
Abstract
Background:
The tall cell variant (TCV) of papillary thyroid carcinoma (PTC) is an aggressive variant of PTC that is believed to have worse outcomes than classical PTC. The objective of this study was to investigate the incidence, survival, and disease recurrence of patients with TCV and compare them with other PTC in a whole population.
Methods:
Information on all thyroid carcinomas diagnosed in Iceland from 1990 to 2009 was obtained from the Icelandic Cancer Registry. PTC diagnosed postmortem was excluded. The date of diagnosis, sex, and age at diagnosis were registered. All histopathology material was re-evaluated, and papillary thyroid tumors classified as either TCV or other types of PTC. Tumors were classified as TCV if >50% of cells were tall (height > twice the width). TNM stage was determined for all the cases. Endpoints were thyroid cancer–specific death and thyroid cancer recurrence.
Results:
Out of 376 patients diagnosed with PTC in the study period, 49 (13%) were classified as TCV. Patients with TCV were older (66 years vs. 49 years, p<0.001), more often had pT4 tumors (71% vs. 15%, p<0.001), had higher rates of nodal metastasis (51% vs. 22%, p<0.001), and more often distant metastasis (14% vs. 2%, p<0.001). The age-adjusted incidence of TCV for men was 0.5/100,000 [confidence interval (CI) 0.3–0.7] and for women 0.7/100,000 [CI 0.4–1.0] between 1990 and 2009. The five-year disease-specific survival for TCV was 83% [CI 68–91] compared to 98% [CI 96–99] for other PTC respectively (p<0.001). In multivariate analysis, TCV histology was an independent risk factor for recurrence (hazard ratio (HR) 3.18 [CI 1.48–6.84]) but not for disease specific survival (HR 1.86 [CI 0.77–4.73]).
Conclusions:
TCV comprises 13% of all diagnosed PTC in Iceland with an incidence of 0.5/100,000 for men and 0.7/100,000 for women. Patients diagnosed with TCV have worse five-year disease-specific survival than patients with other PTC. TCV histology is an independent risk factor for disease recurrence but not for disease-specific survival.
Introduction
F
It is important for both physicians and patients to know what factors influence the prognosis after the diagnosis of PTC. Therefore, it is important to estimate the effect of different histopathological patterns on both survival and disease recurrence.
Our objectives were to investigate the incidence of the TCV of PTC in a nationwide, population-based study, and to compare both overall and disease-specific survival and recurrence rate of the TCV to other PTC.
Materials and Methods
The Icelandic Cancer Registry (ICR) keeps a record of all malignant tumors in the country as of 1955. The ICR has a completeness of around 99%, and cancer registration is mandatory by Icelandic law (22). Patients are identified through a 10-digit personal identification number assigned to all Icelandic residents. Information stored is mainly limited to age, sex, tumor type, location, and, for the most common tumor types, tumor stage. Thyroid carcinomas are classified into the following four main subtypes: papillary, follicular, medullary, and anaplastic. However, a more detailed pathologic classification such as the TCV subgroup of papillary carcinoma is not well recorded in the ICR.
By accessing the ICR, we identified all patients diagnosed with PTC in Iceland between 1990 and 2009. The median age of patients was 50 years (range 13–87 years). We excluded patients diagnosed with PTC at autopsy. All histopathology material was re-evaluated by the same pathologist with a special experience and interest in thyroid tumors (J.G.J.). PTC was classified as either TCV or other PTC. Other PTCs were not sub-classified into other rare variants such as the diffuse sclerosing or columnar cell variant. Tumors were classified as a TCV if more than 50% of the tumor contained tumor cells that were tall (height > twice the width). The number of sections reviewed for each tumor was very different, and depended on the size of the tumor and how many sections had been prepared. In each case, the pathologist reviewed as many slides as he deemed necessary to make a comfortable diagnosis, distinguishing between the TCV and other PTC. The pathologist was blinded to the outcome of the patients but not to the original diagnosis. Medical records from both The National University Hospital of Iceland and Akureyri Hospital were accessed to determine TNM stage (23). We used information from Statistics Iceland on vital status (alive/dead) and the cause of death for all registered patients.
Patient demographics and TNM stage were compared between patients with TCV and those with other PTC. Patients' medical records were analyzed in order to determine extent of disease at diagnosis in order to determine accurate TNM stage. In addition, patients' medical records and death certificates were analyzed in order to determine if cancer recurrence had occurred and, in the case of deaths, to determine if thyroid cancer had been the cause of death. Disease-specific survival and cancer recurrence were the main endpoints of the study, although overall survival is also reported. Thyroid cancer recurrence was defined as a histologically confirmed diagnosis of thyroid cancer in patients who were believed to be in clinical remission following primary treatment.
