
Abstract
Background:
Although fine-needle aspiration (FNA) is a safe and accurate diagnostic procedure for assessing thyroid nodules, it has limitations in diagnosing follicular neoplasms due to its relatively high false-positive rate. The purpose of the present study was to evaluate the diagnostic role of core-needle biopsy (CNB) for thyroid nodules with follicular neoplasm (FN) in comparison with FNA.
Methods:
A series of 107 patients (24 men, 83 women; mean age, 47.4 years) from 231 FNAs and 107 patients (29 men, 78 women; mean age, 46.3 years) from 186 CNBs with FN readings, all of whom underwent surgery, from October 2008 to December 2013 were retrospectively analyzed. The false-positive rate, unnecessary surgery rate, and malignancy rate for the FNA and CNB patients according to the final diagnosis following surgery were evaluated.
Results:
The CNB showed a significantly lower false-positive and unnecessary surgery rate than the FNA (4.7% versus 30.8%, 3.7% versus 26.2%, p<0.001, respectively). In the FNA group, 33 patients (30.8%) had non-neoplasms, including nodular hyperplasia (n=32) and chronic lymphocytic thyroiditis (n=1). In the CNB group, 5 patients (4.7%) had non-neoplasms, all of which were nodular hyperplasia. Moreover, the CNB group showed a significantly higher malignancy rate than FNA (57.9% versus 28%, p<0.001).
Conclusions:
CNB showed a significantly lower false-positive rate and a higher malignancy rate than FNA in diagnosing FN. Therefore, CNB could minimize unnecessary surgery and provide diagnostic confidence when managing patients with FN to perform surgery.
Introduction
U
Our study was performed to compare the false-positive, unnecessary surgery, and malignancy rates for patients with thyroid nodules with FN on FNA and CNB, and for which a final diagnosis was made following surgery.
Materials and Methods
Patients
This retrospective study was approved by the Institutional Review Board of our hospital, and patient informed consent was waived. However, informed consent was obtained from all patients prior to undergo FNA or CNB procedures. From October 2008 to December 2013, 5481 US-guided CNBs were performed at our institution, among which 186 consecutive biopsy results (3.3%) showed FN readings. Among them, 107 patients had a surgically obtained final diagnosis (Fig. 1). We consecutively selected 231 patients who had undergone US-guided FNAs during the same time period and who had been diagnosed with FN readings using US-guided FNA. Among these patients, 107 had a surgically obtained final diagnosis. Among our total patient cohort, 13 cases were simultaneously included in the FNA and CNB groups.
