
Abstract
Background:
A 3-tiered system has been proposed by radiologists for the reporting and workup of incidental thyroid nodules (ITN) detected on computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography/computed tomography (PET/CT). It has been shown to reduce the workup rate, but there remains concern about missed malignancies. This study aims at estimating the proportion of incidental cancers that would be missed relative to all thyroid cancers if the 3-tiered system were applied to ITN seen on CT, MRI, or PET/CT. We also aim to characterize these missed incidental cancers by histology and tumor stage.
Methods:
A retrospective review was performed of 680 consecutive patients with thyroid cancer who underwent surgery between January 2003 and December 2012. Medical records were reviewed to identify incidental thyroid cancers detected on imaging. Patients with incidental cancers detected on CT, MRI, or PET/CT were categorized according to the system as 3-tiered system-positive and 3-tiered system-negative. The system recommends that only 3-tiered system-positive ITN undergo further workup with ultrasound. Three-tiered system-negative cancers were the cancers that would have been missed if the system were used in practice. These tumors are described by tumor type, size, and stage to determine the potential impact if the 3-tiered system were adopted.
Results:
One hundred and one patients had imaging-detected incidental cancers, of whom 64 met the inclusion criteria and were originally detected on CT, MRI, or PET/CT. Eight were 3-tiered system-negative, which represents 13% of the 64 incidental cancers that could be categorized and 1.2% of all thyroid cancers treated at our institution in the 10-year period. Three-tiered system-negative tumors were all papillary in histology and had a median size of 12 mm (interquartile range 10–12 mm). Six tumors (75%) were American Joint Committee on Cancer (AJCC) stage I, one was AJCC stage II, and one was AJCC stage III at diagnosis.
Conclusions:
Based on thyroid cancers diagnosed during a decade, incidental malignancies missed by the 3-tiered system represent 1.2% of all thyroid malignancies. Three-tiered system-negative incidental cancers were all small papillary cancers. Given that few cancers would be missed and most are less aggressive, we propose that the 3-tiered system could be adopted in clinical practice to guide the workup of ITN identified on CT, MRI, and PET/CT.
Introduction
I
Recently, Hoang et al. proposed a categorization method for guiding the evaluation of ITN detected on CT, MRI, or PET/CT (1,6,7). The system was intended for radiologists who have limited clinical history available to them at the time of reporting the study. The method is a 3-tiered system and is based on the patient's age and the imaging findings. According to the 3-tiered system, further workup with ultrasound should be considered for three groups (tiers): (i) nodules with certain imaging features deemed to be high risk (suspicious lymph nodes, local invasion, or any discernable focal metabolic activity on PET); (ii) nodules in patients aged <35 years; and (iii) nodules ≥15 mm in patients aged ≥35 years. The nodule size and age cutoffs for the 3-tiered system were based on existing ultrasound guidelines and a review of the current literature specific to thyroid nodules seen on CT, MRI, and PET/CT (4,5,7,8).
The performance of any set of guidelines is judged by its false-positive and false-negative rates, that is, how many benign nodules would receive unnecessary workup and how many cancers would be missed. In two retrospective studies, the 3-tiered system was found to reduce false-positive cases (1,6). Compared to an academic institution's clinical practice without specific guidelines, there was a 35% reduction in ITN workup with the 3-tiered system (6). Compared to a 1 cm size cutoff, there was a 46% reduction in ITN workup with the 3-tiered system (1). There were no false negative cases (missed cancers) with the 3-tiered system in either study, perhaps because the two study populations had a small number of malignancies (1,6). However, in a sample with a larger number of thyroid malignancies, it is likely that the proposed 3-tiered system categorization method would result in some false-negative cases, and so it would be valuable to gauge the types of cancers that might be missed if the 3-tiered system were widely adopted.
The aim of this study is to estimate the proportion of incidental cancers that would be missed relative to all thyroid cancers if the 3-tiered system were applied to ITN seen on CT, MRI, or PET/CT. We also aim to characterize these potentially missed cancers (3-tiered system-negative) by histology and tumor stage. These aims were achieved by retrospectively applying the 3-tiered system to cancers diagnosed during a decade that were initially detected incidentally on CT, MRI, or PET/CT studies at our institution. Our hypotheses were that 3-tiered system-negative incidental malignancies comprise a minority of surgically treated thyroid cancers and overall are less advanced. These findings, along with existing studies using the 3-tiered system (1,6), could support adoption of this categorization method in clinical practice to guide evaluation of ITN identified on CT, MRI, and PET/CT.
