
Abstract
Background:
While there is a large body of evidence showing a significant impact of controlled ovarian hyperstimulation (COH) on thyroid function in euthyroid patients undergoing in vitro fertilization (IVF), information on the effect of this treatment on thyroid axis equilibrium in hypothyroid-treated patients is insufficient. The goal of this prospective study was to investigate serum thyroid-stimulating hormone (TSH) modifications in hypothyroid-treated patients during IVF.
Methods
: Hypothyroid-treated women selected for IVF between November 2010 and December 2011 were considered for study entry. They were eligible if serum TSH tested the month preceding the IVF cycle was 0.4–2.5 mIU/L. Additional inclusion criteria were as follows: (1) a certified diagnosis of clinical or subclinical hypothyroidism; (2) consumption of at least 25 μg of levothyroxine daily; (3) serum free triiodothyronine and free thyroxine tested the month preceding the IVF cycle within the reference range; (4) no previous IVF cycles; (5) regular menstrual cycles; and (6) day 3 serum follicle-stimulating hormone <12 IU/mL and anti-Müllerian hormone >0.5 ng/mL. Serum TSH was tested at three time points: between day 1 and day 8 of the cycle during the month preceding the start of controlled ovarian hyperstimulation (COH), at the time of human chorionic gonadotropin (hCG) administration and at 16 days after hCG administration.
Results:
Seventy-two women met our selection criteria. The serum levels of TSH at basal assessment, at the time of hCG administration, and at 16 days after hCG administration were 1.7±0.7, 2.9±1.3, and 3.2±1.7 mIU/L, respectively. All pairwise comparisons were statistically significant. Serum TSH exceeded the threshold of 2.5 mIU/L in 46 subjects at the time of hCG administration (64%, [CI: 53–75%]) and in 49 subjects 16 days after hCG administration (68%, [CI: 57–79%]).
Conclusions:
Serum TSH increased considerably during COH in adequately treated hypothyroid women undergoing IVF. We suggest strictly monitoring these women during IVF cycles and, if necessary, promptly adjusting the levothyroxine dose. This is the most pragmatic approach but, to date, it is not supported by clinical evidence. Further studies aimed at clarifying the most suitable therapeutic strategy are thus warranted.
Introduction
C
While modifications of thyroid function during IVF cycles have been extensively investigated in euthyroid women, evidence on the impact of COH on the thyroid axis equilibrium in hypothyroid-treated women is extremely scarce. Stuckey et al. reported a rise in TSH to hypothyroid levels during ovulation induction for IVF in two patients taking thyroxine replacement therapy and who were euthyroid at the start of the cycle (12). In a subsequent prospective study, Gracia et al. observed a more pronounced elevation of serum TSH during IVF in nine hypothyroid-treated women when compared with the 48 euthyroid controls (5). Although these results suggest a compromised capacity to adapt to the COH-related increased thyroid function, the sample size of these contributions is insufficient to draw robust conclusions.
On this basis, we deemed a more detailed investigation of the capacity of women with treated hypothyroidism to adapt to the increased demands associated with COH as being of interest. These women may actually represent a group of patients requiring some additional care during IVF. We thus set up a prospective study in 72 hypothyroid-treated women undergoing IVF. We included women with well-compensated hypothyroidism (i.e., those with a serum TSH prior to beginning IVF of 0.4–2.5 mIU/L) and monitored serum TSH modifications during treatment.
Materials and Methods
Hypothyroid-treated women selected for IVF between November 2010 and December 2011 at the Infertility Unit of the Fondazione Ca' Granda Ospedale Maggiore Policlinico were considered for study entry. They were eligible if serum TSH tested the month preceding the IVF cycle was 0.4–2.5 mIU/L (13). Additional inclusion criteria were as follows: (1) a certified diagnosis of clinical or subclinical hypothyroidism; (2) daily use of at least 25 μg of levothyroxine; (3) serum free triiodothyronine (fT3) and free thyroxine (fT4) tested the month preceding the IVF cycle within the reference range; (4) no previous IVF cycles; (5) regular menstrual cycles; and (6) day 3 serum follicle-stimulating hormone (FSH) <12 IU/mL and anti-Müllerian hormone >0.5 ng/mL. Women who did not complete the treatment cycle and those failing to refer for the three assessments were subsequently excluded. The local institutional review board of the Fondazione Ca` Granda Ospedale Maggiore Policlinico approved the study (approval number 2402/10), and all recruited patients signed an informed consent.
