
Abstract
Background:
Subclinical hypothyroidism (SCH) is postulated to increase stroke risk via atherogenic changes associated with abnormal thyroid function. However, the direct relationship of SCH with subsequent stroke is poorly studied.
Methods:
In this nested case–cohort study, we prospectively evaluated the association between any SCH and severity of SCH in relation to incident ischemic stroke risk among postmenopausal women in the Women's Health Initiative Observational Study. Trained Women's Health Initiative staff, masked to thyroid status, adjudicated stroke cases. We assessed thyroid function using baseline blood specimens. Women with normal free thyroxine levels and thyrotropin (TSH) levels ≥4.69 mU/L were considered to have SCH. Primary analysis included 639 ischemic stroke cases and 2927 randomly selected subcohort members with an average of seven years of follow-up.
Results:
The multivariable adjusted hazard ratios (HR) from weighted Cox models were 1.06 (95% confidence interval [CI]: 0.77, 1.46) and 0.99 (95% CI: 0.67, 1.47) for women with any SCH and with mild SCH (TSH 4.69 to 6.99 mU/L), when compared with women with normal thyroid function. The HR for moderate/severe SCH (TSH ≥7.00 mU/L) was modestly elevated (HR: 1.22; 95% CI: 0.73, 2.05).
Conclusions:
We found no evidence to suggest an association between SCH and ischemic stroke among healthy postmenopausal women.
Introduction
S
Indirect evidence for or against screening can be drawn from observational studies that evaluate the relationship between SCH and cardiovascular diseases. SCH has been reported to be associated with the grouping of conditions loosely termed coronary heart disease (7,8), ischemic heart disease (9), or cardiovascular disease (10), with definitions including but not limited to myocardial infarction (MI), angina, heart failure, stroke, and other cerebrovascular conditions. However, evidence for an association is not consistent and ranges from strong effects (two-fold increased risk) to null (8). Discrepancies likely arise from the heterogeneity of the composite outcomes, varying follow-up time, and differing population characteristics such as age range, sex, and varied cardiovascular disease status at baseline. Mixed findings extend to the relationship between SCH and intermediate endpoints such as atherosclerotic disease and lipid profiles (11,12).
Because the goals of screening for primary prevention are to identify individuals in a preclinical phase in order to reduce morbidity and mortality, motivation to screen for SCH must include specific outcomes that could be prevented if SCH were identified and treated. Using Women's Health Initiative Observational Study (WHI-OS) data comparable to that for this investigation, we have previously reported that an association of SCH with incident myocardial infarction is not supported by prospective data in postmenopausal women (13). The WHI-OS (14) is a well-characterized cohort of ethnically diverse postmenopausal women with biological samples available at baseline, a high follow-up rate, and a rigorous adjudication process for outcomes.
To round out examination of the association of SCH with cardiovascular disease by investigation of specific outcomes, our research team focused on whether there is evidence to support a link between SCH and incident ischemic stroke among healthy postmenopausal women, a population with high prevalence of SCH. Only two other studies, which were underpowered, have reported on the association between SCH and stroke (15,16). Our investigation improves on these previous studies. We employed an efficient nested case–cohort study design to reach sufficient power in the largest prospective study to date that can examine for main effects as well as for analyses by severity of SCH as it relates to incident ischemic stroke.
Methods
Study population
Women in this study were participants in the WHI-OS, a cohort of postmenopausal women between 50 and 79 years of age enrolled at 40 clinical centers across the United States between October 1993 and December 1998 (17). Inclusion/exclusion criteria for this ancillary analysis have been detailed previously (13). Briefly, from 93,676 women in the WHI-OS, women with anticipated residence in the local area for at least three years with baseline serum available in the specimen bank were eligible for inclusion. Exclusion criteria were self-reported history of current or previous thyroid disease, use of medications that may alter thyroid hormones, history of MI or stroke, history of coronary artery bypass grafting or carotid endarterectomy, and missing race/ethnicity data.
