
Abstract
Background:
Cabozantinib targets tyrosine kinases including MET, vascular endothelial growth factor (VEGF) receptor 2, and rearranged during transfection (RET). Differentiated thyroid cancer (DTC) is a tumor type that may be sensitive to cabozantinib. Therefore, we evaluated cabozantinib in a cohort of heavily pretreated patients with metastatic DTC.
Methods:
This single-arm open-label phase I trial assessed the safety, tolerability, and antitumor activity of cabozantinib in DTC patients taking part in a drug–drug interaction study. Adult patients with histologically confirmed metastatic or surgically unresectable DTC (including papillary, follicular, or Hürthle cell) were enrolled. Patients received daily oral dosing of 140 mg cabozantinib. Safety was assessed by evaluation of adverse events (AEs), vital signs, electrocardiograms, laboratory tests, and concomitant medications. Tumor response by magnetic resonance imaging or computed tomography scan was investigator assessed using Response Evaluation Criteria In Solid Tumors (RECIST) v1.0.
Results:
The study enrolled 15 patients who had failed standard radioactive iodine therapy. Patients had received a median of two prior systemic agents, and 11 patients (73%) had previously received at least one VEGF pathway inhibiting therapy. Common AEs included diarrhea, nausea, fatigue, and decreased appetite. Partial response was reported in eight patients (53%). Median progression-free survival and median overall survival were not reached.
Conclusions:
Cabozantinib demonstrates a safety profile similar to other multitargeted VEGFR inhibitors in advanced DTC patients. The antitumor activity observed in this study warrants further investigation of cabozantinib in patients with advanced DTC.
Introduction
C
The molecular pathophysiology of differentiated thyroid cancer (DTC) suggests that this tumor type may also be sensitive to cabozantinib. Patients with metastatic DTC frequently show activation of various receptor tyrosine kinases, including MET, VEGFR2, and RET. Recurrent chromosomal translocations that result in the generation of active RET fusion proteins are implicated in DTC pathogenesis, making RET inhibition an attractive approach for therapy (5). MET is overexpressed in approximately 90% of papillary thyroid cancer (6), and drives thyrocyte neoplastic transformation as a consequence of activated RET/PTC1 rearrangements (7). Also, expression of VEGF and other angiogenic factors in DTC was found to be associated with clinical pathological features and poor outcome (8,9).
Patients with metastatic DTC currently have limited treatment options. Doxorubicin, an FDA-approved systemic treatment for advanced refractory DTC, has shown a low rate of transient tumor response and significant toxicity (10). Sorafenib, a VEGFR-targeting tyrosine kinase inhibitor (TKI), was recently approved for the treatment of patients with locally recurrent or metastatic, progressive DTC that is refractory to radioactive iodine (RAI) treatment. This approval was based on the results of the DECISION trial, which showed improvement in PFS with sorafenib compared with placebo (11). Other VEGFR-targeted TKIs have also resulted in partial responses and prolonged disease stabilization, supporting the activity of this signaling pathway in thyroid tumor progression (12 –14).
Because MET, VEGFR2, and RET are implicated in DTC progression, this phase I study assessed the safety, tolerability, and preliminary antitumor activity of cabozantinib, which targets these pathways simultaneously, in advanced DTC patients. The study also included a cohort of patients with renal cell cancer (RCC), and had a pharmacokinetic primary endpoint based on a drug–drug interaction analysis to support a New Drug Application filing for cabozantinib dosed at 140 mg daily. In this report, we present the safety and efficacy data from DTC patients enrolled in the study (safety and efficacy results in RCC patients and drug–drug interaction and pharmacokinetics results will be published separately).
Methods
Patients
Adult patients with histologically confirmed metastatic or surgically unresectable DTC (including papillary, follicular, or Hürthle cell) were enrolled into the DTC cohort of this single-arm, open-label drug–drug interaction study. All patients were required to have measurable disease per Response Evaluation Criteria in Solid Tumors (RECIST v1.0) (15), and to be refractory to standard therapy with RAI. All patients had to have adequate bone marrow function and a Karnofsky performance score ≥70 (Eastern Cooperative Oncology Group (ECOG) performance status score ≤2). Patients were ineligible if they had received radiotherapy within 14 days, cytotoxic chemotherapy within 28 days, prior TKI or investigational hormonal therapy within the longer of 14 days or five half-lives, or other investigational agents within the shorter of 28 days or five half-lives before the first dose of study treatment. Patients were also ineligible if they were undergoing treatment with drugs known to be extensively metabolized by CYP2C8, or with drugs known to be inhibitors of CYP3A4 or CYP2C8, or that were inducers of CYP3A isozymes. The study was approved by the institutional review board at each study center and conducted in accordance with the Declaration of Helsinki. Patients provided written informed consent according to institutional guidelines.