Materials and Methods
Study group
We performed a retrospective study of 2090 consecutive patients who underwent thyroidectomy or lobectomy between January 1, 2003, and December 31, 2012, at a single large academic institution to identify patients with cancers that were detected on CT, MRI, or PET/CT. The patient population was obtained through surgical Current Procedural Terminology (CPT) codes for thyroid lobectomy and thyroidectomy (see Appendix). Among 2090 patients, 680 had a diagnosis of thyroid cancer on the final surgical pathology specimen (Fig. 1). The medical records of these 680 patients were reviewed to determine if the cancers were discovered initially based on clinical findings or as an incidental discovery on imaging. This study was approved by the Institutional Review Board and was compliant with the Health Insurance Portability and Accountability Act (HIPAA).
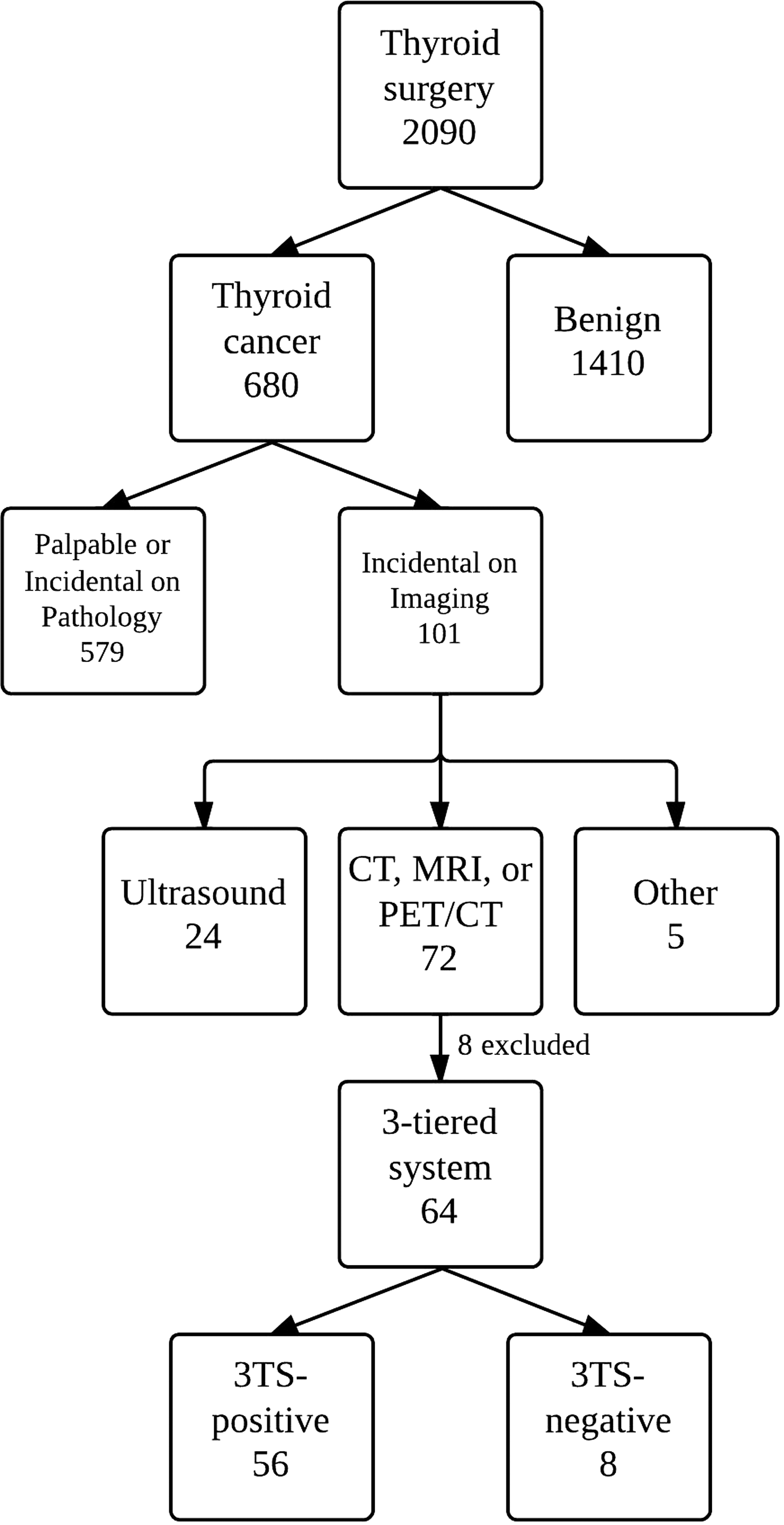
Flowchart of study subjects. 3TS-positive, 3-tiered system criteria–positive thyroid cancer; 3TS-negative, 3-tiered system criteria–negative thyroid cancer.