Ischemic stroke cases
WHI investigators conducted ascertainment of incident ischemic stroke cases every 12 months via review of self-reported annual medical follow-up updates (18). Ischemic stroke was defined as the rapid onset of persistent neurologic deficit lasting for 24 hours or more due to an obstruction, fatal or nonfatal, or detection of lesion through computed tomography or magnetic resonance imaging scan. Fatal and nonfatal locally adjudicated ischemic stroke cases through December 15, 2004 that were additionally confirmed by central adjudication by trained neurologists were considered for inclusion. Adjudicators were masked to participants' thyroid status. Reports of transient ischemic attacks and hemorrhagic strokes were not considered in this study. A total of 1050 cases were identified. After applying our inclusion/exclusion criteria, 675 cases were eligible for this analysis. Figure 1 provides details of exclusions. Because our goal was to examine the effects of SCH at baseline on future ischemic stroke risk, we further excluded observations that our laboratory analyses identified as having overt thyroid disease (n=9) or subclinical hyperthyroidism (n=16). Participants who had negative follow-up time (n=6) or for whom laboratory measures were unavailable (n=5) were also excluded. A total of 639 incident ischemic stroke cases were included in the primary unadjusted analysis.
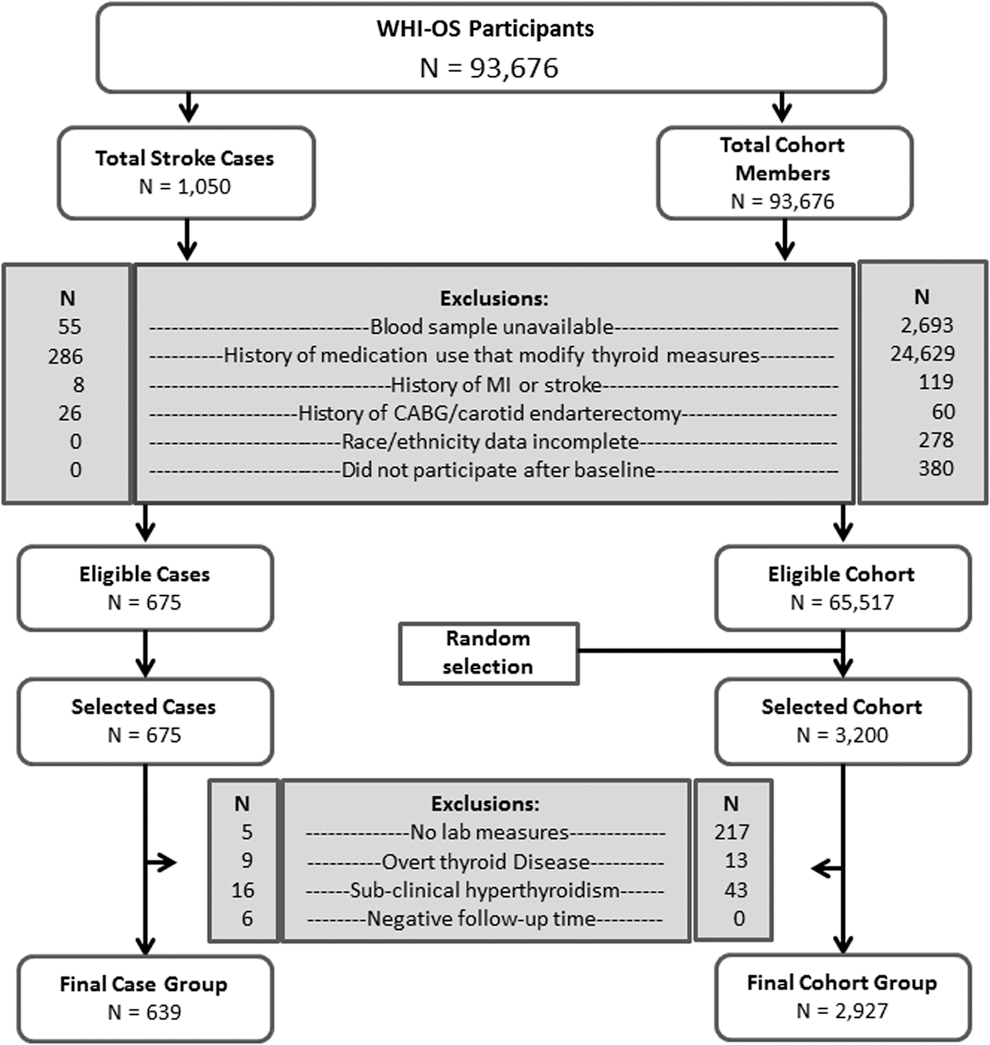
Schema representing the selection process for ischemic stroke cases and subcohort from the Women's Health Initiative Observational Study (WHI-OS). Adapted with permission from LeGrys et al. (13).