Study design
The secondary and exploratory endpoints of this study included evaluating the safety, tolerability, antitumor activity, and effect on overall survival of daily oral administration of cabozantinib in DTC patients. The primary endpoint of the study was to evaluate the effect of cabozantinib on the plasma pharmacokinetics of the CYP2C8 substrate rosiglitazone (results pertaining to this endpoint will be published at a later date). Patients received a single dose of rosiglitazone on day 1 (for the drug–drug interaction portion of the study) and began daily oral dosing of 140 mg cabozantinib on day 2. On day 22, patients who had not experienced an interruption in cabozantinib dosing or a reduction below 100 mg/day received a second dose of rosiglitazone. From day 24 onward, patients continued to receive, at the discretion of the investigator, daily cabozantinib until progressive disease (PD) or unacceptable adverse events (AEs). Treatment compliance was monitored through records of drug dispensing and return.
Safety and efficacy assessments
Safety assessments, including the evaluation of AEs, vital signs, electrocardiograms, laboratory tests, and concomitant medications, were conducted on days 1, 2, 7, 15, 21, 22, and 57, then every four weeks through week 49, and every eight weeks thereafter. AEs were graded according to the Common Terminology Criteria for Adverse Events v3·0. In the event of absolute neutrophil count <1000/mm3, platelet count <50,000/mm3, grade 4 anemia, intolerable grade 2 toxicity, or any grade 3 or higher toxicity, study treatment was withheld. If the patient recovered within six weeks and toxicity was deemed unrelated to study treatment, treatment was restarted at the same dose. If the patient recovered within six weeks and toxicity was deemed possibly related to study treatment, therapy was restarted at a reduced dose (100 mg for the first reduction, and 60 mg for a second reduction), and could be re-escalated, except for cases of neutropenia or thrombocytopenia. Patients who did not recover within six weeks discontinued study treatment.
Tumor response by magnetic resonance imaging or computed tomography scan was investigator assessed using RECIST v1.0 at screening, at day 64 (±4 days), and every eight weeks thereafter until documented progressive disease per RECIST or initiation of subsequent anticancer therapy. Response was confirmed by repeat imaging at least four weeks after the initial assessment. For the analysis of overall survival (OS) and PFS from the first cabozantinib dose, the Kaplan–Meier method was employed to estimate medians.
Results
Patients
Fifteen DTC patients from two U.S. centers were enrolled from December 6, 2010, to July 1, 2011 (Table 1): seven patients (47%) with papillary thyroid cancer, five patients (33%) with follicular thyroid carcinoma, and three patients (20%) with Hürthle cell carcinoma. Patients had received a median of one prior systemic agent (range 0–6) excluding RAI, and most patients had previously received at least one VEGF pathway inhibiting therapy (11 patients; 73%). All patients were refractory to or had progressed following standard therapy with RAI, and had progressed during or after their most recent systemic therapy prior to study entry.
Excludes radioactive iodine.
ECOG PS, Eastern Cooperative Oncology Group performance status; VEGF, vascular endothelial growth factor.
Safety
All patients experienced at least one treatment-emergent AE (irrespective of causality), with 13 experiencing at least one AE that was grade 3 or higher (Table 2). Diarrhea (20%) and hypertension (13%) were frequently reported grade 3 AEs. Other nonlaboratory grade 3 AEs included decreased appetite (13%), weight decreased (13%), fatigue (7%), and vomiting (7%). Two nonlaboratory grade 4 events were reported (myocardial infarction and aspiration pneumonia).
Medical Dictionary for Regulatory Activities v14.1 preferred terms (converted to American English spelling), Common Terminology Criteria for Adverse Events v3.0 grading; n=number of patients with event.
Groupings of preferred terms related to a particular medical condition.
