
Abstract
Background:
The purpose of this study is to validate the generalizability of the efficacy and safety of radiofrequency (RF) ablation for treating autonomously functioning thyroid nodules (AFTN) in a large population multicenter study.
Methods:
This study included 44 patients from 5 institutions who refused or were not suitable for surgery or radioiodine therapy. Twenty-three patients were affected by a toxic nodule and 21 by a pretoxic nodule. RF ablation was performed using an 18-gauge, internally cooled electrode. Nodule volume, thyroid function, scintigraphy, symptom/cosmetic scores, and complications were evaluated before treatment and during each follow-up.
Results:
The mean follow-up period was 19.9±12.6 months. The mean nodule volume was initially 18.5±30.1 mL and significantly decreased after treatment at 1 month (11.8±26.9 mL, p<0.001) and the last month (4.5±9.8 mL, p<0.001). Significant improvement of triiodothyronine, free thyroxine, and thyrotropin was observed at the last follow-up. Regarding scintigraphy, 35 hot nodules became cold or were normal when scanned and 9 decreased uptake, although they remained hot nodules. The mean symptom and cosmetic scores were significantly reduced at the last follow-up. No major complications were encountered.
Conclusions:
This multicenter study validated the efficacy and safety of RF ablation for treating AFTN; RF ablation can be considered an alternative to surgery or radioiodine therapy.
Introduction
F
Radiofrequency (RF) ablation is another method of inducing tissue necrosis using thermal energy and it has been widely used to treat hepatomas as well as other benign and malignant tumors. In the thyroid gland, RF ablation has been used for recurrent cancer (13) and benign nodules (14). Several recent studies have reported the efficacy and safety of RF ablation for treating AFTN (15 –18), however, these small population, single-center studies (9–23 cases) have limitations regarding generalizability of RF ablation in patients with AFTN. Since 2005, The Korean Society of Thyroid Radiology (KSThR) has trained experts in thyroid RF ablation through annual hands-on workshops in order to unify the techniques of RF ablation (19,20).
The purpose of this study was to validate the generalizability of the efficacy and safety of RF ablation for treating AFTN in a large population, multicenter study.
Materials and Methods
The Institutional Review Boards of five participating centers approved this retrospective study and required neither patient approval nor informed consent for the review of images and medical records. However, informed consent for RF ablation was obtained from all patients prior to the RF ablation.
Patients
In November 2011, the research committee of the KSThR organized a retrospective, multicenter study on RF ablation for AFTN through e-mails sent to all KSThR members. Five institutions were included in this multicenter study. From August 2007 to July 2011, 44 nodules in 44 patients (M:F ratio=2:42, mean age, 43±14.7 [range, 17–70] years) were treated by RF ablation (Fig. 1). Twenty-three (52.3%) patients had toxic nodules and 21 (47.7%) had pretoxic nodules. They were referred by their primary physicians to our interventional radiology departments for RF ablation. Appropriate candidates were treated by radioiodine therapy or surgery according to the decision of their primary physicians, rather than being included in this study. The inclusion criteria were as follows: (1) hot nodule with/without suppression of the normal gland seen in a thyroid scan; (2) low serum TSH level and/or increased serum total triiodothyronine/free thryoxine (T3/fT4) levels; (3) patients refused or were not appropriate for radioiodine therapy or surgery; and (4) follow-up periods of more than 6 months. The exclusion criteria were thyroid nodule with malignant ultrasound (US) findings suggested by the KSThR (21,22) and patients who refused RF ablation.
