
Abstract
Background:
Vitamin D has recently attracted attention because reduced levels are associated with the prevalence and aggressiveness of several cancers. This study aimed to evaluate the relationship between preoperative serum 25 hydroxyvitamin D (25(OH) vitamin D) levels and clinicopathologic characteristics in female patients with papillary thyroid cancer (PTC).
Methods:
A total of 548 female patients who underwent total thyroidectomy for PTC between June 2012 and May 2013 were included. Blood samples were obtained within two weeks prior to surgery. Patients were categorized into four quartiles by preoperative serum 25(OH) vitamin D levels. The clinicopathologic features of PTC were analyzed retrospectively.
Results:
Preoperative 25(OH) vitamin D was significantly lower in patients with a tumor size of >1 cm (p=0.041) or lymph node metastasis (LNM; p=0.043). No significant trends in several clinicopathologic features were observed in relation to increasing serum vitamin D concentrations except decreasing tumor size (p=0.010). Patients in the second quartile had a greater occurrence of T stage 3/4 (odds ratio (OR) 2.03 [confidence interval (CI) 1.19–3.44]; p=0.009), LNM (OR 2.03 [CI 1.19–3.44]; p=0.009), lateral LNM (OR 5.03 [CI 1.66–15.28]; p=0.004), and extrathyroidal extension (ETE; OR 1.95 [CI 1.15–3.29]; p=0.013) than those in the fourth quartile. Multivariate analysis showed that patients in the second quartile had a greater occurrence of T stage 3/4 (OR 1.89 [CI 1.08–3.30]; p=0.026), LNM (OR 2.04 [CI 1.20–3.47]; p=0.009), lateral LNM (OR 5.12 [CI 1.68–15.59]; p=0.004), and ETE (OR 1.81 [CI 1.04–3.15]; p=0.036) than those in the fourth quartile. When the subjects were recategorized into two groups by median 25(OH) vitamin D levels, those with values below the median had a significantly higher risk of T stage 3/4, LNM, lateral LNM, stage III/IV, and ETE. All values except ETE sustained significance after adjustment.
Conclusion:
Lower preoperative serum 25(OH) vitamin D levels appear to be associated with poor clinicopathologic features in female patients with PTC.
Introduction
V
Although controversy is present, some prospective observational and meta-analysis studies have reported lower vitamin D levels may increase the risk of several cancers, including colorectal, breast, prostate, and bladder cancer (9 –12). Further, vitamin D insufficiency has been reported to be related to an advanced cancer stage and increased incidence of metastasis and recurrence in colorectal, breast, and prostate cancer (11,13,14). To date, however, very few studies have investigated the relationship between vitamin D and thyroid cancer. One study found vitamin D deficiency, defined as levels below the threshold of 37.5 nmol/L (15 ng/mL), had an inverse relationship with the incidence of well-differentiated thyroid cancer (15). Meanwhile, low levels of 1,25 hydroxyvitamin D [1,25(OH)2 vitamin D] but not 25(OH) vitamin D showed a significant relationship with thyroid cancer (16,17).
Only a limited number of studies have examined the association between 25(OH) vitamin D and clinicopathologic features for various cancers, with only one previous study addressing this type of association for thyroid cancer. However, only a small number of patients and clinicopathologic characteristics were evaluated in this previous pilot study (18). Based on the above-mentioned studies with respect to various cancers, we hypothesized low vitamin D levels would be associated with a poor prognosis in patients with papillary thyroid cancer (PTC). The study aimed to evaluate the correlations between preoperative 25(OH) vitamin D and various clinicopathologic features in patients with PTC.
