
Abstract
Background:
A variety of measures have been proposed to reduce the incidence of post-thyroidectomy hypocalcemia. The aim of this study was to perform a systematic review and meta-analysis of preventive and other surgical measures on post-thyroidectomy hypocalcemia as reported in the literature.
Methods:
Comprehensive searches of the PubMed, EMBASE, and Cochrane databases were performed, and the quality of included papers was assessed using the Cochrane risk of bias tool or a modified Newcastle–Ottawa Scale (NOS). The results of all included studies were summarized, and meta-analyses were performed where appropriate.
Results:
Thirty-nine randomized controlled trials (RCTs) and 37 observational studies were included. Measures studied included hemostatic techniques, extent of thyroidectomy and central neck dissection, surgical approach, calcium/vitamin D/thiazide diuretic supplements, parathyroid gland autotransplantation (PGAT) and intraoperative parathyroid gland (PG) identification, truncal ligation of inferior thyroid artery (ITA), preoperative magnesium infusion, and use of magnification loupes and Surgicel. Measures associated with significantly lower rates of transient hypocalcemia in meta-analysis were postoperative calcium and vitamin D supplementation compared to either calcium supplements alone (odds ratio (OR) 0.66; p=0.04) or no supplements (OR 0.34; p=0.007), and bilateral subtotal thyroidectomy (BST) compared to Hartley Dunhill (HD) procedure (OR 0.35; p=0.01). Meta-analyses did not demonstrate any measure to be significantly associated with a reduction in permanent hypocalcemia.
Conclusion:
This review identified postoperative calcium and vitamin D supplementation and bilateral subtotal thyroidectomy (over HD) as being effective in prevention of transient hypocalcemia. However, the majority of RCTs were of low quality, primarily due to a lack of blinding. The wide variability in study design, definitions of hypocalcemia, and methods of assessment prevented meaningful summation of results for permanent hypocalcemia.
Introduction
H
Features of hypocalcemia include circumoral and peripheral paraesthesia, tetany, carpopedal spasm, laryngospasm, and echocardiogram (ECG) changes (6). Cardiac arrhythmias and arrest can also occur in severe cases (6). Long-term hypocalcemia/hypoparathyroidism has a significant impact on quality of life, and results in patients being at a higher risk of chronic renal impairment and basal ganglia calcification (7).
Various measures have been proposed to reduce the risk of postoperative hypocalcemia. These include use of magnification loupes, modifying the extent of thyroid surgery and lymph node dissection, and the use of various hemostatic techniques. Several studies have suggested that less extensive surgery (i.e., subtotal thyroidectomy (ST) and near-total thyroidectomy (NTT) vs. total thyroidectomy (TT)) can decrease overall complication rates (8 –18). Despite this, there has been increased acceptance of TT as the operation of choice for both benign and malignant thyroid diseases due to lower risks of disease recurrence (8). Other studies have looked at dissection/hemostatic techniques (e.g., harmonic scalpel and LigaSure) and their effect on operative outcomes (19 –25). However, the small numbers of patients studied and conflicting results limit the interpretation with regards to their effect on hypocalcemia. Ecker et al. carried out a meta-analysis comparing the harmonic scalpel versus other hemostatic techniques in thyroid surgery (26) and included RCTs only (total of 12). The quality of included RCTs was discussed, but no formal assessment tool was used. The review reported on operating time, intraoperative blood loss, volume of drainage fluid, and complication rates. Complications were reported collectively, and included recurrent laryngeal nerve (RLN) palsy, hypoparathyroidism, seroma formation, and hematoma. The rate of complications in the “harmonic scalpel” arm was reported to be similar to other hemostatic techniques.
The objective of this study was to assess systematically available literature that reports measures aimed to reduce transient and permanent hypocalcemia rates following bilateral thyroid surgery. Due to the scarcity of high-quality RCTs in this area, it was decided to include both RCTs and cohort studies in this review.
Methodology
Search strategy and study inclusion
A comprehensive search of the PubMed, Embase, and Cochrane library databases was undertaken from January 1, 1990, to December 31, 2013, to identify studies reporting on measures to reduce hypocalcemia following bilateral thyroid surgery. The following terms were used as free text in the search: “low calcium” OR “hypocalc*” AND “thyroi*.” All published original articles of observational or interventional design that reported on prevention of hypocalcemia following bilateral thyroid surgery in humans were included. Reviews, letters/commentaries/editorials, articles with fewer than 25 patients, irretrievable full-text articles, articles not available in English language, animal studies, single-arm studies, noncomparable groups, historical controls, wrong population (i.e., unilateral thyroidectomy), and articles published before 1990 were excluded.
Population, interventions, and outcomes
Patients undergoing bilateral thyroidectomy (with or without lymph node dissection) for benign or malignant disease where both lobes were partly or completely removed were the focus of study. All measures introduced to prevent hypocalcemia were considered for inclusion. Similarly, any study that reported on postoperative hypocalcemia was included, regardless of the definitions used for transient or permanent hypocalcemia.
Data extraction
Two investigators (R.A. and O.E.) screened the abstracts identified from the search. Any discrepancy was resolved by a third investigator (S.P.B.). Full text of initially included articles was further assessed by R.A. E-mails were sent to authors when full-text articles were not available. Excluded studies were confirmed by L.U., and any queries regarding eligibility were resolved by further discussion with other co-authors. In cases of duplicate publications, only the publication with the most recent and complete data was included. All extracted data were counterchecked by the second investigator (O.E.) prior to analysis. The nine-point Newcastle–Ottawa Scale (NOS) (27) was modified (Supplementary Fig. S1; Supplementary Data are available online at
Analysis
The quality scores of included studies and incidence of hypocalcemia were reported as median and interquartile range (IQR). Observational studies were not included in the meta-analysis but were described as part of the systematic review. The difference in quality between prospective and retrospective observational studies was assessed with the Mann–Whitney U-test.
