
Abstract
Background:
PAX8/PPARγ rearrangement is a common genetic alteration in follicular thyroid carcinoma (FTC) and has been reported with variable frequency in papillary thyroid carcinoma (PTC). The diagnostic and phenotypic features of thyroid nodules positive for PAX8/PPARγ on preoperative examination are not well understood.
Methods:
The prevalence of PAX8/PPARγ rearrangement was analyzed in a series of 2015 consecutive thyroid nodules that underwent molecular analysis on cytology specimens and in 446 surgically removed PTCs. For all PAX8/PPARγ positive cases, cytology and surgical pathology slides were examined and the available clinical records were reviewed.
Results:
Twenty-two PAX8/PPARγ rearrangements were identified, including 16 detected preoperatively and 6 postoperatively. The incidence of PAX8/PPARγ in PTC was 1.1%. Cytologically, most of these nodules were diagnosed as a follicular neoplasm (73%), followed by the diagnosis of atypia of undetermined significance (19%), and none of the cases was diagnosed as cytologically malignant. All nodules with PAX8/PPARγ detected preoperatively and surgical follow-up available were found to be malignant, among which the most common diagnosis was the encapsulated follicular variant of PTC. Overall, among 20 PAX8/PPARγ-positive tumors that were surgically excised, 17 (85%) were PTC and 3 (15%) were FTC. On follow-up available for 17 patients (mean, 22.4 months), 16 PAX8/PPARγ-positive cancers showed no evidence of biochemical or structural recurrence, whereas 1 patient with FTC developed bone metastasis.
Conclusions:
In this series, PAX8/PPARγ rearrangement found in thyroid nodules had a 100% predictive value for differentiated thyroid cancer, and was more predictive of PTC than FTC. However, almost all PTC carrying PAX8/PPARγ were encapsulated follicular-pattern tumors, distinguished from FTC only by nuclear features. Although most tumors carrying this mutation appear to be clinically indolent, at least on short-term follow-up, distant metastasis can develop from FTC positive for PAX8/PPARγ.
Introduction
A
The most common genetic aberrations in thyroid cancer are BRAF and RAS point mutations and RET/PTC and PAX8/PPARγ rearrangements (8). Of these, PAX8/PPARγ is formed through the translocation t(2;3)(q13;p25) that fuses the promoter and 5′-coding portion of the thyroid-specific transcription factor PAX8 gene to the full-length coding sequence of the nuclear receptor peroxisome proliferator-activated receptor-gamma 1 gene (9). When first described in 2000, PAX8/PPARγ was presumed to be specific for follicular thyroid carcinoma (FTC) (9). Subsequent studies have confirmed PAX8/PPARγ presence in 30–35% of FTC and also found it in 2–13% of follicular adenomas (10 –13). Additional studies have reported the occurrence of PAX8/PPARγ rearrangement in the follicular variant of papillary thyroid carcinoma (PTC), typically with low frequency (1–5%) (14). However, a much higher prevalence (37.5%) of PAX8/PPARγ rearrangements was reported in the follicular variants of PTC by Castro et al. (15). As a result, the frequency of PAX8/PPARγ rearrangement in PTC remains controversial. Moreover, the histopathologic characteristics of thyroid nodules found to carry this rearrangement in the FNA materials are not clear.
The aim of this study was to establish the prevalence of PAX8/PPARγ rearrangement in PTC and to characterize clinical, cytologic, and pathologic characteristics of thyroid nodules harboring this genetic alteration.
Materials and Methods
Patients
Under University of Pittsburgh Medical Center Institutional approval, the records of all patients identified to have a PAX8/PPARγ rearrangement on either cytologic or histologic analysis between December 2007 and June 2013 were reviewed. At our institution, PAX8/PPARγ translocations have been evaluated prospectively since April 2007 as part of a molecular marker panel that included BRAF, RAS, RET/PTC, and PAX8/PPARγ mutations. The molecular panel was performed on all FNA samples with indeterminate or malignant cytology, and on selected benign FNA samples with concerning ultrasonographic or clinical features.
