
Abstract
Background:
Iodine requirements are increased during pregnancy to maintain maternal and fetal euthyroidism. There have been recent improvements in iodized salt coverage in India, but whether iodized salt is sufficient to sustain iodine requirements during pregnancy remains uncertain. Our aims were to measure thyroid status in first trimester pregnant women in southern India and assess potential determinants of thyroid function, including iodine status, thyroid autoimmunity, dietary patterns, body weight, and anemia.
Methods:
This was a cross-sectional study among 334 pregnant women of ≤14 weeks' gestation, in Bangalore, India. We measured anthropometrics, urinary iodine concentration (UIC), maternal thyroid volume (by ultrasound), and thyroid function. We applied a thyrotropin (TSH) upper limit of 2.5 mIU/L to classify thyroid insufficiency. Using a questionnaire, we obtained sociodemographic and dietary data, obstetric history, and use of iodized salt and iodine supplements.
Results:
Among the women, the mean (standard deviation) gestational age was 10.3 (2.5) weeks, 67% were nulliparous, 21% were vegetarian, 19% were anemic, and 23% were overweight or obese. Iodized salt was used by 98% of women, and they were iodine sufficient: median UIC (range) was 184.2 μg/L (8.1–1152 μg/L) and all had a normal thyroid volume. However, 18% of the women had thyroid insufficiency: 3.7% had overt hypothyroidism (83% with positive TPO-Ab), 9.2% had subclinical hypothyroidism, and 5.2% had hypothyroxinemia. Women consuming vegetarian diets did not have significantly lower iodine intakes or higher risk of hypothyroidism than those consuming mixed diets, but overweight/obesity and anemia predicted thyroid insufficiency.
Conclusion:
In this urban population of southern India, pregnant women have adequate iodine status in the first trimester. Despite this, many have thyroid insufficiency, and the prevalence of overt hypothyroidism is more than fivefold higher than reported in other iodine sufficient populations of pregnant women.
Introduction
I
The World Health Organization states that an established universal salt iodization program with adequate salt iodine levels and good population coverage can meet the increased iodine requirement of pregnant women (4). However, maternal iodine insufficiency is prevalent even in countries with established programs (5 –9). India, because of its large population, high birth rate, and iodine deficient soils, has until recently had a large number of infants potentially exposed to in utero iodine deficiency (10). However, household coverage of iodized salt has increased, and it is now estimated that >70% of households in India have access to iodized salt (10). Nevertheless, recent studies highlight the presence of iodine insufficiency among Indian women (11).
In areas of iodine sufficiency, the prevalence of overt and subclinical hypothyroidism during pregnancy is 0.2–0.4% and 3–5% respectively, but varies by trimester of pregnancy and the diagnostic criteria (particularly the thyrotropin [TSH] upper limit) used for classification (12). More than 90% of thyroid disorders in pregnancy are thought to be of autoimmune etiology (13), and chronic autoimmune thyroiditis is the main cause of hypothyroidism during pregnancy in iodine sufficient regions (14). Two additional variables that may affect the maternal thyroid axis and contribute to thyroid insufficiency during pregnancy are iron deficiency anemia (15) and overweight/obesity (7,16 –19), and both are common among women in urban areas of India (20 –22). Better understanding of the pattern and prevalence of maternal thyroid dysfunction and associated risk factors could improve screening and treatment in the Indian population. Improved detection of maternal hypothyroidism may be particularly valuable in the first trimester because thyroid function should be normalized as quickly as possible early in gestation (12).
Therefore, the aims of this cross-sectional study were: (a) to measure thyroid status in first trimester pregnant women in southern India; and (b) to assess potential determinants of thyroid function in this population, including iodine status, thyroid autoimmunity, body weight, and anemia.
Subjects and Methods
This cross-sectional study consisted of a cohort of pregnant women who were screened for the Maternal Iodine Supplementation and its Effects on Child Development (MITCH) study (Clinicaltrials.gov with the identifier NCT00791466). The parent study investigates the effects of oral iodine supplementation during pregnancy on pregnancy outcome, infant growth, and offspring cognitive development. The study was conducted at the antenatal clinic of the Obstetrics and Gynecology Department of St. Martha's Hospital in Bangalore, India. Pregnant women were recruited between December 2008 and March 2011. We conducted the study in accordance with the Declaration of Helsinki. Institutional ethical review boards at St. John's National Academy of Health Sciences, St. Martha's Hospital, Bangalore, India, and Wageningen University, The Netherlands approved the study. We explained the study in detail to the participating women and one member of their family, and obtained written, witnessed informed consent.
