
Abstract
Background:
Management of patients with thyroglobulin (Tg)-positive/scan-negative thyroid cancer remains challenging. American Thyroid Association (ATA) guidelines recommend potential use of empiric 131I therapy and various scanning modalities, but no standard for managing such cases exists.
Methods:
We surveyed ATA members to assess current practice in management of patients with Tg-positive/scan-negative disease. Members participated in a web-based survey of six case scenarios of Tg elevations but iodine scan negativity.
Results:
A total of 288 ATA members (80% male) participated. Patient age, sex, and basal and stimulated Tg varied between the cases. Respondents were asked their opinion regarding empiric 131I therapy use, including 131I dose, use and duration of low-iodine diet, thyroxine withdrawal or recombinant human thyrotropin (rhTSH), and utilization of additional imaging (neck ultrasound (US) or positron emission tomography/computed tomography (PET/CT)) and reconsideration of 131I therapy. Between 16% and 51% recommended initial use of empiric 131I for the various scenarios. The majority chose a 131I dose between 75 and 150 mCi, and 73% employed a low-iodine diet for two or more weeks. Preference between thyroxine withdrawal versus rhTSH was evenly split. More than 98% obtained a neck US if empiric 131I was not given; 52–89% would proceed to PET/CT if US was negative. Only 44% used rhTSH stimulation in PET scan preparation. 131I use was more common with stimulated Tg significantly >10 ng/mL. 131I therapy was slightly more likely with PET-positive (56%) than PET-negative status (45%). Respondents were split regarding empiric 131I if basal and stimulated Tg increased ≥150% over two years. Providers in North America less commonly utilized 131I treatment than those from other areas. In the face of possible heterophilic antibody interference in the Tg assay, the majority did not recommend 131I therapy.
Conclusions:
Empiric 131I therapy is still utilized for patients with Tg-positive/scan-negative disease. Neck US is frequently used to further evaluate such cases as 18FDG-PET/CT, albeit the latter is used somewhat less often. Use of 131I therapy correlated with the degree of Tg elevation or development of Tg antibodies, and was recommended more commonly with PET-positive than PET-negative status in patients with lower Tg levels. 131I was less commonly used by providers within North America.
Introduction
M
Since many of the recurrences/persistent disease were detected in the neck, once neck ultrasonography (US) became a common method of detecting disease, a strategy of recombinant human thyrotropin (rhTSH) stimulated Tg and neck US was recommended (21). However, some disease still went undetected, and so the era of positron emission tomography (PET), computed tomography (CT), and 18FDG-PET/CT imaging has provided additional diagnostic resources to the clinician (22 –29). Further refinements have involved the use of rhTSH potentially to increase the sensitivity of PET imaging (30).
The current study is a web-based survey of clinician members of the American Thyroid Association (ATA), to assess practice trends of thyroid experts regarding management of patients with Tg positive/imaging negative disease with respect to use of empiric 131I therapy. Six case scenarios are presented, with variables including patient age, Tg level, use of rhTSH, low iodine diet use and duration, as well as imaging options.
Methods
A web-based survey of 67 questions was developed at the Mayo Clinic Survey Research Center, and a link to the survey was provided to the office of the ATA and subsequently distributed by e-mail to 1387 ATA clinician members. Approval to distribute to members was given by the ATA Board of Directors. The survey was determined by the Mayo Clinic Institutional Review Board to be exempt from IRB review. Two follow-up requests asking for survey completion were sent, and a total of 288 responses were received. The data were transferred to the Division of Biostatistics, Health Science Research for analysis. The survey questions and responses are provided in the Supplementary Data (Supplementary Data are available online at
Six cases were presented, as follows:
Case A: A 60-year-old man had a total thyroidectomy and central compartment neck dissection for a 2.5 cm classic papillary thyroid carcinoma with minimal extrathyroidal extension, and 5 of 20 lymph nodes in level VI were involved with metastatic disease. The patient received 150 mCi 131I for ablation while hypothyroid, and the post-therapy WBS showed uptake only in the central neck. One year later, when TSH <0.1 mIU/L, T4-suppressed thyroglobulin (Tg-supp)=1.5 ng/mL, and thyroglobulin antibody was negative. After rhTSH, Tg-stim=8 ng/mL, and 123I WBS showed no uptake in the central neck or elsewhere.