Statistical analysis
Continuous variables were compared with the Student's t-test, and categorical variables with the chi-square test. The method of Kaplan–Meier was used to generate survival curves, and the log-rank test to compare curves between the groups. Risk of thyroid cancer–specific death and thyroid cancer recurrence was estimated using Cox proportional regression, and hazard ratios and confidence intervals were calculated. Predictor variables in both statistical models were age, year of diagnosis, sex, TNM stage, and TCV histology. In the thyroid cancer recurrence model, only patients believed to be in clinical remission were included. Patients were positive for the outcome variable if they had a recurrence in the follow-up period. All statistical tests were two-sided, and p-values of <0.05 were considered significant. Incidence calculations were done in Microsoft Excel, and the World standard was used for age standardization. Other statistics were performed with Stata v10 for Windows and Rstudio v3.01.
Results
Out of 376 patients diagnosed with PTC in Iceland from 1990 to 2009, 49 were classified as TCV cases (13%). The age standardized incidence (World) (24) of TCV for men was 0.5/100,000 [confidence interval (CI) 0.3–0.7] and for women 0.7/100,000 [CI 0.4–1.0]. The incidence did not change significantly in the 20-year time period.
Patient demographics and tumor characteristics for TCV patients and other PTC patients are shown in Table 1. Patients with the TCV were older (66 years vs. 49 years, p<0.001), more frequently had T4 tumors (71% vs. 15%, p<0.001), and had higher rates of nodal metastasis (51% vs. 22%, p<0.001) as well as distant metastasis (14% vs. 2%, p<0.001).
TCV, tall cell variant; PTC, papillary thyroid carcinoma.
Five-year overall survival was 69% [CI 54–80] for TCV patients compared to 94% [CI 91–96] for patients with other PTC (p<0.001; Fig. 1).
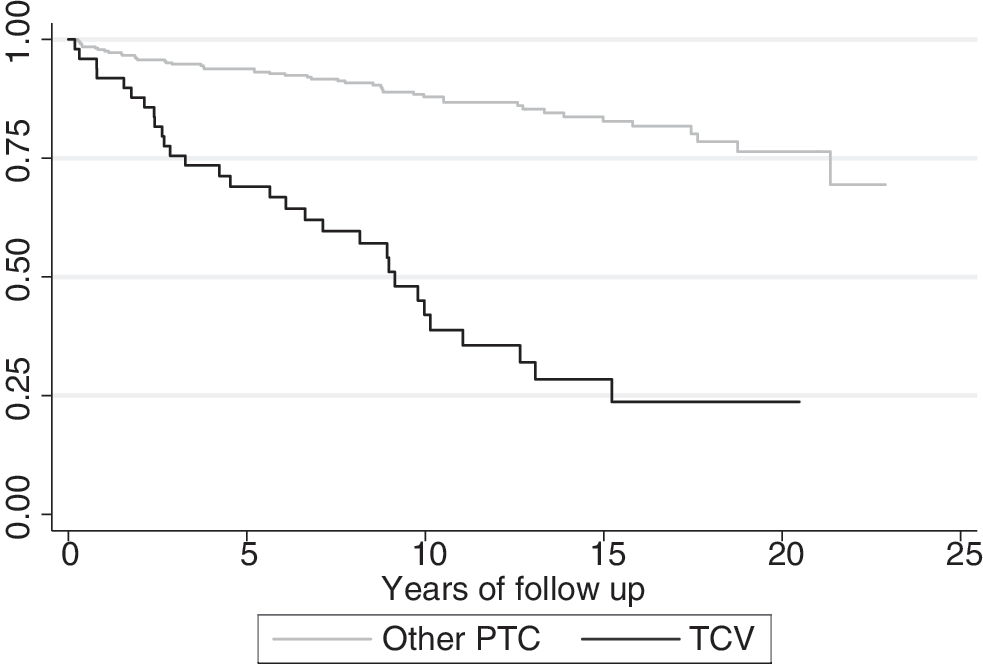
Kaplan–Meier survival estimates for tall cell variant (TCV) and other papillary thyroid carcinoma (PTC; overall survival).