Study population
We screened all women presenting to the antenatal clinic for potential inclusion in the study if they had a positive pregnancy test and were: (a) ≥18 and ≤40 years old; and (b) ≤14 weeks gestational age. Exclusion criteria were: (a) chronic diseases, including diabetes, heart, kidney, and thyroid disease, cancer, hypertension, tuberculosis, asthma, epilepsy, jaundice; (b) a positive test for HIV, HbSAg, or venereal diseases; (c) treatment for infertility; (d) previous repeated spontaneous abortions (four or more); (e) current multiple pregnancy as detected by ultrasound; and (e) currently breastfeeding. Of the 1058 pregnant women who presented at the antenatal clinic at the start of their pregnancy during the study period, 1015 women were contacted for the study; 43 women were not contacted because, based on their hospital record, they did not meet the inclusion criteria. Of the 1015 women contacted, 344 women were not eligible for the study because they did not meet the inclusion criteria. Of the remaining 671 pregnant women who were considered eligible, 337 declined to participate in the study. A total of 334 pregnant women were eligible and consented for their participation in this study. There were no statistically significant differences in age, gestational age, education, occupation, monthly household income, height, weight, or body mass index (BMI) between those who declined participation and those who agreed to participate in the study (data not shown).
Sociodemographic and anthropometric data
We used a structured multiple-choice questionnaire to obtain sociodemographic information on household composition, education, occupation, and income, as well as consanguinity and obstetric history, including parity. We did not collect information on family history of thyroid disease. We calculated gestational age from reported first day of the last menstrual period and confirmed this by using ultrasonography in 63% of the women. We recorded anthropometric measurements in duplicate using standard techniques (23). We recorded weight to the nearest 0.1 kg by using a digital weighing scale (Salter's 9016, Tonbridge, Kent, United Kingdom), and height to the nearest 0.1 cm by using a stadiometer (Biorad, Chennai, India). We calculated BMI as weight in kilograms divided by the square of height in meters (kg/m2); we defined overweight as a BMI of 25.0–29.9 kg/m2 and obesity as ≥30 kg/m2 (23).
Data on diet, salt, and iodine supplement use
By using a self-reported written questionnaire, we obtained data on dietary habits including: (a) whether the subject was a vegan, a lacto-ovo vegetarian, or nonvegetarian; (b) household usage of iodized or noniodized salt, including brand and type of salt; (c) cooking practices using salt; (d) use and frequency of seafood and egg consumption; and (e) knowledge of iodine nutrition and reason for iodized salt consumption, data on consumption of nutritional supplements containing iodine or iodine containing multi-micronutrient powders, including quantity and length of time these supplements had been consumed; these data were collected from a subset of pregnant women. This subset was a convenience sample.
Laboratory analysis
We collected a casual spot nonfasting urine sample that was transported on ice, divided into aliquots, and stored at −20°C until analysis. We determined UIC by using the modification of Pino et al. of the Sandell–Kolthoff reaction (24) with external reference standards (C. Zeder, ETH Zurich, Switzerland). At a mean UIC of 82.6 μg/L, the intra and inter-assay CV was 9.5% and 7.6% respectively, and at a mean UIC of 206.4 μg/L, the intra and inter-assay CV was 3.2% and 5.3% respectively. We collected a nonfasting whole blood sample by venipuncture into plain vacutainers (BD diagnostics, Franklin Lakes, NJ) that was transported on ice and centrifuged to obtain serum, which was stored frozen at −80°C until analysis for TSH, total triiodothyronine (TT3), total thyroxine (TT4), free T3 (fT3), free T4 (fT4), thyroglobulin (Tg), thyroid binding globulin (TBG), antithyroid peroxidise antibodies (TPO-Ab), and anti-Tg antibodies (Tg-Ab). With the exception of TSH, for which trimester-specific ranges are available, we used the manufacturer's recommended reference range for thyroid function tests. We measured TSH by using a third generation solid phase, two-site chemiluminescent assay (IMMULITE 1000, Siemens Healthcare