Materials and Methods
A total of 773 patients underwent total thyroidectomy for thyroid cancer at Pusan National University Hospital from June 1, 2012, to May 31, 2013. Of these, only patients diagnosed with PTC were included in the study because (a) the number of patients with follicular thyroid cancer (n=8) and medullary thyroid cancer (n=1) were too small (9/773; 1.2%) for analysis, and (b) the characteristics of follicular and medullary thyroid cancers differ from those of PTC. Patients were excluded if they were diagnosed with nonthyroidal malignancies before surgery (33/773; 4.3%); had been taking multivitamins, calcium supplements, vitamin D supplements, or bisphosphonate medication (35/773; 4.5%); or were male (90/773; 11.6%). Male patients were excluded because women represent a very high proportion of thyroid cancer patients, and sexual differences are present in vitamin D metabolism. Corrected calcium (corrected Ca=0.8×(4.0 − serum albumin)+total calcium) and intact parathyroid hormone (iPTH) were measured. Patients were excluded if values were outside the reference range (41/773; 5.3%). The estimated glomerular filtration rate (GFR) was calculated using the Modification of Diet in Renal Disease equation (estimated GFR=1.86×(PCr)−1.154×(age)−0.203×0.742 for women). If the estimated GFR was <60 mL/min/1.73 m2, the patients were excluded (17/773; 2.2%). A total of 548 female patients with PTC met the inclusion criteria for analysis in this study. Central compartment neck dissection was routinely performed during total thyroidectomy. Selective neck dissection was performed if metastasis was revealed by ultrasonography or computed tomography findings, or shown by positive cytological results for samples obtained by preoperative fine-needle aspiration from enlarged cervical neck lymph nodes.
Clinical characteristics and demographic data were collected by retrospective chart review. The patient population was classified into those <45 years old and those ≥45 years old, since the general prognosis is worse in the latter patient group (19). Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Seasonal differences were defined by the laboratory sampling date. To adjust for the effect of season on serum 25(OH) vitamin D levels, we categorized patients into four different seasonal groups: group 1, from June to August; group 2, from September to November; group 3, from December to February; group 4, from March to May. Tumor size was defined as the greatest cancer diameter based on postoperative biopsy results. A cutoff value of >1 cm was used for the tumor size, since a tumor size of ≤1 cm was used in the investigation of papillary thyroid microcarcinoma (20). We applied the TNM classification system of the American Joint Committee on Cancer (AJCC) (19). The T stage was classified into 1/2 versus 3/4; the N stage into LNM (N0 vs. N1) and lateral LNM (N0 and N1a vs. N1b); the tumor stage into I/II versus III/IV. Hashimoto's thyroiditis was defined based on postoperative biopsy samples showing extensive infiltration of lymphocytes, plasma cells, and macrophages, substantial formation of lymphoid follicles, and numerous reactive germinal centers.
Blood samples were obtained within two weeks prior to total thyroidectomy, while 25(OH) vitamin D, corrected calcium, iPTH, estimated GFR, and thyrotropin (TSH) were simultaneously measured before surgery. Serum 25(OH) vitamin D was determined by immunoradiometric assay using a 25 OH Vitamin D3 RIA kit (DIAsource ImmunoAssays S.A., Louvain-la-Neuve, Belgium). Patients were categorized into four quartiles by preoperative serum 25(OH) vitamin D levels: quartile 1 (min–max (ng/mL): 3.91–13.62), quartile 2 (13.70–18.52), quartile 3 (18.57–26.23), and quartile 4 (26.26–59.31). Patients were subsequently recategorized into two groups according to the serum 25(OH) vitamin D median concentration (18.57 ng/mL). The iPTH was measured using the total iPTH IRMA kit (IBL Gesellschaft für Immunchemie und Immunbiologie mbH, Hamburg, Germany). The reference range for iPTH was 10–65 pg/mL. TSH was measured by immunoradiometric assay using a commercial kit (Coat-A-Count, TSH IRMA; DPC, Inc., Los Angeles, CA).