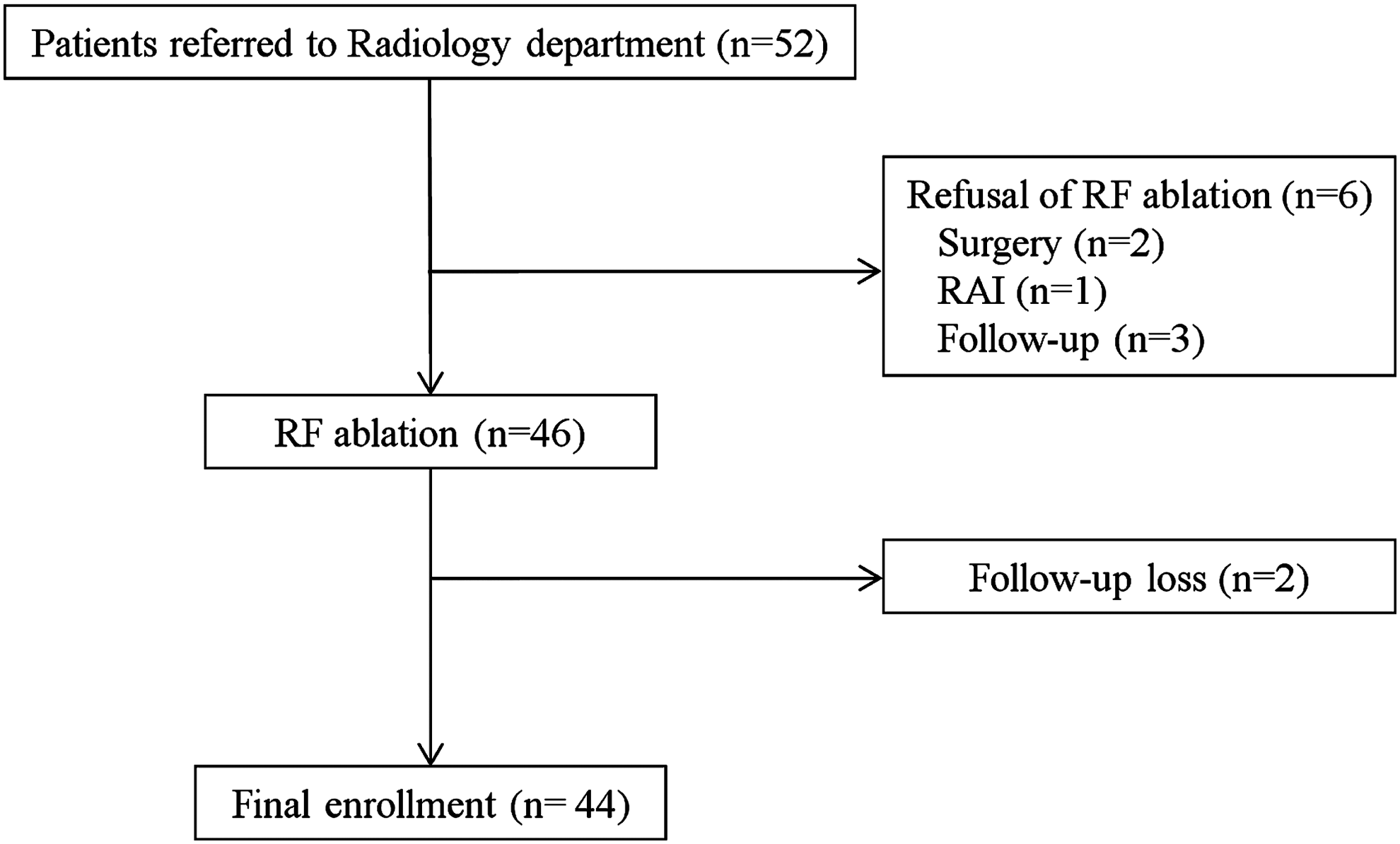
Flowchart of enrollment and follow-up of the study patients.