One grade 5 event (related to study treatment): Hemoptysis due to aortotracheal fistula.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CPK, creatine phosphokinase; LDH, lactate dehydrogenase; PPE, palmar-plantar erythrodysethesia.
One treatment-related death occurred in a patient with a prior history of surgical resection of a mediastinal node, followed by external beam radiation to the mediastinum and antiangiogenic therapy, who developed a tracheoesophageal fistula while on study treatment. The complication was identified due to aspiration pneumonia, and the patient was treated with a stent. The patient died due to hemoptysis 27 days after discontinuing study treatment, and autopsy revealed an aortotracheal fistula as the cause of death. No tumor was found at the fistula site, and no residual tumor remained at this site prior to treatment with cabozantinib.
Fourteen patients had at least one dose interruption leading to a dose reduction to manage AEs; three patients reduced one dose level to 100 mg, and 11 patients reduced two dose levels to 60 mg. The median time to first dose reduction was 15 days (range 3–170 days). The median average daily dose was 62 mg cabozantinib (range 41–139 mg), and the median percentage of the planned dose received was 45% (range 29.4–99.6%).
Efficacy
Eight patients (53% [CI 27–79%]) had a partial response (PR), and six (40%) had stable disease (SD) as their best response, four of whom had SD for six months or more (Fig. 1A). Five PRs occurred in patients with papillary thyroid cancer, and three occurred in patients with follicular thyroid carcinoma. Of the 11 patients pretreated with a VEGF pathway inhibitor, five had a confirmed PR—four of whom had prior sorafenib therapy. Of the three evaluable patients who had not received prior therapy with a VEGF pathway inhibitor, all three had a confirmed PR—two of these responders had no prior systemic therapies beyond standard treatment with RAI. All eight patients with a PR achieved their response after they had the dose reduced to either 100 mg or 60 mg cabozantinib, and maintained their responses with these lower doses.

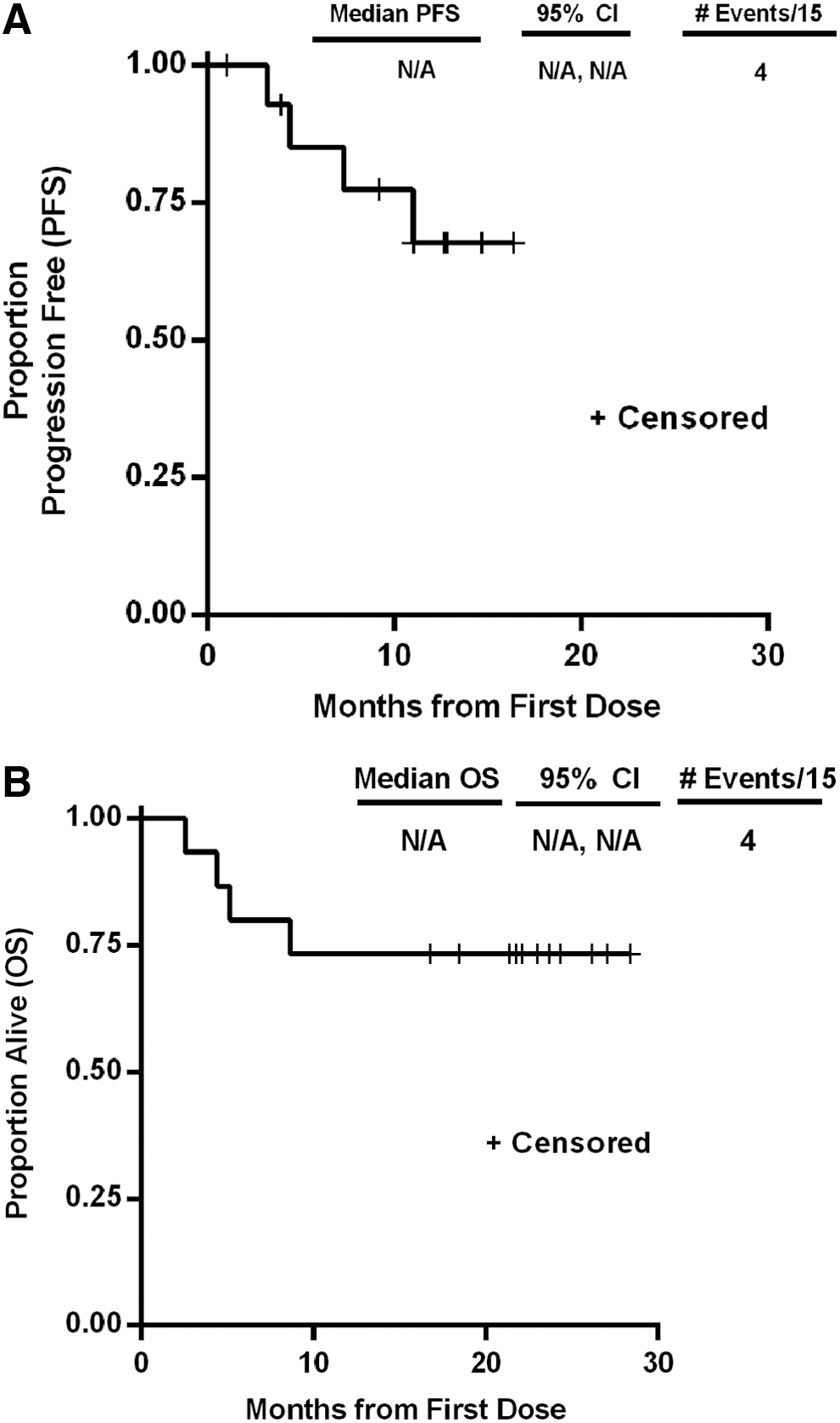
Duration of response ranged from 2.0 to 14.5 months or more; the median duration of response was not reached prior to termination of the trial. All 14 evaluable patients had tumor regression (Fig. 1A), including a patient with RAI-refractory metastatic follicular thyroid cancer pretreated with sorafenib who had a confirmed PR (Fig. 1B). One patient with Hürthle cell carcinoma discontinued treatment prior to the first on-study radiographic assessment and was not evaluable for response. Of nine patients