Selected women underwent basal transvaginal ultrasound between day 1 and day 8 of the cycle during the month preceding the start of COH. Serum TSH and serum antibodies directed against thyroperoxidase (TPO) and thyroglobulin (TG) were tested at this time. Women were subsequently monitored and managed according to a standardized clinical protocol as reported previously (14). Briefly, the stimulation protocol and the dose-type of recombinant FSH (Gonal-F®) were determined on an individual basis according to age, serum hormonal tests, and antral follicle count. Patients underwent serial transvaginal ultrasound and hormonal monitoring during hyperstimulation. When three or more leading follicles with a mean diameter >18 mm were visualized, 250 μg of recombinant human chorionic gonadotropin (hCG) (Ovitrelle®) was administered subcutaneously. The second serum TSH assessment was conducted the same day. Oocyte retrieval was performed transvaginally 36 h after the hCG injection. Embryo transfer was performed 48–72 h after oocyte collection. Cycles were cancelled if there was a poor or hyper-response. We defined hyper-response as a serum estradiol concentration >4000 pg/mL and/or more than 20 follicles identified on ultrasound scan before hCG administration. Poor response was defined by the echographic evidence of fewer than three follicles during ovarian hyperstimulation.
Serum hCG assessment was performed 16 days after hCG administration to ascertain the development of pregnancy. The third serum TSH was scheduled on the same day. All blood samples were obtained between 9:00 a.m. and 12:00 a.m.
Clinical pregnancy was defined as the ultrasonographic demonstration of a viable embryo within an intrauterine gestational sac 4–5 weeks after embryo transfer. The implantation rate was calculated as the ratio between the number of gestational sacs identified at this time and the number of embryos transferred. Levothyroxine dose was not adjusted at the time of the first two TSH measurements. On the other hand, women whose serum TSH exceeded 2.5 mIU/L at 16 days after hCG administration were referred to the endocrinologist for further thyroid function evaluation and modification of the dose of levothyroxine.
Serum TSH was tested using the Immulite analyzer, a fully automated solid-phase third generation immunoassay analyzer with a chemiluminescent detection system (Diagnostic Products Corp.). The intra- and inter-assay coefficients of variation around the values of normal range were both <10%. TPO and TG antibodies were measured using commercial diagnostic kits involving an immunofluorescence assay (Phadia; Thermo Scientific), with normal values set at <35 IU/L (anti-TPO) and <40 IU/L (anti-TG).
Women were diagnosed with overt hypothyroidism if serum TSH was >2.5 mIU/L and serum concentrations of free thyroxine or triiodothyronine were outside their reference ranges. Subclinical hypothyroidism was defined as serum TSH >2.5 mIU/ L and free thyroid hormones within the reference range. Thyroid autoimmunity was defined as the presence of serum antibodies directed against TPO and/or TG (13).
Data analysis was performed using the Statistics Package for Social Sciences (SPSS 18.0). Data were compared using ANOVA for repeated measures, Student's t test, Wilcoxon test for unpaired data, or Fisher's exact test, as appropriate. A binomial distribution model was used to calculate the 95% confidence interval [CI] of proportions. The sample size was calculated considering a 20% increase in serum TSH as being clinically relevant. Based on our preliminary data on serum TSH in women with treated hypothyroidism and setting type I and II errors at 0.05 and 0.20, respectively, the required sample size consisted of about 70 women. p Values below 0.05 were considered statistically significant.