Diagnostics, Llanberis, Gwynedd, United Kingdom) and applied a reference range of 0.1–2.5 mIU/L for the first trimester (25,26). The percent CVs at a TSH of 0.44 and 4.75 were 3.86% and 7.16% respectively. The analytical measurement range of the TSH assay was up to 75 mIU/L, and its analytical sensitivity was 0.004 mIU/L. We measured TT4, fT4, TT3, fT3, Tg, Tg-Ab, TPO-Ab, and TBG by using immunoassays (IMMULITE 1000). The reference range for TT4 was 4.5–12.5 μg/dL, 58–161 nmol/L; the percent CVs at 4.3 and 11.5 μg/dL were 6.5% and 7.6% respectively; the analytical measurement range was 1–24 μg/dL; and analytical sensitivity was 0.4 g/dL. The reference range for TT3 was 70–204 ng/dL, 1.1–3.1 nmol/L; the percent CVs at a TT3 of 61.7 and 192.5 ng/dL were 9.0% and 7.26% respectively; the analytical measurement range was 40–600 ng/dL; and analytical sensitivity was 35 ng/dL. The reference range for thyroxine-binding globulin (TBG) was 15–34 μg/mL, 0.3–0.6 μmol/L; the percent CV at a TBG of 15.09 was 7.58%; the analytical measurement range was 3.5–80 μg/mL; and analytical sensitivity was 1.1 μg/mL. The reference range for fT4 was 0.89–1.76 ng/dL, 11.5–22.7 pmol/L; the percent CVs at a fT4 of 0.95 and 2.5 ng/dL were 5.14% and 4.91% respectively; the analytical measurement range was 0.3–6.0 ng/dL; and the analytical sensitivity was 0.13 ng/dL. The reference range for fT3 was 2.6–4.8 pg/mL, 4.0–7.4 pmol/L; the percent CVs at a fT3 of 2.39 and 5.92 pg/mL were 4.24% and 4.13% respectively; the analytical measurement range was 1–40 pg/mL; and the analytical sensitivity was 1 pg/mL. The reference range for Tg was 1.7–55.6 ng/mL; the percent CV at a Tg of 9.69 ng/mL was 3.64%; the analytical measurement range was up to 300 ng/mL; and the analytical sensitivity was 0.2 ng/mL. The reference range for Tg-Ab was 0–40 IU/mL, the percent CV at 25.21 IU/mL was 5.29%; the analytical measurement range was 20–3000 IU/mL; and the analytical sensitivity was 10 IU/mL. We applied a cutoff value for TPO-Ab of <35 IU/mL. The percent CV at 50.35 IU/mL was 6.97%; the analytical measurement range was 10–1000 IU/mL; and the analytical sensitivity was 7 IU/mL. Hemoglobin (Hb) was measured on an automated Coulter counter (ABX Pentra 60C+, Horriba Ltd, Kyoto, Japan). Anemia was defined as Hb <11.0 g/L.
Thyroid gland measurement
We measured thyroid gland volume by using an Aloka SSD-500 Echocamera (Aloka, Mure, Japan) with a 7.5 MHz linear transducer. We calculated thyroid volume of each lobe using the formula for a prolate ellipsoid where thyroid volume (mL)=0.479×length×breadth×depth (cm), and summed the volumes of both lobes to obtain total thyroid volume (4).
Statistical analysis
All the thyroid function parameters except total T4 were non-normally distributed, and these were log transformed before analysis. We confirmed the normality of the log transformed data using the Kolmogrov–Smirnov test. We report normally distributed data as arithmetic means±standard deviation (SD), non-normally distributed data as medians (quartiles), and categorical data as numbers (%). We examined correlations among thyroid hormones by using Pearson's correlation, the association of thyroid function parameters with maternal characteristics using linear regression analysis, and present the R 2 for each characteristic in the univariate analysis. All characteristics with p<0.20 in the univariate analyses were considered in multiple variable model to adjust for possible confounding effects of maternal characteristics and the results presented with R 2 for multivariate model. The regression coefficient from the linear regression analysis of log transformed data was interpreted as percent change for one unit increase in independent variable (27). The percentage change for TT4 was calculated by dividing the regression coefficient by the reference group mean and multiplied by 100. Regression of TSH, fT4, TT4, and Tg considered maternal age, gestational age (<10 weeks vs. >10 weeks), hemoglobin, BMI (normal vs. underweight, overweight, obese), consanguinity, parity (0 vs. ≥1), maternal education, maternal employment, food habits (vegetarian vs. nonvegetarian, lacto-ovo-vegetarian), reason for salt use (health vs. taste, tradition, quantity, others), seafood intake, egg intake, use of iodine containing multi-micronutrient powders, and presence of Tg-Ab and TPO-Ab above the cutoff values. Statistical analyses were carried out with SPSS v18.0 (SPSS, Inc., Chicago, IL).