with bone metastases at baseline, three had a PR and five had SD as their best response in measureable (i.e., visceral and/or soft tissue) target lesions per RECIST. One heavily pretreated patient (seven prior systemic therapies) showed substantial regression of a parietal skull osteoblastic tumor at eight weeks on study, with a corresponding 91% decrease in thyroglobulin (Fig. 1C). Median PFS (Fig. 2A) was not reached with a median follow-up of 12.2 months (range 10.3–17.0 months). Median OS (Fig. 2B) was not reached with a median follow-up of 25.8 months (range 23.9–30.7 months).
Discussion
Anticancer therapies targeting the VEGF signaling pathway have been extensively evaluated in patients with DTC, and these therapies now play an important role in the treatment of many of these patients. Sorafenib is currently the only approved agent for first-line treatment of DTC patients with RAI-refractory disease (11). However, patients eventually experience disease progression, and various other VEGF pathway-targeted agents have been investigated as salvage treatment for patients who progress on sorafenib (16). Compelling evidence for a role for MET and RET in the disease pathophysiology and/or in the development of resistance to therapies targeting the VEGF signaling pathway makes cabozantinib an attractive candidate for evaluation in patients with DTC. Therefore, we utilized a planned drug–drug interaction study of cabozantinib in cancer patients as an opportunity for such an assessment.
In this study, treatment with cabozantinib was generally well tolerated with a safety profile similar to that seen with other VEGFR TKIs in DTC patients (11,17). The most common nonlaboratory AEs regardless of causality were diarrhea, decreased appetite, fatigue, nausea, and weight decreased. Hypertension, which is the most common cardiovascular AE reported for antiangiogenic drugs, occurred in 53% of patients, which is comparable to the rates reported for other agents targeting the VEGF signaling pathway (11,17 –19). Larger trials of cabozantinib in castration-resistant prostate cancer and medullary thyroid cancer had similar rates and types of AEs (3,4).
One grade 5 adverse event related to study treatment (hemoptysis due to an aortotracheal fistula) was observed in this study and has been described in detail elsewhere (20). Such life-threatening AEs (including fistula development, gastrointestinal perforations, and hemorrhage) have previously been observed with VEGF pathway inhibition (20,21) as well as in a phase III trial of cabozantinib in patients with medullary thyroid cancer (4). Caution is required when treating patients who are at risk for such events.