Results
Seventy-two women met our selection criteria. The serum levels of TSH at basal assessment, at the time of hCG administration and at 16 days after hCG administration were 1.7±0.7, 2.9±1.3 and 3.2±1.7 mIU/L, respectively (Fig. 1). All comparisons were statistically significant. The mean [95% CI] increase from baseline to the time of hCG administration and from baseline to 16 days after hCG administration was 71% [CI: 47–87%] and 88% [CI: 66–97%], respectively. Serum TSH at the time of hCG administration exceeded the threshold of 2.5 mIU/L in 46 subjects, corresponding to 64% [CI: 53–75%]. This occurred in 49 subjects (68% [CI: 57–79%]) at 16 days after hCG administration. Taking 4.5 mIU/L as the threshold, serum TSH was higher than this limit in five women (7% [CI: 3–15%]) at the time of hCG administration and in 12 women (17% [CI: 10–27%]) at 16 days after hCG administration. Serum TSH below 0.4 mIU/L at the time of hCG administration was not observed in any of the studied cases, but was observed in one pregnant woman 16 days after hCG administration. The baseline characteristics and cycle outcome of women whose serum TSH did and did not exceed the threshold of 2.5 mIU/L at the time of hCG administration are shown in Table 1. No statistically significant differences were observed. This analysis was repeated for patients whose serum TSH did and did not exceed the threshold value at 16 days after hCG administration, and again, no significant differences were observed (data not shown).
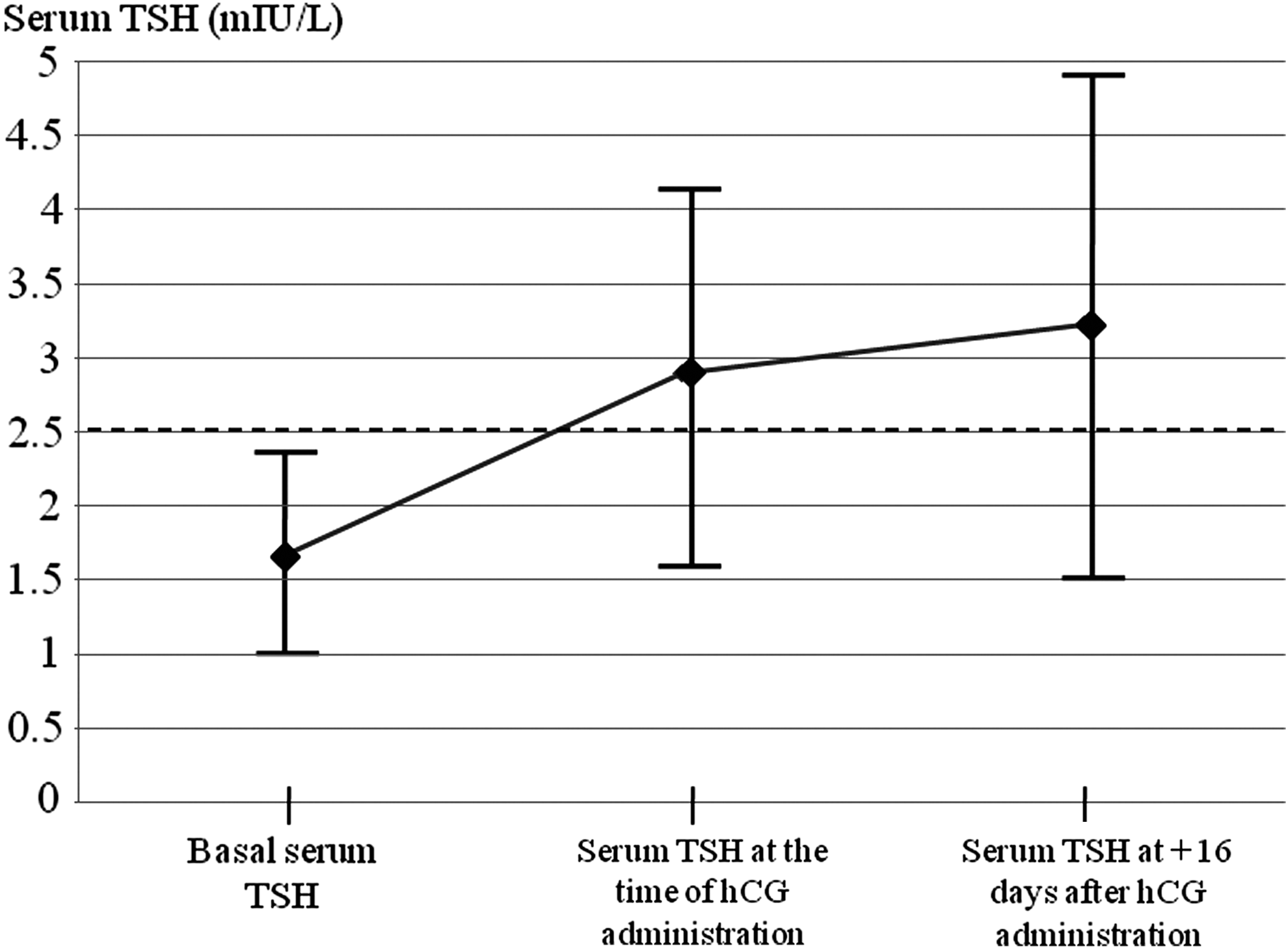
Serum levels of thyroid-stimulating hormone (TSH) at basal assessment, at the time of human chorionic gonadotropin (hCG) administration and at +16 days after hCG administration. A statistically significant increase occurred between basal levels and levels at the time of hCG administration (p<0.001), between basal levels and levels at +16 days after hCG administration (p<0.001), and between levels on the day of hCG administration and those at +16 days from hCG administration (p=0.031). Data are expressed as mean±standard deviation.
Data are reported as number (%) or mean±standard deviation, as appropriate.