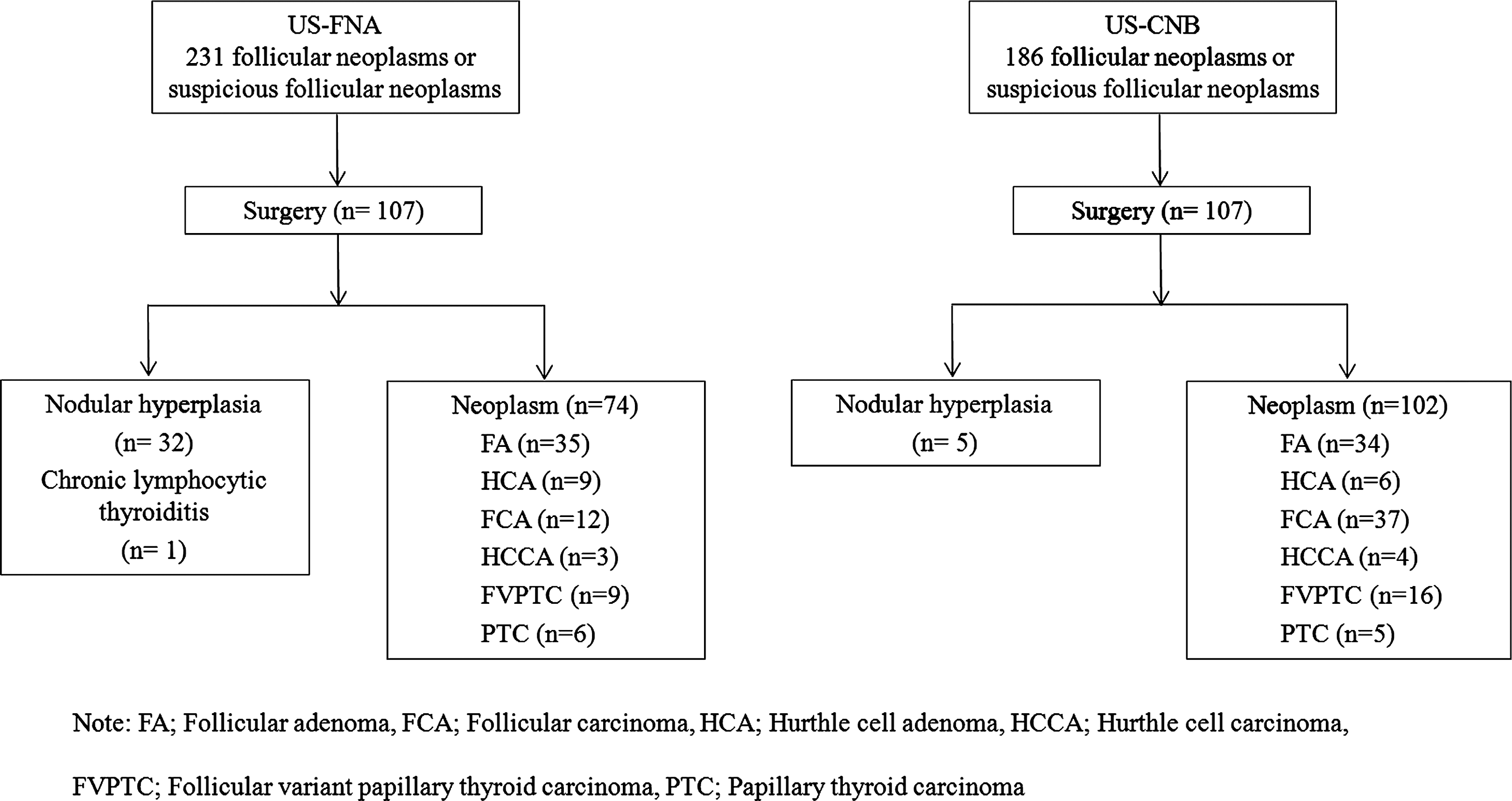
Flowchart of the study population and final diagnoses in the study groups.
US-guided FNA and CNB procedures
All US examinations were performed using one of three systems: an HDI-5000 (Philips Healthcare, Bothell, WA) equipped with a linear high-frequency probe (5–14 MHz), an iU22 unit (Philips Healthcare) or an EUB-7500 (Hitachi Medical System, Tokyo, Japan). US examinations were performed to determine the size (largest diameter), location, composition, and vascularity of the thyroid nodules. FNA and CNB procedures were performed by two clinically experienced thyroid radiologists (J.H.B. and J.H.L.) or by residents and fellows under their supervision. For FNA, a combination of 21- and 23-gauge needles with a combination of aspiration and capillary techniques were used according to the characteristics of the nodules (12). All cases were examined using direct smears, which were immediately fixed with alcohol after FNA and stained with Papanicolaou. The number of needle passes was determined by the operator during the FNA procedure, and a maximum of five passes were permitted for each nodule.
For CNB, the biopsy procedures were performed by the same radiologists using a 1.1- or 1.6-cm excursion, 18-gauge, double-action, spring-activated needle (TSK Ace-cut; Create Medic, Yokohama, Japan) (9,10,13). Before the CNB procedure, we measured the size of the nodule and used power Doppler US to evaluate the vessels along the approach route in order to avoid hemorrhage. After induction of local anesthesia with 1% lidocaine at the puncture site, the core-needle was advanced into the solid part of a nodule using a free-hand technique (14) (Fig. 2). After the core needle had been advanced through the edge of the nodule, we reevaluated the vessels to minimize vessel injury. After measuring the distance of fire (1.1 or 1.6 cm), the stylet and cutting cannula of the needle were sequentially fired. Tissue cores were placed in 10% buffered formalin immediately after the procedure and then conventionally processed (10). The adequacy of the procedure was assessed using real-time US imaging, and the adequacy of the specimens was assessed visually. To be adequate, all negative smears had to contain at least 6 groups of epithelial cells with 10 cells per group for FNA and any identifiable thyroid tissue for CNB (9,10).