Informed consent was obtained from all patients at the time of surgery. This study was approved by the Institutional Review Board at Pusan National University Hospital, Busan, Korea.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows v21.0 (IBM Corp., Armonk, NY). Because serum 25(OH) vitamin D was not normally distributed according to the Kolmogorov–Smirnoff test, the results are expressed as the median value and interquartile range (IQR). Age, tumor size, BMI, and TSH were evaluated as continuous variables. To adjust for the effects of season and month of blood collection, we categorized the patients into four different seasonal groups (described above) and calculated adjusted odds ratios (ORs). Next, we calculated standardized 25 (OH) vitamin D levels through regression of 25(OH) vitamin D levels on the periodic function − sin(2πx/12) − cos(2πx/12), where x is the sample collection month (21,22). Student's t-test was used to perform comparisons between two groups. One-way analysis of variance (ANOVA) was conducted in the comparison of LNM. One-way ANOVA and Pearson's chi square test were conducted in the comparison of the different quartile groups. Pearson correlation coefficient was determined between tumor size and standardized 25(OH) vitamin D by simple linear regression analysis. Crude ORs and confidence intervals (CIs) were calculated with a univariate logistic regression model. Factors related to T stage 3/4, LNM, lateral LNM, stage III/IV, and extrathyroidal extension (ETE) were evaluated with multivariate logistic regression analysis. Adjusted ORs were calculated after controlling for model 1 (age) and model 2 (model 1+BMI, seasonal differences, TSH). A p-value of <0.05 was considered significant.
Results
The 548 female patients ranged in age from 15–80 years (M (SD): 49.8 (10.9)). The median preoperative serum 25(OH) vitamin D level was 18.5 ng/mL (IQR: 12.6). The mean tumor size (SD) and number of PTCs (SD) were 0.77 (0.23 cm; range 0.1–3.7 cm) and 1.51 (0.04; range 1–7) respectively. Table 1 shows the patient and tumor characteristics.
Data are expressed as the median (interquartile range).
Statistical significance was tested by one way analysis of variance.
25(OH) vitamin D, 25 hydroxyvitamin D; IQR, interquartile range; ETE, extrathyroidal extension; LVI, lymphovascular invasion.
Serum 25(OH) vitamin D was significantly higher in patients who were <45 years of age as compared to those who were ≥45 years old (18.9 vs. 17.5 ng/mL; p=0.029) and in patients with a tumor size of <1 cm than in those with a tumor size of ≥1 cm (18.9 vs. 16.4 ng/mL, p=0.041; Table 1). Serum 25(OH) vitamin D levels were also significantly decreased in patients with LNM (N0 vs. N1a vs. N1b; 16.2 vs. 17.4 vs. 19.2 ng/mL; p=0.043). Although T stage 3/4, lateral LNM, distant metastasis, stage III/IV, positive results for multifocality, ETE, lymphovascular invasion (LVI), and presence of a BRAF mutation showed reduced serum 25(OH) vitamin D, no statistical significance was evident. No differences in serum 25(OH) vitamin D levels were observed between patients with or without Hashimoto's thyroiditis.
When patients were categorized into quartiles, no trends were observed in terms of age, BMI, or TSH (Table 2). Meanwhile, tumor size decreased from the first quartile to the fourth quartile (p=0.010). A left-skewed distribution of 25(OH) vitamin D levels was evident in patients with LNM as the quartile number increased (33.6%, 37.2%, 27%, 22.6%; p=0.014). With the exception of multifocality and BRAF mutation, other factors also showed a left-skewed pattern as the quartile number increased. However, no significant trends were observed with respect to these parameters. Only three patients had distant metastasis: one in the first quartile, and two in the second quartile.
Data are expressed as *mean±standard deviation, †median (IQR), or n (%). * ,†Statistical significance was tested by one-way analysis of variance or the chi square test.
BMI, body mass index; TSH, thyrotropin; LNM, lymph node metastasis.
As shown by simple linear regression analysis, tumor size increased with decreasing standardized 25(OH) vitamin D levels (r=−0.105, p=0.014; Fig. 1). The relationship remained significant following adjustment for age, BMI, seasonal differences, and TSH (r=−0.081, p=0.048).
