The purpose of our study was to evaluate the function and morphology of the thyroid in patients with acromegaly referred to the Department of Endocrinology, Hospital Vargas in Caracas- Venezuela. Specific Objectives: Determine the function of the thyroid. Set a personal and / or family history of thyroid disease. Describe the structure of the thyroid: volume, ultrasound echogenicity and presence or not of nodules.
Observational and descriptive trial. TSH levels, free T4, antiperoxidase autoantibodies, anti-thyroglobulin, basal insulin, GH and IGF-1 fasting and post-glucose load were measured in a series of 10 patients with Acromegaly. Were classified into 2 groups: active disease (n=7) vs. inactive (n=3), according to standardized criteria. Thyroid U.S. was performed with Doppler effect, by the same operator and equipment. FNA was performed for solid or mixed lesions greater than 1 cm or suspicious for malignancy.
90% of patients had normal TSH. 20% had positive antiperoxidasa autoantibodies, one of which (10%) had associated hypofunction and ultrasound suggestive of chronic thyroiditis. 80% had normal free T4. The prevalence of goiter (volume >16 cc) was 50%. 60% had nodules.
Like others our study showed that thyroid function in acromegaly is predominantly normal while its structure is altered by the presence of nodules.
Thyroid Nodules & Goiter Saturday Poster Clinical
Familial adenomatous polyposis (FAP) is a hereditary colon cancer syndrome that can involve multiple extracolonic organs, including the thyroid. While several studies have estimated that thyroid cancer (TC) in FAP occurs at 5× the rate of the general population, little is known about the prevalence of benign thyroid disease. Our study seeks to define the features of FAP-associated benign thyroid disease and propose screening and surveillance recommendations.
Prospective screening for early thyroid cancer detection with thyroid ultrasound (US) was performed on FAP patients at the time of annual colonoscopy since November 2008. We reviewed clinical and ultrasound (US) data to characterize the prevalence and nature of thyroid nodules.
205 patients (mean age 42, 55% female) underwent 404 screening US exams during a surveillance period of 4 years (11/2008-11/2012). At least one thyroid nodule was detected in 106 (51.7%) patients, with 90% of these seen on initial exam. 40/106 (37.7%) patients required fine needle aspiration biopsy of a dominant nodule (mean size 14 mm), and 28/40 (70%) of these were performed at first ultrasound visit. Suspicious US features were present in 16/40 (40%) patients, including 5 with sub-centimeter nodules. Cytology was abnormal in 14/205 screened patients, leading to surgery and revealing 13 papillary TC and 1 medullary (6.8%). Non-diagnostic cytology in 2/40 (5%) patients was found to be benign on subsequent follow-up. Of 99 patients without initial thyroid pathology, and 26 with benign cytology, subsequent US surveillance detected no further disease.
Given the age and gender distribution of our screened cohort, our study reveals a higher-than-expected prevalence of both benign and malignant thyroid disease in the FAP population. The initial US was responsible for 90% of detected nodules and 70% of biopsies, with the remainder detected/biopsied on follow-up examination. Although no standardized guidelines exist, given the increased prevalence of both benign and malignant thyroid nodules, we recommend baseline and subsequent ultrasound surveillance in all FAP patients.
Thyroid Nodules & Goiter Saturday Poster Clinical
Thyroid nodules are common. The current standard of diagnosis, ultrasound guided fine needle aspiration biopsy (FNAB) yields insufficient results between 5–10% of the time, necessitating a repeat biopsy or surgery for diagnosis. Elastic scattering spectroscopy (ESS) is a minimally invasive optical-biopsy technique that we have adapted for use in the clinic by miniaturizing it to fit through a 23 gauge needle. We hypothesized that ESS in vivo can reduce our insufficiency rate.
Under an IRB approved protocol, patients receiving a FNAB had ESS data collected using our ESS integrated biopsy probe, then up to 5 subsequent and separate passes with a standard 23 gauge needle. Insufficiency rates and causes were compared between all needle passes.
122 patients were enrolled and had data available for analysis. Only 2.5% had an insufficient biopsy when performing the biopsy with the ESS probe, compared to 10% with a standard needle.
A clinical trial using an integrated ESS/biopsy probe in vivo is feasible and acceptable to patients. Both spectral data and cytologic material are adequate in the majority of patients. The real-time feedback provided by ESS may significantly increase the likelihood of material adequacy. With further accrual and analysis, this ESS device may establish standardized criteria for adequate FNAB specimens.
Thyroid Nodules & Goiter Saturday Poster Clinical
Functional autonomy is part of the natural history of multinodular goitre, it is often occult and sometimes associated to TSH value in the low-normal range. So far, autonomous functioning thyroid areas (AFTA) may remain a hidden problem thus exposing patients to heart arrhythmias. By using an individually tailored dose (ITD) of thyroxine (T4) in the treatment of nodular goitre, a serum TSH lower than expected may be recorded. This finding may be attributable to the presence of AFTA. This study was aimed at characterizing the presence of occult autonomous functioning areas in the thyroid of patients hyperresponding to treatment with an ITD of thyroxine.
In a cohort of about 3000 consecutively examined outpatients, we assessed 94 patients (84 F and 10 M; median age=56 years) with multinodular goitre in treatment with ITD, who showed an unexpected lower serum TSH as compared to the one observed in a reference group (n=123; 109 F and 14 M; median age=54 years) in whom iodine and drug interferences, as well as autonomous functioning areas, were positively excluded.
Patients of the study group showed significantly lower median TSH (0.052 vs 0.20 mU/l, p<0.0001), despite a significantly lower dose administered (1.19 vs 1.49 μg/Kg/day, p<0.0001). When analyzed according to age, these differences were confirmed both in adult patients <60 years (median TSH: 0.06 vs 0.2 mU/l, p<0.0001; median T4 dose: 1.29 vs 1.56 μg/Kg/day, p<0.0001) and in older patients >60 years (median TSH: 0.05 vs 0.22 mU/l, p<0.0025; median T4 dose: 0.94 vs 1.33 μg/Kg/day, p<0.0005). Interestingly, when treatment was withdrawn, 86/94 patients (91.5%) had serum TSH in the normal range and the median TSH of the whole study group was 1.09 mU/l. All these patients underwent thyroid scintiscan and radioactive iodine uptake test (RAIU- 4th and 24th hour). The presence of autonomous functioning areas has been detected in 65 out of 94 patients (69%). RAIU at 4th hour (17 vs 13%, p<0.0199) and 24th hour (33.5 vs 28%, p<0.001) were both significantly higher in patients with AFTA.
These results show that T4 treatment, when individually tailored dose approach is used, represents a novel tool to detect hidden autonomous functioning thyroid areas.
Thyroid Nodules & Goiter Saturday Poster Clinical
Fine-needle aspiration (FNA) is considered the gold standard diagnostic tool in thyroid nodule evaluation.