A meta-analysis was performed when there were two or more RCTs with comparable populations that evaluated the same measure. The meta-analysis was performed using the random effects model due to the variability in the populations, nature of preventative measures, and definitions of outcomes across the included studies. The meta-analysis is presented as odds ratio (OR) with confidence intervals (CI). The p-value for chi-square test for heterogeneity, I2 statistic for the degree of heterogeneity across studies, and Forest plots illustrating the results of meta-analyses were obtained using Revman5 software. A rough guide to interpreting the I2 statistic for the degree of heterogeneity is as follows (29): 0–40% may not be important; 30–60% may represent moderate heterogeneity; 50–90% may represent substantial heterogeneity; and 75–100% represent considerable heterogeneity.
The protocol of this systematic review was registered with PROSPERO database (registration number CRD42012003447), and the review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (30).
Review
Figure 1 illustrates the PRISMA flow diagram of the selection process.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the study selection process.
The study included 39 RCTs and 37 interventional cohort studies (Supplementary Table S1). The 39 RCTs had a median (IQR) score of 3 (2–3). Of the 37 cohort studies, 25 were retrospective and 12 were prospective. The 25 retrospective cohort studies had a median (IQR) quality score of 7 (6 –8), and the 12 prospective cohort studies had a median (IQR) quality score of 5 (5 –7). Quality scores were not significantly different between retrospective and prospective cohorts (p=0.124). Preventative and surgical measures included the extent of thyroid surgery and neck dissection, hemostatic technique, surgical approach, perioperative administration of calcium, vitamin D, thiazide and/or magnesium supplements, use of magnification loupes, inferior thyroid artery (ITA) truncal ligation, parathyroid gland autotransplantation (PGAT), and intraoperative PG identification.
Various parameters have been used to define transient and long-term/permanent hypocalcemia in the included studies (Supplementary Tables S2 and S3). The level of calcium used to define transient hypocalcemia in 48 studies is listed in Supplementary Table S4, and the duration used to define permanent hypocalcemia in 44 studies is listed in Supplementary Table S5. Transient and long-term hypocalcemia were not defined in 16 and 31 studies respectively.
The most common biochemical cutoff value used to define transient hypocalcemia was a total serum calcium <2.0 mmol/L in 31 studies (Supplementary Table S4). Three studies used a combination of biochemical markers to define transient hypocalcemia: total serum calcium <2.0 mmol/L and/or ionized calcium <1.0 mmol/L (31,32), total serum calcium <2.0 mmol/L and/or parathyroid hormone (PTH) <15 pg/mL (33). Besic et al. defined transient hypocalcemia as serum calcium <2.1 mmol/L, which resolved within six months (34). The most common duration used to define permanent hypocalcemia was six months or more in 32 studies (Supplementary Table S5).