Q1: Would you give an empiric therapeutic dose of 131I?
If yes, would you prepare the patient with rhTSH? Hypothyroidism?
Q2: What dose would you administer?
30–50 mCi, 75–100 mCi, or 125–150 mCi? Other dose?
Q3: Would you prepare with a low-iodine diet?
If yes, for how long? One week, two weeks, other?
Q4: If empiric 131I is not given, would you perform a neck US?
Q5: If neck US is negative, would you give empiric 131I?
Q6: If both DxWBS and US are negative and you do not give empiric 131I, would you order an 18FDG-PET/CT scan?
Q7: If you order a 18FDG-PET/CT scan, would you pretreat with rhTSH?
Q8: If the 18FDG-PET/CT scan is also negative, would you recommend empiric 131I therapy?
Q9: If the 18FDG-PET/CT scan is positive, would you recommend empiric 131I?
For Cases B–D, the same questions were asked as in Case A, with the exception of the two relating to low-iodine diet. We assumed that respondents would use the same preparation under all scenarios. For Cases E and F, we asked only two and one question(s) respectively.
Case B: Same scenario as Case A, except Tg-supp=12 ng/mL and Tg-stim=80 ng/mL.
Case C: A 25-year-old woman had a total thyroidectomy and central compartment neck dissection for a 2.5 cm classic papillary thyroid carcinoma with minimal extrathyroidal extension, and 5 of 20 lymph nodes in level VI were involved with metastatic disease. The patient received 150 mCi 131I for ablation while hypothyroid, and the post-therapy WBS showed uptake only in the central neck. One year later, when TSH <0.1 mIU/L, T4-suppressed thyroglobulin (Tg-supp)=1.5 ng/mL, and thyroglobulin antibody was negative. After rhTSH, Tg-stim=8 ng/mL, and 123I WBS showed no uptake in the central neck or elsewhere.
Case D: Same scenario as Case C, except Tg-supp=12 ng/mL and Tg-stim=80 ng/mL.
Case E: A 60-year-old man with Tg-supp=1.5 ng/mL and Tg-stim=8 ng/mL had negative Dx-123I, US, and 18FDG-PET/CT imaging, and did not receive empiric 131I therapy. Two years later, Tg-supp=3.8 ng/mL when TSH <0.1 mIU/L, and rhTSH-stim Tg=20 ng/mL. Dx-131I, US, and 18FDG-PET/CT imaging were again negative for recurrence.
Q1: Would you give an empiric therapeutic dose of 131I?
Q2: If the thyroglobulin antibody had become strongly positive, would you give empiric 131I? (Case E′)
Case F: A 50-year-old woman had total thyroidectomy for a 2.5 cm papillary thyroid carcinoma and received 75 mCi 131I for ablation. One year later, serum Tg was <0.1 ng/mL before and after rhTSH, and Dx-131I WBS and neck US were negative. Two years later, she developed rheumatoid arthritis and was treated with infliximab. Serum Tg=12 ng/mL when TSH <0.1 mIU/L and was 12.4 ng/mL after rhTSH. Neck US, Dx-123I, and 18FDG-PET/CT scans were negative.
Q1: Would you give an empiric therapeutic dose of 131I?
Results
Demographics of survey respondents
Two hundred eighty-eight physicians responded to the survey, although not all individuals responded to every question for every case (Supplementary Table S1). The majority were male. Ages were broadly distributed, although 60% of respondents were aged 50 years or older. Almost 80% of participants were from North America, but all regions of the world were represented (Table 1).
The majority (63.8%) listed an academic institution as their primary workplace, while private practice with (14.2%) or without (15.6%) academic affiliation was the workplace of almost all others. A few were retired (3.9%), and some were hospital or government facility based (2.5%). Three-quarters of physicians were endocrinologists (76.4%), with surgeons (endocrine=8.5%; ENT=4.6%) representing the second most frequent specialty. The percentage of practice devoted to thyroid disease was more than half in the majority (56.4%) and less than 25% of their practice in 7.8% of respondents.