Ultrasound images of a 57-year-old woman showing a 2.6-cm hypoechoic nodule with a peripheral hypoechoic rim in the left lobe of the thyroid gland. An 18-gauge core needle was advanced into the edge of the nodule
Additional FNA or CNB procedures were performed when a lesion was considered inaccurately targeted in the case of small nodules or when an insufficient specimen was suspected by visual inspection (10). After the biopsy, each patient was observed while using firm, local compression of the biopsy site for 10–20 minutes. When a patient complained of pain or swelling of their neck, a repeat US examination was performed to evaluate these complications (10).
Cytology and histology analysis
FNA cytology and CNB histology specimens were reviewed by experienced pathologists. FNA cytology diagnoses were categorized into six categories according to the Bethesda System for Reporting Thyroid Cytopathology (15) (i.e., nondiagnostic, benign, AUS/FLUS, FN/SFN, suspicious for malignancy, and malignancy). As our hospital has used the Bethesda System for FNA cytology diagnoses since 2012, we have replaced all cytology readings made prior to 2012. As the diagnostic criteria of CNB have not yet been standardized for thyroid nodules, CNB histology diagnoses were categorized into the same six Bethesda System categories in accordance with the CNB histopathology results (9,10). The FN readings obtained from FNA and CNB procedures included nodules with histology features favoring follicular neoplasm (16).
Statistical analysis
Statistical analysis was performed using statistical software (SPSS, version 11.0; SPSS, Chicago, IL). The χ2 test and the unpaired Student's t test were used to compare demographic data between the FNA and CNB group (i.e., age, sex, mean nodule size, mean number of biopsies). The χ2 test or the Fisher's exact test was used to compare the false-positive rate (i.e., positive predictive value and unnecessary surgery rate in the FNA and CNB groups) in accordance with the final diagnosis. The false-positive rate was defined as the final diagnosis of non-neoplasms, including nodular hyperplasia or thyroiditis. The true-positive rate was defined as the final diagnosis of a neoplasm (other than nodular hyperplasia or thyroiditis). The unnecessary surgery rate was calculated based on the false-positive rate, after excluding patients for whom surgery was inevitable, such as cases with a coexisting, known papillary thyroid carcinoma or a cosmetic problem caused by the large size of a thyroid nodule. The χ2 test or Fisher's exact test was also used to compare the malignancy rates between the FNA and CNB groups. A p value <0.05 was considered statistically significant.
Results
Demographic characteristics
The demographic characteristics are summarized in Table 1. In the FNA group, there were 24 men (mean age, 52.8 years; age range, 31–72 years) and 83 women (mean age, 45.9 years; age range, 19–70 years). In the CNB group, there were 29 men (mean age, 51.2 years; age range, 13–83 years) and 78 women (mean age, 44.5 years; age range, 16–74 years). There was no significant difference in age or sex between the two groups. The mean nodule size was 2.2 cm (range, 0.4–19.6 cm) in the FNA group and 2.9 cm (range, 0.6–13 cm) in the CNB group, which showed a significant difference (p<0.001). There were 9 nodules of less than 1 cm in the FNA group and 5 nodules in CNB group. The mean number of biopsies was significantly greater in the FNA group than in the CNB group (p=0.016). In all patients, CNB procedures were tolerable and were fully completed without immediate complications. There was no evidence of major complications resulting in hospitalization, such as hematoma, infection, or pain after CNB.
A p value of <0.05 was considered statistically significant.
FNA, fine-needle aspiration; CNB, core-needle biopsy.
Final diagnosis of FNA and CNB with FN reading
Among the patients with FN readings, 52.7% (107/231) in the FNA group and 57.5% (107/180) in the CNB group underwent surgery. The number and proportion of the final diagnosis after surgery in the FNA and CNB groups are listed in Table 2. The false-positive, unnecessary surgery, and malignancy rates in each group are shown in Table 3. CNB showed a significantly lower false-positive rate than FNA (4.7% versus 30.8%, p<0.001). In the FNA group, 33 patients (30.8%) had non-neoplasms, including nodular hyperplasia (n=32) and chronic lymphocytic thyroiditis (n=1). In the CNB group, 5 patients (4.7%) had non-neoplasms, all of which were nodular hyperplasia. Among the total patients with FN readings, 4 had coexisting, known papillary thyroid carcinoma in the FNA group, and 1 patient in the FNA group and 1 patient in the CNB group had cosmetic problems due to the large size of their nodule. Other than these patients, the CNB group showed a significantly lower unnecessary surgery rate than the FNA group (3.7% versus 26.2%, p<0.001).