Hemostatic techniques
A summary of hemostatic techniques is shown in Supplementary Table S6. Four methods were studied, including the harmonic scalpel, LigaSure, a novel BiClamp device, and a new vessel sealer device—the Starion TLS2 vessel sealing system.
Twenty-two studies compared the harmonic system versus conventional hemostasis, three of which had three arms assessing harmonic and LigaSure versus conventional techniques (22,24,35). A meta-analysis of 17 RCTs (20,21,24,25,33,35 –46) showed no significant effect on transient hypocalcemia associated with the use of the harmonic scalpel (Fig. 2A; OR 0.74 [CI 0.47–1.16]; p=0.19), and no significant effect on permanent hypocalcemia (Fig. 2B; OR 0.35 [CI 0.08–1.59]; p=0.17). A recent multicenter observational study by Materazzi et al. comparing harmonic focus to clamp-and-tie hemostasis showed a significantly reduced risk of transient hypocalcemia with the harmonic device (47).
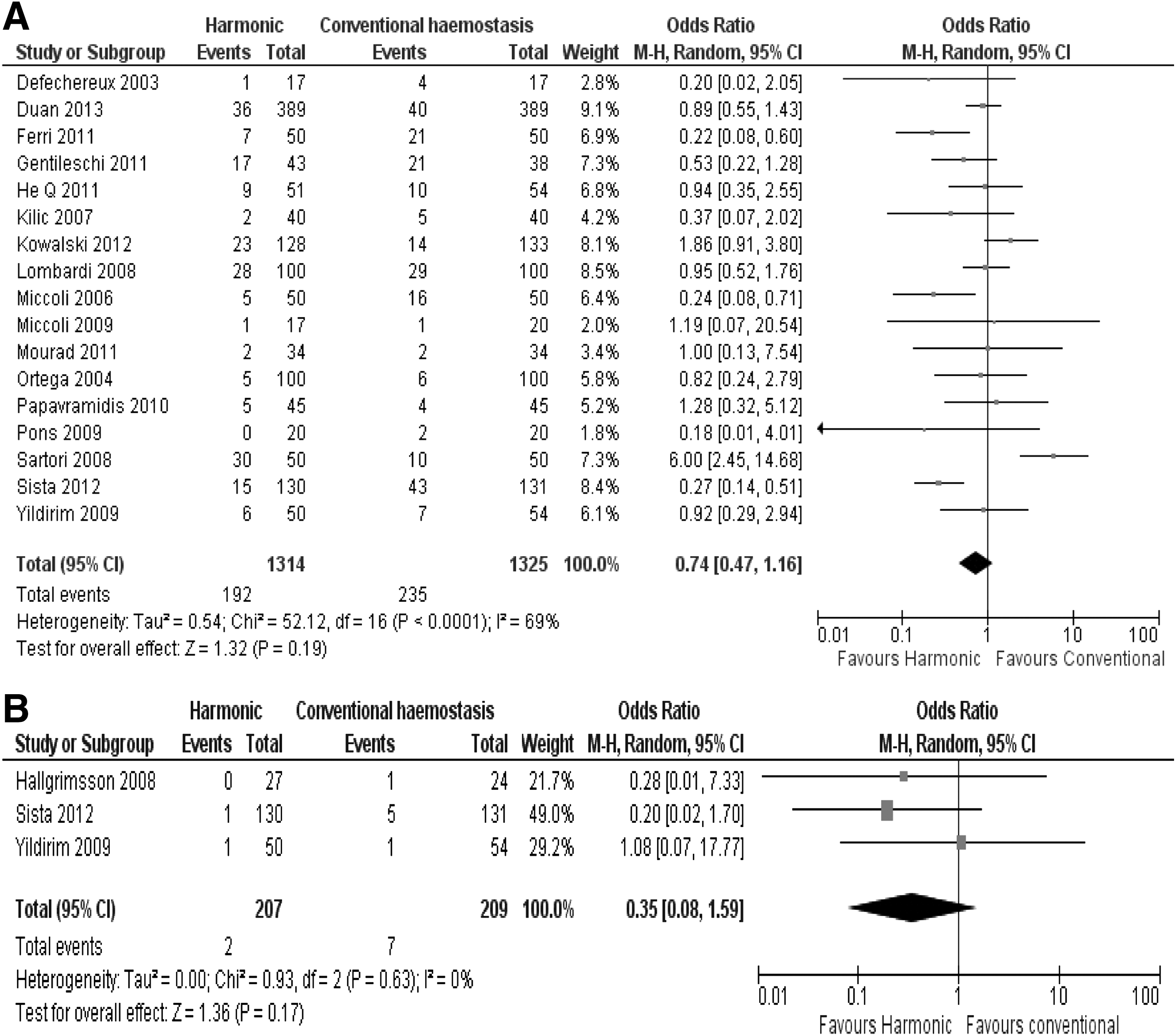
Meta-analysis comparing harmonic versus conventional hemostasis (knot tying, clips, and diathermy) on (
Five studies compared LigaSure with conventional techniques (22,24,35,48,49). None of the studies demonstrated any advantage of LigaSure over conventional hemostasis (Supplementary Table S6). A meta-analysis of two RCTs (24,35) showed no significant effect on transient hypocalcemia with LigaSure compared to conventional hemostasis (Fig. 3; OR 0.57 [CI 0.10–3.13]; p=0.51). Neither trial reported on permanent hypocalcemia.
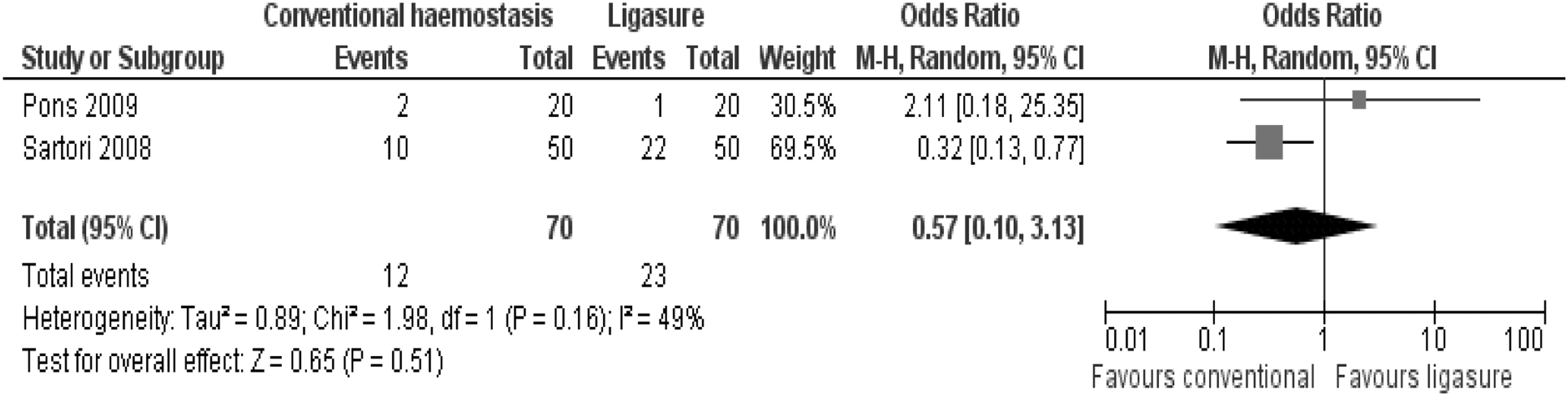
Meta-analysis comparing LigaSure versus conventional hemostasis (knot tying, clips, and diathermy) on transient hypocalcemia.
Scerrino et al. carried out a RCT comparing a new vessel sealer device—the Starion TLS2—to the clamp-and-tie technique. This demonstrated no effect on either transient or permanent hypocalcemia (50). Another prospective study compared a new BiClamp device with LigaSure, showing lower risk of transient hypocalcemia in the former; permanent hypocalcemia was not assessed (51). Zarebczan et al. retrospectively compared the harmonic scalpel to LigaSure and found no significant differences between both devices on transient and permanent hypocalcemia rates (23).
Extent of thyroid surgery
The extent of thyroid surgery is summarized in Supplementary Table S7. Sixteen studies (8 –18,52 –56) assessed the extent of thyroid surgery and its impact on postoperative morbidity including hypocalcemia. Five studies compared NTT versus TT (control arm) in patients with multinodular goiter. Meta-analysis of two RCTs (14,17) demonstrated no significant effect on transient hypocalcemia associated with NTT compared to TT (Fig. 4; OR 0.09 [CI 0.00–1.69]; p=0.11). However, no patient developed permanent hypocalcemia in either RCT.