Dx-123I WBS
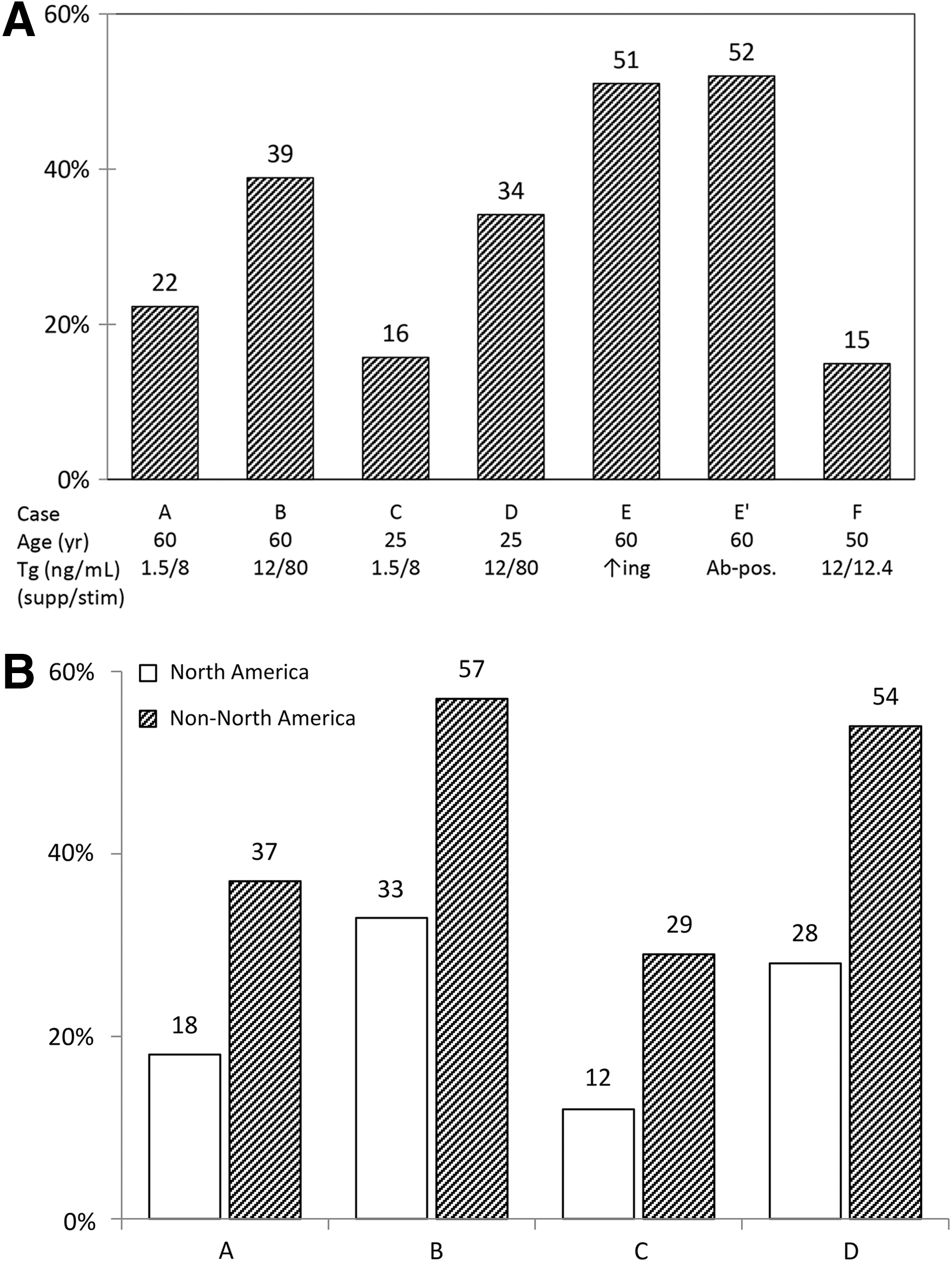
The effect of serum Tg on respondents' decision to give an empiric dose of 131I when the diagnostic WBS was negative is illustrated in Figure 1A. There appears to be an effect of serum Tg, either T4-suppressed or rhTSH stimulated, on whether patients received a treatment dose of 131I. Both Case A, an older man, and Case C, a young woman, were approximately twice as likely to be treated empirically when serum Tg (suppressed or stimulated) was higher (Case B and D respectively). The patient was most likely to receive 131I (51% would treat) when a low detectable T4-suppressed serum Tg of 1.5 ng/mL increased to 3.8 ng/mL (Case E) or the patient developed Tg antibodies (Case E′). Case F was a patient with a concerning suppressed Tg of 12 ng/mL but which did not increase after rhTSH. She was receiving a biologic response modifying antibody for rheumatoid arthritis and was at risk of developing heterophilic antibodies, which could interfere with the Tg assay (31). Despite the patient being over 45 years of age and having a moderately elevated serum Tg, only 15% of respondents recommended empiric 131I. For Cases A–D, non-North Americans recommended empiric 131I 73–142% more often than did North American respondents (Fig. 1B).