In order to establish the prevalence of PAX8/PPARγ in PTC, a series of 446 unselected PTCs diagnosed at our institution with tumor tissue available was studied for PAX8/PPARγ and other major molecular alterations, including BRAF and RAS point mutations and RET/PTC1 and RET/PTC3 rearrangements.
Detection of PAX8/PPARγ rearrangement and other mutations
Detection of PAX8/PPARγ transcripts and BRAF, RAS, and RET/PTC mutations was performed as previously described (7,16). For cytology and frozen samples, extraction of DNA and RNA was performed using standard laboratory procedures. Briefly, RNA isolation from cytologic FNA specimens and snap-frozen tissue was performed using Nucleic Acid Isolation Kit (Roche, Indianapolis, IN). Three micrograms of total RNA extracted from frozen tissue and cytologic FNA biopsy specimens were reverse-transcribed in a volume of 50 μL, using random hexamer priming and Superscript II RT (Invitrogen, Carlsbad, CA) according to the manufacturer's protocol. Single-step real-time reverse transcription-polymerase chain reaction (RT-PCR) was performed to amplify the fusion points of PAX8/PPARγ rearrangements on ABI7500. Amplification of the GAPDH and KRT7 genes was used to control quality and quantity of RNA and amount of epithelial cells present in the specimen.
Cytologic and histologic diagnosis
All patients had a dominant nodule ≥1 cm. Ultrasound-guided FNA was performed for indications based on American Thyroid Association (ATA) guidelines (17). All cytology cases were reported using the Bethesda System for Reporting for Thyroid Cytology (BSRTC) (18,19). Cytologic smears from FNA samples positive for PAX8/PPARγ were reviewed to confirm the diagnosis and characterize the cytologic features. For cases that were resected, the preoperative finding of PAX8/PPARγ was a consideration for total thyroidectomy. The histologic slides of respective surgical specimens were reviewed to confirm the assigned diagnosis and evaluate the histopathologic features corresponding to the aspirated nodule. The tumors were staged based on American Joint Committee on Cancer (AJCC) criteria (20). Tumors were diagnosed based on the current World Health Organization (WHO) classification of endocrine tumors (21). The criteria for diagnosing the encapsulated follicular variant of papillary carcinoma included an encapsulated or well demarcated nodule showing predominantly the follicular growth pattern with no well-formed papillae (22). The entire capsule of the tumor was examined microscopically to determine the presence of tumor capsule or vascular invasion.
Results
Study cohort
Molecular analysis of 2015 thyroid FNA samples during the study period identified PAX8/PPARγ rearrangement transcripts by RT-PCR in 15 (0.7%) thyroid nodules. One additional patient was diagnosed with a PAX8/PPARγ-positive nodule in the material obtained by a core biopsy. Six additional thyroid cancers revealed PAX8/PPARγ rearrangement only by the analysis of surgically removed tumors (no preoperative FNA or core biopsy specimen was available). This encompassed the analysis of 446 consecutive PTCs for PAX8/PPARγ and other major molecular alterations, including BRAF and RAS point mutations and RET/PTC1 and RET/PTC3 rearrangements. In this tumor group, our analysis revealed 5 PAX8/PPARγ rearrangements, resulting in a 1.1% incidence of PAX8/PPARγ rearrangements in histologic PTC (Table 1). In all 22 thyroid nodules and thyroid cancers positive for PAX8/PPARγ, molecular testing revealed no other coexisting mutations commonly occurring in thyroid cancer.
Among patients with PAX8/PPARγ detected either preoperatively or postoperatively, the mean age was 39.6 years (range, 13–68 years); 14 were females and 8 were males. Five patients presented with a history of Hashimoto's thyroiditis.
Among 20 patients with PAX8/PPARγ-positive nodules who underwent surgery at our institution, 16 had initial total thyroidectomy, 1 patient received reoperative completion total thyroidectomy, and 3 patients received diagnostic lobectomy. Each lobectomy patient had subsequent completion total thyroidectomy. One patient elected to have no surgery and another continued clinical care at another institution.
