
Abstract
Background:
Excessive iodine intake is related to a higher prevalence of hypothyroidism, including subclinical hypothyroidism (SCH), in iodine-replete areas. This study aimed to evaluate the effect of iodine restriction on thyroid function in SCH patients in an iodine-replete area and analyze the relationship between serum thyrotropin (TSH) levels and iodine intake.
Methods:
The study consisted of 146 consecutive patients who were diagnosed with SCH at the Samsung Medical Center between 2010 and 2012. Urinary iodine concentration (UIC) was measured in 82 patients. Of these, 20 patients with UIC <300 μg/L were excluded, and 62 patients with UIC ≥300 μg/L were educated about the restriction of iodine-rich foods. Following the first follow-up visit, these patients were divided into two groups based on the UIC level: group A (well-controlled iodine intake, UIC <300 μg/L, n=40), and group B (poorly controlled iodine intake, UIC ≥300 μg/L, n=22). The remaining 64 patients did not restrict iodine rich foods (group C). The 82 patients with measured UICs were reevaluated every 3–6 months, and the median follow-up was 13 months (range 3–32 months). Thyroid function and UIC were measured at each visit. The correlation between serum TSH level and UIC was determined for the 82 patients in whom UIC was measured.
Results:
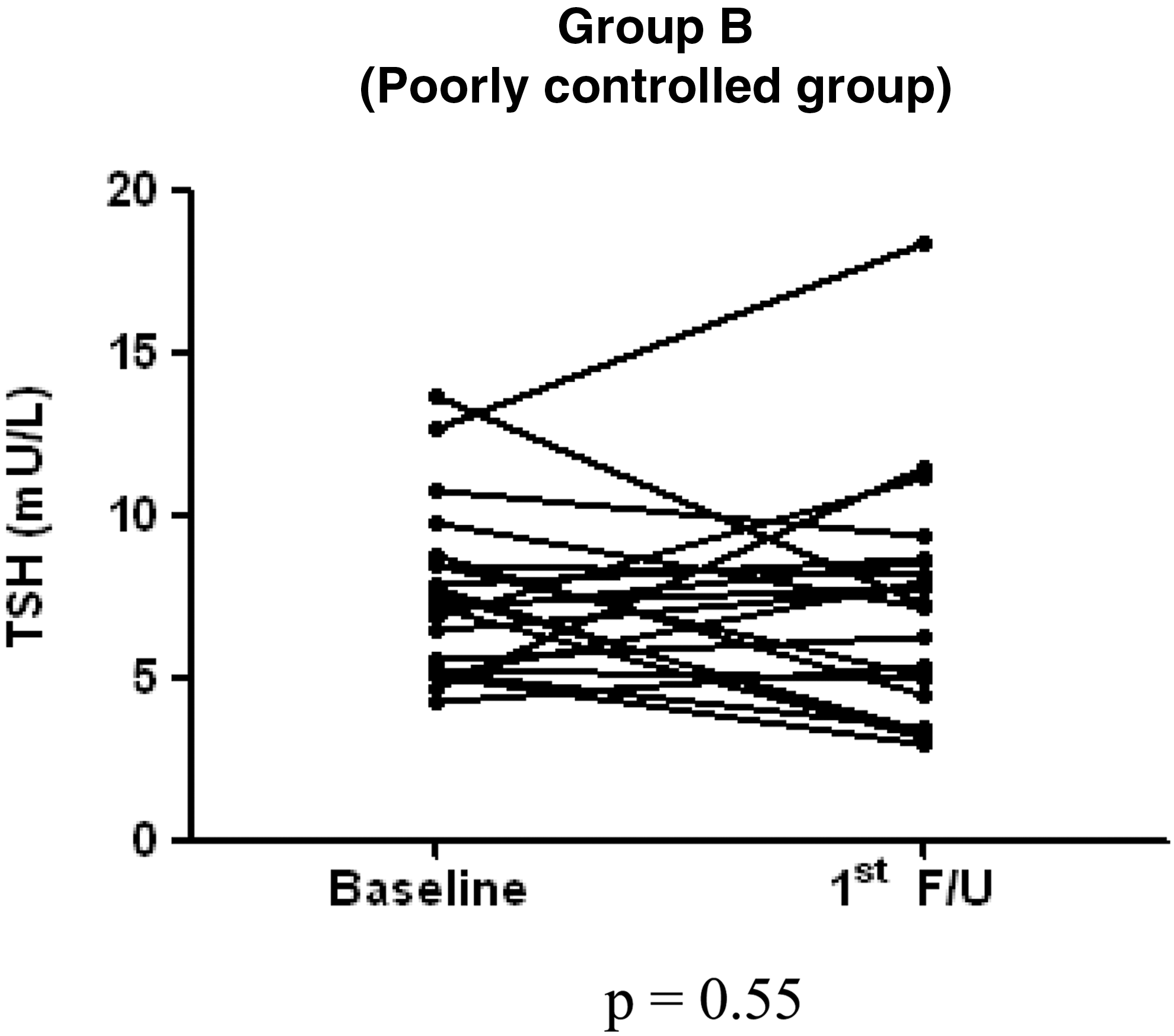
Following 3–6 months of iodine restriction, the serum TSH levels significantly decreased in group A (from 9.0 mU/L to 4.7 mU/L; p<0.01). In addition, the serum free thyroxine (T4) levels in group A significantly increased (from 1.11±0.23 ng/dL to 1.18±0.17 ng/dL; p<0.05). However, there were no significant changes in serum TSH or free T4 levels in groups B and C. Serum TSH levels significantly correlated with UIC (r=0.33, p<0.01).