(
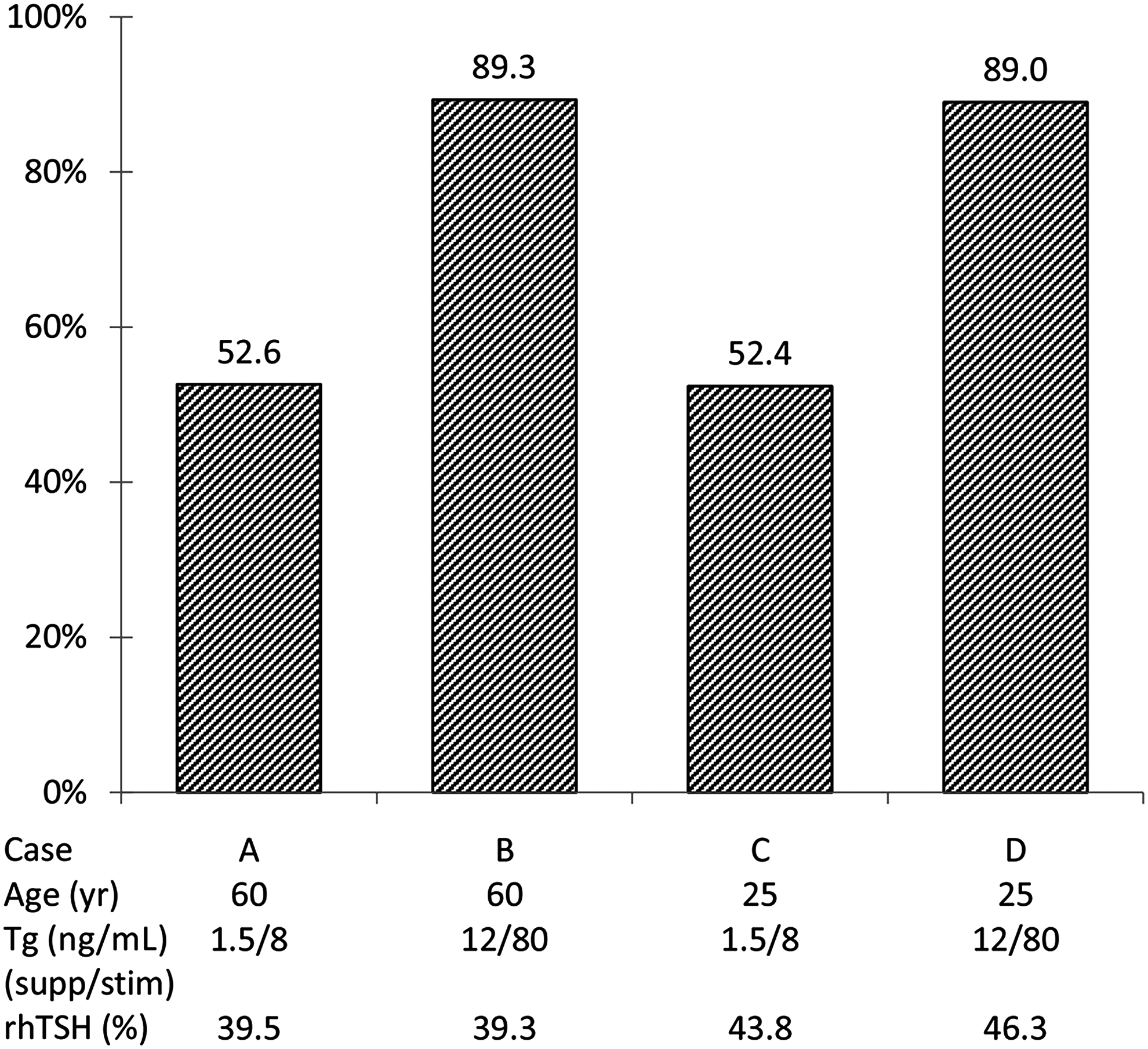
The selection of rhTSH versus withdrawal was similar in frequency and across case scenarios (Table 2). The vast majority (78–88%) chose a dose of 131I between 75 and 150 mCi, regardless of patient age or serum Tg level, while smaller doses were used in only 20% of the lowest risk (Case C) and only 5% of highest risk (Case B) patients (Fig. 2A).

(
rhTSH, recombinant human thyrotropin.
A low-iodine diet was recommended in 90.8% of patients using 131I in Case A. The duration was for one week in 27%, two weeks in 61%, and three to four weeks in 12%.
Neck US
The decision to use neck US in patients who did not receive empiric 131I after a negative DxWBS was almost universal, ranging from 97.5% to 100% in Cases A–D. For those patients with a negative neck US, respondents were queried as to whether they would then give empiric 131I therapy. In patients with this additional imaging information, the percentage who would receive empiric 131I was similar to therapy for negative DxWBS alone in Cases B–D, but was less in Case A (4% vs. 22%; Figs. 2B & 1A).
18FDG-PET/CT scan
Survey respondents were then asked if they would order a 18FDG-PET/CT scan if both the DxWBS and neck US were negative and an empiric dose of 131I was not given. Approximately half the time, patients with the lower Tg levels had further imaging, but this increased to almost 90% with the higher Tg levels independently of age (Fig. 3). Approximately 40% of clinicians would pretreat with rhTSH, with little variability across Cases A–D (Fig. 3).
Percentage of physicians who would recommend a 18FDG-PET/CT scan in 123I-DxWBS and neck US negative patients.
The final questions asked whether physicians would give an empiric 131I dose after 18FDG-PET/CT scan and if it mattered whether the scan was negative or positive (Fig. 4). The use of empiric 131I was much higher in patients with higher serum Tg (Cases B and D), and the presence or absence of 18FDG-PET positive lesions appeared not to influence the management. In contrast, patients with lower serum Tg (Cases A and C) were considerably less likely to receive empiric 131I, although those with PET positive scans would be treated more often (Fig. 4).