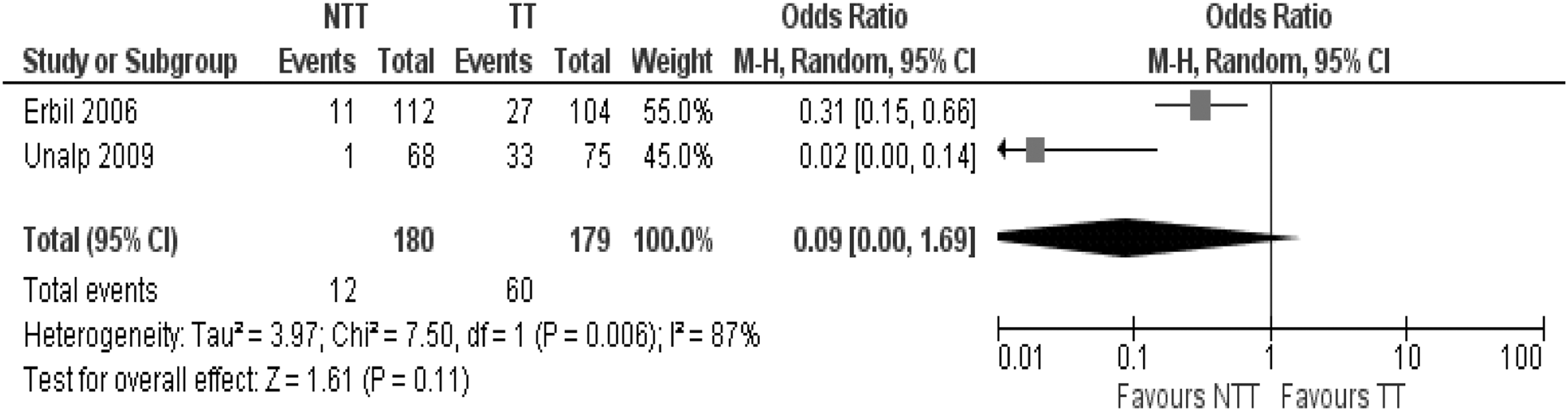
Meta-analysis comparing near-total thyroidectomy versus total thyroidectomy on transient hypocalcemia.
For the purpose of this review, all procedures described as “subtotal” resections were considered as a single group regardless of the extent of resection. Three RCTs compared bilateral subtotal thyroidectomy (BST) to the Hartley Dunhill (HD) procedure (control) in treating patients with benign thyroid disease (52 –54). Meta-analysis demonstrated significantly lower rates of transient hypocalcemia associated with BST (Fig. 5A; OR 0.35 [CI 0.15–0.79]; p=0.01) but no effect on permanent hypocalcemia (Fig. 5B; OR 0.47 [CI 0.07–3.29]; p=0.45).
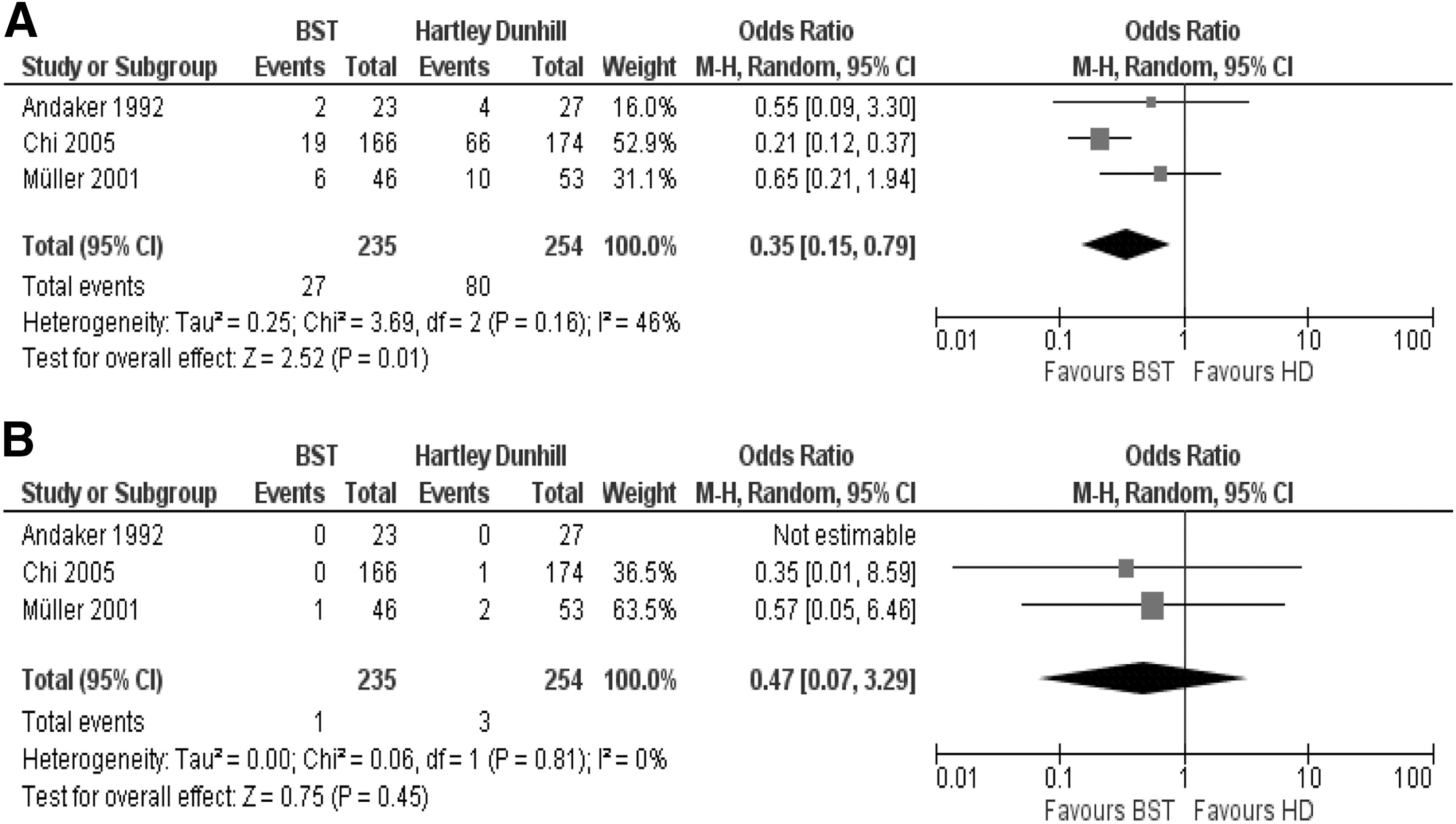
Meta-analysis comparing bilateral subtotal thyroidectomy (BST) procedure versus HD on (
Four retrospective studies (10,11,18,55) examined the role of TT versus subtotal thyroidectomy (control group) in treating benign thyroid disease. One study found that TT significantly increased the risk of transient hypocalcemia (OR 5.4 [CI 3.1–9.2]) (55), but recurrence rates were not reported. However, there was no increased risk of transient or permanent hypocalcemia in the remaining studies in patients undergoing TT (10,11,18).