Preoperative Detection of PAX8/PPARγ
Of the 16 patients with thyroid nodules that harbored a PAX8/PPARγ rearrangement on preoperative examination, 15 patients underwent FNA with cytologic examination and 1 had a core biopsy of the nodule. The most common cytologic FNA diagnosis was follicular neoplasm or oncocytic (Hürthle cell) neoplasm (FN/ON) found in 11 (73%) of cases, followed by the diagnosis of atypia of indeterminate significance in 3 cases, and benign cytology in 1 case. Cytologic preparations diagnosed as FN/ON demonstrated numerous microfollicles and frequently dense colloid, and did not show nuclear features of papillary carcinoma sufficiently expressed to diagnose these cases as suspicious for malignancy or malignant (Figs. 1 –3). One patient at age 13 was managed with preoperative core biopsy that yielded a histologic diagnosis of suspicious for papillary carcinoma. None of the PAX8/PPARγ-positive lesions had the diagnosis of malignancy established preoperatively.
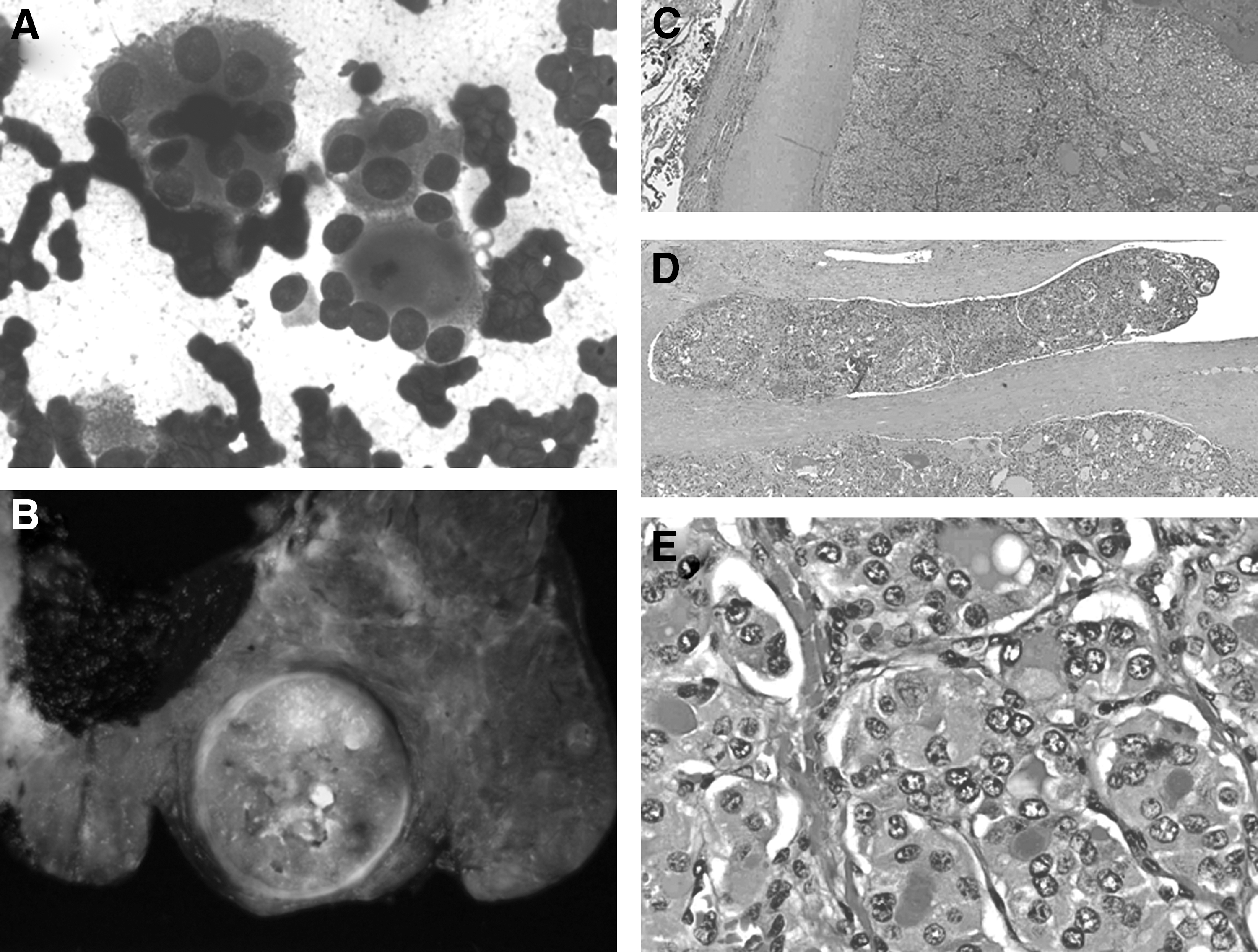
Cytologic and histologic appearance of the follicular variant of papillary thyroid carcinoma (PTC) positive for PAX8/PPARγ.