Preablation assessment
US, laboratory, 99mTc pertechnetate scintigraphy, and clinical results were evaluated before RF ablation. Six radiologists, all of whom specialized in thyroid US with experience of 12–18 years, performed the US examinations and US-guided RF ablation using 5–14 MHz linear probes on real-time US systems (Aplio SSA-770A, Toshiba, Otawara-shi, Japan; iU22 unit, Philips Healthcare, Bothell, WA; Hitachi Logos E, EUB-7500, Hitachi Medical System, Tokyo, Japan). Three orthogonal diameters of the nodules were measured before initiating RF ablation. When measuring the nodule size, we located the calipers at the outer margin of the halo of the nodule. On the axial image, the width and height were measured. The length was measured as the largest diameter on sagittal image. The volume of each nodule was calculated using the following equation: V=πabc/6 (V: volume, a: the largest diameter, b and c: other two perpendicular diameters) (23). The composition of the solid portion was classified using three categories: solid (solid>90%); predominantly solid (50% <solid<90%); and predominantly cystic (solid<10%) (21). The vascularity grade of each nodule was classified using a five-point scale: 0 (no signal in the tumor); 1 (a few spotty signals in the tumor); 2 (signals in<25% of the tumor); 3 (signals in 25–50% of the tumor); and 4 (signals in>50% of the tumor). Laboratory studies included determination of the serum levels of TSH, total T3, fT4, anti-thyroid peroxidase antibody (anti-TPOAb), and anti-thyroglobulin antibody (anti-TGAb). 99mTc pertechnetate scintigraphy was performed in all patients prior to ablation. Clinical symptoms and signs were evaluated using the symptom score (visual analog scale, 0–10 cm) and the cosmetic score: 1, no palpable mass; 2, no cosmetic problem but a palpable mass; 3, indicating a cosmetic problem on swallowing only; and 4, indicating a readily detected cosmetic problem (20,24).
Procedure
All procedures were performed by the same six radiologists who were trained in thyroid RF ablation training programs organized by the KSThR (20). The treatment protocol has been described previously. RF ablation was performed using US guidance and on an outpatient basis using a generator (VIVA RF generator, STARmed, Gyeonggi, Korea; M-2004, RF Medical, Seoul, Korea; Cool-tip RF system, Radionics, Burlington, MA) and internally cooled electrodes of 7 cm length, 18 gauge, 0.5-, 1-, and 1.5-cm active-tips (Well-Point RF Electrodes, Taewoong Medical, Kyeonggi, Korea; VIVA, STARmed, Gyeonggi, Korea; RFT-0710, RF Medical, Seoul, Korea). A modified, straight, internally cooled electrode is short (7 cm) to permit easy control, thin (18 gauge) to minimize injury to the normal thyroid gland, and can be used with active tips of various sizes (0.5, 1, and 1.5 cm) (15,20,25,26).
The patients were placed in the supine position with the neck extended, and two grounding pads were firmly attached to both thighs. All procedures were performed using the US-guided, free-hand technique. After treatment with 2% lidocaine for local anesthesia of the puncture site and around the thyroid gland, the skin was not incised so as to prevent unnecessary scar formation. An electrode was inserted into the thyroid nodule along the short axis of the nodule using the trans-isthmic approach method (15,20,24,26 –30). Baek et al. (23) have proposed a moving shot technique for benign thyroid nodules and recurrent thyroid cancers rather than the fixed electrode technique that has been used to treat liver tumors. In the latter technique, the electrode is fixed in position during ablation, thus resulting in a round ablation zone. Because thyroid nodules are usually ellipsoid rather than round in shape, prolonged fixation of the electrode is dangerous to surrounding critical structures. The thyroid nodule can be divided into multiple, small, conceptual ablation units, and the procedure can be performed unit by unit, by continuously moving the electrode tip. The conceptual ablation units are smaller at the periphery of the nodule and larger in the safe center of the nodule. Initially, the electrode tip was positioned in the deepest and most remote portion of the nodule to enable the tip to be easily monitored in the absence of any disturbance caused by microbubbles. The RF power started with 15–20 W in a 0.5-cm active tip, 30–50 W in a 1-cm active tip, and 50–70 W in a 1.5-cm active tip, according to the status of the nodule composition. If the formation of a transient hyperechoic zone at the electrode tip did not appear within 5–10 seconds, the RF power was increased in 5- to 10-W increments, reaching full capacity at 40 W with a 0.5-cm active tip, 100 W with a 1-cm active tip, and 120 W with a 1.5 cm-active tip. In cases of thyroid nodules containing a cystic portion, we performed RF ablation after aspiration of the internal fluid (20,24,26 –30). If a patient complained of pain during the procedure, we reduced the RF power or stopped the ablation for several seconds. Ablation was terminated when all conceptual ablation units of the nodule had changed to transient hyperechoic zones. Any complications during and immediately after the procedure were checked in order to assess its safety. After RF ablation, the patient was observed for 1–2 hours in the hospital (20,23,31).