Comparison subcohort
By design, the subcohort for this study was generated to serve as a common comparison group for two separate analyses— one that evaluates SCH and risk for MI (13) and the present analysis. The same inclusion/exclusion criteria used for selection of MI and stroke cases were also applied to the entire WHI-OS cohort. We used random sampling and density matching within five-year age strata to match the age distribution of the 800 MI and 675 stroke cases, identifying 3200 members for the comparison subcohort (Fig. 1). We obtained stored specimens for the subcohort and conducted the same laboratory analyses as for case groups; observations in the subcohort with subclinical hyperthyroidism, with overt thyroid disease, and with no laboratory measures were excluded. After exclusions, the subcohort consisted of 2927 observations available for primary unadjusted analysis.
Thyroid hormone measurement
Laboratory procedures for thyroid measurements have been described in detail previously (13). Briefly, specimens were analyzed between March 2005 and December 2006. Laboratory personnel were blind to participant characteristics including stroke or MI status. TSH was measured using a chemiluminescent immunometric assay with a detection range from 0.01 to 100 mU/L. TSH values between 0.46 and 4.68 mU/L were considered the normal reference range (euthyroid). Specimens with TSH values above or below the normal reference range were tested for free thyroxine (FT4) and thyroid peroxidase antibodies (TPOAb). FT4 was measured using a competitive chemiluminescent assay with a detection range of 0.1–12.0 ng/dL. FT4 concentrations within 0.70–1.85 ng/dL were the normal reference range. TPOAb was measured using a solid-phase, sequential chemiluminescent immunometric assay with a detection range of 10–1000 IU/mL. Specimens with TPOAb concentrations ≥35 IU/mL were considered to be TPOAb positive. All samples included in the study met quality control criteria. Samples with TSH values ≥4.69 mU/L and normal FT4 levels were classified as indicating SCH.
Statistical analyses
The sampling strategy of a case–cohort design allows resampling of cases into the subcohort portion of the population. Thus, pseudo-likelihood based methods must be used to account for the non-independent score contributions. We used weighted Cox-proportional hazards models as proposed by Barlow and colleagues (19) along with jackknife estimated robust standard errors (20) to appropriately account for the non-independence and provide reliable estimates of the hazard ratio (HR) and variance. We report unadjusted and multivariable adjusted associations between SCH and stroke. Candidate covariates were chosen a priori as either potential confounders or established risk factors for stroke. These included age, race/ethnicity, WHI site, years since menopause, gravidity, parity, hypertension, current diabetes, hormone therapy (HT), smoking history, alcohol consumption, physical activity, body mass index, and waist-to-hip ratio.
We developed a parsimonious model using directed acyclic graphs to include only confounders in the assessment of any SCH and its relationship to stroke. We did not impute missing data and report hazard ratios based on complete-case analysis. There were 626 cases and 2843 subcohort members available in the primary parsimonious model examining any SCH and stroke. Variables included in the parsimonious models were age, ethnicity, smoking status, HT use, gravidity, and alcohol consumption. All subsequent models were adjusted for these variables. Additional adjustment for risk factors such as diabetes status, physical activity, waist-to-hip ratio, and/or body mass index in a fully adjusted model changed effect estimates negligibly. In addition to examining the association between any SCH and stroke, we conducted separate analyses by stratum of SCH severity, restricted to exposed individuals who had mild SCH (TSH 4.69 to 6.99 mU/L), moderate/severe SCH (TSH≥7.00 mU/L), and individuals who had moderate/severe SCH and were TPOAb-positive. All were compared to women with normal thyroid function. We used the likelihood ratio test to formally evaluate effect modification of the association between severities of SCH and stroke by age, smoking status, waist-to-hip ratio, ethnicity, alcohol consumption, gravidity, and HT use. We tested the proportional hazards (PH) assumption by visual inspection of log–log survival curves and by including an interaction term for natural log–transformed follow-up time and the SCH variables in the Cox-models. We detected no gross violations of the PH assumption.