Seven studies compared ST versus TT (control group) in management of benign disease (8,9,12,13,15,16,56). Two studies reported significantly lower rates of transient hypocalcemia with ST (9,16), with no effect on permanent hypocalcemia.
Extent of lymph node dissection
The extent of lymph node dissection is summarized in Supplementary Table S8. The need for a prophylactic central compartment lymph node dissection (pCND) remains a controversial issue in the management of patients with thyroid cancer without clinical or radiological evidence of cervical lymphadenopathy. A primary concern of doing a pCND is the incidence of hypoparathyroidism. Six retrospective studies assessed the role of TT with pCND versus TT alone (57 –62). Three reported significantly higher rates of transient hypocalcemia (57,59,61), and one reported significantly increased risk of permanent hypocalcemia in patients undergoing pCND (57). The three other studies showed no significant effect on either transient or permanent hypocalcemia (58,60,62).
Son et al. and Lee et al. compared TT with ipsilateral pCND versus TT with routine bilateral pCND (control group) in the management of papillary thyroid cancer (PTC) (63,64). Both were retrospective studies and found that ipsilateral pCND was associated with significantly lower rates of transient hypocalcemia and no effect on permanent hypocalcemia. Raffaelli et al. compared the effect of TT with selective removal of enlarged lymph nodes (control group) versus TT with either routine ipsilateral or bilateral pCND (65). TT with routine bilateral pCND was associated with significantly higher rates of transient but not permanent hypocalcemia.
El Khatib et al. carried out a retrospective study comparing the effect of unilateral versus bilateral thymectomy in patients undergoing TT with pCND (66). They showed that bilateral thymectomy significantly increased the risk of transient hypocalcemia (p<0.001). In addition, no benefit regarding cancer resection was observed, as none of the cases had metastasis in the contralateral thymus. Only two patients had micro-metastases in lymph nodes located at the upper pole of ipsilateral thymus but no metastasis within the thymic tissue itself.
Calcium and vitamin D supplementation
Calcium and vitamin D supplementation is summarized in Supplementary Table S9. Calcium and vitamin D medications are usually given for the treatment of post-thyroidectomy hypocalcemia but have been tried as prophylactic treatment to reduce the risk of this complication. Eight studies met our inclusion criteria, and all patients had undergone TT±CND. Seven studies included patients with both benign and malignant thyroid disease, and one study only included patients with PTC (67).
Bellantone et al. randomly assigned patients into one of three arms: one arm (control group) receiving no supplements, the second arm received oral calcium only (3 g/day), and the third arm received oral calcium 3 g/day+calcitriol 1 μg/day postoperatively (68). They found a significantly lower risk of transient hypocalcemia associated with postoperative supplements but did not assess permanent hypocalcemia.
Two other RCTs compared combined oral calcium and vitamin D supplements versus oral calcium alone (69,70). One study showed significant reduction in the risk of transient hypocalcemia associated with oral calcium and vitamin D (1 μg calcitriol) (70) but no effect on permanent hypocalcemia. The other study found that combined supplementation of calcium and vitamin D decreased the risk of severe/symptomatic hypocalcemia (not assessed transient and permanent hypocalcemia separately) (69). Meta-analysis demonstrated that combined calcium and vitamin D supplementation was associated with significant reduction in transient hypocalcemia compared to calcium supplements alone (Fig. 6A; OR 0.66 [CI 0.45–0.98]; p=0.04).