We describe four cases where cytopathology results suggested thyroidal origin but further evaluation revealed non-thyroid pathology.
Case 1 is a 49 year old female with history of papillary thyroid cancer (PTC) resected in toto in 2005. Eight years later surveillance ultrasound revealed a 14 mm left sided thyroid bed nodule but undetectable serum thyroglobulin. FNA of this nodule was interpreted as “suspicious for follicular neoplasm.” Surgical excision revealed this mass to be a hyperplastic parathyroid gland. The patient's pre-operative calcium was 9.5 mg/dl. Case 2 is a 66 year old female found to have a right sided 25 mm thyroid nodule on ultrasound. FNA of this nodule was reported as follicular lesion of undetermined significance (FLUS) but Afirma® Gene Expression Classifier found it to be genetically similar to parathyroid tissue. Biochemical workup confirmed hyperparathyroidism. Case 3 is a 67 year old female found to have a 9 mm suspicious appearing nodule on ultrasound that was reported as FLUS on FNA. Afirma® Gene Expression Classifier revealed that the sample was genetically similar to parathyroid tissue and the patient was found to have mild biochemical hyperparathyroidism. Case 4 is a 63 year old male with Grave's disease who was found to have a suspicious right sided 14 mm thyroid nodule and a suspicious left sided 15 mm level 2 lymph node on ultrasound. FNA reported PTC in the thyroid nodule and “suspicious for PTC” in the lymph node. Surgical pathology confirmed PTC in the right thyroid nodule, however the left lymph node was a pleomorphic adenoma. The patient had a pleomorphic adenoma resected 20 years ago.
FNA is an important tool in risk stratification of thyroid nodules and helps determine the appropriate need for surgery. We describe four cases where FNA misdiagnosed thyroid pathology. Careful evaluation to rule out parathyroid disease and utilization of thyroglobulin or PTH wash or stain where appropriate would be useful.
Autoimmunity Saturday Poster Case Report
Hyperthyroidism occurs in 3–8% patients of myasthenia gravis. Hypothyroidism with myasthenia is even rarer. There are very few reports of isolated ocular myasthenia with thyroid associated ophthalmopathy (TAO) in Graves' disease. We report a case of TAO with ocular myasthenia as the presenting symptom of primary hypothyroidism. As per our knowledge such an association of TAO with ocular myasthenia in primary hypothyroidism has not been reported before.
A 52 year lady i) presented with grittiness, redness, watering and pain in both eyes, with bilateral proptosis for 10 months ii) and noticed drooping of the right eye for 2 months without weakness of the bulbar, neck and limb muscles. There was no history of weight loss, heat intolerance and tremulousness. She had a firm grade 1b goiter, bilateral proptosis (right eye 23 mm and left eye 26 mm) with a clinical activity score of 1/6, and drooping of the right eyelid.
Investigations revealed - Low free T4- 0.8 ng/dl (normal: 0.9–1.8 ng/dl) - Elevated TSH- 38 μU/ml (normal: 0.4–4.2μU/ml) - Positive anti-thyroid peroxidase antibody- 189 IU/ml (normal <35 IU/ml) - Positive anti-acetylcholine receptor antibody- 2.32 nmol/L (normal <0.5 nmol/L) - Repetitive nerve stimulation test of bilateral nasalis muscle was suggestive of ocular myasthenia. - Electrodiagnostic studies of the limbs were normal. - Computerized Tomography (CT) of orbits revealed extraocular muscle thickening and expansion of the retro-orbital fibro-fatty tissue suggestive of thyroid associated ophthalmopathy (TAO). - CT scan of the thorax was normal - A diagnosis of Primary Autoimmune Hypothyroidism with Thyroid Associated Ophthalmopathy with Ocular Myasthenia was made - 3 months after diagnosis, ptosis improved with Pyridostigmine (60 mg 4 times daily) and Levothyroxine (75 μg/day) therapy.
Any patient of TAO with ptosis should be evaluated for ocular myasthenia. This case aims to highlight that TAO and ocular myasthenia can co-exist with primary hypothyroidism and could be a diagnostic challenge. Failure to achieve euthyroid status can worsen both TAO and myasthenia.

Photograph of the patient showing bilateral proptosis (left > right) with right eye ptosis
Disorders of Thyroid Function Saturday Poster Case Report
Painless subacute (giant cell) thyroiditis is rare and only 8 patients have been reported in Japanese literatures since 1992. Three cases of the disease seen in these 3 years are reported.
Case 1. A 45-year-old man presented a focus of intense tracer uptake in the right thyroid lobe on F-18-FDG-PET/CT in March, 2010. He had a non-tender nodule and ultrasound showed a 26 mm hypoechoic area in the right thyroid. Case 2. A 63-year-old woman with multi-nodular goiter presented a new hard, non-tender nodule and ultrasound demonstrated a 24 mm hypoechoic area in the left upper part in July, 2012,. Case 3. A 61-year-old woman presented a nodule in the left thyroid lobe in December 2012. Ultrasound revealed a 5 mm hypoechoic nodule in the contralateral, right lobe in April 2013. It was speculated to be an inflammatory lesion based on our experiences of Cases 1 and 2.
In all cases, the histological diagnosis of subacute thyroiditis was made by needle core biopsy, however, aspiration cytology was not pathognomonic. Throughout the observed periods, all patients presented neither thyroid pain nor fever. C-reactive protein was normal. Thyroid function tests were normal with negative for autoantibodies for thyroglobulin (Tg) and thyroperoidase except Case 1. He had been euthyroid with transient suppression of TSH and transient increase of TgAb in July. Tg concentrations were mildly increased in Cases 1 and 2. Case 1. Enlargement in size and a new hypoechoic area were observed in the left lobe suggestive of creep upon the left lobe in July. Shrinkage in size of whole thyroid with uniform echogenicity was seen in October. Case 2. The left hypoechoic area was gradually decreased in size and almost disappeared in February, 2013. Case 3. Up to today, she has no complaints of fever nor thyroid pain.
Painless subacute thyroiditis was incidentally found in 3 cases. One of them may be the first case of painless subacute thyroiditis with a focus of less than 10 mm in diameter. It is speculated that there may be more numbers of patients with painless subacute thyroiditis who do not visit hospitals because they do not realize the presence of subacute thyroiditis.
Disorders of Thyroid Function Saturday Poster Case Report
Hypokalemic Periodic Paralysis (HPP) is a rare cause of acute weakness. We present an unusual case of spontaneous HPP associated thyrotoxicosis in a non-Asian patient.
A 25 year old African-American male was evaluated in the emergency room with complete paralysis. He reported gradual development of stiffness and difficulty moving in the morning. Mild weakness began approximately 1 month before initial evaluation and progressed to a point of being completely unable to get up out of bed on admission. Review of systems was noted for moderate palpitations. No changes in diet or activities. He had no other documented medical history. He was taking no medications and had no allergies or recent travel. He used no alcohol and smoked ½ pack of cigarettes per day. Family history was unremarkable.