Five-year disease-specific survival was 83% [CI 68–91] for patients with TCV compared to 98% [CI 96–99] for patients with other PTC (p<0.001). Ten-year disease-specific survival was 64% [CI 44–78] for TCV and 96% [CI 94–98] for other PTC. Mean follow-up time was 7.7 years for TCV and 10.9 years for other PTC (Fig. 2).
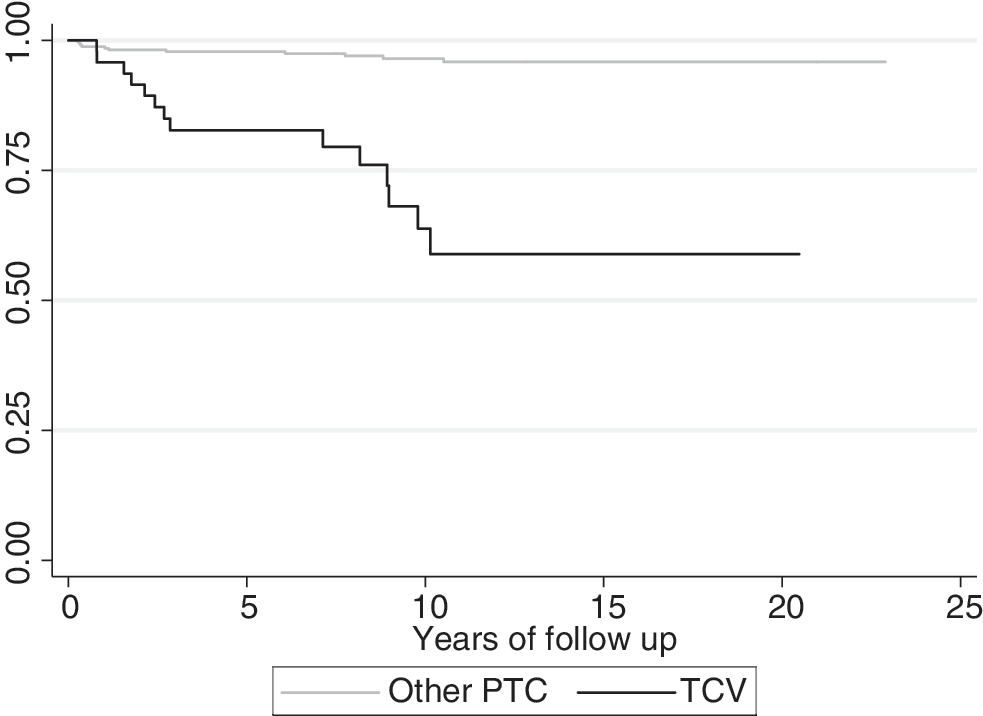
Kaplan–Meier survival estimates for TCV and other PTC (disease-specific survival).
Risk factors for thyroid cancer–specific death are shown in Table 2. When corrected for age, year of diagnosis, sex, and TNM stage, the TCV histology was not an independent risk factor for thyroid cancer–specific death (hazard ratio (HR) 1.86 [CI 0.77–4.73]).
CI, confidence interval.
Complete clinical remission following primary treatment was not achieved in 15 cases (4%), and they were excluded from the recurrence model; nine of those had TCV. Out of 361 patients included in the calculations, 44 (12%) experienced recurrence, 15 of which had TCV. Risk factors for thyroid cancer recurrence are shown in Table 3. TCV histology was a significant risk factor for recurrence when corrected for age, year of diagnosis, sex, and TNM stage (HR 3.18 [CI 1.48–6.84]).
Discussion
The proportion of TCV in patients diagnosed with PTC was 13% in our study. This proportion is higher than in most recent studies, where it ranges from 3.7% to 17%. Ito et al. reported a proportion of 3.7% (11), and Michels et al. a proportion of 8.4% (18). In both of these studies, all histopathology material was reviewed by one pathologist, but while Ito et al. set the proportion of tall cell pattern required for diagnosis of TCV at 50%, Michels et al. set the criteria at 30%. These studies were not population-based and not supported by a centralized cancer registry. Ghossein et al. reported 10% of thyroid tumors as TCV, and their diagnostic criteria for TCV were the same as in our study. Not all of their histopathology material was reviewed, and their cohort was from a single institution (12). The diagnosis of TCV is subject to observer variability, especially since the criteria for diagnosis of this variant is variable between studies.