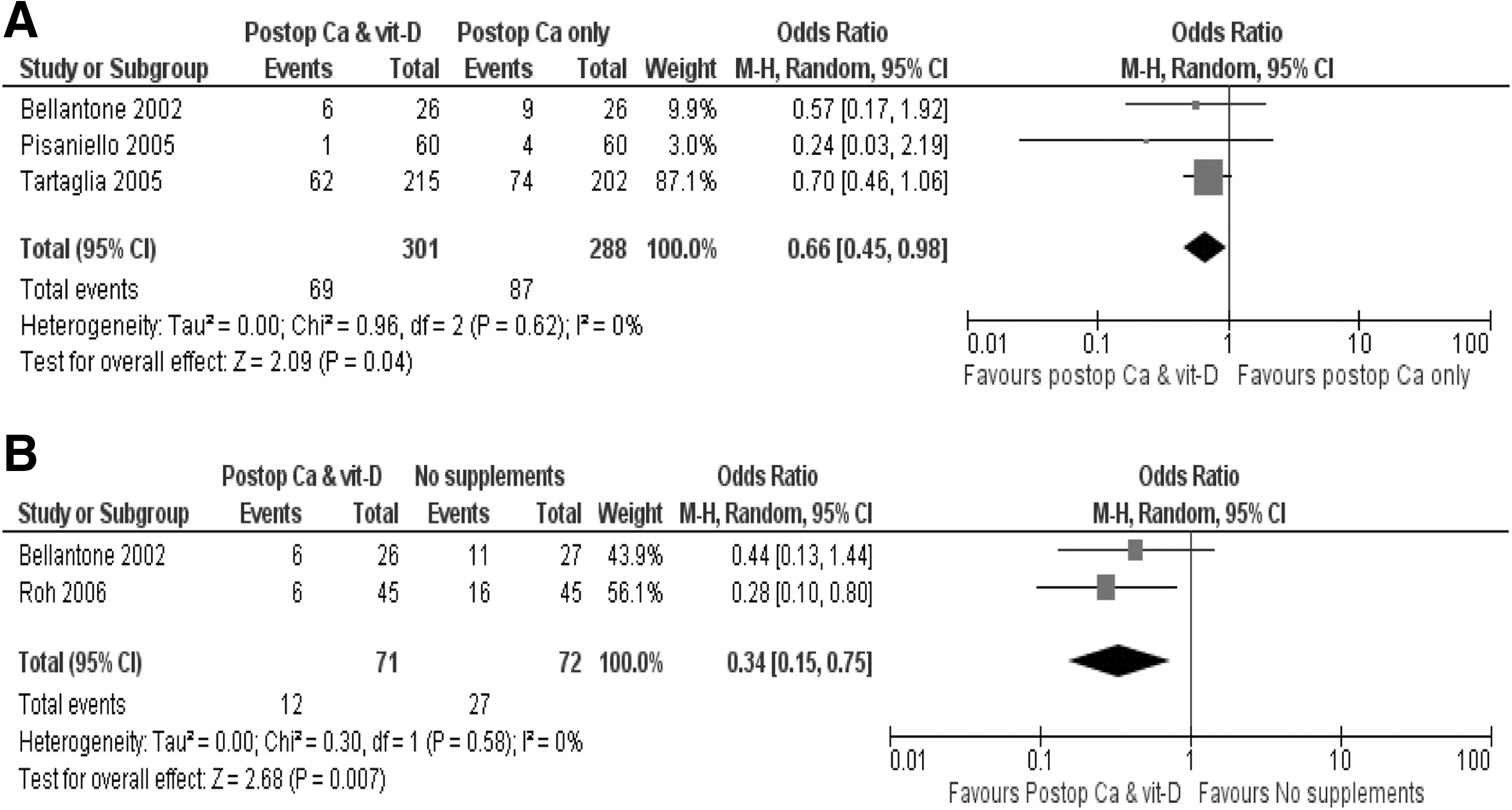
Meta-analysis comparing oral calcium and vitamin D supplements versus (
Roh et al. found that routine supplementation with combined oral calcium and vitamin D significantly reduced the risk of transient hypocalcemia but had no effect on permanent hypocalcemia when compared to no supplementation (31). Meta-analysis showed that postoperative calcium and vitamin D supplementation was associated with significantly lower rates of transient hypocalcemia compared to no supplements (Fig. 6B; OR 0.34 [CI 0.15–0.75]; p=0.007).
Genser et al. randomly assigned 108 patients to a control group who received no supplementation and a further 111 patients who received 2 μg of alfacalcidol daily from the day before surgery (D1) to postoperative day 8 (POD8) (71). They found that routine alfacalcidol supplements significantly reduced the incidence of severe, symptomatic, and permanent but not transient hypocalcemia.
Testa et al. examined the effect of a one-week preoperative administration of vitamin D with a thiazide diuretic versus no supplements/placebo (72). They reported significantly lower rates of transient hypocalcemia and shorter length of hospital stay (LOS), but they did not assess permanent hypocalcemia.
Uruno et al. carried out a prospective cohort study to assess if postoperative intravenous prophylactic calcium infusion could reduce the incidence of symptomatic hypocalcemia (73). The group receiving prophylactic calcium infusion had significantly more patients who underwent TT with CND for thyroid cancer; this could represent a potential confounding factor. Patients who received prophylactic infusions had significantly lower incidence rates of postoperative numbness and tetany and higher postoperative mean serum calcium levels. Transient and permanent hypocalcemia were not assessed.
Roh et al. carried out a RCT to assess the effect of postoperative supplements on rates of hypocalcemia in a cohort of patients with PTC (67). The study had patients randomized to one of three intervention arms: TT+CND receiving routine oral calcium and vitamin D (group A); TT+CND receiving routine oral calcium only (group B); TT+CND receiving no routine supplements (group C). These groups were compared to a control group of patients who had TT without CND and received no postoperative supplements. Combined oral calcium and vitamin D supplementation (group A) significantly reduced the rates of symptomatic and biochemical hypocalcemia. In addition, patients who received calcium alone had significantly lower rates of transient hypocalcemia. Supplementation with combined calcium and vitamin D or calcium alone had no effect on permanent hypocalcemia.
Truncal ligation of the inferior thyroid artery
Truncal ligation of the inferior thyroid artery is summarized in Supplementary Table S10. Three RCTs (74 –76) and one prospective cohort study (77) assessed the role of ITA truncal ligation versus no truncal ligation (capsular hemostasis). They found no association between ITA truncal ligation and transient or permanent hypocalcemia. Meta-analyses of the three RCTs also showed no significant effects (Fig. 7A and B).
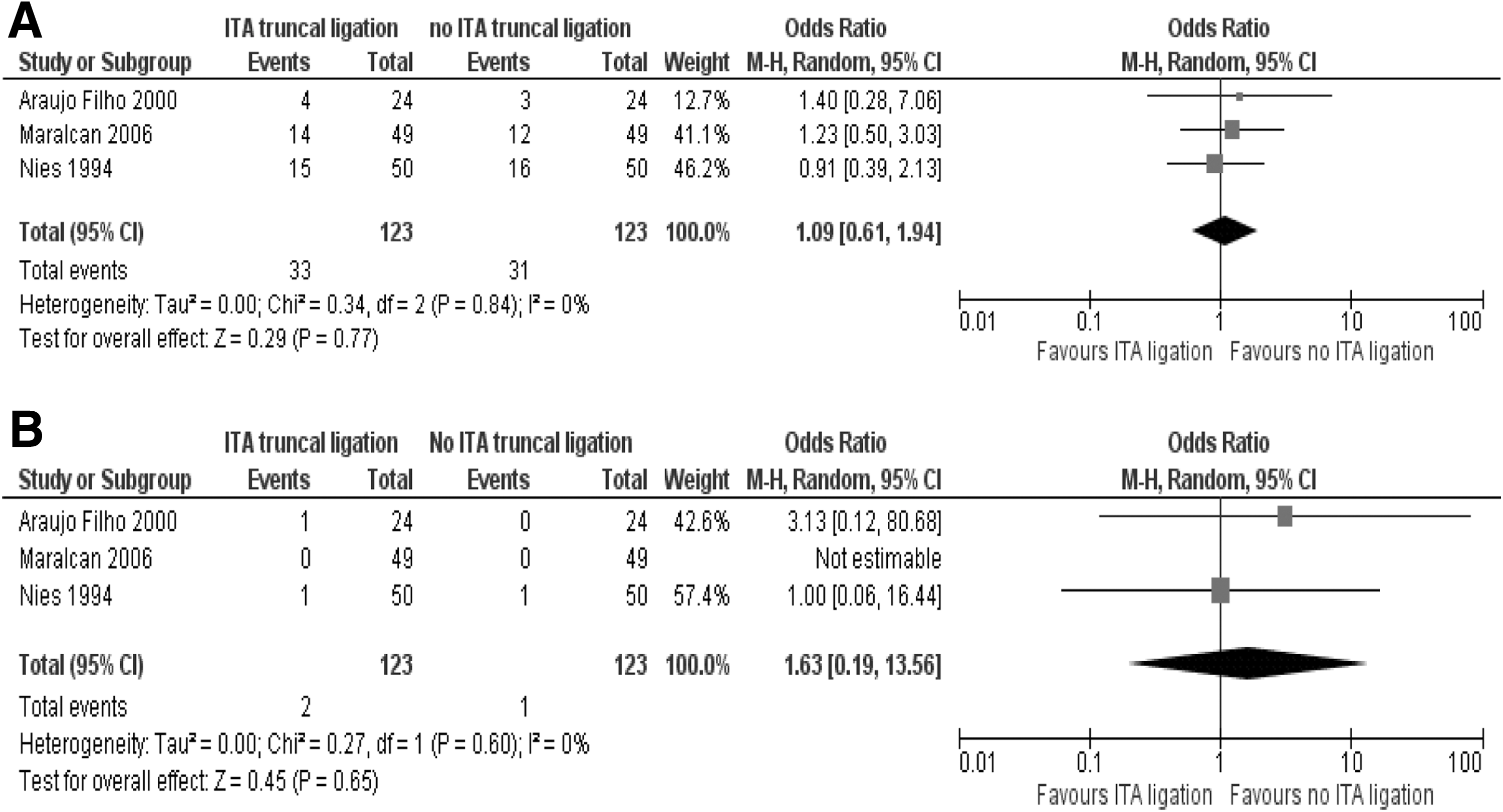
Meta-analysis comparing inferior thyroid artery (ITA) truncal ligation versus no ITA ligation on (
PGAT