Follow-up
Follow-up US examinations, laboratory tests, 99mTc pertechnetate scintigraphy, and checking the symptom/cosmetic score were performed at 1- and 6-month follow-up and thereafter every 6–12 months. On US examination, changes in the largest diameter, the nodular volume, and the vascularity were evaluated. The volume reduction was assessed by US and was calculated using the following equation: volume reduction (%)=([initial volume (mL)−final volume (mL)]×100)/initial volume. The serum levels of T3, fT4, TSH, anti-TPOAb, and anti-TGAb were checked during the follow-up periods. Changes in thyroid scans were also determined. In follow-up thyroid scans, thyroid nodules were classified into three categories: type 1, hot nodule; type 2, nodule uptake similar to extranodular thyroid tissue; and type 3, cold nodule or invisible status. Symptoms and cosmetic scores were evaluated at each follow-up examination. Repeat RF ablation was performed during the follow-up periods when the serum TSH level was not normalized after the first RF ablation (15).
Statistical analysis
Statistical analyses were performed using SPSS for Windows (version 17.0; SPSS, Chicago, IL). At each treatment interval, the nodule volume change and the percent volume reduction, changes in the vascularity grade, changes of T3, fT4, and TSH, changes in thyroid scans, and changes in symptom/cosmetic scores were compared using the Wilcoxon signed rank test. The level of significance was defined as p<0.05.
Results
US characteristics
The mean follow-up period was 19.9±12.6 months (range, 6–56 months). The mean largest diameter of the index nodule was 3.8±1.4 cm (range, 1.3–9.0 cm). The mean volume of the index nodule was 18.5±30.1 mL (range, 0.5–174.3 mL). A significant decrease in the mean nodule volume was observed at 1 month (11.8±26.9 mL, p<0.001), 3 months (12.2±28.2 mL, p<0.001), 6 months (7.0±14.7 mL, p<0.001), and at the last month (4.5±9.8 mL, p<.001) (Table 1) (Fig. 2). The mean volume reduction was 45.9±22.1% at the 1-month follow-up, 64.1±18.4% at the 3-month follow-up, 74.5±15.7% at the 6-month follow-up, and 81.7±13.6% at the last follow-up. The compositions of the index nodules was solid (n=26), predominantly solid (n=16), and predominantly cystic (n=2). There was no patient with a cystic thyroid nodule. After ablation, color and power Doppler US showed significant reduction of the peripheral and/or intranodular vascular signals (vascular grade, initial versus last follow-up, 3.1±0.7 versus 0.9±1.0, p<0.001) (Table 1).

Changes in nodule volume, symptoms, and the cosmetic score prior to radiofrequency (RF) ablation and at the last follow-up. †Symptom score: visual analog scale, 0–10 cm. ††Cosmetic score: 1 (no palpable mass), 2 (no cosmetic problem but a palpable mass), 3 (indicating a cosmetic problem on swallowing only), 4 (indicating a readily detected cosmetic problem).
Vascular grade: 0 (no signal in the tumor), 1 (a few spotty signals in the tumor), 2 (signals in <25% of the tumor), 3 (signals in 25–50% of the tumor), 4 (signals in >50% of the tumor).
Symptom score: visual analog scale, 0–10.
Cosmetic score: 1 (no palpable mass), 2 (no cosmetic problem but a palpable mass), 3 (indicating a cosmetic problem on swallowing only), 4 (indicating a readily detected cosmetic problem).
RFA, radiofrequency ablation; T3, triiodothyronine, fT4, free thyroxine; TSH, thyrotropin.