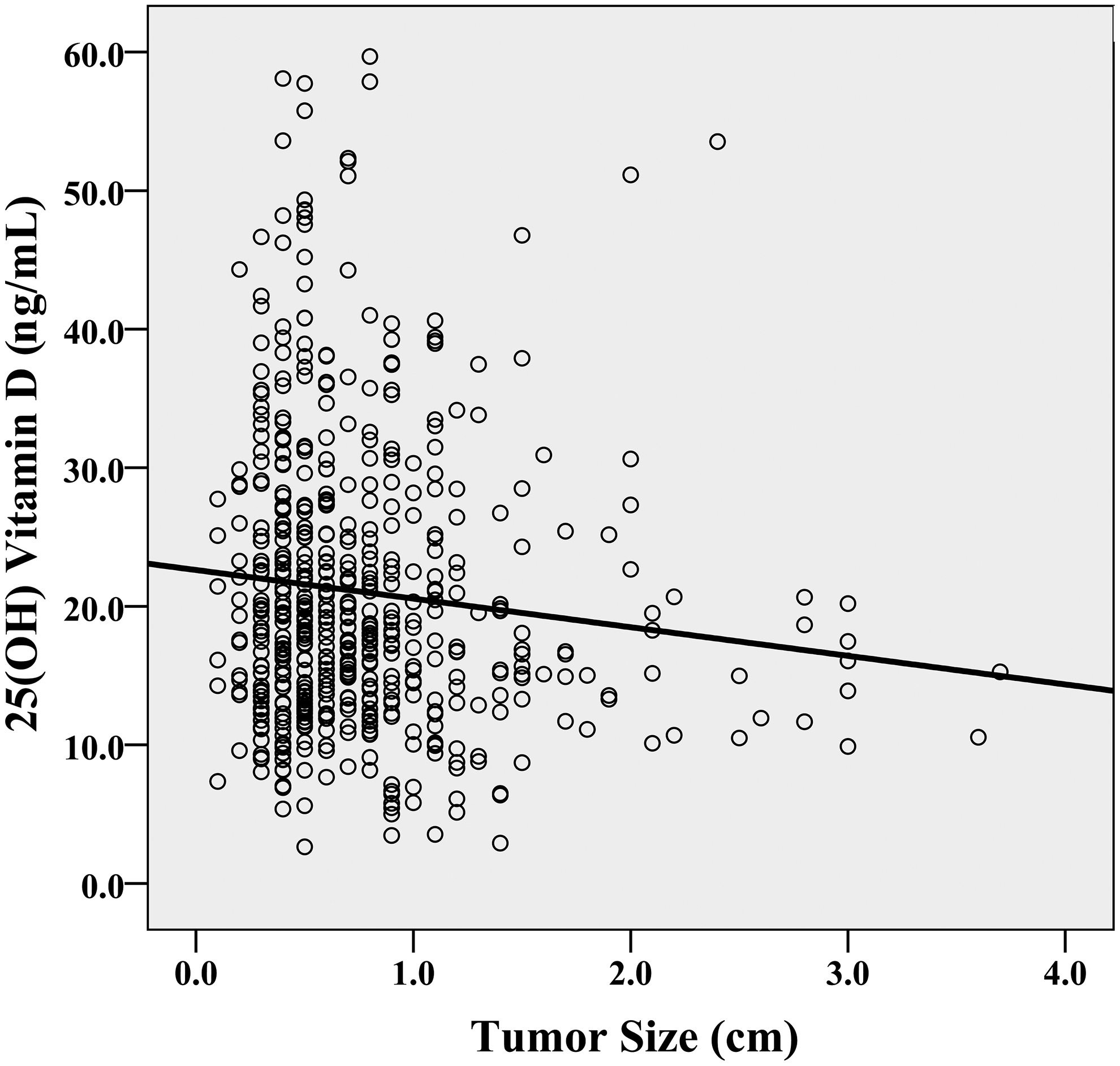
Simple linear regression analysis between tumor size (cm) and 25(OH) vitamin D (ng/mL). r=−0.105; p=0.014.