Conclusion:
Iodine restriction may normalize or, at the very least, decrease serum TSH levels in SCH patients, and serum TSH levels are strongly correlated with UIC. Therefore, restriction of iodine intake could be a primary treatment option in SCH patients in an iodine-replete area.
Introduction
I
SCH is characterized by an elevated serum thyrotropin (TSH) level in conjunction with a normal free thyroxine (T4) level. SCH can develop into overt hypothyroidism and is associated with an increased risk of coronary heart disease and mortality (6). Therefore, the American Thyroid Association (ATA) and the American Association of Clinical Endocrinologists recommend thyroid hormone replacement in SCH in the following situations: serum TSH levels >10 mU/L; serum TSH levels between the upper limit of a given laboratory's reference range and 10 mU/L if patients have symptoms suggestive of hypothyroidism, positive anti-TPO antibodies, or evidence of atherosclerotic cardiovascular disease, heart failure, or associated risk factors for these diseases; and pregnancy (7).
As an excessive iodine intake could induce SCH in iodine-sufficient areas, iodine restriction may be effective as a primary therapeutic modality prior to the use of thyroid hormone replacement in patients with SCH. Studies have reported that iodine restriction can decrease serum TSH levels and reverse thyroid function to a euthyroid state. However, these studies were limited by small sample sizes and short durations (8,9).
Therefore, this study aimed at documenting the effect of iodine restriction on thyroid function in patients with SCH and analyzing the relationship between serum TSH levels and iodine intake during a long period of observation.
Methods
Subjects and study design
One hundred forty-six consecutive patients with SCH were enrolled from the thyroid clinic of the Samsung Medical Center in Seoul, Korea, between 2010 and 2012. SCH was defined as a serum TSH level of 4–20 mU/L with a normal free T4 level. Patients who met the criteria for SCH at least twice within an interval of 1–3 months were included. The exclusion criteria included overt hypothyroidism, a history of antithyroid drug or amiodarone use, pregnancy, renal failure, and recent use of iodine-containing contrast media.
The urinary iodine concentration (UIC) is an excellent biomarker of recent iodine intake and a recommended method to assess iodine status in the population because more than 90% of dietary iodine is excreted in the urine (10). Therefore, UIC was measured in 82 of the 146 patients to provide an index for recent iodine intake. Of these 82 patients, 20 who had a basal UIC <300 μg/L were excluded from the comparative study, which evaluated the effect of iodine restriction on thyroid function in the remaining 126 patients who were then divided into three groups. Those patients with UIC ≥300 μg/L (n=62) were informed of which iodine-rich foods to avoid: sea tangle or kelp, brown seaweed or sea mustard, laver, and green laver. Those patients with a well-controlled iodine intake (UIC <300 μg/L at the first visit following iodine restriction) became group A (n=40). Group B (n=22) included patients with a poorly controlled iodine intake (UIC ≥300 μg/L at the first visit), and group C (n=64) included patients who did not have to restrict iodine intake (Fig. 1). Group C was a control group to represent natural TSH changes and was evaluated for spontaneous recovery of thyroid function in SCH in the absence of any intervention. We also performed subgroup analysis according to baseline TSH levels.