We conducted several sensitivity analyses. First, we reexamined the association between SCH and stroke by removing individuals with potentially impending overt thyroid disease (TSH ≥20 mU/L). Second, to facilitate comparisons with other studies which report varying thresholds for SCH (8,21,22), we reanalyzed data by changing the TSH threshold for SCH, decreasing it to 4.50 mU/L and increasing it to 5.00 mU/L. Third, to examine the association between SCH and stroke without the influence of intercurrent diagnosis and treatment of thyroid disease, we restricted our analysis to women who had follow-up information on these factors in year three, and then excluded women who reported using thyroid medications. Data compilation and bivariate analyses were done in STATA 12 (College Station, TX). Weighted Cox-PH models were generated using SAS 9.3 (Cary, NC). This study was reviewed and determined to be exempt from further review by the Institutional Review Board at the University of North Carolina, Chapel Hill, and was approved by the Institutional Review Board at Vanderbilt University.
Results
The mean age of the 3566 women included in this case–cohort analysis was 67.5 years, and the majority self-identified as Caucasian/white (83.9%). Baseline thyroid measures indicated 280 women (7.8%) had SCH (TSH ≥4.69 mU/L), the majority (68.2%) of whom had mild SCH (TSH 4.69 to 6.99 mU/L), and the remaining had moderate/severe SCH (TSH ≥7.00 mU/L). Increasing age was positively associated with SCH, and whites were more likely to have SCH than other races/ethnicities. At baseline, compared with participants in the subcohort, stroke cases were more likely to be older, heavier, and more likely to have had 5 or more pregnancies. Stroke cases were also more likely to be current smokers, and have diabetes and hypertension. Stroke cases were less likely to consume alcohol and less likely to be physically active, although the latter was not statistically significant (Table 1). Baseline characteristics of the randomly sampled subcohort are very similar to the entire WHI-OS cohort (17).
Numbers do not always total 3566 due to missing data for covariates.
p-Value: calculated using the Pearson's chi-squared test.