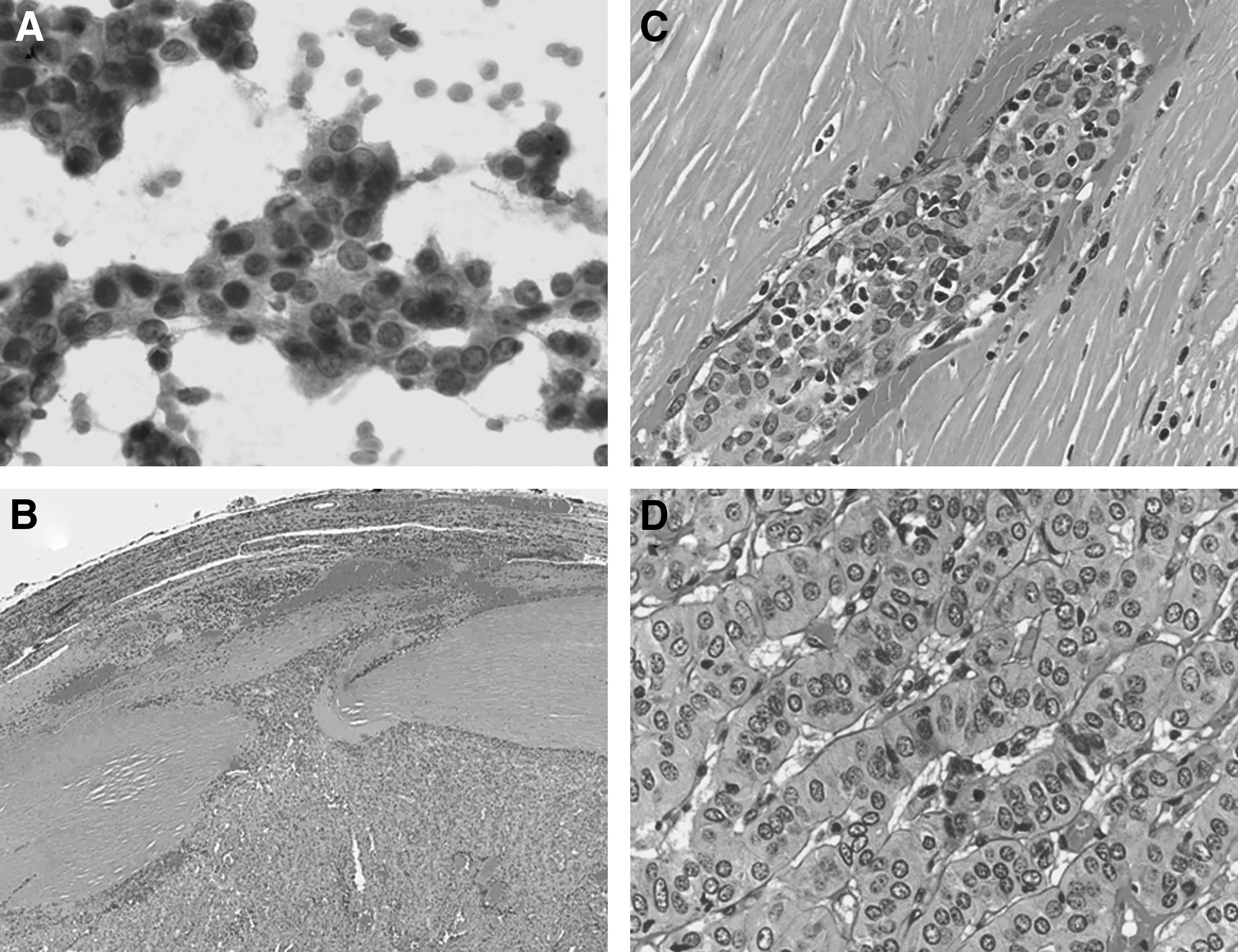
Solid variant of papillary thyroid carcinoma (PTC) positive for PAX8/PPARγ.