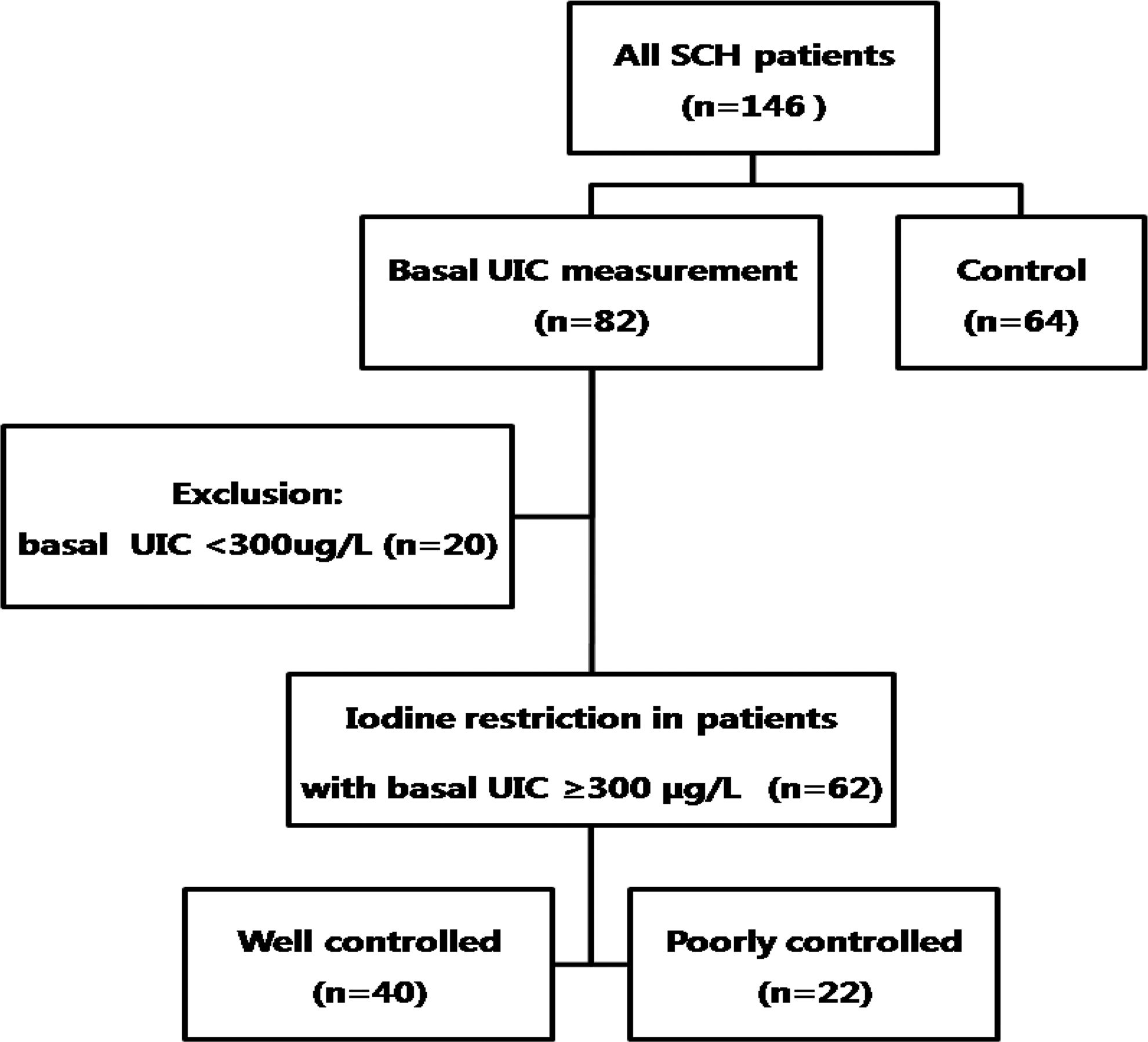
Enrollment of 146 patients with subclinical hypothyroidism.
Prior to the iodine restriction, serum triiodothyronine (T3), free T4, TSH levels, and titers of thyroid autoantibodies were measured at least twice within an interval of 1–3 months. The 82 patients with measured UICs were reevaluated for thyroid function (serum T3, free T4, TSH levels, and titers of thyroid autoantibodies) every 3–6 months, and the median follow-up duration was 13 months (range 3–32 months). These patients also had the UIC measured at each visit and were subsequently educated again about iodine restriction when UIC was ≥300 μg/L at the follow-up visits. We compared the changes in thyroid function between the three groups as a primary endpoint. Furthermore, to evaluate the relationship between thyroid function and iodine intake in SCH, we compared the correlation between serum TSH levels and UIC based on data from a long period of observation.
Laboratory assays
Serum TSH levels were measured using an immunoradiometric assay kit (Immunotech, Marseille Cedex, France). Serum T3 and free T4 levels were measured using a radioimmunoassay kit (FT4 RIA KIT; Immunotech). Serum titers of antithyroglobulin and anti-TPO antibodies were measured using a commercial radioimmunoassay kit (BRAHMS AG, Hennigsdorf, Germany). UIC was measured by inductively coupled plasma mass spectrometry using an Agilent 7500 series instrument (Agilent Technologies, Inc., Tokyo, Japan).
Statistical analysis
Data are expressed as median and range for the variables with a distribution that was not normally distributed or as mean±standard deviation (SD) for the variables with a normal distribution. One-way analysis of variance (ANOVA) and Kruskal–Wallis tests were used to compare the baseline characteristics between the three groups. The Wilcoxon signed-rank test and paired t-test were used to analyze the changes in thyroid function following iodine restriction. The effect of age and sex on thyroid function during the follow-up was assessed using linear mixed models for repeated measurements. To evaluate the relationship between thyroid function and iodine intake, Spearman correlation analysis was conducted with serum TSH levels and UIC in the 82 patients with UIC measurements. Statistical analyses were performed using SPSS v19.0 for Windows (IBM Corp., Armonk, NY). A p-value of <0.05 was considered statistically significant.
Results
Clinical characteristics of the SCH patients
The clinical characteristics of the 146 patients with SCH are provided in Table 1. Of the 146 patients, 43 (29.5%) were men, and 103 (70.5%) were women. The median age at the time of diagnosis was 55 years (range 20–86 years). Of the 82 patients with UIC measurements, 62 patients (76%) had excessive iodine intake according to the WHO criteria for assessing iodine (UIC ≥300 μg/L) (10).
Data are expressed as median (range), *mean±SD, or ** n (%).
†Hashimoto's thyroiditis was defined as the presence of goiter and serum anti-TPO antibody ≥60 U/mL or anti-Tg antibody ≥60 U/mL.
TSH, thyrotropin; T4, thyroxine; Tg, thyroglobulin; TPO, thyroid peroxidase; UIC, urinary iodine concentration.