On presentation, the patient had a normal temperature and stable vital signs but had complete paralysis of his upper and lower extremities. Laboratory data: Potassium 1.5 Meq/L, phosphorus 1.6 Meq/L; all other baseline labs (including renal function, magnesium and glucose) were normal. The patient was started on aggressive IV potassium supplementation with rapid paralysis improvement. His potassium remained stable and he was discharged home after 3 days with a potassium of 4 Meq/L. The following day, the patient had similar symptoms and was readmitted with a potassium of 2.1 Meq/L. Thyroid function tests revealed TSH 0.01 uIU/mL, and a free T4 of 2.65 ng/dL. In addition to further potassium supplementation, the patient was started on Methimazole. Thyroid ultrasound was consistent with thyroiditis. Over the following 2–3 months as thyroid status improved, all muscular symptoms completely resolved.
Thyrotoxic HPP is unusual in North America affecting only 0.1–0.2% of thyrotoxic patients and the reported cases are largely in Caucasians. In contrast, Asian populations have a higher incidence of 1.8–1.9%. The underlying mechanism remains unclear. This is an unusual case occurring in an African-American male unrelated to any familial, dietary or activity changes. This potentially fatal, but curable disorder must be considered in patients presenting with acute weakness.
Thyroid Cancer Saturday Poster Case Report
This is an extremely rare case of a patient with metastatic thyroid carcinoma who remained euthyroid after thyroidectomy and radioiodine therapy. Metastatic lesions were positive on whole body scan without stimulation.
A 76 year old Caucasian male was diagnosed with metastatic follicular thyroid carcinoma on lung nodule biopsy after a chest CT for unrelated reasons showed non-calcified lung nodules which increased in size over the course of a year. Total thyroidectomy was performed with final pathology positive for left 4 cm follicular thyroid carcinoma. He was ablated with 160 mCi of I-131 after thyrogen stimulation. Whole body scan after treatment showed uptake in bilateral lungs, right sacrum and pelvis. The thyroglobulin decreased from 2,063 to 965 four months after treatment but rapidly increased to 2,506 eleven months after I131.
TSH remained suppressed and free T4 remained elevated after I-131 therapy without thyroid hormone supplementation. TSH was 1.2 and diagnostic whole body scan was strongly positive in lungs and pelvis fourteen months after initial I-131 treatment. He was treated with 209 mCi with whole body scan positive in lung and pelvis. Despite I131, new metastatic lesions were noted in the left thyroid bed and a large destructive lesion in C1, four months after the second I131dose. Treatment with an investigational tyrosine kinase inhibitor was begun with greater than 30% response in metastatic lesions and a drop in thyroglobulin. Lesions remain stable 13 months after initiation of tyrosine kinase inhibitor therapy.
Metastatic follicular cancer producing thyroid hormone remains extremely rare with only 47 cases reported from 1946 to 2005 as noted by Tardy et al.1 This case is exceptional because of the disconnect between tumor differentiation and aggressiveness. The metastatic lesions continued to secrete thyroid hormone and remained radioiodine avid despite rapid progression after I-131 therapy.
1. Tardy M, et al. [A case of hyperthyroidism due to functioning metastasis of differentiated thyroid carcinoma. Ann Endocrinol (Paris). 2007 Feb;68(1):39–44.
Thyroid Cancer Saturday Poster Case Report
Graves' disease with concurrent hyperfunctioning nodules is called Marine-Lenhart syndrome (MLS). Hyperfunctioning nodules are generally considered benign with malignancy potential being less than 1%. We present an extremely rare case of MLS in which the hyperfunctioning nodule was malignant.
A 44-year-old female with past medical history of migraines presented with hyperthyroid symptoms of heat intolerance, weight loss of 16 pounds, anxiety, tremulousness, increased sweating and hypomenorrhea. Examination revealed a diffusely enlarged soft goiter with no cervical adenopathy and no signs of Graves' orbitopathy. Biochemical profile showed suppressed TSH, elevated free thyroid hormones and elevated thyroid stimulating immunoglobulins at 313% (normal <140%). Iodine-123 thyroid scan showed elevated uptakes of 35% at 2 hours and 67% at 24 hours with a hyperfunctioning nodule in the right lower pole and minimal suppression of the remainder of the thyroid. A thyroid ultrasound showed diffuse goiter and two nodules in the right lower pole, one measured 1.1 cm with microcalcifications. FNA biopsy of the suspicious nodule revealed papillary thyroid carcinoma (PTC). Following treatment with methimazole, the patient underwent total thyroidectomy with pathology confirming PTC.
Recent studies have found an increased incidence of differentiated thyroid cancers in patients with Graves' disease with higher aggressiveness, poorer prognosis and increased mortality compared with controls. Though later studies reached controversial conclusions, the presence of thyroid nodules in a patient with Graves' disease requires further evaluation to rule out malignancy. The prevalence of thyroid nodules in patients with Graves' disease is nearly as common as in general population and estimated to be around 15%, most of which are cold nodules. Coexistence of autonomously functioning nodules with Graves' disease (MLS) is rare. Malignant hyperfunctioning nodules are also rare. The simultaneous occurrence of MLS and PTC is extremely rare with only 3 cases reported in medical literature.
Malignancy in a hyperfunctioning nodule in Graves' disease, though rare, should be considered.
Thyroid Cancer Saturday Poster Case Report
Paragangliomas of the thyroid gland rarely occur. Their evaluation and diagnosis can prove challenging, often leading to the misdiagnosis of a more common thyroid pathology.
We report the case of a 63-year-old female with a gangliocytic paraganglioma of the right thyroid lobe. We describe the ultrasonographic, histopathologic, and immunohistochemical features in addition to clinical characteristics.
Our patient presented with an incidental finding of a thyroid nodule. Ultrasonography revealed a 2-cm-diameter solid hypoechoic, hypervascular nodule in the right upper pole. Fine needle aspiration cytology suggested a papillary thyroid carcinoma. The patient underwent right thyroid lobectomy. The diagnosis of gangliocytic paraganglioma was made following histologic and immunohistochemical analysis. Neurofilament protein identified ganglion cells and axons coursing through tumor. Synaptophysin and chromogranin marked the chief cells whereas S100 marked the sustentacular cells. The tumor cells were negative for cytokeratin AE1/3, and calcitonin. Thyroglobulin stains were negative in tumor cells as well.
Cytologic, histologic and immunohistochemical features can be used to definitively diagnose paragangliomas of the thyroid. While rare, they do require definitive resection and appropriate post operative genetic evaluation.
Thyroid Hormone Action Saturday Poster Case Report
We describe a case of a 62 year old gentleman with a history of thyroid cancer on excessive doses of liothyronine admitted with new onset atrial fibrillation, new depressed ejection fraction, and cardioembolic stroke.