Laboratory data, scintigraphy, and clinical findings
The initial mean T3, fT4, and TSH were 179.3±102.5 ng/dL, 1.9±1.3 ng/dL, and 0.12±0.12 μIU/mL, respectively. A significant improvement in the mean T3, fT4, and TSH was observed at the last follow-up (T3; 133.3±63.1 ng/dL, p<0.001, fT4; 1.3±0.4 ng/dL, p<0.001, TSH; and 1.22±0.93 μIU/mL, p<0.001) (Table 1). The serum TSH levels normalized in 36 of 44 patients and were improved but still decreased in 8 patients. Before ablation, anti-TPOAb and anti-TGAb were assessed in 35 patients. Elevation of anti-TPOAb and/or anti-TGAb was detected in 7 patients. In addition, 1 patient developed elevation of anti-TGAb during the follow-up period, however, no patient developed hypothyroidism.
After ablation, 35 nodules showed a cold or normal scan and nine remained as hot nodules. Thirty-one of 35 patients with cold or normal scans had normal serum hormone levels. In 4 of these 35 patients, the serum TSH level was slightly improved, although it was still decreased. Nine patients had sustained hot nodules showing various serum levels of TSH (6, normal; 1, low; 2, undetectable serum level of TSH).
The mean symptom and cosmetic scores were significantly reduced from 3.3±2.1 to 0.9±1.0 (p<0.001) and from 3.8±0.5 to 1.9±0.9 (p<0.001), respectively (Table 1) (Fig. 2). No patient complained of aggravation of symptoms or cosmetic problems after RF ablation. Before ablation, an anti-thyroid drug was prescribed for 5 patients. Three of these 5 patients were able to stop the anti-thyroid drug following ablation. However, 2 of the 5 patients were not able to stop their medication, although the amount of medication could be decreased after ablation.
Treatment characteristics
The mean number of treatment sessions was 1.8±0.9 (range, 1–6 sessions). The mean ablation time and power were 12±5.9 minutes (range, 2.5–30 minutes) and 63.3±26.3 W (range, 20–120 W), respectively. The total energy deposition ranged from 4,500 to 539,460 J (mean±standard deviation [SD], 76,939.6±87,264.2, median, 48,600.0). The mean energy deposited at the first treatment (n=44) was 49,547.5±41,678.1 J, during the second treatment (n=27) it was 33,283.6±43,102.0 J, and during the third treatment (n=7) it was 38,142.9±29,919.4 J. Fourth, fifth, and sixth ablations were performed in only one patient and the energies deposited were 39,600 J, 52,800 J and 42,000 J at each session. The mean total energy delivered per milliliter of the pretreatment nodule volume was 6417.3±4318.4 J/mL (range, 1589–19014 J/mL).
Complications
During the RF ablation, all patients complained of various degrees of pain and/or of a sensation of heat in their neck, sometimes radiating to their head, shoulders, teeth, back, and chest (20). However, no one complained of symptoms that made it necessary to stop the procedure before completion. There were no major complications, such as voice changes, skin burning, or damage to the vital structures of the neck during the procedure or during the follow-up period.
Discussion
This multicenter study demonstrates that hyperthyroidism caused by AFTN improved in all patients and completely normalized in 81.8% (36/44) of our study patients without development of hypothyroidism. RF ablation also significantly improved symptomatic and cosmetic problems by reducing nodule volume (mean volume reduction ratio, 81.7% during the mean follow-up period of 19.9 months). In our study, we did not notice any major complications or hypothyroidism during the follow-up period. These results demonstrate that this relatively large population, multicenter study performed by well-trained radiologists, validates the efficacy and safety of RF ablation for treating AFTN.
RF ablation was recently introduced as an alternative for treating AFTN (15). A recent systematic review also suggested the efficacy of RF ablation for AFTN in terms of withdrawal from anti-hyperthyroid medication after RF ablation (32). There are two types of RF ablation studies using different techniques and devices. The first study used a fixed-needle technique and a multi-tined expandable electrode (16,17). The mean volume reduction ratios that were achieved were 52.1% and 79.4% at the 6- to 24-month follow-up. Another study by Baek et al. (15) used the moving shot technique and a straight type of internally cooled electrode. This study achieved a 79.7% mean volume reduction ratio at the mean follow-up period of 11 months. Baek et al. (15) showed somewhat superior results compared with studies performed using the fixed-needle technique and a multi-tined expandable electrode. Our multicenter study was performed by six radiologists at five medical institutions and it also used the moving shot technique with an internally cooled electrode according to the guidelines recommended by the KSThR (20). The final volume reduction was 81.7%, which is similar to that (79.7%) seen in the study by Baek et al. (15). Our study validates the concept that RF ablation performed by well-trained radiologists could provide reproducible results and a low complication rate.