The baseline clinical characteristics of the three groups are provided in Table 2. There were no significant differences between the three groups in terms of age, sex, serum free T4 level, titers of anti-TPO and antithyroglobulin antibodies, or the proportion of patients with Hashimoto's thyroiditis. However, the patients in group A had significantly higher initial serum TSH levels than those in groups B and C (9.0 mU/L, 7.2 mU/L, and 7.2 mU/L respectively; p<0.05).
Data are expressed as median (range), *mean±SD, or ** n (%).
†Group A (well-controlled iodine intake): UIC <300 μg/L following 3–6 months of iodine restriction; Group B (poorly controlled iodine intake): UIC ≥300 μg/L following 3–6 months of iodine restriction; Group C (no iodine restriction and no UIC measurement).
‡Hashimoto's thyroiditis was defined as serum anti-TPO antibody ≥60 U/mL or anti-Tg antibody ≥60 U/mL.
Tg Ab, thyroglobulin antibody; TPO Ab, thyroid peroxidase antibody.
Changes in thyroid function after short-term (<6 months) iodine restriction
Following 3–6 months of iodine restriction, the serum TSH levels in group A significantly decreased from 9.0 mU/L to 4.7 mU/L (p<0.01; Table 3 and Fig. 2). In addition, the serum free T4 levels in group A significantly increased from 1.11±0.23 ng/dL to 1.18±0.17 ng/dL (p<0.05). However, there were no significant changes in serum TSH or free T4 levels in either group B or group C (Table 3). There were also no changes in the titers of anti-TPO and antithyroglobulin antibodies in the three groups.
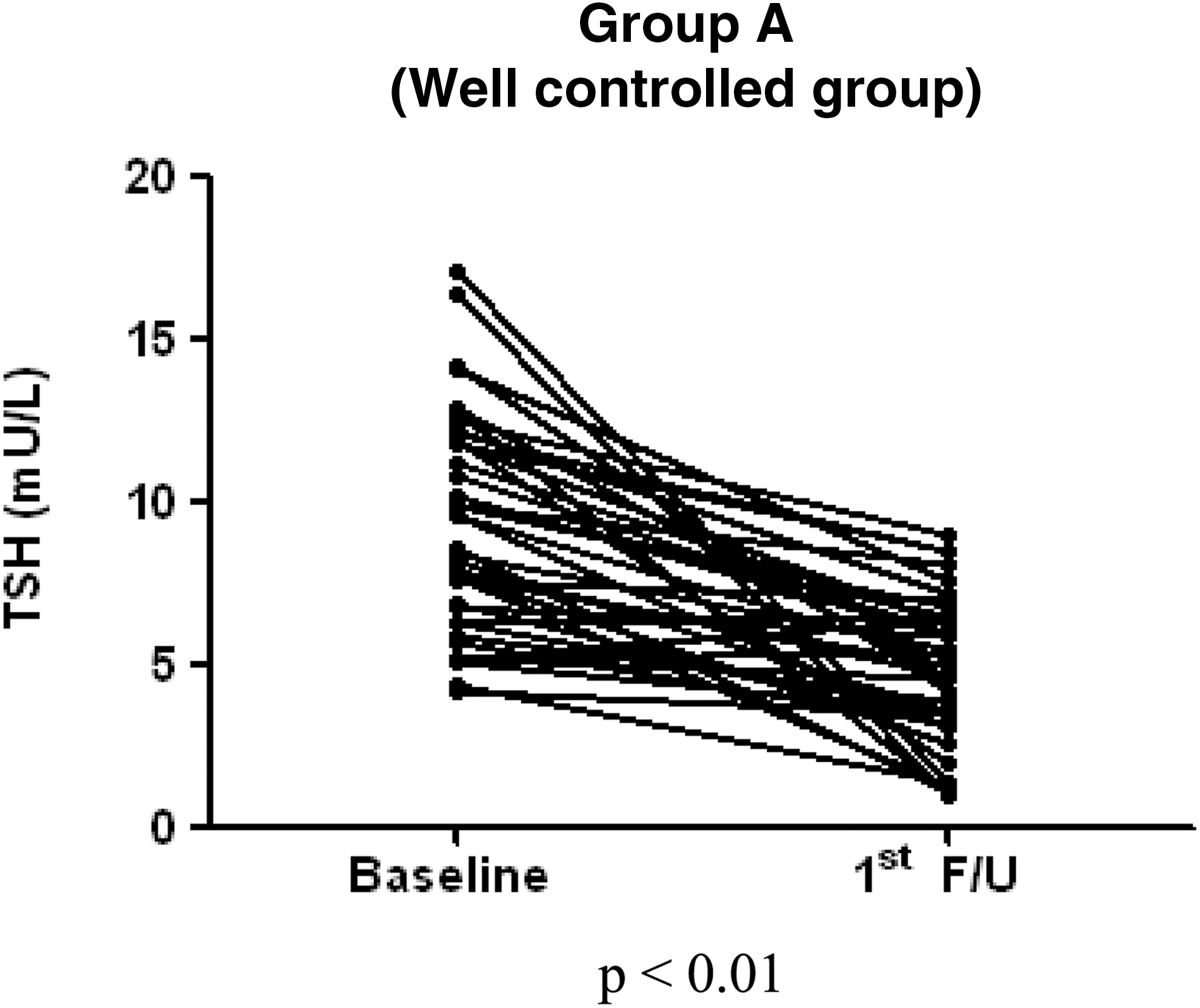
Changes in serum TSH levels in the 3 groups of patients with subclinical hypothyroidism at the first follow-up visit (3–6 months; n=126). TSH, thyrotropin.