He has a history of papillary thyroid cancer in 2010, and underwent total thyroidectomy followed by treatment with 103 mCi I131. The patient had forgone traditional surveillance of thyroid cancer. He followed with non-endocrine (anti-aging specialist) physicians who prescribed liothyronine (175 mcg daily, previously 225 mcg), as well as testosterone (50 mcg twice daily), DHEA (25 mg daily) and ioderal (25 mg daily). The patient presented with blurred vision, left arm stiffness, gait disturbance and dysarthria and was diagnosed with right posterior cerebral artery infarct. Within 24 hours of admission, he exhibited atrial flutter/fibrillation with rapid ventricular response. It was thought his stroke was cardioembolic in origin. His workup included an ECHO, which revealed a severely depressed ejection fraction of 25% with global hypokinesis. He has no prior history of arrhythmia, cardiomyopathy or coronary artery disease. He complained of tremor, as well as unintentional weight loss while on this liothyronine dosage. His exam was notable for sinus tachycardia to 120 and fine tremor in his hands, with otherwise normal findings. His thyroid function tests were significant for undetectable T4 levels, undetectable TSH levels, and total T3 202 (94–170) ng/dL. Upon holding liothyronine treatment, which allowed for normalization of his T3, the patient reverted to sinus rhythm. The patient likely developed a tachycardia induced cardiomyopathy secondary to thyrotoxicosis. His new onset atrial flutter/fibrillation was also attributed to his T3-thyrotoxicosis.
To our knowledge, this is the first case reported in the literature of a liothyronine induced cardiomyopathy. The patient was discharged on levothyroxine 137 mcg. He planned to follow with an endocrinologist and avoid excessive hormonal supplementation in the future. This case illustrates the need for more oversight of nontraditional uses of hormonal therapy.
Thyroid Nodules & Goiter Saturday Poster Case Report
Plasmacytoma of the thyroid gland is a rare condition. Less than 80 cases have been reported in literature. Its pathology, prognosis, and treatment remain largely unknown. To date, the majority of reported cases have been diagnosed on surgical pathology specimens obtained during thyroidectomy or thyroid lobectomy.
We present a case in which the diagnosis was made by ultrasound guided core needle biopsy (USGCNB).
A 64 year old man notes neck swelling and neck ultrasound showed a 3.6 cm mass in the right thyroid lobe. He had no history of thyroid dysfunction and thyroid function tests were normal. FNA of the nodule showed preliminary findings of lymphocytic infiltration. Final cytopathology revealed findings concerning for medullary thyroid cancer. Serum calcitonin was <2. FNA was repeated 6 weeks later and 3 passes were sent for cytopathology which revealed findings concerning for lymphoproliferative neoplasm. An additional pass was sent for flow cytometry, however results were inconclusive. He was also found to have a possible pathologic fracture of the left clavicle. He then underwent USGCNB of the thyroid lesion. This revealed kappa restricted lymphocytes with plasmacytoid morphology. He was diagnosed with intra-thyroidal plasmacytoma. An evaluation for multiple myeloma was negative. He underwent external beam radiation therapy with dose of 30 Gy in 12 fractions focused to the right neck, left lower neck, and left clavicle.
Extramedullary plasmacytoma of the thyroid is a unique subset of monoclonal gammopathies. To date, the majority of documented cases have been diagnosed with surgical pathology. In our case the diagnosis was made after core needle biopsy was performed. Thus far, the literature has suggested that possible treatment options include either radiation therapy or surgical resection of lesions. Making this diagnosis by core biopsy may be beneficial in patients for whom surgical resection may not be desirable.
Abstract Author Index
A'Amar, O.M. 159, 163, 250
Abdel Nabi, H.H. 230
Abid, A. 256
Ablan, F. 248
Abraham, A. 259
Acampado, L.T. 176
Aceves, C. 237
Adili, A. 96
Adzick, N. 131
Aftab, D.T. 4
Agcaoglu, O. 132
Agosto, M. 87
Aguilar, A.I. 175
Akamizu, T. 12
Al-Brahim, N. 60
Al-Qurayshi, Z. 64
Alexander, E. 16
Ali, H. 119
Ali, M. 90
Ali, S.K. 96
Aliyev, S. 132
Allende, M. 87
Almeida, J.M. 207
Alva-Sánchez, C. 66
Amaral, L.P. 207