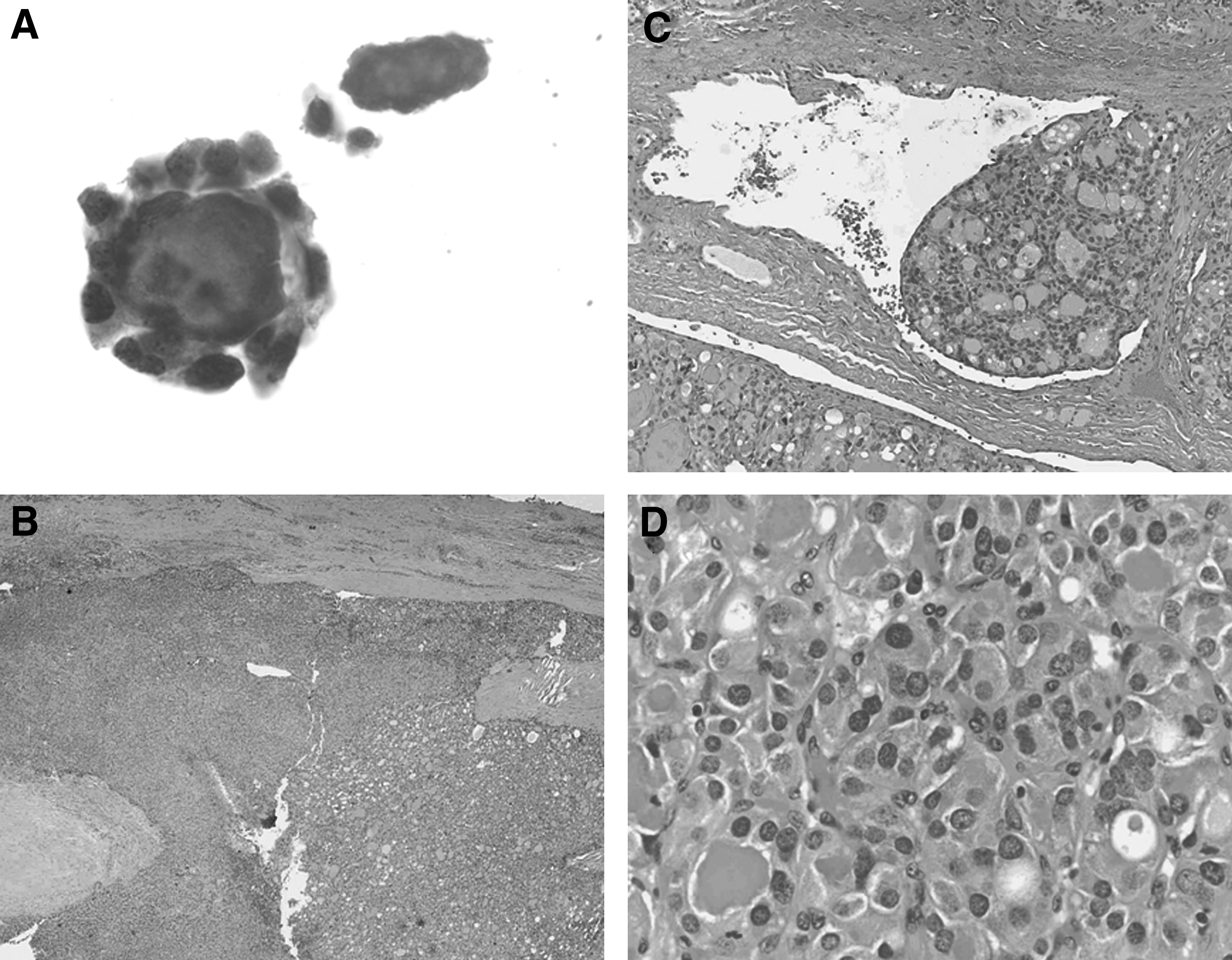
Follicular thyroid carcinoma (FTC) positive for PAX8/PPARγ.