Table 3 shows the results of a univariate logistic regression with unadjusted ORs in which the 4th quartile was established as a reference (unadjusted OR for all parameters=1). Compared to the fourth quartile, the second quartile showed an unadjusted OR of 2.03 for T stage 3/4 ([CI 1.19–3.44]; p=0.009), 2.03 for LNM ([CI 1.19–3.44]; p=0.009), 5.03 for lateral LNM ([CI 1.66–15.28], p=0.004), and 1.95 for ETE prevalence ([CI 1.15–3.29], p=0.013). When the lowest and highest quartiles were compared, only the risk of LNM was statistically significant (OR 1.73 [CI 1.01–2.95]; p=0.045).
OR, odds ratio; CI, confidence interval.
Multivariate logistic regression analysis was conducted to examine the interaction between poor clinicopathologic features and age, BMI, seasonal differences, and TSH on serum 25(OH) vitamin D (Table 4). In model 1, the second quartile as compared with the fourth quartile had a significantly higher risk of T stage 3/4 (OR 2.07 [CI 1.22–3.52]; p=0.007), LNM (OR 2.00 [CI 1.18–3.41]; p=0.010), lateral LNM (OR 5.03 [CI 1.66–15.28]; p=0.004), and ETE prevalence (OR 1.98 [CI 1.17–3.36]; p=0.011). In model 2, the same relationship was observed for T stage 3/4 (OR 1.89 [CI 1.08–3.30]; p=0.026), LNM (OR 2.04 [CI 1.20–3.47]; p=0.009), lateral LNM (OR 5.12 [CI 1.68–15.59]; p=0.004), and ETE prevalence (OR 1.81 [CI 1.04–3.15]; p=0.036). When the first and fourth quartiles were compared, only LNM showed statistical significance in model 2 (OR 1.72 [CI 1.00–2.95]; p=0.048).
Model 1 was adjusted for age; model 2 was adjusted for the variables in model 1 plus BMI, seasonal differences, and TSH.
When patients were recategorized into two groups according to median serum 25(OH) vitamin D levels, the group with the lower vitamin D levels showed a significantly higher risk of T stage 3/4 (OR 1.49 [CI 1.02–2.16]; p=0.038), LNM (OR 1.66 [CI 1.15–2.40]; p=0.007), lateral LNM (OR 3.09 [CI 1.42–6.72]; p=0.004), stage III/IV (OR 1.45 [CI 1.00–2.10]; p=0.049), and ETE (OR 1.45 [CI 1.00–2.10]; p=0.049; Table 5). Lower serum 25(OH) vitamin D levels were associated with greater LNM (OR 1.69 [CI 1.16–2.45]; p=0.006), lateral LNM (OR 3.14 [CI 1.44–6.86]; p=0.004), and stage III/IV (OR 1.60 [CI 1.03–2.48]; p=0.036) independent of age, BMI, seasonal differences, and TSH.
Adjusted by age, BMI, seasonal differences, and TSH.
Discussion
In the current study, female PTC patients with low 25(OH) vitamin D levels seemed to have poor clinicopathologic features. Patients in the second quartile had a significantly increased incidence of T stage 3/4, LNM, lateral LNM, and ETE than those in the fourth quartile. The relationship was sustained following adjustment for age, BMI, seasonal differences, and TSH. Similar results were observed for patients with vitamin D values lower than the median. The incidence of LNM, lateral LNM, and stage III/IV was increased in these patients following adjustment for the same above-mentioned factors. However, a linear relationship was not observed between 25(OH) vitamin D levels and poor clinicopathologic features.
Several studies have reported a significant association between low vitamin D status and markers of inflammation (23,24), and thyroid cancer often shows inflammatory cell infiltration (25,26). Further, some experimental evidence suggests that these inflammatory cells possess protumorigenic potential and that oncoproteins expressed in PTC trigger proinflammatory processes in thyroid cells (27 –29). Thus, inflammatory processes could provide an underlying explanation for the potential link between low vitamin D status and advanced PTC.