PGAT is summarized in Supplementary Table S10. The role of PGAT in the prevention of hypocalcemia is another debatable issue in thyroid surgery. Most surgeons would perform it only if the PGs looked ischemic toward the end of surgery (78). Three cohort studies compared routine PGAT (suspiciously viable PG and at the surgeon's discretion) versus no PGAT. Lo et al. prospectively found a significantly higher risk of transient (78), while Testini et al. retrospectively found a significantly lower risk of transient hypocalcemia with routine PGAT (79). Both studies found that routine PGAT had no significant effect on permanent hypocalcemia. In contrast, Ahmed et al. reported a significantly lower risk of permanent (but no effect on transient) hypocalcemia associated with routine PGAT retrospectively (80).
Abboud et al. carried out a retrospective cohort study comparing the effect of autotransplantation of two or more PGs versus routine autotransplantation of one gland (81). They showed a significantly higher risk of transient (but not permanent) hypocalcemia with autotransplantation of two or more PGs.
Barczynski et al. performed a RCT to compare intraoperative PTH (ioPTH) guided PGAT versus elective autotransplantation of at least one PG (82) with 170 patients in each group. They found that ioPTH-guided PGAT significantly reduced the rates of transient hypocalcemia with no effect on permanent hypocalcemia.
Other preventive measures
Other preventative measures are summarized in Supplementary Table S11.
Surgical approach
Two cohort studies compared minimally invasive video-assisted thyroidectomy (MIVAT) to open TT (83,84). There was no difference in the incidence of transient (83,84) and permanent (84) hypocalcemia between MIVAT and open TT. Del Rio et al. did not assess permanent hypocalcemia (83).
Use of magnification loupes
Testini et al. carried out a RCT to assess the benefit of using loupe magnification in patients undergoing TT (85). They found that the incidence of transient hypocalcemia was 4.3% with loupe magnification compared to 14% without. No statistical tests for significance testing were reported.
Use of oxidized regenerated cellulose (Surgicel)
In a prospective study of 372 patients undergoing TT, Del Rio et al. examined the effect of using Surgicel on the rates of hypocalcemia (86). Despite having defined transient (serum calcium <2.0 mmol/L) and permanent (persistent >12 months) hypocalcemia, results were reported as mean postoperative calcium levels and found no difference associated with the use of Surgicel.
Preoperative intravenous magnesium infusion
Besic et al. carried out a RCT to test the effect of a preoperative intravenous magnesium infusion in patients undergoing TT and NTT without LND (34). Preoperative magnesium infusion had no significant effect on hypocalcemia rates.
Intraoperative identification of PGs
Another prospective cohort study of 126 patients found that intraoperative identification of three or more PGs (compared to zero to two PGs) was associated with a significantly higher rate of symptomatic, but no effect on transient hypocalcemia (87). Table 1 summarizes the effects of the preventative and other surgical measures that are covered in this review.
CH, conventional hemostasis; NTT, near total thyroidectomy; TT, total thyroidectomy; ST, subtotal thyroidectomy; HD, Hartley Dunhill; pCND, prophylactic central neck dissection; MIVAT, minimally invasive video-assisted thyroidectomy; ITA, inferior thyroid artery; ioPTH, intraoperative parathyroid hormone; i.v., intravenous; Mg, magnesium; Ca, calcium; vit D, vitamin D; PG, parathyroid gland; PGAT, parathyroid gland autotransplantation; preop, preoperative; intraop, intraoperative; postop, postoperative.
Discussion
Hypocalcemia is by far the most common complication following thyroid surgery, with a significant short- and long-term impact on patients' health. The effectiveness of preventative measures aimed to reduce the risk of post-thyroidectomy hypocalcemia has been evaluated in many original articles.