Histologic features of PAX8/PPARγ-positive nodules
Of the 16 patients with thyroid nodules found to be positive for PAX8/PPARγ preoperatively, 14 patients underwent surgery and had histologic slides available for examination. Of these, 12 patients were found to have PTC and 2 had FTC. Therefore, in this series of thyroid nodules, PAX8/PPARγ detection preoperatively had a 100% positive predictive value for malignancy. Six additional tumors had no molecular testing performed preoperatively and were found to have a PAX8/PPARγ during molecular analysis of the surgically removed tumors. Among those, 5 tumors had a histologic diagnosis of PTC and 1 was FTC.
Among PTC, the tumor size ranged from 1.5 to 7.2 cm (mean, 3.4 cm). The majority of PTC (15/17, 88%) were diagnosed as the follicular variant (Fig. 1). Two other tumors were the solid variant and oncocytic variant of PTC. Neither of these tumors showed tumor necrosis or increased mitotic activity. All 17 tumors were encapsulated and most had a thick capsule (Fig. 1). Capsular invasion was found in 8 (47%) and vascular invasion in 6 (35%) tumors, with 2 tumors showing both tumor capsule and vascular invasion. The number of foci of vascular invasion varied from 1 to 4. The follicular variant tumors had mostly a microfollicular growth pattern. The solid variant PTC demonstrated solid, insular, and trabecular growth patterns (Fig. 2). None of the tumors showed well-formed papillary structures. In all tumors, the nuclear features of papillary carcinoma were seen throughout the tumor nodule but were demonstrated only modestly. The most common nuclear features included nuclear enlargement, overlapping, irregularity of the nuclear contours, and nuclear grooves, whereas nuclear pseudoinclusions were virtually never seen (Fig. 1). None of the tumors showed evidence of extrathyroidal extension or positive margins. Ten patients had at least 1 lymph node resected (range, 1–8) and none exhibited regional metastasis.
Among three follicular carcinomas, all had a complete capsule and showed capsular (2 tumors) or vascular (1 tumor) invasion. Both cytologic and histopathologic specimens demonstrated the microfollicular growth patterns with dense colloid (Fig. 3).
Of the 20 PAX8/PPARγ-positive carcinomas, 7 were multifocal. Papillary microcarcinomas were found in 5 thyroid glands affected by the follicular variant of PTC, with a total number of foci ranging from 2 to 4, and in 2 of the cases of follicular carcinoma. In 1 multifocal follicular variant of PTC, PAX8/PPARγ rearrangement was present in the larger tumor while a different mutation, NRAS, was present in the papillary microcarcinoma.
Patient follow-up
Follow-up information was available for 17 patients. The mean length of follow-up was 22.4 months (range, 0.2–61.8 months). Twelve patients received radioactive iodine ablation (RAI) treatment at a mean dose of 79.4 mCi (48–158 μCi I131), and 4 patients had RAI deferred. Sixteen patients with PAX8/PPARγ-positive carcinoma demonstrated no evidence of recurrence based on thyroglobulin levels and imaging results. One patient with follicular carcinoma that had multifocal capsular invasion and no vascular invasion at presentation developed a metastatic lesion to the femur that was detected 2 months after thyroid surgery and confirmed by biopsy.
Discussion
Although PAX8/PPARγ rearrangement has been known to occur in thyroid cancer for over a decade, it was perceived as a prototypic mutational event for FTC and its prevalence in papillary cancer remained controversial. Moreover, despite significant progress in preoperative detection of mutations in thyroid nodules, the risk of thyroid cancer and the predominant tumor type expected in a nodule found to be positive for PAX8/PPARγ rearrangement in the FNA sample remained unclear. In this study, we used a large series of PTC and determined that overall PAX8/PPARγ rearrangements remain a rare event in PTC because it was found in approximately 1% of these tumors. However, because PTC is by far the most common type of thyroid cancer, we report here that overall the majority of thyroid cancers positive for this mutational event are actually PTC. In fact, 3 of 4 nodules detected as carrying a PAX8/PPARγ rearrangement in this study were PTC and one-fourth was FTC at surgery.