Cabozantinib demonstrated clinical activity in heavily pretreated DTC patients, with a response rate of 53%. The median PFS and median OS were not reached, despite a median follow-up of 12 months for PFS and 26 months for OS. Other antiangiogenic TKIs have also shown activity in DTC. Sorafenib, an inhibitor of VEGFR2, PDGFR, BRAF, RET, and KIT, showed a response rate of 12% and a PFS of 10.8 months in a phase III study in the first-line setting (11), and a response rate of 21% in a meta-analysis of 159 DTC patients in seven phase II trials (22). Motesanib, an inhibitor of VEGF receptors, PDGFR, and KIT, demonstrated a response rate of 14% and a median PFS of 40 weeks in DTC patients who were primarily receiving first-line therapy and were not previously treated with a VEGFR TKI (17). Lenvatinib, an inhibitor of VEGFR1-3, FGFR1-4, RET, KIT, and PDGFR-β, demonstrated a response rate of 54% and a median PFS of 14.4 months in DTC patients who were not previously treated with a VEGFR TKI, and a response rate of 41% and a median PFS of 11.4 months in patients who were previously treated with a VEGFR TKI (23). Pazopanib, an inhibitor of VEGFR1-3, PDGFR-β and -α, KIT, and other kinases, demonstrated a response rate of 49% and a median PFS of 11.7 months in a phase II study of 37 DTC patients, the majority of whom (73%) were pretreated only with RAI and TSH suppression (24). Thus, the tumor response and PFS results with cabozantinib are noteworthy, particularly given that this study enrolled a heavily pretreated patient population (including 10 patients who received prior sorafenib).
Bone metastases are a frequent complication for DTC patients (25), but are often resistant to antiangiogenic treatment (26,27). Both the MET and VEGF signaling pathways appear to be important for regulating the function of osteoblasts and osteoclasts, which are two key cell types in the bone microenvironment that are involved in the development of metastatic bone lesions (28). In nonclinical studies, cabozantinib blocked progression of both osteoblastic and osteolytic lesions in prostate cancer xenografts in bone (29 –31). In this study, activity of cabozantinib on existing bone lesions was observed. These observations are consistent with the bone scan resolution previously reported with cabozantinib in castration-resistant prostate cancer and metastatic breast cancer patients in phase I and phase II studies (3,32 –34). Based upon these results, the effects of cabozantinib on bone metastases are being prospectively assessed in DTC patients in a recently initiated phase II trial (NCT01811212).
The initial daily dose of cabozantinib in this study of 140 mg was selected to support the drug-drug interaction trial endpoint based on the MTD in the initial phase I study (2). However, the majority of patients had a dose reduction following a dose interruption to manage tolerability, with the first reduction occurring no more than 170 days after initiation of study treatment. The majority of patients underwent a dose reduction to 60 mg. Despite this reduced dose, clinical activity was maintained with median duration of response and median PFS not reached despite a median follow-up of 12 months. These results are consistent with data from other studies that have also shown long-term tolerability and marked activity associated with lower doses of cabozantinib (32,34,35), and 60 mg daily has been selected as the starting dose in many ongoing or future trials of cabozantinib.
In conclusion, the safety profile and antitumor activity observed with cabozantinib in heavily pretreated DTC patients, most of whom had received prior therapies targeting the VEGF signaling pathway, warrant further investigation in this tumor type. Accordingly, phase II studies of the efficacy and safety of cabozantinib in DTC patients are ongoing (NCT01811212 and NCT02041260).
Footnotes
Acknowledgments
We thank the study medical monitor David Ramies (Exelixis, Inc.); Frauke Schimmoller, Colin Hessel, Jeffrey Zhang, and Yihua Lee (Exelixis, Inc.) who assisted greatly in data management and analysis; Dana Aftab and Gisela Schwab (Exelixis, Inc.) for their critical review of the manuscript; and Becky Norquist for medical writing support for the manuscript. Supported by the NIH/NCI under award number P30CA016672.
Author Disclosure Statement
M.E.C., M.S.B., and S.I.S. have received consultancy fees from Exelixis, Inc. J.H. and K.C.F. are full-time employees of Exelixis, Inc. M.S.B. has received speaker honoraria from Exelixis, Inc.