Results
The demographic, anthropometric, and dietary characteristics of the women are shown in Table 1. Mean gestational age was 10.3 weeks, and two-thirds of the women were nulliparous. Notably, 23% were overweight or obese, 18.3% were anemic (Hb <11.0 g/dL), 20.7% were vegetarian, and 56.1% and 36.9% of the women were not consuming seafood and eggs respectively. Although nearly all were using iodized salt at home, only about half were aware of iodine in their diet, and only 10% specifically chose iodized salt for health reasons. One third of women were consuming multi-micronutrient powders (5–10 g/day) containing iodine in the range of 73–294 μg/100 g. But the mean (range) iodine intake from these powders was low: 12.4 (4 –59) μg/day for a mean (range) duration of 10 (0–180) months.
Data are mean±standard deviation (SD), median with quartiles in parentheses, and numbers with percentages in parentheses.
Sociodemography, 2obstetrics history, 3anthropometry, 4dietary characteristics.
Parity was defined as the number of times a woman has given birth to a fetus with a gestational age of 24 weeks or more, regardless of whether the child was born alive or was stillborn. Abortion was defined as termination of pregnancy, whether spontaneous or induced.
Thyroid parameters and UICs in the women are shown in Table 2. The median UIC (range) was 184.2 (8.1–1152) μg/L, and none of the women had an elevated thyroid volume or an elevated thyroglobulin; all of these indicators suggest iodine sufficiency (28). The distribution of UIC is shown in Figure 1. The prevalence of thyroid function tests outside reference ranges is shown in Figure 2. Only seven (2.1%) women were hyperthyroid, six of whom had subclinical hyperthyroidism. In contrast, 42 (12.9%) were hypothyroid, 30 of whom had subclinical hypothyroidism; and 17 (5.2%) had isolated hypothyroxinemia with a normal serum TSH. Thirty-two (9.7%) and 46 (14.0%) of the women had elevated TPO-Abs and Tg-Abs respectively.
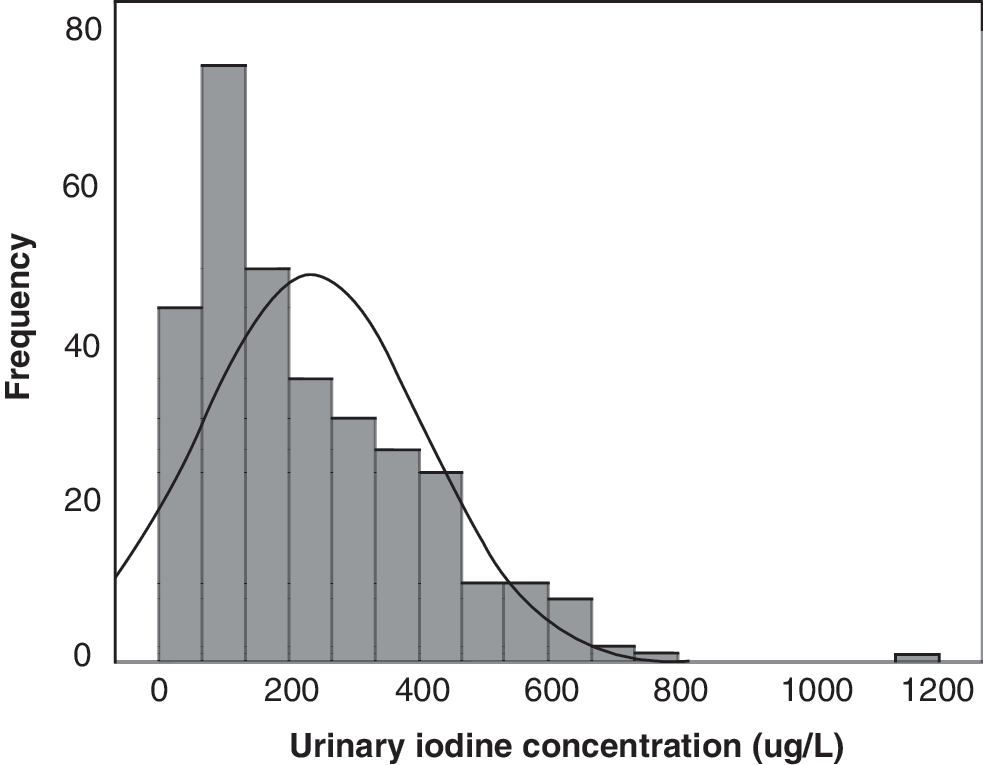
Distribution of urinary iodine concentrations (UICs) in first trimester pregnant women from Bangalore, India (n=321).