Surprisingly, most PTC positive for a PAX8/PPARγ rearrangement were encapsulated and showed the follicular growth pattern (i.e., sharing these phenotypical features with FTC). Similar to PTC, these tumors were frequently encapsulated, had a thick capsule, and showed capsular and/or vascular invasion. These findings indicate that many PAX8/PPARγ-positive tumors, which were diagnosed as PTC due to the presence of characteristic nuclear features, share a number of important histologic features with FTC. Moreover, no PTC in this group demonstrated lymph node metastases, and one tumor manifested with bone metastasis. The lack of lymph node involvement and predisposition to the spread to distant site is another feature of these PTC tumors that is characteristic of FTC. Therefore, the results of this study suggest that the PAX8/PPARγ-positive thyroid cancer, despite being histologically diagnosed as PTC, have many histopathologic and biologic properties of FTC. In fact, since the histopathologic criteria for diagnosis papillary carcinoma has become progressively relaxed over the last 20 years (23 –25), it is possible that this in part is responsible for a higher proportion of papillary rather than follicular cancers diagnosed in this series.
We further report for the first time the occurrence of PAX8/PPARγ rearrangement in the solid variant of PTC. Solid variant PTC is more frequently found in patients with the history of radiation exposure (8), and in some studies was associated with higher rates of extrathyroidal extension and lymph node metastasis, and with a slightly worse survival (26). In this study, however, the patient with the solid variant of PTC had no history of radiation exposure and showed no recurrence or other complications on follow-up.
In this series of cases, the preoperative detection the PAX8/PPARγ rearrangement had a 100% predictive value for differentiated thyroid cancer. Although none of the nodules positive for PAX8/PPARγ in this study was found to be benign, cases of follicular adenoma carrying this mutation have been previously reported (10 –13). These reports, as well as the results of this study, suggest that although occasional tumors carrying this rearrangement may be benign, overall the occurrence of this mutation in a thyroid nodule confer a high risk of well-differentiated thyroid cancer. Notably, none of the nodules in this study were diagnosed as cancer on cytology, highlighting the importance of ancillary molecular testing to augment the results of FNA cytology for clinical decision-making.
Despite the presence of capsular and vascular invasion in a significant number of cases in this series, most of these tumors did not have overtly invasive features at presentation, and the clinical follow-up available in this study revealed no recurrences or distant metastases with the exception of one case. This suggests that the majority of PAX8/PPARγ-positive tumors are likely to have an indolent clinical course, although tumors with multifocal capsular invasion or vascular invasion may metastasize to distant sites and therefore may require more aggressive treatment. The knowledge of the mutational status of these tumors is important because of the availability of clinical trials such as that of pioglitazone in follicular-patterned thyroid cancers that contain the PAX8/PPARγ rearrangement (ClinicalTrials.gov Identifier NCT01655719). Since PAX8/PPARγ confer a very high risk of malignancy in a given nodule, it suggests that upfront total thyroidectomy may be an appropriate surgical approach for these patients. On the other hand, a small proportion of the PAX8/PPARγ-positive tumors may still be benign follicular adenomas, and the results of this study demonstrate that many of these tumors are encapsulated and noninvasive, raising the possibility that lobectomy may also be considered, at least for those nodules that are small in size and show no ultrasonographic evidence for invasion.
In summary, the results of this study indicate that PAX8/PPARγ rearrangement detected preoperatively in a thyroid nodule is highly predictive of well-differentiated thyroid carcinoma, particularly the encapsulated follicular variant of papillary cancer, which, however, typically express phenotypic features and clinical behavior expected for FTCs rather than classic papillary carcinomas.
Footnotes
Acknowledgments
Y.E.N. is a consultant for Quest Diagnostics. All other authors have nothing to disclose. Supported in part by a National Institutes of Health (NIH) grant CA88041 to Y.E.N.
Author Disclosure Statement
No competing financial interests exist.