Definitions of incidental cancer
An “incidental cancer on imaging” was defined as a cancer that was originally detected on imaging studies performed for other reasons in patients without any clinical symptoms, examination findings, or suspicion for thyroid cancer. In this study, we were primarily studying patients with incidental cancers on CT, MRI, or PET/CT, but also evaluated the rate of incidental cancers detected on other imaging modalities. Cancers were not considered to be incidental if imaging was performed for a palpable nodule/mass (representing the primary or nodal disease), or if a dedicated thyroid ultrasound was performed for thyroid-related symptoms, including abnormal thyroid function tests and clinical risk factors defined by the ATA (4).
The patients with incidental cancers had surgery because they all presented with ITN that had a subsequent biopsy with cytology results that warranted thyroidectomy or diagnostic lobectomy. Cytology results that led to surgery were follicular neoplasm, suspicious for malignancy, or consistent with malignancy (9).
Medical records were also reviewed for demographic information (patient age and sex); clinical features, including the risk factors for thyroid cancer; and pathologic characteristics, including tumor histology, size, and American Joint Committee on Cancer (AJCC) stage.
Application of the 3-tiered system
The 3-tiered system was applied retrospectively to the group of patients with incidental cancers detected on CT, MRI, and PET/CT because the categorization method only applies to these imaging modalities. The 3-tiered system had not been implemented at our institution at the time of the study, so we were retrospectively comparing the outcomes of previous clinical practice to the outcomes had the 3-tiered system been adopted by radiologists. Patients were excluded if imaging studies and full radiology reports were not available for review, or if the patient had active metastatic disease from another known primary tumor or risk factors for thyroid cancer as described by the ATA (4). The latter exclusion criteria were applied because the 3-tiered system is intended for the management of ITN (asymptomatic thyroid nodules) in low-risk patients.
For application of the 3-tiered system, the original CT, MRI, or PET/CT imaging studies were reviewed independently by two radiologists (with seven and three years of experience). Patients who did not have images were still included if they had a full radiology report in the medical records that included comments about nodule size and status of lymph nodes. The imaging studies were reviewed for the following three risk categories of the 3-tiered system.
Risk Category 1 (highest risk) includes patients with concerning findings such as local invasion, suspicious lymph nodes, focal metabolic uptake on PET, and distant metastases. Suspicious lymph nodes were defined as nodes >10 mm in short axis (with the exception of jugulodigastric lymph nodes, which were permitted to be up to 15 mm in the short axis), or nodes that contained either calcifications, cystic components, or irregular margins.
Risk Category 2 includes patients <35 years of age who do not meet criteria for Risk Category 1. This age-group cutoff was selected because young patients have a higher ratio of malignant to benign nodules in prior studies (8,10 –14). A recent study also shows a slightly higher risk of tumor progression in young patients with subclinical low-risk papillary thyroid cancer who undergo observation rather than surgery (15).
Risk Category 3 includes patients aged ≥35 years with nodule size ≥15 mm who do not meet criteria for Risk Category 1. The 15 mm cutoff for Risk Category 3 is intended to reflect a higher size threshold for workup of nodules that lack aggressive imaging findings or demographic risk factors. A 15 mm size cutoff has also been used by several groups for ultrasound guidelines (5,16). In patients with multiple nodules, the side and quadrant of the thyroid cancer were noted from the surgical and pathology report. The size on pathology was correlated with the nodules in the corresponding quadrant on CT or MRI to obtain the imaging diameter for the best-matched nodule.