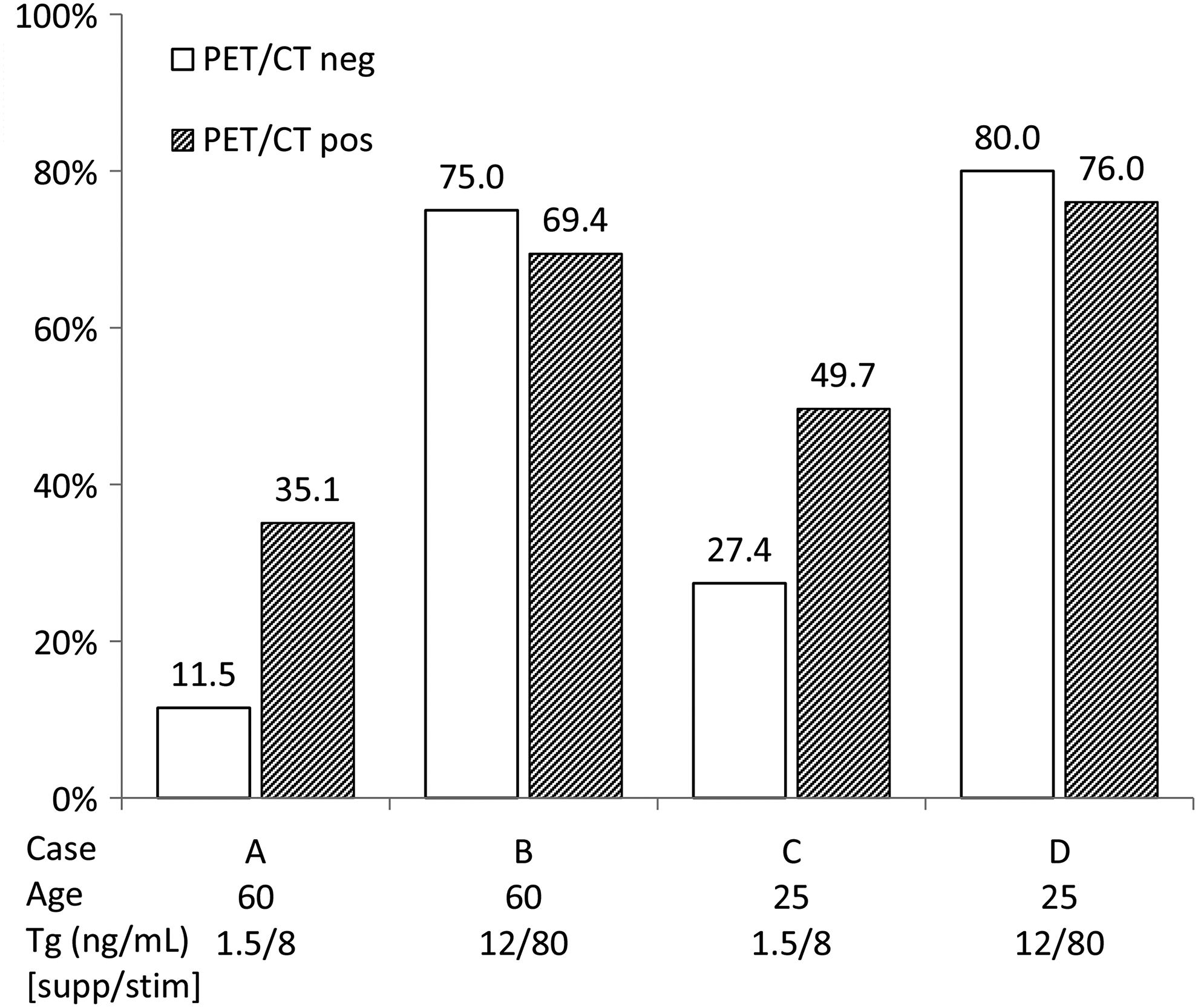
Percentage of physicians who would recommend empiric 131I therapy in patients with negative 123I-DxWBS and neck US: effect of 18FDG-PET/CT imaging.