Data are expressed as median (range), *mean±SD, or ** n (%).
†Group A (well-controlled iodine intake): UIC <300 μg/L following 3–6 months of iodine restriction; group B (poorly controlled iodine intake): UIC ≥300 μg/L following 3–6 months of iodine restriction; group C (no iodine restriction and no UIC measurement).
F/U, follow-up; NA, not assessed.
Among the patients with baseline TSH <10 mU/L (n=97), baseline serum TSH levels in group A (n=25) were not significantly different from group B (n=19) or group C (n=53; median TSH: 7.6, 7.1, and 6.7 respectively; p=0.66). After iodine restriction, serum TSH levels significantly decreased in group A (median TSH: 7.6 to 4.5; p<0.01). However, there were no significant changes in serum TSH levels in groups B or C. In patients with baseline TSH levels ≥10 mU/L (n=29), baseline TSH levels in group A (n=15) were similar to those in groups B (n=3) and C (n=11). After 3–6 months of iodine restriction, the serum TSH levels in group A significantly decreased (median TSH: from 12.2 to 6.0 mU/L; p<0.01). However, the serum TSH levels in groups B and C did not significantly decrease. Therefore, the serum TSH levels in group A significantly decreased in patients with serum TSH <10 mU/L, as well as in those with serum TSH ≥10 mU/L.
The results of the linear mixed models analysis indicated that TSH level changes were not influenced by sex (group A: p=0.283; group B: p=0.484; group C: p=0.207) or age (group A: p=0.632; group B: p=0.802; group C: p=0.830).
Correlation between serum TSH level and UIC
Eighty-two patients were followed up at an interval of 3–6 months, and their thyroid function and UIC were measured at each visit. The majority of the 82 patients with UIC measurements were followed up between three and seven times. When we analyzed the relationship between the serum TSH levels and UIC, the serum TSH levels significantly correlated with UIC (r=0.33, p<0.01; Fig. 3).
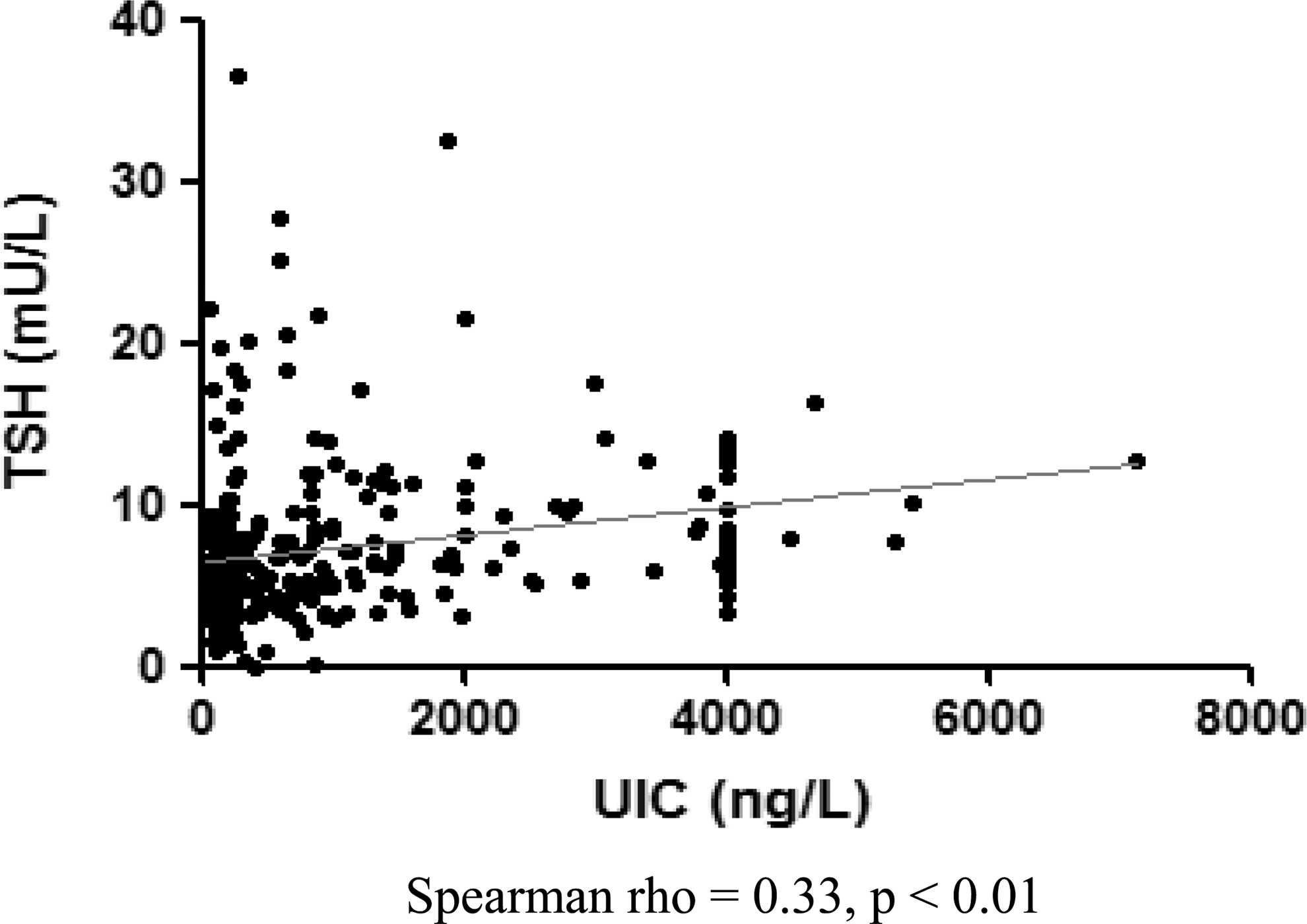
Correlation between serum TSH levels and UIC in patients with subclinical hypothyroidism (n=82) based on data from long-term follow-up. UIC, urinary iodine concentration.