A recent meta-analysis of eight studies compared the use of the harmonic scalpel versus LigaSure in patients undergoing unilateral and bilateral thyroid surgery (88). They found no significant difference between the two devices on postoperative morbidity including hypocalcemia. Our meta-analyses found no significant impact on either transient or permanent hypocalcemia with the use of harmonic system compared to conventional hemostasis (Fig. 2A and B). In addition, LigaSure did not reduce transient hypocalcemia rates, when compared to conventional hemostatic techniques (Fig. 3). There were more studies on the harmonic device (17 studies with 1314 patients) than for LigaSure (two studies with 70 patients) that were eligible for inclusion in our meta-analyses. Funding from commercial sponsors could introduce risk of publication bias. Of the 22 studies that compared the harmonic scalpel to other hemostatic techniques, 11 did not report on funding source, 10 declared no external funding source, and one declared funding by Ethicon (45). Of the seven studies that compared LigaSure to other hemostatic techniques, four did not report on funding source, two declared no external funding (35,51), and one was funded by a research scholarship from the American College of Surgeons (23). Therefore, well-designed large RCTs are required to evaluate the effectiveness of these two devices.
In recent years, surgeons have increasingly adopted TT as the operation of choice for both benign and malignant disease to reduce the risk of disease recurrence and at the same time have demonstrated similar complication rates (8,89). However, our meta-analysis suggests that less extensive surgery is associated with lower rates of transient hypocalcemia such as in BST versus HD (Fig. 5A). In another meta-analysis of four studies comparing ST (n=332) to TT (n=342) in patients with Graves' disease, ST was found to reduce the incidence of transient but not permanent hypocalcemia (90). We do not believe that these results significantly influence the argument in favor of less extensive surgery, as there is no demonstrable impact on permanent hypocalcemia, and a number of other outcomes such as risk of disease recurrence and nerve injury rates need to be taken into account.
PTC usually has an excellent prognosis, and therefore prophylactic CND in patients without macroscopic evidence of lymph node disease is not routinely advocated (91). Although there are no RCTs on this topic, observational evidence from included studies in this review suggests that routine pCND increases the risk of hypocalcemia. Hypocalcemia rates may be improved by reducing the extent of central neck dissection. Limiting CND to the ipsilateral central compartment (63,64) or by preserving the contralateral thymus (66) could reduce the risk of transient (but not permanent) hypocalcemia (Supplementary Table S8).
The use of prophylactic calcium and vitamin D supplementation and the nature of the supplementation regime vary considerably in clinical practice as shown in this review. Evidence from this review showed that patients who receive prophylactic calcium and/or vitamin D supplements are at a lower risk of developing transient but not permanent hypocalcemia. Some studies also postulated that routine postoperative supplementation may allow earlier and safe patient discharge (67,68,70,72). This may be more cost-effective and facilitate the growing trend toward outpatient surgery. However, this may mask true hypocalcemia rates, and lead to overtreatment in some patients, with potential for harm if supplements are continued in the long term (92,93).
Alhefdhi et al. performed a meta-analysis of RCTs to assess the role of routine calcium and vitamin D supplementation in reducing the rate of symptomatic post-thyroidectomy hypocalcemia (94). However, they have erroneously included one prospective study (73) and another cohort study with a historical control (95). They also included a study that compared routine to “on demand” supplements in patients with symptomatic hypocalcemia, which represents a treatment rather than a prevention study (32). Despite significant variability in patient characteristics and definitions used, they concluded that routine postoperative supplementation, particularly combined calcium and vitamin D, significantly reduced postoperative hypocalcemia. A similar meta-analysis of four RCTs assessed the effect of routine calcium and vitamin D on reducing the incidence of postoperative symptomatic hypocalcemia (96). They reported that combined calcium and vitamin D supplements was associated with significantly lower rates of symptomatic hypocalcemia compared to either calcium alone or no supplements. The variability in the form, dose, and duration of supplements used in the different studies limits the strength of evidence and the applicability of the results to clinical practice.
The authors of this review recently published a meta-analysis on predictors of post-thyroidectomy hypocalcemia where intraoperative and postoperative PTH were found to be effective predictors of transient hypocalcemia with a sensitivity ranging from 59% to 100% (4). Given the relative benefits and risks of routine postoperative calcium and vitamin D supplementation, the use of intra- (or post-) operative PTH levels to predict the risk of post-thyroidectomy hypocalcemia and guide the need for supplements in a proportion of patients appears to be a reasonable way forward. Islam et al. recently presented a management algorithm using postoperative serum PTH levels to guide the use and weaning of postoperative supplements in patients undergoing total and completion thyroidectomy (97).
Truncal ligation of the inferior thyroid artery (ITA), adopted to reduce bleeding during thyroidectomy, was thought to result in parathyroid devascularisation and increased risk of post-thyroidectomy hypocalcemia. However, this was not demonstrated to be the case in the four studies included in this review (Fig. 7A and B). The role of routine autotransplantation of PGs in reducing hypocalcemia remains controversial. However, selective transplantation based on ioPTH measurements may be useful in reducing transient hypocalcemia rates (82).
Several other measures such as video-assisted thyroidectomy, preoperative magnesium infusion, and use of loupes have not been demonstrated to be effective preventative measures.
Limitations
Several potentially significant factors were only assessed in observational studies or single RCTs preventing the incorporation into meta-analyses. Most of these studies did not carry out a multivariable analysis to adjust for potential confounders. Small sample sizes (<50 patients) (21,25,34,72,74) combined with the infrequent occurrence of permanent hypocalcemia could have increased the risk of type II error. The significant variation in the definitions of hypocalcemia, intervention regimes, surgical techniques, and assessment methods could have biased the strength of the meta-analyses presented.
Recommendations
Consensus guidelines for the definitions of transient and permanent hypocalcemia should be established and adhered to in the reporting of these outcomes. This would increase the generalizability and reliability of published results. Well-designed, large, multicenter RCTs are still needed to determine the effectiveness of currently used preventative measures such as hemostatic devices and prophylactic calcium/vitamin D supplements in prevention of post-thyroidectomy hypocalcemia. The role of novel methods of early identification and preservation of PGs during thyroid surgery remain to be explored.
Footnotes
Acknowledgment
This work will be submitted for presentation in the upcoming annual BAETS conference in October 2014.
Author Disclosure Statement
There was no source of funding and no conflicts of interest to report.