Discussion
The development of a radioimmunoassay for serum thyroglobulin (Tg) led to the discovery that some patients with a history of differentiated thyroid cancer have detectable Tg levels after thyroidectomy and 131I ablation and a follow-up negative Dx-131I WBS, suggesting persistent or recurrent cancer (1). Subsequent reports demonstrated that more than half of such patients, if given an empiric therapeutic dose of 131I, had visible uptake on a post-therapy WBS, and the median percentage of positive scans was 57% (range 0–94%) (6 –16). Most lesions were in the cervical lymph nodes, but thyroid bed uptake (which could represent normal thyroid remnant) and distant metastases were also detected. Potential reasons for false negative diagnostic 131I WBS include: patient's TSH inadequately elevated or patient has recent excessive exogenous exposure, patient has small volume disease, or the tumor tissue is capable of producing Tg but has reduced efficiency of I− uptake. Alzahrani et al. (32) found in a multivariate analysis that only soft-tissue invasion predicted whether a patient would be Tg positive/WBS negative. Factors not associated included age, sex, duration of goiter, pressure symptoms, tumor size or multifocality, TNM stage, lymph node metastases, or 131I ablation dose (32). Reasons for giving an empiric dose of 131I include for disease localization and for therapeutic benefit (decrease in Tg and/or lesion size, or improved survival), although a reduction in Tg may reflect destruction of normal thyroid tissue. Reasons against its use are side effects (salivary gland injury, tear duct stenosis, second malignancy) and unproven benefit. In a review of 18 studies (17 in Ref. 33 and 1 in Ref. 22), empiric 131I reduced serum Tg in 193/349 (55%) of patients, but in six studies where no 131I was given (five in Ref. 33 and one in Ref. 22), Tg decreased during follow-up of <1 to 12.7 years in 111/261 (42%) of patients (22,33). In one long-term study, 31 of 42 patients had remission (defined as Tg <2 ng/mL), and the median Tg was 6.3 ng/mL at 13 months and decreased to <0.2 ng/mL at 72 months (32). Serum Tg can also decrease spontaneously in the absence of 131I ablation. Of 78 low-risk patients treated by surgery but no 131I, serum Tg was <0.2 ng/mL at 3–12 months in almost 60% and decreased to undetectable levels in another 19% by year 5 (34). Few studies have examined the effect of empiric 131I on structural distant metastases in Tg positive/DxWBS negative patients, but two found no evidence of tumor regression (10,35).
How did the survey respondents utilize empiric 131I compared to the literature? In the current survey, 22% and 16% of respondents chose to give empiric 131I when Tg-supp was 1.5 ng/mL and rhTSH stimulated Tg was 8 ng/mL, irrespective of the patient's age (Cases A and C). Higher Tg levels, either basal or stimulated (Cases B and D), led to recommending empiric 131I in almost twice as many patients (Fig. 1A). Only a few authors have suggested threshold Tg levels for administering empiric 131I. Schlumberger et al. (3) recommended 131I if Tg (on L-T4) >10 or (off L-T4) >40 ng/mL; Pineda et al. (5) used a Tg level of >8 ng/mL, and Koh et al. (11) used values of (on L-T4) >2 and (off L-T4) >10 ng/mL. The ATA management guidelines (36) suggest empiric 131I “might be considered” when Tg is ≥10 ng/mL (hypothyroid) or ≥5 ng/mL (after rhTSH) or Tg is rising, and when “imaging” (not defined) is negative (Recommendation 75).
The results of additional imaging beyond a diagnostic 123I-WBS suggest that a negative neck US (done almost universally in the survey if DxWBS was negative) had little effect or reduced the use of empiric 131I in patients with the lower Tg levels (Cases A and C; Fig. 2B vs. Fig. 1A). In contrast, empiric 131I was used slightly more often in both young and older patients when both DxWBS and neck US were negative and the Tg levels were higher (Cases B and D; Fig. 2B vs. Fig 1A). Of interest, the patient most likely to receive empiric 131I was one who had a rising serum Tg or developed a Tg antibody, even though DxWBS, neck US, and 18FDG-PET/CT were all negative. Ringel and Nabhan (37) recommend similar comprehensive imaging for a newly detected or rising Tg-Ab, but do not recommend empiric 131I therapy if all imaging is negative, except for high-risk patients. A recent position statement also recommends additional imaging looking for recurrence when Tg-Ab occurs (38).
Following the early experience relying only on DxWBS, additional imaging modalities have been utilized. Pacini et al. (21) reported a sensitivity of 96.3% for disease detection when using rhTSH stim-Tg and neck US, but only 20.5% using diagnostic 131I WBS alone. Many studies have evaluated the utility of PET or 18FDG-PET/CT scans, and a few have utilized CT imaging alone in detecting disease in the Tg positive/DxWBS negative patient. Issues pertaining to 18FDG-PET include: does the serum Tg level correlate with PET scan results? Is 18FDG-PET/CT more accurate than a PET scan alone? Does the presence or absence of PET activity affect whether a tumor will incorporate an empiric dose of 131I? Does TSH stimulation enhance PET uptake? Does a positive or negative 18FDG-PET/CT scan predict clinical outcome in this subset of thyroid cancer patients?