Andersen, S. 18
Andersen, S.L. 183
Anderson, R.J. 150, 177
Andersson, M. 114
Andrade, C. 2
Angajala, A. 151
Angamuthu, A. 257
Angell, T.E. 209
Angelos, P. 158
Anguiano, B. 237
Antonelli, A. 19, 33, 139
Antonopulos, C. 79
Aponte, M.A. 248
Araújo, P.P. 207
Arce, K.M. 115
Arcidiacono, A. 246
Armstrong, M. 219
Artymyshyn, R. 57
Arumugam, D. 57
Asa, S.L. 84
Aschebrook-Kilfoy, B. 158
Assaf, R.R. 81
Assi, J. 220
Assumpæão, L.M. 122
Astapova, I. 1, 9
Au, J. 226
Aydogan, B.I. 49
Ayers, S. 151
Azar, F. 159
Bach, P.R. 186
Bae, J. 55
Baek, K. 55
Bahn, R.S. 3, 91
Baker J.R., Jr. 17
Balakrishnan, V. 257
Balazs, G. 2, 93
Baldanza, M. 2
Balm, A.J. 118
Banerjee, M. 126
Barajas, L. 89
Barbagli, L. 39
Bargi-Souza, P. 95
Barnard, N.J. 57
Barrera, J.R. 82
Barros Filho, M. 202
Bastholt, L. 100
Bauer, A.J. 131
Bazotte, R.B. 241
Beadnell, T.C. 179
Becerra-Cervera, A. 66
Begnami, M. 122
Belfort, M.B. 15
Bellabarba, D. 178
Benamira, L. 228
Benvenga, S. 162, 186
Berber, E. 108, 132, 156
Bernet, V.J. 215, 216
Bhaat, N. 210
Bhagavatula, S. 168
Bhat, S. 169
Bhatia, N.D. 141
Bianchi, L. 251
Bianco, A. 2, 65, 93, 149
Bible, K.C. 180
Bielory, B. 168
Bigio, I.J. 159, 163, 250
Bilban, M. 1
Bischoff, L.A. 252
Bizhanova, A. 113
Bjelobaba, I. 95
Bliddal, S. 11
Block, R. 211
Boas, M. 11
Bocco, B. 93
Bockisch, A. 100
Bodenner, D. 256
Boelaert, K. 30, 32, 34
Bok, I. 203
Bom, H. 212
Bong, J.G. 244
Bongarzoni, G. 79
Bonomo, G. 77
Borkenstein, M.H. 67
Borucu, T. 104
Bossou, A.R. 180
Bossowski, A. 102
Boufraqech, M. 7
Bouhassira, E. 36
Boutin, A. 240
Bove, A. 79
Bowers, B. 179
Boyle, L. 225
Bradley, E.A. 3
Braren, R. 5
Braverman, L.E. 15, 24, 184, 185
Brickman, D. 125
Brilz, A. 226
Brose, M.S. 4, 100
Brown, R.S. 15, 102
Brown, S. 92
Brugos, A. 154
Brusca, N. 251
Buckey, T.M. 37
Bufalo, N. 122, 207
Builes-Barrera, C. 28, 196
Burke, C. 249
Burman, K.D. 23, 142, 153, 225
Burns, R. 114
Busaidy, N. 38, 96, 97, 227
Bümming, P. 46
Cabanillas, M.E. 35, 38, 96, 97, 227
Cabral, J. 115
Caldwell, K. 199
Calil-Silveira, J. 113, 198
Calzone, K. 44
Camerieri, L. 245
Campbell, M.J. 138
Campos, A. 122
Candell, L. 138
Cantara, S. 103
Cappola, A.R. 92
Cardenas, A. 193
Carlo-Chevere, V.J. 56
Carlson, D.L. 118
Carlé, A. 18
Carraro, D.M. 41
Carroll, N. 225
Carty, S.E. 13, 219
Carvalho, A. 241
Carvalho, A.L. 41
Caselli, M. 39
Casey, M. 114
Casillas, J. 124
Casler, J.D. 216
Castagna, M. 39
Castillo, M. 93
Cella, D. 100
Cellini, M. 251
Cenci, V. 103
Centanni, M. 110, 251
Ceyhan, K. 49
Chai, Y. 48, 121
Chan, C. 179, 201
Chandarana, S. 226
Chang, K. 157
Channon, S. 184
Chanthasenanont, A. 24
Chapuis, H. 119
Charatcharoenwitthaya, N. 24
Chasen, B. 96
Chen, A. 157
Chen, C. 157
Chen, G.G. 40
Chen, H. 52, 191
Chen, K. 157
Chen, R. 213
Cheng, J.K. 47, 220
Cheng, S. 10
Chernoff, A. 109
Chertman, M. 81
Chiarini, S. 79
Chin-Lenn, L. 226
Chindris, A. 216
Chiriboga, P. 91
Chiu, J. 182
Cho, J. 27, 128, 194, 232, 247
Cho, S. 212, 229
Cho, Y. 217
Choi, J. 48
Chomienne, C. 36
Choudhary, C. 142
Chowdhry, M. 172
Chowdhury, S. 253
Chu, R. 40
Chune, G. 86
Chung, I. 48, 229
Chung, J. 100
Chung, K. 27, 128, 194, 232, 247
Church, J. 249
Cibas, E. 117
Clark, O.H. 138
Clarke, B.L. 106
Clary, D.O. 4
Clayman, G. 210
Clemmens, C.S. 131
Coenen, M. 91
Cohen, E.E. 4
Cohen, R. 1
Copland, J.A. 203, 206
Corapcioglu, D. 49
Corazza, A. 245, 246
Corrado, A. 19, 33
Correa, A. 209
Correa da Costa, V. 69
Correa-Medina, M. 93
Cosentino, G.L. 255
Cote, G. 38, 96, 97
Couvreur, P. 119
Cox, K. 68
Cradic, K.W. 180
Crawford, B. 134
Crist, A. 206
Cunha, L.L. 41
Curry, J. 252
Cysneiros, R.M. 65
D'Addetta, V. 79
D'Haene, N. 101
Da Settimo, F. 33
Dadu, R. 96, 97, 227
Dali, D. 64
Danysh, B.P. 35
Darwin, C.H. 88
Davidov, T. 57
Davies, T.F. 8, 90
Dayan, C.M. 184
de la Chapelle, A. 92
de la Fouchardiere, C. 100
De Nève, N. 101
De Remigis, A. 189
De Remigis, P. 189
Deen, M. 57
Degand, C. 101
Del Duca, S. 110, 251
Delgado, E. 237
den Heijer, M. 92
Deniz, O. 49
Desantis, P. 115
Desmaële, D. 119
Deutschmann, M. 226
Devine, C. 97
Di Domenicantonio, A. 139
Di Renzo, R. 79
Diacovo, J. 115
Diana, T. 102, 188
Diehl, N.N. 215
Dietz, N.E. 177
Diggans, J. 75
Dinets, A. 99
Dipp, S. 62
Dort, J. 226
Du, Z. 213
Dubin, R.L. 255
Duh, Q. 138
Duke, W.S. 223
Dutta, D. 253
Ebner, S. 259
Edwards, C. 85
Ehrenkranz, J. 186
Ekblad, L. 6
Eliseeva, E. 94, 240
Elisei, R. 4, 100
Ellis, R. 7
Elson, D.F. 191
Emral, R. 49
Eng, J. 72
Epstein, A.L. 209