Cases with fluctuating TSH levels similar to those of UIC
During the follow-up period, some patients recovered a euthyroid status following a period of iodine restriction. However, the serum TSH levels in some of these patients increased again when iodine intake was not controlled. Figure 4 displays fluctuating serum TSH levels in relation to UIC in two of these patients.
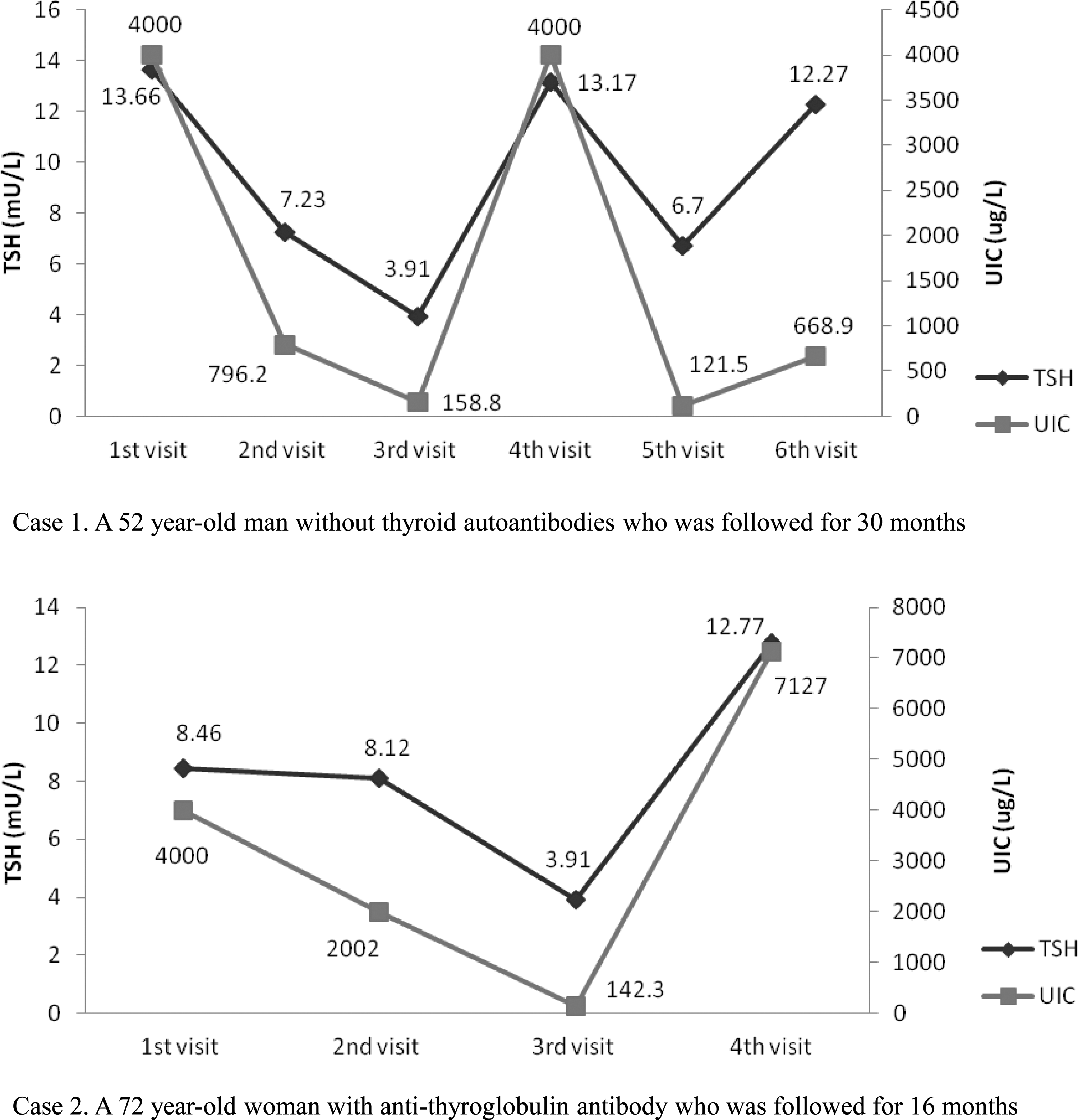
Two patients with subclinical hypothyroidism with fluctuating serum TSH levels related to changes in UIC.