Before 18FDG-PET/CT fusion scans became routine, Schlüter et al. (23) found that PET scan-identified lesions were more likely to be true (rather than false) positive if serum Tg was >10 ng/mL. Bannas et al. (24) reported that 18FDG-PET/CT was more accurate if Tg-stim was >10 ng/mL, and Salvatore et al. (25) found 18FDG-PET/CT positive in 87% of patients if Tg was >100, but 53% if <10 ng/mL. Accuracy across modalities was 18FDG-PET/CT>PET+CT>PET>CT (26), and Leboulleux et al. (27) reported that the greatest number of lesions was detected by 18FDG-PET/CT, followed by CT, and then empiric 131I post-therapy WBS. In two meta-analyses, 18FDG-PET/CT was more sensitive than PET (28) and TSH-stimulated PET more sensitive than PET for both detecting patients with lesions and the number of lesions detected (30).
The ATA guidelines suggest considering a 18FDG-PET/CT scan if a post-treatment 131I scan does not identify disease and the unstimulated Tg is>10–20 ng/mL (Recommendation 78). Survey respondents frequently would order a 18FDG-PET/CT scan if both the DxWBS and neck US were negative. Serum Tg level, but not patient age, influenced their decision (Fig. 3). The ATA guidelines do not advise for or against TSH stimulation, but do indicate “TSH…may minimally enhance the sensitivity and specificity of 18FDG-PET/CT scanning” (36). Stimulation with rhTSH was common in the survey, with about 40% of respondents choosing this diagnostic modality (Fig. 3). Future studies should examine the cost-effectiveness of this method.
While 18FDG-PET/CT scans are useful in detecting disease in 131I-scan negative patients, does the imaging help prognostically or predict whether empiric 131I should be given? FDG-PET avidity and number of lesions are both associated with reduced survival (39). In one study, PET was predictive of outcome in patients with a Tg >1 ng/mL and negative post-therapy 131I WBS, with a five-year cause-specific survival of only 63% in PET-positive patients, but 100% in PET-negative subjects (29). The ATA guidelines do not provide recommendations on whether 18FDG-PET/CT imaging could aid in the decision to give empiric 131I. In the survey, a small percentage of respondents would treat if the serum Tg level was only 12 ng/mL after rhTSH and 18FDG-PET/CT was negative, but approximately 30–50% would be treated if the PET/CT scan was positive (Fig. 4; Cases A and C). In contrast, in patients who were 123I-DxWBS and neck US negative, and in whom a 18FDG-PET/CT scan was ordered, a large majority would be treated with 131I, irrespective of the 18FDG-PET/CT results if the Tg-supp is 12 and the Tg-stim is 80 ng/mL (Fig. 4; Cases B and D).
The presence of structural disease versus only biochemical disease appears to predict a greater likelihood of persistent disease, with incomplete biochemical responses more likely to be classified as no evidence of disease that does not prompt further therapy (40,41).
Conclusions
Empiric 131I continues to be utilized in patients in whom Tg is positive and scanning is negative. Both neck ultrasound and 18FDG-PET/CT are commonly used in this scenario, with the former being used most frequently. Use of empiric 131I appeared to correlate primarily with a higher degree of Tg elevation, the development of Tg antibodies, or a positive PET/CT in patients with low Tg levels (Cases A and C). Providers outside North America were more apt to utilize empiric 131I. A low iodine diet was typically used prior to 131I therapy, and a relative even split was noted between the use of rhTSH and thyroid hormone withdrawal prior to empiric 131I therapy or 18FDG-PET/CT scanning.
Footnotes
Acknowledgments
Financial support comes from a generous gift from Alfred D. and Audrey M. Petersen and NCI grant P30-CA015083-40 (Biostatistics and Survey Research Center Shared Resources). The authors wish to thank Kathleen Norton for manuscript preparation.
Author Disclosure Statement
No competing financial interests exist.