LA and EA have also been introduced as minimally invasive treatments for AFTN (6,12,33,34). Our study results revealed similar or slightly superior results compared with those of LA (81.7% versus 44–81.9%) (5 –7,9,10,12), however, the mean number of treatment sessions appears to be similar (1–2.2 in RF ablation versus 1–2.7 in LA). EA has shown good results in normalization of the thyroid function (35.3–91.1%) for AFTN, however, the mean number of treatment sessions is much higher (4,8,11,33 –35) than that needed for RF ablation (3.9–8.1 versus 1–2.2) (15 –17). The higher number of treatment sessions with EA was due to the uneven distribution of injected ethanol inside solid thyroid nodules (36). In addition, the mean volume reductions of EA (4,8,11,33 –35) seem to be inferior to those of RF ablation (43.1–66% versus 52.1–81.7%) (15 –17).
The wide range of volume reduction may be caused by the amount of untreated tissue at the thyroid nodule margin, which can be a cause of insufficient volume reduction and regrowing of the nodule margin during the follow-up period (15,31,37). Therefore, the strategy of minimally invasive treatment, regardless of the treatment tools, should attempt complete ablation of the entire nodule. The moving shot technique is a safer method for ablating the nodule margin, and the internally cooled electrode is more suitable for use in the moving shot technique, however, a multi-tined, expandable electrode is not easy to move and simultaneous US observation of the multiple, expandable prongs is difficult during the ablation (24,26,31). The moving shot technique was also suggested as an effective technique in the treatment of recurrent thyroid cancers (13,36,38).
It is difficult to exactly compare the costs of RF ablation and other treatment modalities. The cost of RF ablation is similar to that of surgery, although it is more expensive than radioiodine therapy. RF ablation requires RF equipment and is associated with a distinct learning curve.
Regarding the complications, EA has been associated with various complications such as transient voice problems (4,8,11,33 –35), hypothyroidism (34,35), hematoma (4,8,33), abscess (4), and pain (14,20). These complications may relate to leakage of injected ethanol outside the thyroid gland. Multiple treatment sessions could also increase the incidence of complications in EA. In RF ablation studies, there were no complications other than pain (15 –17). We did not observe hypothyroidism during the follow-up period. This result suggested that RF ablation could preserve normal thyroid function after treatment of AFTN, unlike that seen with surgery or radioiodine therapy. RF ablation also preserves the thyroid function after treatment for patients with benign, cold thyroid nodules (14,20) and for patients who have undergone previous lobectomy (39). Thermal injury to the trachea, esophagus, and recurrent laryngeal nerve adjacent to AFTN can be avoided by using the moving shot technique and by undertreating adjacent parts to these vital structures. The carotid artery may not be damaged by thermal injury, under the influence of heat sink effect. The heat sink effect, or perfusion-mediated tissue cooling, refers to the fact that a large vessel close to the tumor can act as a heat sink due to blood flow moving away from the area of ablation resulting in an ineffective ablation zone. The amount of the undertreated portion is dependent on the performer's proficiency, and a considerable undertreated remnant can be a source of recurrence. Although the clinical outcomes of RF ablation seem to be superior to those of other treatment modalities, a direct comparison is not possible because each study enrolled patients with different nodule features (i.e., nodule volume and the proportion of the solid composition) and used various ablation techniques (37).
Our study has several limitations. The first is its retrospective design, however, this study is the largest population multicenter study that corroborates findings of previous RF studies. Second, our study did not compare RF ablation with surgery or RI therapy. Third, the follow-up period was relatively short.
In conclusion, this relatively large patient population, multicenter study conducted by trained radiologists verified the safety and efficacy of RF ablation for treating AFTN. RF ablation can thus be considered a possible alternative to surgery or radioiodine therapy without development of hypothyroidism.
Footnotes
Author Disclosure Statement
No competing financial interests exist.