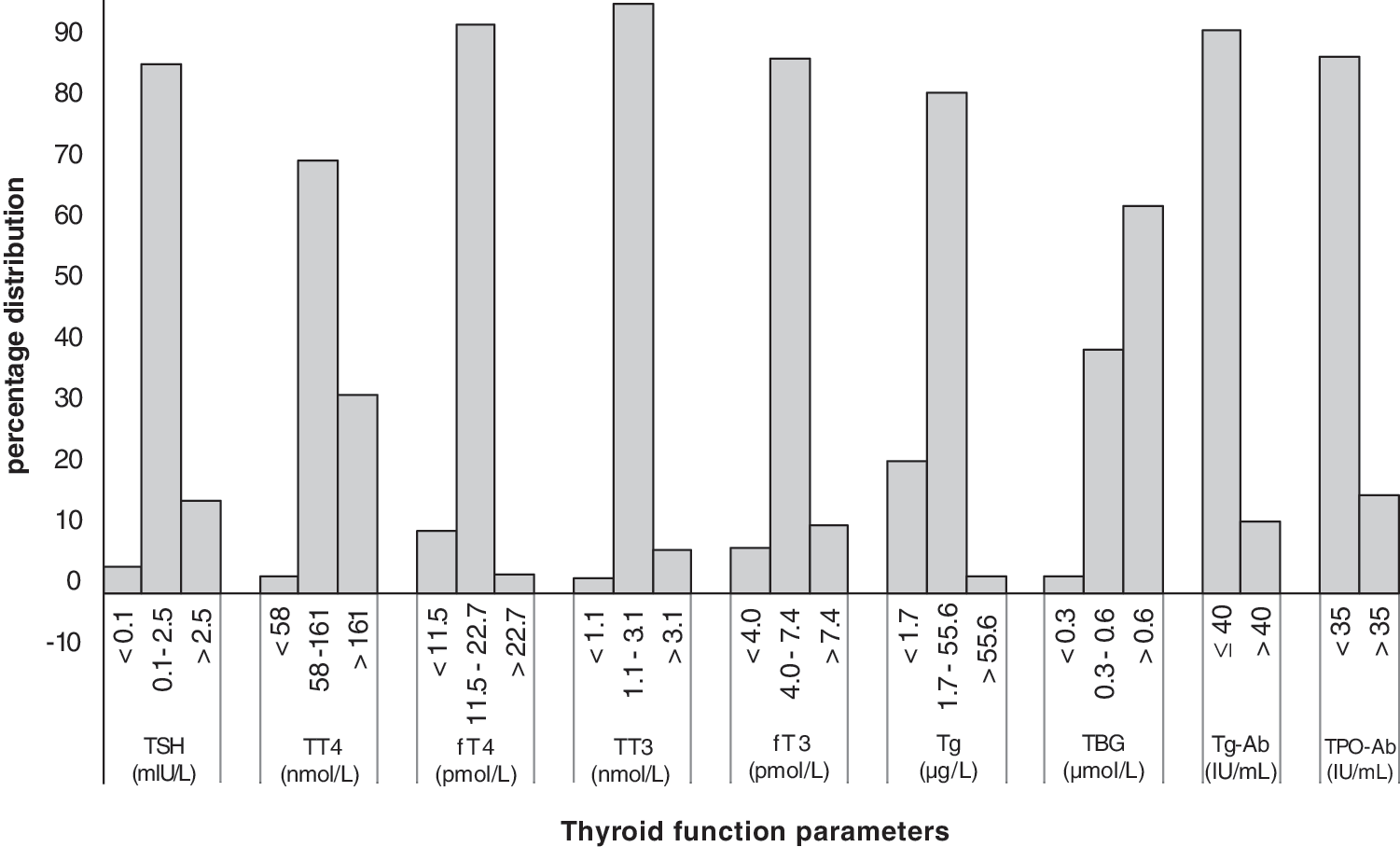
Prevalence of thyroid function tests outside reference ranges in first trimester pregnant women from Bangalore, India. Each set of bars on the x-axis indicate the distribution of each thyroid function parameters; the y-axis represents percentages.
Overt hyperthyroidism, low TSH+high free T4; subclinical hyperthyroidism, low TSH+normal free T4; overt hypothyroidism, high TSH+low free T4; subclinical hypothyroidism, high TSH+normal free T4; isolated hypothyroxinemia, normal TSH+low free T4.