Cumulative stroke incidence curves for euthyroid women, women with mild SCH, and women with moderate/severe SCH during the average 7-year follow-up period are shown in Fig. 2. Risk for stroke among women with any SCH at baseline was not appreciably different than for women with normal thyroid function at baseline (Table 2); the corresponding multivariable adjusted hazard ratio was 1.06 [95% confidence interval (CI): 0.77, 1.46]. Compared with women with normal thyroid function, HRs for women with mild SCH and moderate/severe SCH were 0.99 [CI: 0.67, 1.47] and 1.22 [CI: 0.73, 2.05], respectively. Women who had moderate/severe SCH and were also TPOAb positive had a hazard ratio of 0.83 [CI: 0.42, 1.64] (Table 3).
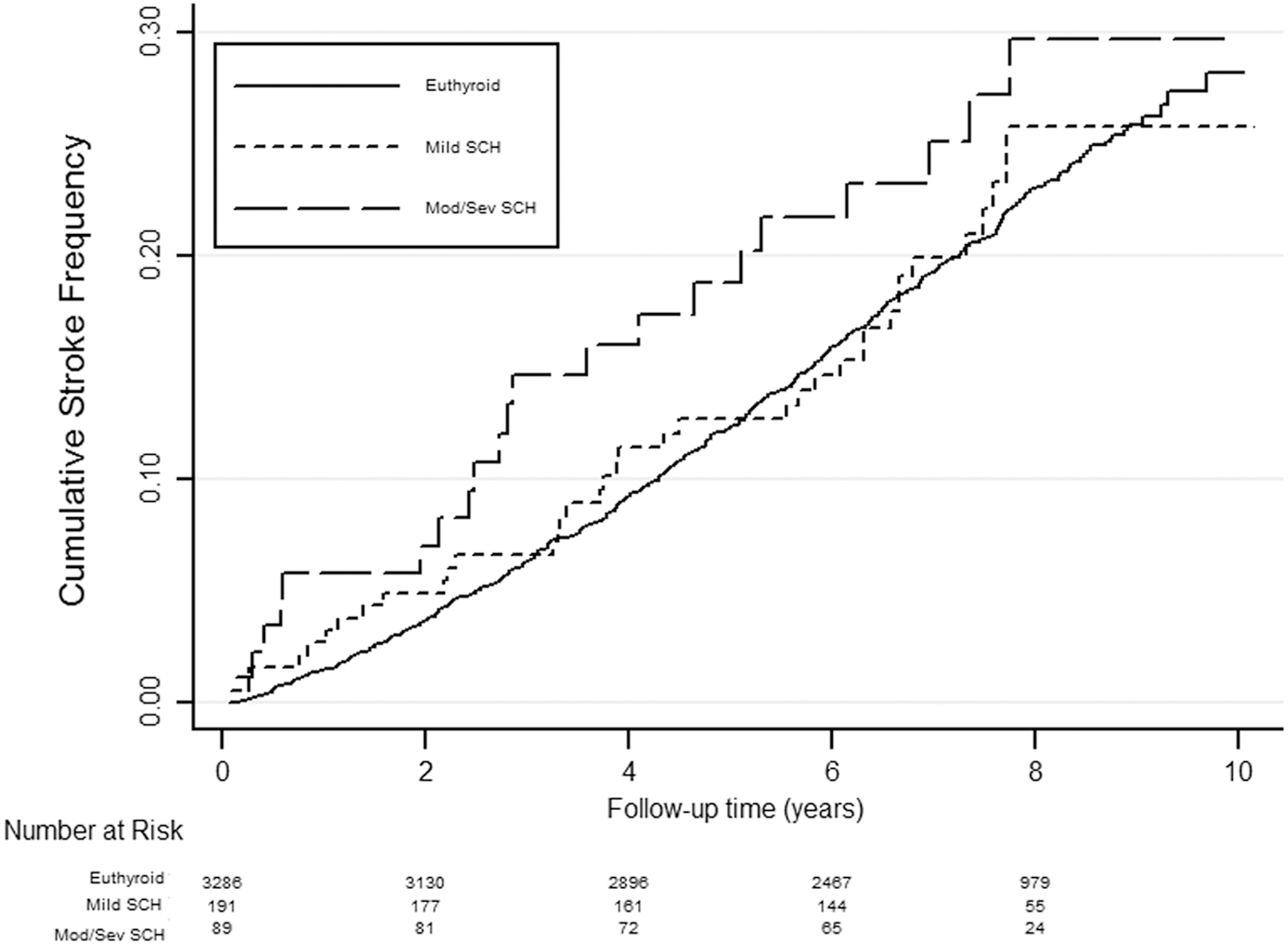
Nelson-Aalen cumulative hazard estimates for ischemic stroke by severity of subclinical hypothyroidism (SCH) among women from the WHI-OS. Solid line represents euthyroid participants; short-dashed line represents participants with mild subclinical hypothyroidism; long-dashed line represents individuals with moderate/severe subclinical hypothyroidism. Mod/sev, moderate/severe; Euthyroid, thyrotropin (TSH) 0.46–4.68 mU/L; Mild SCH, TSH 4.69–6.99 mU/L; Mod/Sev SCH, TSH ≥7.00 mU/L.
Sample size based on entire sample.
Any subclinical hypothyroid vs. euthyroid.
Mild subclinical hypothyroid (thyrotropin [TSH] 4.69 to 7.0 mU/L) vs. euthyroid (moderate/severe category omitted).
Moderate/severe subclinical hypothyroid (TSH≥7.0 mU/L) vs. euthyroid (mild category omitted).
Moderate/severe and thyroid peroxidase antibody (TPOAb) positive vs. euthyroid (mild and TPOAb negative omitted).
Cox regression was modeled with ln(TSH) as a continuous variable; corresponding hazard ratios are for every 20% increase in TSH.
Sample size based on same observations used in the adjusted model.
Adjusted for age, ethnicity, gravidity, smoking status, hormone therapy, and alcohol consumption; covariates measured at baseline only.
CI, 95% confidence interval; HR, hazard ratio; SCH, subclinical hypothyroidism.
Total euthyroid, total number of participants with normal thyroid at baseline; euthyroid stroke cases, total number of euthyroid participants who developed stroke during study follow-up; total SCH, total number of participants with SCH at baseline; SCH stroke cases, number of SCH participants who developed stroke during study follow-up.