Eriksson, H. 99
Ersoy, B. 104
Escalada, J. 154
Eszlinger, M. 117
Faber, J. 11
Fagin, J.A. 118
Fallahi, P. 19, 33, 139
Fan, Y. 17, 147
Fatemi, S. 137
Faugeron, I. 36
Fei, C. 37
Feldt-Rasmussen, U. 11
Felger, E. 225
Feng, X. 249
Fernandes, G. 2, 93
Ferrannini, E. 19, 33, 139
Ferrari, S. 19, 33, 139
Ferreira, A. 93
Filipsson Nyström, H. 31
Finigan, D. 23
Fioravanti, C. 103
Fletcher, R. 34
Florea, A. 228
Fong, J.C. 32
Fonseca, T. 2, 93
Fontenot, T.E. 221
Forest, V. 228
Franklyn, J. 34
Franklyn, J.A. 30, 32
Frayling, T. 92
Freathy, R. 92
Friedlander, P.L. 64, 134, 136, 155, 221
Friedrich, N. 238
Friis-Hansen, L. 11
Fröhlich-Reiterer, E. 67
Fronteras, M. 168
Fu, L. 182
Furlong, K.J. 258
Furukawa, Y. 12
Gaba, R. 173
Galleri, D. 33
Gallistl, S. 67
Galofré, J. 154
Ganly, I. 43, 51, 53, 118
Gannon, A.W. 131
Garces, A. 58
Garcia-Rueda, K. 196
Gargano, L. 110, 251
Garmendia, A. 154
Garrity, J.A. 3
Gatto, I. 110
Ge, K. 148
Gershengorn, M.C. 94, 148, 240
Gesuwan, K. 44
Ghossein, R.A. 118
Gianoukakis, A.G. 89, 135
Giordano, N.J. 159, 160, 163, 250
Göke, B. 5
Goldfarb, M. 124
Goldfarb, R. 146
Goldstein, D. 54
Gomez-Rueda, H. 63
Gong, R. 213
Gong, Y. 213
Gonzalez, R. 87
Gonzalez-Rodriguez, L. 58, 87
Gordon, J.H. 15
Gornet, T. 38
Gosnell, J.E. 138
Gough, S. 92
Goulart-Silva, F. 95
Gounden, V. 190
Grangl, G. 67
Grebe, S.K. 180
Grogan, R. 158
Gruenwald, G. 5, 236
Gu, J. 23
Guerrero, M. 193
Guillén-Grima, F. 154
Gulati, N. 44
Gunnarsdottir, K.A. 46
Habra, M.A. 96, 97, 227
Hale, A.R. 15
Hamman, K. 125
Hammond, R. 131
Han, J. 133
Hands, K.E. 214
Handy, B. 38
Hansen, D.P. 11
Hardman, J.C. 164
Haugen, B. 16, 116, 201
Hay, I.D. 129, 216
Haymart, M. 126
He, M. 7, 44
He, X. 15, 24
Heiden, K. 181
Heller, K.S. 78
Hennessey, J.V. 161
Hernandez, M. 97
Hernandez-Puga, G. 166
Hier, M. 228
Higuchi, Y. 71
Hilsted, L. 11
Ho, A.S. 51
Hodak, S.P. 13, 219
Hofer, N. 67
Hoffman, T. 114
Hofmann, M. 35
Hollenberg, A.N. 1, 9
Holmberg, E. 46
Homuth, G. 238
Hong, J. 130
Hong, S. 27, 128, 194, 232, 247
Horasan, G.D. 104
Hu, M.I. 38, 96, 97, 227
Hu, Z. 75
Huang, H. 239
Huang, J.Y. 244
Huang, M. 105
Huang, R. 114
Hulthén, L. 31
Hurtado-Lopez, M.L. 61
Husemoen, L. 92
Hussain, A. 168
Hwang, S. 217
Höög, A. 6, 99
Ibrahim, Y. 134, 155
Ibrahimpasic, T. 118
Ignacio, D.L. 2
Imam, S. 174
Imamura, Y. 254
Inaba, H. 12
Inoue, Y. 71
Isham, C.R. 180
Iskander, M. 77
Islam, F. 14
Ito, K. 73, 195, 242, 243
Iwaku, K. 73, 195, 242, 243
Iyer, S. 91
Jabbour, S. 252
Jaimes, F. 28
Jain, M. 7
Jansson, S. 46
Jarzab, B. 100
Jaume, J.C. 174, 191, 260
Jee, H. 121
Jensen, R. 92
Jeon, M. 133
Jeong, Y.J. 244
Jiang, N. 105
Jimenez, C. 38, 96, 97, 227
Jimeno, C. 231
Jin, J. 108, 156
Jing, X. 179
Jirajariyavej, T. 89, 135
Johnson, T. 108
Jones, M.F. 191
Jonklaas, J. 23, 190
Jozaghi, Y. 228
Juhlin, C. 6
Jung, C. 55
Jung, J. 48, 121
Jung, S. 127
Juul, A. 11
Kahaly, G.J. 102, 188
Kalady, M. 249
Kallakury, B.V. 37
Kameda, T. 73, 242, 243
Kaminskyy, V.O. 6
Kandil, E. 64, 134, 136, 155, 221
Kang, D. 235
Kang, M. 55
Kang, S. 212
Kanitz, M. 102, 188
Kannan, L. 109
Kantarci, M. 170
Kaplan, E. 158
Kaplan, S. 258
Kappeler, C. 100
Karmisholt, J. 18
Kashat, L. 47, 220
Kattan, M. 43
Katz, L.S. 148
Kazahaya, K. 131
Keating, K. 100
Kebebew, E. 7, 44
Kennedy, G.C. 75
Kerege, A.A. 201
Khadra, H. 64
Khan, A. 171
Kieth Cryar, A. 80
Kim, B. 167
Kim, C. 16
Kim, D. 10
Kim, E. 48, 121, 229
Kim, H.T. 244
Kim, J. 179, 212
Kim, K. 48, 59, 217, 244
Kim, M. 55
Kim, S. 48, 121
Kim, T. 133
Kim, W. 133
Kim, Y. 59, 144
Kinuya, S. 254
Kiremitci, S. 104
Kloos, R. 75
Klopper, J. 16
Klutz, K. 5
Knoop, K. 5, 236
Kobayashi, S. 73, 195, 242, 243
Koenig, J. 102
Kolukula, S. 150
Konishi, K. 71
Koo, D. 48, 121
Kopp, P. 113, 198
Kovatch, K. 131
Krane, J. 117
Krejbjerg, A. 18
Kucka, M. 95
Kumar, S. 91
Kunii, Y. 73, 195, 242, 243
Kushchayev, S. 225
Kushchayeva, Y. 225
Kwon, H. 48, 121
Kwon, S. 212
Kyouzuka, A. 71
Köhrle, J. 238
La Motta, C. 33
Lagari-Libhaber, V. 167
Lagast, H. 106
LaGuardia, L. 249
Lahti, J. 92
Lammel, J. 151
Lanman, R. 75
Larsen, T. 11
Larsson, C. 6, 31, 99
Latif, R. 8, 90
Latuf-Filho, P. 41, 122
Laurberg, P. 18, 183
Lazarus, J. 184
Le Mercier, M. 101
Lechner, M.G. 209
Lee, E. 217
Lee, H. 48, 121
Lee, J. 89
Lee, K. 48, 55, 121, 229
Lee, R.A. 129
Lee, S. 59, 127
Lee, S.L. 159, 160, 163, 208, 250
Lee, S.Y. 185
Lee, Y. 27, 128, 194, 232, 247
Lehmphul, I. 238
Lehtiö, J. 99
Leon Guerrero, A.H. 141
Leung, A.M. 15