Table 3 shows the comparisons of characteristics of women with thyroid hypofunction (hypothyroidism or hypothyroxinemia) to those who were euthyroid. In women with thyroid hypofunction, hemoglobin was lower (p=0.005), and there was a significantly increased prevalence of TPO-Ab (34.5% vs. 9.2%) and Tg-Ab (22.4% vs. 6.5%; p≤0.001) compared to euthyroid women. Hemoglobin levels did not differ between pregnant women with overt and subclinical hypothyroidism (p=0.825). The prevalence of elevated TPO-Ab was 12.5%, 26.7%, and 83.3% in women with hypothyroxinemia, subclinical hypothyroidism, and overt hypothyroidism respectively, and the median UICs in these three subgroups were 146.8, 166.1, and 195.9 μg/L respectively.
Data are mean±SD with min/max in parentheses, median with quartiles in parentheses, and numbers with percentages in parentheses.
p-Values are from t-test for normally distributed data, Mann–Whitney U-test for non-normally distributed data, and chi-square test for categorical data.
Table 4 presents the significant univariate and multivariate regression models with TSH, fT4, TT4, and Tg as dependent variables. Vegetarianism was not associated with any of the thyroid function tests. In the multivariate regression, presence of elevated TPO-Ab was associated with higher TSH (β=0.238; p=0.006), and lower fT4 (β=−0.094; p=0.032) and lower Tg (β=−0.96; p≤0.001). Use of iodine supplements was associated with lower Tg (β=−0.286; p=0.028) and higher fT4 (β=0.055; p=0.045). Overweight and obesity were associated with lower fT4 (β=−0.08; p=0.018) and TT4 (β=−20.9; p=0.023) respectively, with fT4 and TT4 concentrations 8.2% and 14.2% lower in overweight/obese women compared to normal weight women. As fewer data were available for iodine supplement use (n=231) and salt use reason (n=275), the multiple variable linear regression analyses were repeated excluding these two variables in order to examine the associations in the complete sample (Supplementary Table S1; Supplementary Data are available online at
For description of the regression models, please see statistical methods.
Discussion
The major findings of this study are that first trimester pregnant women in Bangalore have sufficient iodine status, as indicated by an adequate median UIC and normal thyroid volumes and serum Tg concentrations. But despite this, nearly one in five women had thyroid insufficiency and in these women, more than one-third had signs of autoimmune thyroiditis, and there was a high prevalence of overt hypothyroidism (3.7%), with 83% of these women having positive TPO-Ab. A potential explanation for the high prevalence of hypothyroidism in our sample could be thyroidal disruptors, from environmental or dietary sources (29). We have no data on potential exposure to environmental thyroid disruptors, such as perchlorate, in our sample. Dietary goitrogens have been described in selected plant foods of Indian origin (30), and include thiocyanates (metabolites of cyagenic glucosides present in plant foods such as cabbage, cauliflower, bamboo shoot, cassava, mustard, turnip, and radish) and isoflavones. The consumption of isoflavones (found in soy products, peas, bean, nuts, grain products, coffee, and tea) is high in some Asian populations (31). A study looking for associations between isoflavone intake and thyroid function and autoimmunity in menopausal Indian women reported a modest reduction in serum fT3 levels (32). A limitation of the present study is that we did not collect data on intake of goitrogenic foods, although we did collect single 24 hour dietary recall data and frequency of consumption of seafood and eggs in the pregnant population. However, it is unlikely that the quantity and frequency of consumption of these potentially goitrogenic foods in the rice-based diet of south India would be high enough to produce hypothyroidism.