We found no meaningful interactions with age, smoking status, ethnicity, alcohol consumption, or gravidity (Supplementary Table S1; Supplementary Data are available online at
In our first sensitivity analysis, excluding women who had impending overt hypothyroidism (TSH ≥20 mU/L) yielded similar results as those for women with any SCH (HR: 1.05; [CI: 0.76, 1.45]), and those with moderate/severe SCH (HR: 1.19; [CI: 0.69, 2.05]). Similarly, in our second analysis, changing the TSH threshold from 4.69 mU/L to 4.50 mU/L or to 5.00 mU/L did not substantially change our results. Third, among women who reported information on thyroid medication use at 3 years of follow-up, exclusion of women who were using thyroid medications yielded similar results (HR: 0.91; [CI: 0.74, 1.13]) for any SCH.
Discussion
In this large case–cohort investigation of postmenopausal women from the WHI-OS, we did not find evidence to suggest an association between SCH at baseline and risk for incident ischemic stroke. Compared with women with normal thyroid function, effect estimates were only modestly elevated for women with moderate/severe SCH (TSH ≥7.00 mU/mL); however, the confidence interval included unity. Projecting 750 stroke cases, a 1:4 case–cohort ratio, and a type-1 error of 5%, a priori approximation of the minimum detectable effect estimate was 1.43 with 90% power if prevalence of SCH was 10%, and 1.81 with 80% power if prevalence of SCH was 2%. Post-hoc calculations based on population available for analysis (639 cases, 2927 comparison cases) demonstrated a 7.8% SCH prevalence; with a type-1 error rate of 5%, we had 80% power to detect an effect estimate of 1.51. Despite targeting our investigation to a population with high prevalence of SCH and relatively high incidence of stroke, the effect estimates we observed for SCH were very close to the null.
Our search of the literature identified only two prospective cohort studies (Table 3) that specifically reported on SCH and stroke risk. They have diametrically opposed and underpowered associations (15,16). Rodondi and colleagues reported larger effect estimates for participants with moderate SCH, defined as TSH 7.00 to 9.99 mU/L (HR: 2.16; [CI: 0.93, 5.00]; with 7 strokes) than for those with mild SCH, defined as TSH 4.5 to 6.9 mU/L (HR: 1.13; [CI: 0.62, 2.07]; 12 strokes), during a 4-year follow-up (15). Schultz and colleagues reported a hazard ratio of 0.74 [CI: 0.10, 5.50] for participants with SCH compared with euthyroid participants with 31 SCH cases at baseline and 28 incident stroke cases (one stroke case in the SCH group) (16). Effect estimates from both studies lack precision, as indicated by the confidence intervals. Two other studies reported the association between SCH and incident cerebrovascular disease, including stroke events. One observed a null effect-estimate (21), HR of 1.01 [CI: 0.79, 1.29], and the other observed elevated risk with an HR of 1.9 [CI: 0.5, 7.30] (22); neither performed analyses using information about severity of SCH.
The mechanisms relating overt hypothyroidism to cardiovascular and cerebrovascular conditions including coronary heart disease, MI, and stroke are well understood. Overt hypothyroidism has been associated with atherogenic lipid profiles, diastolic hypertension, impaired endothelial function, hyperhomocysteinemia, and increased C-reactive protein levels (23 –26). The mechanisms relating SCH to cerebrovascular conditions such as stroke are less clearly understood. Studies have shown SCH to be associated with increased carotid arterial stiffness (27), elevated serum low-density-lipoprotein cholesterol (28,29) and apolipoprotein-B (30), elevated mean platelet volume (31), and altered low-density-lipoprotein-C oxidizability (32); however, evidence has not been consistent (12). In the context of vascular diseases, it is likely that the downstream effects of overt hypothyroidism are due to reduced thyroxine levels rather than elevated TSH, which serves as an indicator of the dysfunction. If SCH is in fact associated with stroke or MI, it would likely be due to similar mechanisms as with overt hypothyroidism. Contrary to expectations, the hazard ratio for individuals with moderate/severe SCH who were also TPOAb positive was in the inverse direction in our study.