Patient 1 was a 52-year-old man who was followed for 30 months. The initial UIC was 4000 μg/L, and the initial serum TSH level was 13.66 mU/L. Following the iodine-restriction diet, the UIC decreased to 158.8 μg/L, and the serum TSH level decreased to 3.91 mU/L. However, when the iodine intake was not restricted, UIC increased again to 4000 μg/L, and the serum TSH level also increased to 13.17 mU/L.
Patient 2 was a 72-year-old woman with a high titer of antithyroglobulin antibody who was followed for 16 months. The initial UIC was 4000 μg/L, and the initial serum TSH level was 8.46 mU/L. The serum TSH level decreased to 3.91 mU/L with a gradual decrease in UIC following iodine restriction. However, when the UIC increased to 7127 μg/L, the serum TSH level also increased to 12.77 mU/L (Fig. 4).
Discussion
The results of the present study demonstrate that, in patients with SCH, controlling iodine intake results in decreased serum TSH levels. There was also a strong correlation between serum TSH levels and UIC. Furthermore, we report that, in some patients, serum TSH levels fluctuate with UIC when monitored over a long period.
Despite a lack of nationwide data regarding the median UIC in Korea, a few studies have reported that the median UIC is higher than those recommended by the WHO (11 –13). Furthermore, Kang et al. reported that the estimated daily iodine intake in the Korean population is 1084 μg/day based on the Korean National Health and Nutrition Examination Survey data (14). Recently, Kim et al. evaluated the median UIC in 1072 Korean euthyroid subjects with benign thyroid nodules at the Samsung Medical Center; the patients had a median UIC of 358 μg/L (range 24–9224 μg/L; data not published). In the present study, the median UIC in patients with SCH was 997 μg/L, and 76% of the patients had an initial excessive iodine intake (UIC ≥300 μg/L). Compared to the euthyroid patients, the patients with SCH had a higher median UIC, which is consistent with previous studies reporting a relationship between excessive iodine intake and a higher prevalence of hypothyroidism, SCH, and autoimmune thyroiditis, especially in iodine-sufficient areas (3 –5). Teng et al. conducted a five-year prospective study to compare the incidence of thyroid disease in China in cohorts from three regions with different levels of iodine intake (5). They found that the cumulative incidence of overt hypothyroidism, SCH, and autoimmune thyroiditis was higher in subjects with an iodine intake that was more than adequate compared to those with a mildly deficient iodine intake.
Iodine intake varies depending on the region and individual dietary patterns. It is challenging, and sometimes impractical, to maintain a stringent iodine-restricted diet for a long period of time in a population with excessive iodine intake. Iodine-restricted diets over a long period can negatively affect a person's well-being and mental health (15). In the present study, the patients were educated about the foods that were not allowed. The major sources of dietary iodine in the Korean population are seaweed (66%), milk and dairy products (11%), and fish (9%) (12). Seaweed is easily available as a primary dietary source in Korea, with recent reports indicating that sea tangle or kelp, brown seaweed or sea mustard, laver, and green laver are the most iodine-rich foods in Korea (iodine content: 60,468–179,060 μg/100 g, 8730–11,600 μg/100 g, 527–3800 μg/100 g, and 2516 μg/100 g respectively) (14,16,17). The majority of Koreans use sea tangle or kelp as a basic ingredient in soup. In addition, Koreans traditionally consume brown seaweed soup during the early postpartum period as well as on birthdays. Therefore, the major foods that were not allowed in the present study included the following: sea tangle or kelp, brown seaweed or sea mustard, laver, and green laver.
The effect of iodine restriction on serum TSH levels in the SCH patients in the present study was consistent with previously reported results. Kasagi et al. evaluated the effect of iodine restriction on thyroid function in 33 hypothyroid patients in Japan and reported that 21 (64%) patients recovered from hypothyroidism following iodine restriction, and the reversibility of hypothyroidism was not significantly associated with Hashimoto's thyroiditis (8). Yoon et al. also reported that 18 out of 23 patients (78%) with hypothyroidism due to Hashimoto's thyroiditis returned to euthyroidism only with iodine restriction, and this recovery occurred within three months for the majority of patients (9).
Although previous studies have documented the effect of iodine restriction on thyroid function in patients with hypothyroidism, results are lacking regarding the sustainability of the euthyroid state in recovered patients. In the present study, we monitored UIC, which reflects recent iodine intake, every 3–6 months in 82 patients for a median of 13 months (maximum of 32 months). Although many patients attempted to reduce the intake of iodine-rich foods, UIC levels fluctuated at each visit. The serum TSH levels significantly correlated with UIC; similar results were reported by Alsayed et al. in 73 Egyptian women with autoimmune SCH, in whom a significant correlation between UIC and serum TSH levels (r=0.335, p<0.05) existed (18).