The prevalence of overt hypothyroidism in our study population is more than fivefold higher than reported from other iodine-sufficient women early in pregnancy (12). The prevalence of thyroid insufficiency in iodine-sufficient women in pregnancy varies and is in large part dependent on gestational age and the definition of the upper reference limit for TSH used. We used the widely accepted criteria of the American Thyroid Association, that is, a TSH upper limit of 2.5 mIU/L in the first trimester (25). In women in the United Kingdom and Italy at <15 weeks' gestation (using a TSH upper limit of 3.65 mIU/L in the United Kingdom and 3.5 mIU/L in Italy), the overall prevalence of subclinical and overt hypothyroidism was 2.3% and 0.25% respectively (33). In women in the Czech Republic at 9–12 weeks' gestation, using a TSH upper limit of 3.67 mIU/L, the respective prevalences were 3.9% and 0.4% (34), and in U.S. women at <20 weeks of gestation, using a TSH upper limit of between 2.74 and 5.09 mIU/L, the respective prevalences were 2.3% and 0.2% (35). A recent retrospective study of U.S. women in all three trimesters, using the same TSH reference range in the first trimester that we used in this study (2.5 mIU/L), reported much higher prevalences of subclinical hypothyroidism (15.1%) but a low prevalence (<0.5%) of overt hypothyroidism (36). A recent study from China found a 27.8% prevalence of subclinical hypothyroidism using the diagnostic criteria of TSH >2.5 mIU/L and 4.0% using the laboratory TSH reference interval of 0.14–4.87 mIU/L (37). A recent study from the Netherlands suggested that there may be ethnic differences in reference ranges to diagnose thyroid disease (38). However, if we apply a TSH upper limit of 3.5 mIU/L in our population to draw better comparison with studies from the available literature, the prevalence of subclinical hypothyroidism drops to 3.1%, but the prevalence of overt hypothyroidism remains the same at 3.7%, more than fivefold higher than reported in other iodine-sufficient populations of pregnant women.
In a cross-sectional study among healthy pregnant women without a family history of thyroid illness conducted in northern India in 2008, the prevalence of overt and subclinical hypothyroidism was 1.3% and 14.2% respectively, using a TSH reference range of 0.27–4.2 mIU/L (39). In another study among pregnant women from northern India, the prevalence of overt and subclinical hypothyroidism was 4.6% and 6.5% respectively, using a TSH reference range of 0.5–5.5 mIU/L (40). In iodine-sufficient areas, the main cause of hypothyroidism during pregnancy is chronic autoimmune thyroiditis (14), and this also appears to be the primary cause in our study population. In women early in pregnancy in Europe and the United States, positive TPO-Ab are present in 10% of women with hypothyroxinemia, 30–60% with subclinical hypothyroidism, and 70–90% with overt hypothyroidism (41). These prevalences are similar to the ones in our subjects: TPO-Ab were elevated in 12.5%, 26.7%, and 83.3% of women with hypothyroxinemia, subclinical hypothyroidism, and overt hypothyroidism respectively. Advancing parity may increase risk for thyroid autoimmunity (42), but in our data, the prevalence of TPO-Ab did not differ significantly between nulliparous and multiparous pregnant women.
Worldwide, iodine deficiency is a common cause of maternal thyroid insufficiency (1). Moderate to severe iodine deficiency can result in both maternal and fetal hypothyroxinemia (43,44). In less severely affected areas, isolated maternal hypothyroxinemia is more common (12). A review of iodine status in Indian pregnant women reported a range of median UICs of 95–178 μg/L, with 60–95% consuming adequately iodized salt (11). In a recent cross-sectional study from the Bangalore region, we found a median UIC of 172 μg/L in pregnant women consuming adequate amounts of iodized salt (45). In large populations of pregnant women, although the overall median UIC may indicate an adequate iodine status, subgroups with different dietary patterns may remain at risk of low intakes. For example, among pregnant women in Maharashtra, the median UIC was 203 and 211 μg/L at 17 and 34 weeks of gestation, but a subgroup of women were hypothyroxinemic and borderline iodine deficient with a median UIC of only 147 μg/L (46). However, in our study, the subgroup of women with thyroid insufficiency had a sufficient median UIC that was not significantly different from women who were euthyroid. In addition, women consuming vegetarian diets did not have lower iodine intakes than those consuming mixed diets, nor did those consuming less fish (the food group richest in native iodine). Thus, it appears that poor iodine intake in a subgroup of pregnant women is not the cause of the high prevalence of thyroid dysfunction in our sample.
Other potential contributing factors to thyroid insufficiency in our women were the high prevalence of anemia (19%) and overweight/obesity (23%). Hemoglobin was significantly lower in women with thyroid insufficiency than in euthyroid women (Table 3), and a lower hemoglobin was associated with higher TSH and lower fT4 levels (Table 4). Iron deficiency may impair thyroid function during pregnancy because thyroid peroxidase is an iron-dependent enzyme (47). Previous studies in children have shown that iron deficiency impairs correction of thyroid dysfunction during iodine repletion, and in Swiss pregnant women in the second and third trimester, the relative risk of hypothyroxinaemia was more than sevenfold higher in women who were anemic (15). A limitation of our study is that we did not measure other markers of iron status besides hemoglobin.