AFC, antral follicle count; AMH, anti-Müllerian hormone; BMI, body mass index; FSH, follicle-stimulating hormone; FT3, free triiodothyronine; FT4, free thyroxine; GnRH, gonadotropin-releasing hormone; hCG, human chorionic gonadotropin; IVF-ICSI, in vitro fertilization–intracytoplasmic sperm injection; TSH, thyroid-stimulating hormone.
The modifications of serum TSH were separately evaluated in different subgroups: women with and without thyroid autoimmunity, those with subclinical hypothyroidism and overt hypothyroidism, and in pregnant and nonpregnant women. These results are summarized in Table 2. In patients with thyroid autoimmunity an intragroup analysis according to the specific antibodies detected (anti-TPO or anti-TG) was also performed but failed to document any significant result (data not shown). Comparison between women who did and did not achieve pregnancy is illustrated in Table 3.
Data are expressed as mean±standard deviation.
Time 1, basal assessment; Time 2, at hCG administration; Time 3, at +16 days after hCG administration.
Data are expressed as mean±standard deviation or median (interquartile range).
Time 1, basal assessment; Time 2, at hCG administration; Time 3, at +16 days after hCG administration.
Discussion
Serum TSH increases considerably during COH in adequately treated hypothyroid women undergoing IVF. This increase mainly occurs during gonadotropin treatment (i.e., prior to hCG administration). Thereafter, serum TSH continues to increase, but the change is less prominent and is statistically significant only in women who achieve pregnancy. Of utmost relevance is that serum TSH exceeds the recommended threshold of 2.5 mIU/L in up to two thirds of patients. Overall, the pattern of serum TSH modification is similar to that observed in euthyroid women, but the magnitude of the modifications is more pronounced and the rate of women exceeding the threshold of 2.5 mIU/L is almost two-fold higher (1 –7). We speculate that this result is due to the inability of a compromised thyroid to face the increased demand for thyroid hormones during COH.