The exact mechanism of iodine-induced hypothyroidism is unknown. However, failure to escape from the acute Wolff–Chaikoff effect, which is the acute inhibition of the formation of organic iodine, has been thought to be the primary cause of iodine-induced hypothyroidism (19). If the administration of iodine continues, normal thyroid hormone synthesis resumes, resulting in an “escape” (or adaptation) phenomenon (20). This adaptation to the inhibitory effect of a large dose of iodide occurs through a decrease in sodium-iodide symporter (NIS) expression, which results in a decrease of the intrathyroidal iodide concentration that becomes insufficient to sustain the Wolff–Chaikoff effect (21). However, susceptible individuals might have an increased risk of failure to escape the acute Wolff–Chaikoff effect (22). For example, euthyroid patients with Hashimoto's thyroiditis have an increased susceptibility for iodine-induced hypothyroidism (23). Other risk factors include Graves' disease with euthyroidism after radioactive iodine therapy or thyroidectomy; subclinical hypothyroidism after postpartum thyroiditis, amiodarone-destructive thyrotoxicosis, hemithyroidectomy for benign nodules, or previous interferon-α therapy; and concomitant use of potential goitrogens, such as lithium (24). Excess dietary iodine can slow thyroid hormone secretion in normal, euthyroid individuals, at least on a short-term basis (25). Reduced intrathyroidal deiodinase activity as a result of iodine load could decrease synthesis of thyroid hormones (26). Another possible mechanism for iodine-induced hypothyroidism is the potential damaging effect of excessive iodine on endogenous thyroid peroxidase and apoptosis of thyroid follicular cells. However, this theory has not been well established (27 –29).
High levels of iodine exposure have been reported to initiate and exacerbate lymphocyte infiltration of the thyroid gland, resulting in autoimmune thyroiditis in experimental animals (30,31). In the present study, thyroid autoantibody levels were similar in all three groups, and there was no detectable alteration in thyroid autoantibody levels in any of the groups, even the group with poorly controlled iodine intake. It is possible that 3–6 months is too short to initiate or enhance thyroid autoimmunity, and daily variation in dietary iodine may act as a confounder. It has been previously demonstrated that patients with Hashimoto's thyroiditis develop hypothyroidism after daily ingestion of a potassium iodide solution (23). Furthermore, a significant correlation between UIC and titers of anti-TPO antibodies has been reported in autoimmune SCH (r=0.296, p<0.01) (18). Therefore, an increased susceptibility to iodine may exist in patients with preexisting thyroid autoimmunity. In the present study, 38 of 82 patients with measured UIC had Hashimoto's thyroiditis, and 14 of these 38 patients (37%) had an initial excessive iodine intake (UIC ≥300 μg/L). Although an association between UIC and titers of anti-TPO antibodies has been previously reported in patients with Hashimoto's thyroiditis, a similar relationship with titers of anti-TPO antibodies was not detected (p=0.916). However, titers of antithyroglobulin antibodies correlated with UIC in our study (r=0.296, p<0.01). While the patients with Hashimoto's thyroiditis in group B (n=9) did not experience a significant change in thyroid autoantibody titers, the patients with Hashimoto's thyroiditis in group A (n=15) experienced a significant decrease of antithyroglobulin antibodies titers after iodine restriction (median: 100.40 U/mL to 90.30 U/mL, p<0.05). This observed difference might be explained by the small sample size.
SCH is an independent risk factor for coronary heart disease. Levothyroxine is the drug of choice for the treatment of SCH, especially in SCH patients with hypothyroidism symptoms and the presence of risk factors for cardiovascular disease. However, serum TSH levels may normalize spontaneously in patients with SCH, and excessive iodine intake could accelerate the progression to overt hypothyroidism. Therefore, prior to thyroid hormone replacement therapy, restriction of iodine intake could be considered as a primary therapy. In iodine-sufficient areas, we recommend that all SCH patients should have their iodine intake initially evaluated, and iodine restriction could be tried if excessive iodine intake is suspected. Levothyroxine therapy should be considered if the patient has poor compliance with iodine restriction or the thyroid function does not recover, which then requires thyroid hormone replacement according to the ATA guidelines (7). In the present study, we discovered that, even in patients who recovered to a euthyroid status following iodine restriction, thyroid function can decline with an increase in UIC. Therefore, we recommend regular evaluation of the thyroid function even in patients who have recovered to the euthyroid state following iodine restriction.
This study has certain limitations. First, this study enrolled a specific group of patients with SCH in an in an iodine-replete area, and the effect of iodine restriction on thyroid function was clinically modest. Second, in group C (n=64), UIC was not measured. However, the patients in group C were enrolled to evaluate the spontaneous recovery of thyroid function in SCH in the absence of an intervention and to compare with those who restricted iodine intake.
To the best of our knowledge, this is the first study to evaluate the relationship between iodine intake and thyroid function in patients with SCH over a long period of time. Furthermore, this study included a larger sample of patients with SCH than did previous studies.
In conclusion, iodine restriction may decrease serum TSH levels in SCH patients. In addition, serum TSH levels strongly correlated with UIC. Therefore, restriction of daily iodine intake could be a treatment option in patients with SCH in an iodine-sufficient area.
Footnotes
Author Disclosure Statement
No competing financial interests exist.