Several studies have observed improvement in cardiovascular outcomes associated with overt hypothyroidism and SCH after treatment with L-thyroxine (30,33,34), although results are inconsistent. Even though FT4 levels among patients with SCH are within “normal range,” there is a continuum of FT4 levels within this group, with some individuals presenting with FT4 concentrations closer to the overt hypothyroidism spectrum. This is also evident in our study; we observed a mean decrease in FT4 levels with increasing severity of SCH. Mean FT4 concentrations in individuals with mild (TSH 4.69 to 6.99 mU/L), moderate (TSH 7.00 to 9.99 mU/L), and severe SCH (TSH ≥10.00 mU/L) were 1.03, 0.94, and 0.86 ng/dL respectively (data not shown). Thus lower thyroxine levels in more severe forms of SCH could diminish its inhibitory effects on collagen-induced platelet aggregation and increase vascular resistance. Hypothesizing that SCH-mediated onset of coronary heart disease and stroke share similar pathways, Rodondi and colleagues conducted a meta-analysis of SCH and coronary heart disease and found elevated risk in participants with severe SCH (TSH ≥10.00 mU/L), but not in participants with relatively milder forms of SCH (8), a likely consequence of decreased FT4. Similarly, McQuade and colleagues reported a lack of association between mild-SCH and all-cause mortality, but reported statistically significant hazard ratios for those with moderate SCH and severe SCH, all compared with euthyroid participants (35). Additionally, studies have suggested an inverse correlation between serum FT4 levels and atherosclerosis among euthyroid patients (36,37). The antagonistic effect of estrogen use on efficacy of
A plausible reason for observing no association between any SCH and stroke is potential misclassification of SCH subjects over the course of the study, which could have biased our results towards the null. We measured thyroid hormones only at baseline and were unable to track thyroid status after baseline except by claim. Somwaru and colleagues reported 46% of participants with mild SCH reverted from SCH to euthyroid status over a two-year period (39). However, in the same study as few as 10% of the participants with moderate SCH (TSH 7.0 to 9.9 mU/L) and 7% of the participants with severe SCH (TSH ≥10.0 mU/L) reverted back to euthyroid status during the same 2-year period. Thus, in our study, error due to misclassification in the moderate/severe group is likely to be low. Furthermore, we are unable to assess stroke risk by FT4 levels because only specimens above and below the normal TSH reference range were tested for FT4. Additionally, we did not assess stroke risk exclusively among individuals with severe SCH due to the small number of participants that met this criterion. It is also possible that an average of 7 years (interquartile range: 6.0 to 8.4 years) of follow-up was not sufficient to detect the cumulative effect of mild SCH on stroke occurrence. Finally, lacking information on lipid characteristics, we were not able to examine the mediating effects of lipids on SCH-mediated stroke occurrence. It should however be noted that even if this information were available and we assume that this model is correct, adjustment for lipid characteristics would only further work to nullify any elevated association between SCH and stroke, consequently strengthening the current conclusion of this investigation.
Despite these drawbacks, to our knowledge, this is the largest study (639 stroke cases) to date to have explicitly examined SCH and risk for stroke. The size of the study allowed us to report the marginal association between SCH and stroke, after adjusting for potential confounders. Our sample was also large enough to report effect estimates by severity of SCH. Furthermore, we conducted multiple sensitivity analyses, which did not appreciably change our results. Density-matched sampling of the comparison cohort from the entire eligible WHI-OS ensured a good approximation of the risk ratio and minimized the possibility of selection bias because cases and subcohort both originated from the same base population.
In this population of postmenopausal women with no history of cardiovascular conditions, we did not find evidence of association between SCH and risk for incident ischemic stroke. This was particularly true for mild SCH. In conjunction with biological rationale, there is still reason to speculate that individuals with more severe forms of SCH may be at increased risk for stroke. However, given the lower prevalence of moderate/severe SCH and the modest elevation of stroke risk (if any) associated with it, its impact on a population level is likely to be small and thus the utility of screening to forestall stroke outcomes extremely low or absent. The European Commission recently funded the Thyroid Hormone Replacement for Untreated Older Adults with Subclinical Hypothyroidism Trial (40), which examines the relationship between thyroid hormone treatment and several cardiovascular and noncardiovascular outcomes. Until the results of the trial are published, efficient observational studies such as ours provide the best available evidence for clinical or policy decisions.
Footnotes
Acknowledgments
The WHI program is funded by the National Heart, Lung, and Blood Institute, National Institutes of Health, US Department of Health and Human Services through contracts N01WH22110, 24152, 32100-2, 32105-6, 32108-9, 32111-13, 32115, 32118-32119, 32122, 42107-26, 42129-32, and 44221. The authors thank the WHI investigators and staff for their dedication, and the study participants for making the program possible. The complete list of WHI centers and investigators can be found online at
Author Disclosure Statement
The authors have nothing to disclose.