One of the problems with studies on TCV is the relative paucity of cases in reported studies. They mostly range from 7 to 63 (11,16 –19), but two recent studies by Morris et al. and Kazaure et al. reported 278 and 573 TCV cases respectively. Both Morris et al. and Kazaure et al. used information from the Surveillance, Epidemiology, and End Results Program cancer registry in the United States, which captures around 26% of the U.S. population. However, this registry does not have a centralized pathology review, and their data rely on medical records from treating hospitals. Kazaure et al. reported an increasing incidence of TCV between 2001 and 2008 (0.05/100,000–0.13/100,000, age-adjusted for 2000 U.S. population), which is much lower than the incidence in Iceland, which is 0.5/100,000 for males and 0.7/100,000 for females (9,10).
TCV is diagnosed at an older age and more frequently diagnosed in males compared to other PTC variants. Both these parameters are associated with worse survival of PTC (10). The TCV patients in our study had a mean age of 66 years, which is also high when compared to other studies where the mean age of TCV patients ranges from 50 to 55 years (9,10,16,18,19). TCV patients also have significantly worse pathologic parameters; 70% have T4 tumors, which indicates extrathyroidal extension at the time of diagnosis, 50% have lymph node metastasis, and 14% distant metastases. TCV patients in Iceland clearly have a worse five-year disease-specific survival than other PTC variants (83% vs. 98%). With longer follow-up, the disease-specific survival for TCV patients becomes even worse (64% vs. 96% at 10 years), indicating that even with longer follow-up, patients with PTC variants other than TCV have an excellent survival compared to TCV. Older individuals diagnosed with PTC usually have a worse prognosis than younger patients, and it has been hypothesized that PTC tumors evolve through time into more aggressive variants such as TCV and, at that time, patients have acquired extrathyroidal extension or distant metastases (25).
As TCV patients are older and are more likely to have nodal disease and distant metastases at diagnosis, there is a debate over whether TCV histology alone is an independent risk factor for worse survival. Many studies have produced similar results as ours regarding patients survival (18,19,26). However, in contrast, two recent studies from Kazaure et al. and Morris et al. had more TCV cases than any other published studies, and both found that TCV histology was an independent risk factor for worse survival (9,10). Morris et al. matched TCV and PTC cases for age, sex, extrathyroidal extension, lymph node metastasis, and distant metastasis, and found that TCV cases had an 81.9% five-year survival compared to 91.3% for matched PTC patients. Kazaure et al. used a Cox proportional hazards model similar to ours with 43.738 patients and 573 TCV cases, and they found TCV histology to be a risk factor (HR 1.9). In our study, TCV histology was not an independent risk factor for cancer-specific death. However, TCV histology was an independent risk factor for thyroid cancer recurrence with a threefold increase in recurrence compared to other PTC. This is an important finding, as these patients might require closer follow-up.
Clinicians treating patients should be aware of this information, and pathologists should report tumors with tall cell features, since this is important when making decision on treatment and follow-up of patients. Patients with TCV should be under closer surveillance and may need more aggressive treatment than patients with other PTC variants. However, despite the worse outcome of TCV patients, the most important prognostic factor still remains the TNM stage, which should be the main basis for decision on treatment.
The main strength of our study is that we have a well-defined population including the whole population of Iceland, and our centralized cancer registry captures more than 99% of cancers. An experienced pathologist reviewed all PTC specimens for the 20-year period and separated the TCV variant from other PTC. This is important because TCV is often missed by pathologists (12,17). We also have complete follow-up data, as statistics on vital status recurrent disease and the cause of death for all Icelandic residents is stored by Statistics Iceland with the use of personal identification numbers unique to each resident.
There are a few limitations to our study. First, we only have 49 TCV cases; this is similar to most studies but less than in the studies by Morris et al. and Kazaure et al. (9,10). The reviewing pathologist was not blinded to the original diagnosis of patients, and this may have led to a detection bias. However, we believe this risk is minimal, as the pathologist was blinded to the outcome of the patients. We also do not have information on differences in treatment of the patients.
Conclusion
TCV comprises 13% of all diagnosed PTC in Iceland with an incidence of 0.5/100,000 for men and 0.7/100,000 for women. Patients diagnosed with TCV have a substantially worse five-year disease-specific survival than patients with other PTC. TCV histology is an independent risk factor for disease recurrence but not for disease-specific survival.
Footnotes
Acknowledgment
The abstract has been presented as an oral presentation at the ANCR 2013 meeting in Reykjavik, Iceland.
Author Disclosure Statement
No competing financial interests exist.