The categories represent descending levels of risk. Patients meeting the criteria for any of the three risk categories were considered to be patients who needed the incidental finding to be reported in the impression of the radiology report so that the clinician could consider further workup by ultrasound based on clinical information. Nodules not meeting any of the 3-tiered criteria comprised the subgroup that would not have been reported in the impression of the radiology report and would not have undergone workup if the system had been used during the study period. Identifying 3-tiered negative cancers allowed us to determine the number of missed malignancies that would occur and characteristics of missed malignancies if the 3-tiered system were applied to ITN on CT, MRI, or PET/CT studies.
Outcome measures and statistical analysis
After application of a 3-tiered system to incidental cancers that met inclusion criteria, we calculated the proportion of 3-tiered system-negative cancers among incidental cancers and all thyroid cancers. The 3-tiered system-negative cancers were described according to patient demographics, tumor histology, size, and AJCC stage. The data were entered into a Microsoft Excel spreadsheet (2007 version; Microsoft, Redmond, WA). Statistical analyses were performed using SAS Enterprise (v4.2; SAS Institute, Cary, NC).
Results
Study group
In the 10-year study period, there were 680 patients with thyroid cancer; of these, 101 (15%) had incidental cancers that were identified on imaging (Fig. 1). The mean diameter of incidental cancers on imaging was 21 mm (SD=10 mm), which was larger than their mean size on pathology of 16 mm (SD=13 mm). Among the patients with cancers incidentally identified on imaging, the modalities responsible for detection were CT (37/101, 37%), PET/CT (27/101, 27%), ultrasound (24/101, 24%), MRI (8/101, 8%), plain radiographs (3/101, 3%), nuclear medicine octreotide scan (1/101, 1%), and echocardiography (1/101, 1%). Thus, there were 72 patients with tumors initially detected on CT, MRI, or PET/CT who were eligible for retrospective evaluation of the 3-tiered system.
Application of the 3-tiered system
Categorization according to the 3-tiered system was possible in 64 of 72 patients. Six patients were excluded because they did not have available imaging or radiology reports. Two patients with widely metastatic, nonthyroid malignancies were excluded because these were not considered to be low-risk patients with ITN. In the remaining 64 patients, 56 patients had imaging available for review, and eight patients had complete radiology reports in their records.
Table 1 illustrates the distribution of the 64 cancers in each of the 3-tiered categories. The two radiologists agreed on all cases for assignment to the categories. Notably, 13% (8/64) of patients did not meet criteria for the 3-tiered system and would not have proceeded with sonographic workup had the criteria been applied at the time of initial imaging. Overall, the 3-tiered system-negative group of incidental thyroid cancers represented 1.2% (8/672) of all thyroid cancers. The total number of patients with cancer was 672 because we excluded eight patients from 680 patients who could not be categorized according to the 3-tiered system (Fig. 1).
Eight patients excluded from 72 patients because they could not be categorized by the 3-tiered system.
There were no deaths among the eight 3-tiered system-negative patients over a median follow-up time of 16.5 months (interquartile range 11.3–27.8 months). All of these 3-tiered system-negative patients had images available for review. The median size of the 3-tiered system-negative cancers was 12 mm (interquartile range 10–12 mm) on imaging, and they were all papillary thyroid cancers (Table 2). One patient had nodal metastases to the central compartment (N1a) that were not appreciated on imaging but were present on surgical pathology from a central lymph node dissection. None of the 3-tiered system-negative patients had lateral compartment nodal metastases (N1b). All 3-tiered system-negative patients were stage I at diagnosis except for one who was stage II because of the combination of age >45 years and a tumor size of >2 cm (age 64 years, T2N0M0), and one who was stage III because of the combination of age >45 years, extrathyroidal extension into the perithyroidal soft tissues (not appreciated on CT), and a central compartment nodal metastasis (age 51 years, T3N1aM0).
Extrathyroid extension to the perithyroid soft tissues (not appreciated on CT) was detected at surgery.