Increasing tumor size has been shown to be a poor prognostic factor for papillary and follicular thyroid cancer (30). Here, we observed an inverse correlation between tumor size and vitamin D, suggesting decreased vitamin D might be an independent risk factor for PTC. LNM has also been found to be a poor prognostic factor of PTC (30,31). Similarly, we found that a significant association was present between vitamin D and LNM, and that low vitamin D was related to an advanced AJCC TNM Stage. However, no significant correlations were observed between stage III/IV and low 25(OH) vitamin D levels. For patients ≥45 years of age, serum 25(OH) vitamin D levels were significantly lower in those with stage III/IV than with stage I/II (22.8 vs. 20.0 ng/mL; p=0.017). When a multivariate analysis was conducted for patients ≥45 years of age, the second quartile showed a significantly higher risk of stage III/IV than the fourth quartile (OR 2.29 [CI 1.21–4.22]; p=0.011). Hence, the present results are consistent with a role for vitamin D insufficiency in thyroid cancer.
In the previous pilot study of Jonklaas et al. (18), no relationships were observed between serum 25(OH) vitamin D and poor clinicopathologic features. However, the number of enrolled patients was too small to reach strong conclusions. Here, we investigated a large number of patients to compare the clinicopathologic factors of thyroid cancer, and found lower 25(OH) vitamin D was significantly correlated with advanced PTC. However, no linear relationship was observed between the quartiles for 25(OH) vitamin D, and significant differences were only seen between the second and fourth quartiles. Several studies have reported a similar pattern in the correlations for other cancers. In particular, the ORs of 1,25 dihydroxyvitamin D showed an inverse J-shape pattern for the incidence of aggressive prostate cancer and for the survival of diffuse large B-cell lymphoma (11,32). The present study also observed an inverse J-shape pattern for the prevalence of T stage 3/4, LNM, lateral LNM, stage III/IV, ETE, and LVI in relation to vitamin D levels (Table 2). Further, LNM (p=0.041) and lateral LNM (p=0.004) both showed a significant trend for the ORs (Table 3). However, one study reported a linear trend in the ORs for the incidence of colorectal cancer (9). Thus, controversy remains with respect to the relationship between 25(OH) vitamin D and clinicopathologic features. Further studies are necessary to define the mechanisms underlying this association and to determine its potential prognostic and therapeutic implications.
Our study has several limitations. First, the study design was a retrospective cross-sectional one. Second, because only patients of Asian ethnicity were included, the findings may not be applicable to other ethnic groups, particularly those with different latitude or dietary habits. Third, some studies have reported a significant relationship between vitamin D and occupation or socioeconomic status. However, this type of data was not included in the analysis (33). Fourth, data were not obtained for 1,25 (OH)2 vitamin D, the active form of vitamin D. The 1,25 (OH)2 vitamin D levels can easily change according to the patient's condition and may therefore not show stable levels. However, several studies have found the active form shows a greater correlation with thyroid cancer than the inactive form (16,17). Fifth, only female patients were used in the investigation. Hence, the results might be applicable only to the female sex. Sixth, 25(OH) vitamin D was measured by immunoradiometric assay. If tandem mass spectrometry was used to measure 25(OH) vitamin D levels, more precise data could be obtained.
A strength of the study is that a greater number of patients and clinicopathologic features were investigated when compared to previous studies. In particular, although no significant correlation was observed between BRAF and vitamin D in relation to thyroid cancer, no previous study on vitamin D related thyroid cancer has addressed the possible correlation between these factors. An additional strength is the use of vitamin D supplementation and GFR levels as selection criteria. The exclusion of patients with vitamin D supplementation allowed us to analyze relatively stable vitamin D levels. We included patients with a GFR >60 mL/min, since some studies have reported that a GFR <60 mL/min influences vitamin D concentrations and metabolism (34,35). Hence, these selection criteria potentially enabled us to obtain more stable data independent of extrinsic factors when compared to previous studies.
In conclusion, lower preoperative serum 25(OH) vitamin D levels appeared to be associated with poor clinicopathologic features with respect to PTC in female patients. Vitamin D insufficiency may be a modifiable risk factor for PTC. We recommend further prospective investigations on vitamin D supplementation for patients with PTC and on prognostic outcomes divided according to preoperative vitamin D levels using larger cohorts.
Footnotes
Author Disclosure Statement
No competing financial interests exist.