Lewis, M. 143
Lewy, G. 32
Li, C. 197
Li, H. 197
Li, J. 105, 239
Li, Z. 213
Lim, D. 55, 201
Lim, I.P. 141
Lindahl, B. 31
Linneberg, A. 92
Liu, B. 187
Liu, S. 40
Liu, W. 187
Liu, X. 37
Lo, T. 231
LoPresti, J.S. 209
Lu, S. 57
Lucido, D. 77
Lundqvist, A. 6
Lupo, M. 76
Luttrell, L. 112
Ma, R. 8
Ma, S. 48
Macias, C.A. 57
Madison, D. 125
Madorin, C.A. 42, 211
Maino, F. 39
Maisnam, I. 253
Maletkovic, J. 88, 169
Mancusi, C. 139
Mandel, S. 16
Mangeshkar, M. 4
Manousou, S. 31
Marcello, M. 207
Marcello, M.A. 41
Marlow, L. 206
Marlow, L.A. 203
Marques, A.R. 241
Marti, J. 77, 98
Martinez, M. 87
Martins, M.B. 122
Masoodi, H.M. 134, 136, 221
Massaad-Massade, L. 119
Materazzi, G. 33, 139
Mathison, J. 75
Matsumoto, M. 73, 195, 242, 243
Mattei, P. 79
May, M. 57
Mazzaglia, P.J. 74
McAndrews, M. 22
McAninch, E. 93, 149, 167
McCabe, C.J. 30, 32, 34, 164
McCoy, K.L. 219
McKenney, R. 174, 260
McPhaul, L. 89
Medici, M. 92
Meisinger, C. 92
Mellberg, C. 31
Melvin, C. 72, 153
Memmo, S. 39
Merino, M. 7
Mete, O. 84
Metzger, R. 156
Meyer zu Schwabedissen, H. 92
Miccoli, P. 33, 139
Michaelis, C. 38
Michigishi, T. 254
Milas, M. 74, 125, 132, 156, 249
Milas, Z.L. 210
Miller, J.L. 252
Miller, T.C. 182
Milosevic, D. 180
Min, J. 212
Mino, J. 45
Minuto, M. 33
Miracle, S. 61, 165
Miranda, M.F. 2
Mitchell, J. 108, 156
Mitsuhashi, T. 123, 145, 233, 234
Mizukami, Y. 254
Mlynarek, A. 228
Modasia, B. 30
Mohamed, S.H. 64, 136, 155
Mohan, V. 115
Moises, C. 93
Molnar, I. 100
Momotani, N. 71
Monteiro, R. 45
Moo-Young, T.A. 42, 211
Moon, S. 55
Morari, E.C. 41
Morino, M. 71
Moroz, K. 155
Morris, L.G. 98
Morrison, J.A. 116
Morshed, S.A. 90
Mostoufi-Moab, S. 131
Muenz, D. 126
Mukasa, K. 73, 195, 242, 243
Mukhopadhyay, S. 253
Mullan, K. 114
Muntean, W. 67
Murcy, M.A. 134, 136
Murono, S. 205
Musa Yola, I. 221
Müller, A.M. 236
Nabhan, F. 16
Naeem, A. 54
Nagar, S. 158
Nagataki, S. 50, 73, 195, 242, 243
Nagavalli, S. 89
Nagy, R. 92
Nahar, N.N. 177
Naitza, S. 92
Nakoneshny, S. 226
Napolitano, G. 189
Nardi, M. 19
Nassif, R.J. 65
Nauck, M. 238
Navarrete-Ramírez, P. 166
Nelson, P.J. 236
Nelson, S.M. 15
Netzel, B.C. 180
Neumann, S. 94, 240
Newfield, R. 199
Ng, E.K. 40
Niedziela, M. 102
Nikiforov, Y.E. 13, 219
Nikiforova, M.N. 13
Nilubol, N. 7, 44
Ning, G. 120
Nishi, M. 12
Nixon, I. 118
Nixon, I.J. 43
Noh, J.Y. 195, 242
Nosenzo, F. 245
Nowak, J. 211
Nunes, M. 69, 95, 113, 198, 241
Nutting, C. 100
Nygaard, B. 18
O'Dowd, C. 114
O'Malley, M. 249
Occhini, R. 39
Ogilvie, J.B. 141
Ogris, M. 5
Ohye, H. 73, 195, 242, 243
Ojomo, K.A. 191
Okosieme, O.E. 184
Olsen, J. 183
Olsson, T. 31
Oltmann, S. 52
Ong, E. 193
Ongphiphadhanakul, B. 24
Orbak, Z. 170
Orlov, S. 47, 220
Orozco, A. 166
Pacini, F. 39, 100, 103
Paek, S. 48, 121
Pai, R.R. 80
Palacios, K. 28
Palmer, F.L. 43, 51, 53, 118
Palone, G. 79
Pan, C. 187
Pan, Y. 199
Pankratz, D. 75
Pantaleao, T. 69
Panunti, B. 62
Panveloski-Costa, A. 241
Park, H. 130, 212
Park, J. 10
Park, K. 217
Park, S. 48, 59
Park, S.H. 244
Park, W. 133
Parker, C. 16
Parrack, K. 156
Paschke, R. 100, 117
Pasieka, J. 226
Pasqui, L. 103
Patel, D. 7
Patel, K.N. 78, 141
Patel, R. 146
Patel, S.G. 43, 53, 118
Payne, R.J. 228
Paz-Pacheco, E. 231
Pearce, E.N. 15, 24, 107, 184, 185
Pedersen, I. 18
Peeters, R. 92
Pepper, G.M. 25
Perlman, S.B. 191
Pernemalm, M. 99
Perugin Bernardi, S. 246
Pervaiz Munir, N. 54
Petrovic, I. 137
Phillips, K. 152
Pietzner, D. 92
Pietzner, M. 238
Pike, L.A. 116, 179
Pilli, T. 39, 103
Pistis, G. 92
Pomerantz, S. 109
Ponnusamy, D. 86
Poole, V.L. 30
Porcu, E. 92
Pribitkin, E. 252
Prinz, R.A. 42, 181, 211
Psaty, B. 92
Puzziferri, N. 70
Qu, S. 197
Racedo, K. 146
Rachinsky, I. 218
Räikkönen, K. 92
Rajab, H. 112
Ramadoss, P. 1
Ramalho Prado dos Santos, N. 69
Ramaswami, N. 173
Ramirez, M. 58, 87
Rangel, I.F. 2
Rawal, R. 92
Read, M. 34
Read, M.L. 30, 32
Recker, R.R. 177
Reiher, A. 211
Reynolds, J. 75
Ribeiro, M.O. 65
Ricarte-Filho, J.C. 118
Richards, R.J. 255
Riggs, A. 256
Rivadeneira, F. 92
Rivera, K. 85
Rivera, M. 216
Roberts, D. 210
Rocha, A.G. 122
Rodriguez-Diaz, E. 159, 163
Roef, G. 92
Roman-Gonzalez, A. 196
Rorive, S. 101
Rosen, D. 258
Rosen, J.E. 159, 160, 163, 208, 250
Rossi, C.L. 207
Rotstein, L. 84
Rovet, J.F. 14, 22
Ruffilli, I. 19, 33
Ryan, G. 30, 32
Ryberg, M. 31
Sacks, W. 172
Sadowski, S.M. 44
Sahin, M. 49
Salari, F. 47, 220
Salathe, M. 149
Salcedo, F. 87
Salmon, I. 101
Sampson, J. 125
Sams, S.B. 116
Sandberg, S. 31
Sanders, J. 106