Discussion
A 3-tiered system has been proposed as a categorization method for radiologists to reduce the workup of benign ITN seen on CT, MRI, or PET/CT (1,6,7). The 3-tiered system is based on patient age, nodule size, and associated suspicious imaging findings. According to this categorization method, workup would not be recommended for patients aged ≥35 years with an indeterminate thyroid nodule <15 mm. This study estimates the worst-case scenario from the perspective of missed malignancies if the 3-tiered system had been adopted in practice for ITN seen on CT, MRI, and PET/CT. We demonstrate that the cancers that would be missed by the 3-tiered system represent only 1.2% of all thyroid cancers and that all missed incidental cancers were small papillary thyroid cancers.
It may seem unusual for a study to evaluate proposed guidelines for ITN workup in a population consisting entirely of patients with cancer. Ideally, the evaluation of guidelines should be performed with a large population of patients with benign and malignant nodules with sufficient follow-up to allow disease to manifest. For ITN and thyroid cancer, however, there are barriers to the “ideal” research design because malignancy is rare, and most small cancers have an indolent course and may even remain entirely subclinical over the course of the patient's lifetime (17,18). Based on current literature, it would require enrollment of up to 100 patients with benign ITN for each case of malignancy and follow-up periods of up to 10 years to demonstrate sufficiently the natural history of ITN (17,19). Two previous studies evaluating the 3-tiered system did have populations consisting of patients with benign and malignant nodules; they were patients with consecutive ITN seen on CT and patients undergoing ultrasound-guided FNA for nodules initially detected on CT, MRI, or PET/CT (1,6). These studies found that the 3-tiered system had the potential to reduce radiographic and endocrinologic workup by 35–46% without missing a malignancy. However, these studies were limited by their inclusion of only six patients with cancer (1,6).
The present study fills a gap in knowledge by studying the 3-tiered system in a large population of patients with incidental malignancies detected on imaging. The overall intention was to provide the worst-case scenario for radiologists and clinicians who adopted the 3-tiered system in their practice and to address the underlying fear of operating under the premise of false-negative results and, therefore, the potential for delayed cancer diagnosis and medico-legal ramifications. The worst-case scenario in our institution appears to be that eight thyroid cancers would have been missed over 10 years if the 3-tiered system were adopted by radiologists for incidental cancers initially seen on CT, MRI, and PET/CT. Incidental thyroid cancers not meeting the 3-tiered system criteria represented 1.2% of all thyroid cancer patients that underwent surgery. This is not the false-negative rate of the system, which will be discussed later, but this proportion gives perspective on the impact of using the 3-tiered system on overall cancer diagnoses. Furthermore, incidental malignancies that were 3-tiered system-negative were all small papillary thyroid cancers, and there was only one case of an N1a nodal metastasis and one case of early extrathyroidal invasion. Absence of other thyroid histologies among 3-tiered system negative tumors could represent undersampling, but may also reflect the behavior of nonpapillary thyroid malignancies. On average, they are more aggressive than papillary carcinoma and likely to be larger at presentation and, thus, more likely to be 3-tiered system-positive. None of the eight 3-tiered system-negative patients died in the follow-up period, and it remains unknown if they would have remained subclinical if left undiagnosed and untreated.
This study demonstrates that when the proposed 3-tiered system was applied to incidental cancers seen on CT, MRI, and PET/CT, the false negative rate was 13%. Although some may regard 13% as a high percentage of missed cancers, it is important to appreciate that the system is intended only for subclinical incidental thyroid nodules seen on CT, MRI, and PET/CT. This group consists of mostly benign thyroid nodules, and current practices of selection for workup have low specificity and low positive predictive value (6). It is also relevant to compare this false-negative rate of 13% to other existing imaging guidelines. The BI-RADS guidelines for reporting screening mammography misses up to 8% of breast cancers, which are considered to be “probably benign,” and a recent study demonstrated that the Society of Radiologists in Ultrasound (SRU) recommendations for thyroid fine-needle aspirations are associated with a false-negative rate of 18% for incidental cancers (20 –22).