In the multiple regression analysis, overweight and obesity were significant predictors of a lower fT4 and TT4 (Table 4). Adiposity may increase the risk for thyroid insufficiency, and overweight adults tend to have higher TSH and lower fT4 concentrations than normal weight adults (48). Previous studies have reported an inverse relationship between fT4 concentrations and maternal weight and BMI during early pregnancy (17 –19). One study found that high maternal BMI at mid-gestation positively correlated with the fT3/fT4 ratio (16). In mildly iodine-deficient pregnant Thai women, those who were overweight had a 3.6-fold higher risk of hypothyroxinemia in the first trimester compared to normal weight women (7). As India modernizes, overweight and obesity prevalence among adult women is increasing (22). If higher BMI is a risk factor for thyroid insufficiency in pregnant women, this may become increasingly important in India.
Currently, screening of maternal thyroid function is not routinely performed during antenatal care at hospitals in Bangalore. Our data suggest screening should be considered in this setting. The high prevalence of thyroid insufficiency in pregnant women in Bangalore may have important health consequences. Overt maternal hypothyroidism increases the risk for multiple adverse pregnancy outcomes, including pre-eclampsia, spontaneous abortion, and postpartum hemorrhage, as well as premature birth and low birth weight (49,50). Many of these complications have also been associated with subclinical hypothyroidism at lower rates (51), but not all studies have found adverse impacts (18). Mild hypothyroidism may also adversely affect cognitive development of the offspring, but not all studies agree (12). The largest controlled trial showed no benefit of treatment of mild maternal hypothyroidism on offspring IQ at 3.5 years of age (33). In summary, evidence is stronger that detection and treatment of overt and subclinical hypothyroidism will benefit obstetric outcomes rather than offspring cognitive development.
Almost all the salt (both powder and crystal) used in the households of the pregnant women in our study was iodized, illustrating the wide coverage of the Indian salt iodization program in this region. Household coverage of adequately iodized salt in India has increased remarkably over the past decade, with the national coverage reaching 51% in 2005–2006 and 71% in 2009 (10). But there is better coverage of adequately iodized salt in urban areas and higher socioeconomic groups (10). Our subjects were urban women from low- to middle-income families, and the very high coverage and adequate iodine status reported here might not be generalizable to other areas of India. Use of iodized salt during the reproductive years leading up to pregnancy improves maternal thyroid economy during gestation and reduces the risk of maternal thyroid insufficiency because it contributes to normal intrathyroidal iodine stores (52). In countries with salt iodization programs, if pregnant women restrict their dietary salt intake, they have an increased risk of becoming hypothyroxinemic (53), indicating the importance of iodized salt as a dietary source of iodine. Among our women, fewer than one in five chose iodized salt for health reasons, and almost 50% had no knowledge of iodine nutrition. The low awareness of the health benefits of iodized salt in our study are consistent with findings from a recent survey in Karnataka (the Indian State where this study was done) that found awareness of the health benefits of iodized salt played a minimal role in salt purchase choice (54). These findings argue that although the program of salt iodization is currently effective, in order to increase consumer awareness and maintain demand for iodized salt in Bangalore, public health strategies such as a consumer education campaign would be valuable for program sustainability.
In conclusion, in this population of urban first trimester pregnant Indian women, the prevalence of overt hypothyroidism is surprisingly high. But iodine intake appears to be adequate, and there are apparently no subgroups of the population with low iodine intake that predict thyroid insufficiency. The most common factor underlying the high prevalence of thyroid insufficiency is autoimmune thyroiditis. Both a low hemoglobin and higher BMI predict an increased risk. These findings contribute to a better understanding of the pattern and prevalence of maternal thyroid dysfunction and associated risk factors in the Indian population that could improve screening and treatment of gestational thyroid insufficiency.
Footnotes
Acknowledgments
The authors thank the pregnant women and their children for their participation in the study. They are thankful to the doctors, nurses, and technical staff at St. Martha's Hospital for their support. The authors also acknowledge Dr. Sumithra Muthayya for her contribution to the study, and Ms. Madhumitha J, Ms. Menega Mary, Ms. Usha Rani, Ms. Ramya HP, and Ms. Manjula M for technical support. This work was supported by the Nestle Foundation, Lausanne, Switzerland, the ETH Zurich, Switzerland, and Wageningen University, The Netherlands. An abstract of 250 words was presented at the 45th annual conference of the Nutrition Society of India, November 2013.
Author Disclosure Statement
The authors declare that they have nothing to disclose. No competing financial interests exist.