Sanders, R.L. 57
Sandoval, M.S. 175
Sandro, C. 103
Sanna, S. 92
Santaguida, M. 110, 251
Santos, S. 154
Saraceno, G. 162
Sarapuddin, S.T. 82
Sartoris, R. 245, 246
Sasaki, E. 73
Sathasivam, A. 23
Sauseng, W. 67
Sawicki, M. 143
Sawka, A. 54
Schiavon, F.P. 241
Schlagenhauf, A. 67
Schlageter, M. 36
Schlumberger, M. 4, 100
Schmid, N. 149
Schmohl, K.A. 236
Schneider, D.F. 52, 191
Schorr, M. 16
Schurmann, C. 238
Schwaiger, M. 5
Schwenk, N. 5, 236
Schweppe, R.E. 116, 179, 201
Schöffski, P. 4
Scorza, F.A. 65
Segni, M. 102
Sellari-Franceschini, S. 19
Sellin, R.V. 96, 97
Senekowitsch-Schmidtke, R. 5
Serrano-Nascimento, C. 69
Sestini, F. 103
Settles, M. 5
Sevell, R. 209
Shah, J.P. 43, 51, 53, 118
Shah, K. 227
Shaha, A.R. 43, 53
Sharma, N. 34
Sharma, V. 116
Shen, L. 120
Shen, W.T. 138
Sheng, C. 197
Sheng, H. 197
Sherman, S. 97
Sherman, S.I. 4, 38, 96, 100, 227
Shi, Y. 182
Shields, B. 92
Shimizu, H. 1
Shin, D. 217
Shin, J. 108, 156, 249
Shindo, M. 125
Shong, Y. 100, 133
Shrestha, R.T. 161
Shum, L. 58
Siena, S. 100
Silva, A.N. 41, 122
Silvestri, E. 245, 246
Simmonds, M. 92
Siperstein, A.E. 45, 108, 132, 156, 249
Sipos, J. 16
Sippel, R.S. 52, 191
Siveke, J. 5
Skocic, J. 14
Smallridge, R.C. 203, 206, 215, 216
Smit, J. 92, 100
Smith, J.A. 164
Smith, V.E. 30, 32, 34
Smyth, P. 184
Smyth, P.P. 114
Soares, F.A. 41
Sofiadis, A. 99
Soldin, O.P. 23, 37, 72, 153
Soldin, S.J. 23, 190
Somprasit, C. 24
Sonderman, P.E. 191
Song, H. 187, 212
Spencer, C. 137
Spitzweg, C. 5, 236
Srimatkandada, P. 107
Stack, B. 256
Stagnaro-Green, A. 68, 107
Stan, M.N. 3
Stang, M.T. 219
Steward, D. 16
Stojilkovic, S.S. 95
Straub, J.E. 160
Stulin, I. 248
Ståhl, M. 31
Su, B. 197
Sugisaki, H. 123, 145, 233, 234
Suh, H. 163, 208
Suh, Y. 48, 121
Sung, J. 48, 229
Sung, T. 27, 128, 194, 232, 247
Suzuki, M. 73, 195, 242, 243
Suzuki, N. 73, 242, 243
Sviatoha, V. 6, 99
Tabor, A. 11
Tae, S. 48, 121
Takeda, H. 254
Takeshima, K. 12
Tamilia, M. 228
Tan, A. 179
Tarasova, V.D. 150, 177
Tassaduq, S. 136
Taylor, P. 184
Teixeira, S.S. 241
Tentler, J. 179
Terris, D.J. 223
Tessnow, A. 70
Teumer, A. 92
Thapa, P. 3
Theimer, C. 36
Thida, S. 174
Thomas, C. 216
Thomas, D. 53
Thomas, E. 36
Tincani, A.J. 207
Tirado, M. 58
Tirumalasetty, N. 62
Tomemori, T. 123, 145, 233, 234
Toniolo, D. 92
Tonyukuk, V. 49
Torres Garcia, E. 29
Toti, P. 39
Toubert, M. 36
Traikovic-Arsic, M. 5
Treviño, V. 63
Trimarchi, F. 162
Trooskin, S.Z. 57
Truong, K. 76
Tsai, W. 135
Tsuji, S. 254
Tsukatani, T. 254
Turtulici, G. 245, 246
Tuttle, R. 43, 51, 53, 98, 118
Uitterlinden, A. 92
Uppal, A. 158
Urbanozo, H.C. 176
Urbinati, G. 119
Urrea Pineda, L. 196
Uysal, A.R. 49
Vaisman, M. 192
van Hasselt, C. 40
Van Rossum, N. 178
Van Uum, S. 218
Vargas, C. 196
Vassallo, J. 41, 122
Vega, M.A. 58
Velez, R. 87
Velichko, S. 75
Vella, K. 1, 9
Veloski, C. 257
Via, M. 146
Vianale, L. 189
Villabona, C.V. 115
Villanueva, I. 66
Vimont, V. 36
Virili, C. 110, 251
Visser, T.J. 92
Vita, R. 162
Vlantis, A.C. 40
Völker, U. 238
Völzke, H. 92, 238
von Roemeling, C. 206
Voroshilov, V. 160
Wagner, E. 5
Waguespack, S.G. 38, 96, 97, 227
Wald, A. 13
Walfish, P. 47, 220
Wallaschofski, H. 238
Waller, J.L. 223
Walsh, J. 92
Walsh, S. 75
Wang, A. 171
Wang, F. 208
Wang, H. 23
Wang, J. 197
Wang, L.Y. 53
Wang, M.B. 143
Wang, S. 17
Ward, L.S. 41, 122, 207
Watanabe, N. 73, 195, 242, 243
Watanabe, R. 123, 145, 233, 234
Watkins, R. 34
Watkins, R.J. 30, 32
Watkinson, J.C. 32, 164
Webb, P. 151
Wechselberger, A. 236
Wei, T. 213
Wennerberg, E. 6
Wennerberg, J. 6
Werneck de Castro, J. 93
Werneck-de-Castro, J.S. 2
Westphal, S.A. 216
White, J.R. 223
Williams, M. 96
Williamson, A.J. 181
Willoughby, K.A. 22
Wilson, S. 92
Winchester, D.J. 42, 211
Wirth, L. 4
Wolfson, R. 218
Woliner, K.N. 111
Wong, M. 75
Woo, J. 48, 121
Wood, W.M. 116
Worden, F. 100
Wu, C.S. 183
Wu, M. 157
Xiong, Y. 7
Xu, C. 167
Xu, S. 148
Xu, X. 181
Xue, L. 187
Yamaoka, H. 12
Yan, Z. 239
Yang, H. 219
Yang, S. 187
Yao, Y. 21
Yau, H. 85
Ye, F. 1, 9
Ye, L. 120
Yen, V. 146
Ying, A. 97, 227
Yip, L. 219
Yokoyama, K. 254
Yoon, J. 27, 128, 194, 232, 247
Yoshihara, A. 73, 195, 242, 243
Yoshimura Noh, J. 73, 243
Yoshizaki, T. 205
Youn, Y. 48, 121, 229
Younis, I. 153
Yu, C. 43
Yu, J.Z. 141
Yuan, X. 197
Yun, N. 128
Zamudio, S. 66
Zava, D.T. 26
Zava, T.T. 26
Zedenius, J. 6, 99
Zhang, L. 7
Zhang, Z. 105
Zhao, S. 187
Zhivotovsky, B. 6
Zhou, J. 197
Zhou, Q. 116
Zhou, Y. 42
Zhu, J. 213
Zumoff, B. 146