In our study, we did not attempt to clarify the causes of these findings. Various hypotheses can however be put forward. In particular, we claim a role for estrogens because they typically rise markedly during COH. Of note, it has been shown that serum estrogens increase circulating thyroid binding globulin (TBG). This modification would result from a combination of factors: increased TBG production and release by the liver and prolonged half-life due to increased glycosylation (15,16). This rise in the number of circulating T4 binding sites would result in a decline in the fT4 index and, as a consequence, in stimulation of the thyrotropic feedback mechanism with a further increase in the TSH serum concentration. These effects may occur in all women during IVF but may be more pronounced in women with hypothyroidism since these women are less able to face the increased demand. Estrogens may also explain the increase after hCG administration in pregnant women. In a prospective study, Ganesh et al. compared the luteal phase hormonal profile in 113 pregnant and 155 nonpregnant women undergoing their first IVF cycle and demonstrated a markedly higher estradiol level in the later part of the luteal phase in those achieving pregnancy (17). This observation is consistent with the reports of other research groups (18 –20) and would explain the different patterns of serum TSH changes in the luteal phase between pregnant and non-pregnant women observed in our study.
Our results have clinical and therapeutic implications. In particular, they highlight the frequent need to adjust the levothyroxine dose in hypothyroid-treated women undergoing COH for IVF. In this regard, we hypothesize two possible management strategies. Firstly, thyroid function should be strictly monitored during the cycle and, if appropriate, the dose of levothyroxine should be promptly adjusted. Alternatively, one may anticipate the adjustment of therapy before starting the cycle. This latter strategy is simpler and may be justified by the high proportion of women exceeding the threshold of 2.5 mIU/L. The observation that due to the long half-life of levothyroxine, dosage adjustments may not reach the steady state equilibrium for 3–5 weeks after changes are made further supports this approach (21). On the other hand, this latter strategy has some relevant drawbacks. In particular, we are unable to infer the magnitude of levothyroxine increase that should be adopted. Moreover, serum TSH did not exceed the threshold in a minority but still relevant proportion of women and we failed to identify predictive factors for this condition. There is actually the risk of inappropriate treatment in a consistent proportion of patients. Future studies are warranted to determine the best therapeutic strategy. In the meantime, the first option (i.e., the strict monitoring of serum TSH and prompt adjustment of the levothyroxine dose) appears more pragmatic and, in our opinion, is preferable.
Some limitations of the study should be recognized. Firstly, we exclusively monitored serum TSH. We did not assess serum free T4 modifications. However, there is a strong inverse log-linear relationship between serum TSH and serum free T4 concentrations. Small changes in T4 concentrations provoke relevant changes in serum TSH, and we thus deemed it unnecessary to monitor this variable (22). Secondly, we speculate that adjustment of the levothyroxine dose is necessary, but our data actually failed to document any effect on IVF outcomes. The chances of pregnancy did not differ between women whose serum TSH did or did not exceed the 2.5 mIU/L threshold. However, it should be noted that our study was underpowered to address this issue. Moreover, there is a large body of evidence supporting the importance of adequately treating hypothyroidism already in the earliest stages of pregnancy (8,10,11,22). The Endocrine Society actually recommends prompt levothyroxine replacement in pregnancy for women with both overt and subclinical hypothyroidism (9). Thirdly, we arbitrarily decided to use 2.5 mIU/L as a threshold. It would have been more appropriate to refer to a local threshold since reference range may vary among different populations and is not always correct to use the same threshold for all populations. Unfortunately, we failed to identify large well-designed studies on serum TSH in childbearing women in our area. On the other hand, we do not deem that this inaccuracy might significantly affect our conclusions. Moreover, it has to be noted that 2.5 mIU/L is commonly used as a threshold in studies from several independent areas.
In conclusion, in adequately treated hypothyroid women, the serum TSH concentration increases significantly during COH in IVF cycles. Of particular relevance from a clinical perspective is the high proportion of patients in whom the serum TSH exceeds the recommended threshold of 2.5 mIU/L. Based on our findings, we suggest strictly monitoring serum TSH in hypothyroid-treated women during IVF cycles and, if necessary, prompt adjustment of the levothyroxine dose. This is the most pragmatic approach despite the fact that, to date, it is not supported by clinical evidence. Further studies aimed at clarifying the most suitable therapeutic strategy are warranted.
Footnotes
Author Disclosure Statement
No competing financial interests exist.