The disadvantages of a missed cancer with the 3-tiered system should be weighed against two important benefits: improved standardization of radiology reports and reduced false-positive results, leading to fewer subsequent evaluations resulting in benign outcomes. This potentially translates into more consistent patient care, less anxiety for patients, and savings in healthcare costs from unnecessary ultrasounds, biopsies, and potentially diagnostic surgeries. Finally, the natural history of thyroid cancer should be considered when using the 3-tiered system. Thyroid cancer is generally less aggressive than other primary cancers, such as breast, prostate, and lung. Small papillary thyroid cancers are associated with an excellent prognosis. According to the 2009 Surveillance, Epidemiology, and End Results Program (SEER) database, the 10-year survival rate for a 10–14 mm thyroid cancer is 99.6% without nodal metastases and 98.9% with nodal metastases (3). Thyroid cancer may also remain subclinical, such that many patients die with, rather than from, thyroid cancer, which was demonstrated in one postmortem study in which small foci of thyroid cancer were present in the thyroid glands of 36% of patients who died from other causes (18).
As for any categorization method for workup, there are fundamental limitations of the 3-tiered system and reasons for specific criteria. First, the system does not consider patient risk factors because the system is intended for asymptomatic patients without risk factors. Patients with risk factors should not be classified with the 3-tiered system. Patient sex is not addressed by the 3-tiered system, but this is in keeping with all thyroid guidelines based on sonographic criteria; none of these guidelines applies different criteria to men and women (4,5).
The risk factor of age was addressed with the 3-tiered system; it is notably different from the AJCC thyroid cancer staging system, which uses an age cutoff of 45 years (23). The age cutoff in the 3-tiered system is not based on prognosis of missed cancers, but based on previously published literature showing a higher rate of malignancy in patients aged <35 years who had an ITN detected on CT (8). It would also seem cost-effective to have a lower threshold for workup in younger patients because these patients less frequently have imaging and comprise only a small proportion of patients with ITN (1,6). Finally, it may be more important to diagnose an asymptomatic cancer in a younger patient. A recent study found a slightly higher risk of tumor progression in young patients (defined as aged <40 years) with subclinical, low-risk papillary thyroid cancers who undergo observation rather than surgery (15).
It is also useful to address the rationale behind the 15 mm size cutoff in patients aged ≥35 years. The 3-tiered system aims to reduce the workup of benign ITNs while capturing malignancy if clinically significant. Thus, the larger size cutoff was applied to older patients without other concerning imaging features. We believe that the 15 mm cutoff is in keeping with many existing sonographic guidelines. The ATA guidelines for ultrasound criteria recommend workup in solid and iso-/hyperechoic nodules ≥10–15 mm in diameter. The SRU recommend workup for solid nodules ≥15 mm. Recently, a large population based case-control study found nodule size of 20 mm to be a better predictor of malignancy in a thyroid nodule seen on ultrasound (17).
There are several limitations to this study. First, this is a retrospective study performed at a single institution, which may differ from other institutions with regard to the reporting and workup of thyroid nodules detected on CT, MRI, and PET/CT (24). We suspect that our radiology reporting practices could result in fewer incidental cancer diagnoses than at other institutions. Second, we chose to include patients without imaging for review but who still had full radiology reports. We recognize that the radiology reports were interpreted by just one radiologist, and patients with imaging for review were evaluated by two radiologists who focused on specific criteria. However, these reports were issued by nationally board-certified radiologists, and the radiology reports were detailed, containing all the essential information needed to apply the 3-tiered system, including suspicious findings on imaging, patient age, and thyroid nodule size. Miscategorization was possible if important criteria in the 3-tiered system were missed on the outside reports. However, it was reassuring that all patients with only radiology reports were 3-tiered system-positive. Finally, we may be underestimating the false negative rate of the 3-tiered system, since there may be cases of subclinical malignancy in ITN that did not undergo workup. However, these cases are more likely to have an indolent natural history.
This study quantifies and qualifies the malignancies that could be missed if the 3-tiered system were used to work up ITN seen initially on CT, MRI, and PET/CT. The incidental malignancies missed by the categorization method represented only 1.2% of all thyroid malignancies. Malignancies that would be missed were small in size and generally associated with an early AJCC stage. Given the results from this study and prior studies showing the potential for reduction in benign nodule workup, the 3-tiered system could form the basis of future guidelines for the reporting and workup of ITN seen on CT, MRI, and PET/CT.
Footnotes
Author Disclosure Statement
No competing financial interests exist.