A p value of <0.05 was considered statistically significant.
FNA, fine-needle aspiration; CNB, core-needle biopsy; FVPTC, follicular variant papillary thyroid carcinoma; PTC, papillary thyroid carcinoma.
A p value of <0.05 was considered statistically significant.
FNA, fine-needle aspiration; CNB, core-needle biopsy.
In our total cohort, the patients who underwent CNB showed a significantly higher malignancy rate than the FNA group (57.9% versus 28%, p<0.001). In the neoplasm group, the patients who underwent CNB also showed a significantly higher malignancy rate than the FNA group (60.8% versus 40.5%, p<0.001). A summary of the false-positive and malignancy rates of the FNA and CNB groups in our present study and in recently published reports is presented in Table 4.
A p value of <0.05 was considered statistically significant.
FNA, fine-needle aspiration; CNB, core-needle biopsy.
Discussion
Our present study findings demonstrate that the CNB procedure has significantly lower false-positive and unnecessary surgery rates in diagnosing FN compared with FNA. Moreover, the malignancy rate was significantly higher in the CNB group compared with the FNA group. According to our large population study, we could thus suggest that CNB is a better diagnostic tool for FN.
Regarding the false-positive rate of FNA in diagnosing FN, it has been reported to range from 22.2% to 35% (2 –4). Our study showed a similar false-positive rate in the FNA group (30.8%) to that seen in previous studies. In contrast, the false-positive rate of CNB is reported to be 0–18.2% after surgery (11,12) and our current result of 4.7% is in this range. Hence, with regard to the false-positive rate, CNB seems to be superior to FNA in diagnosing FN. More notable is that the unnecessary surgery rate was significantly lower in the CNB than in FNA group. This result also supports the positive value of CNB.
Regarding the malignancy rate, the proportion of thyroid nodules classified as FN by FNA ranged from 19.4% to 31% in previous studies (3,17,18). The malignancy rate of FNA in our present study (28%) is consistent with previous reports, while CNB showed a higher malignancy rate (57.9%) than that reported in an earlier study (45.5%) (12). The cause of the lower malignancy rate in the FNA group might be due to the high false-positive rate of this procedure for FN. Accordingly, for thyroid nodules with FN as determined by CNB, surgery seems to be a reasonable next step.
Recently, the value of CNB for diagnosing thyroid nodules has also been suggested by Ha et al. (14) who have reported that CNB is clinically useful in managing thyroid nodules with suspicious US features after initially benign FNA results. In addition, other studies have concluded that CNB demonstrates high rates of conclusive and accurate diagnoses in patients previously categorized as nondiagnostic or AUS/FLUS by FNA (9 –11,19). Nasrollah et al. (11) have suggested a new CNB technique that can sample the nodular tissue, extranodular parenchyma, and the nodule's capsule. Using this method on 20 patients diagnosed with FN, it produced no false-negative or false-positive results. However, there are only a limited number of studies that include final surgical results when validating FNA and CNB for diagnosing FN. The results of our large population study validate the usefulness of CNB for diagnosing FN compared with FNA, which thus reinforces the role of CNB.
There is some controversy regarding the clinical significance of thyroid nodules with FN using FNA. For cytologically suspected FN, surgery is recommended as the only way to distinguish malignant from benign nodules by detecting the presence of vascular and/or capsular invasion (20). Although the ultimate purpose of surgery for FN is to distinguish follicular carcinomas from adenomas (4), patients who undergo surgical treatment because of a diagnosis of FN on FNA are quite possibly undergoing unnecessary surgery due to the its high false-positive and low malignancy rate. Considering our current results and those of previously published reports, a further histologic validation by CNB may improve the diagnostic confidence in thyroid nodules with FN on FNA, and thus prevent unnecessary surgery.
In terms of pathology, there have been several debates regarding the usefulness of FNA, especially for diagnosing FN. FNA might fail to diagnose FN in the presence of mixed micro- and macrofollicular proliferation or macrofollicular proliferation only. In addition, the major difference between adenomatous nodules (which lack a well-defined, complete, fibrous capsule) and FN (which manifests as a completely encapsulated lesion) cannot be evaluated by cytology alone. In these cases, a diagnostic lobectomy is mandatory (11,21). However, CNB is advantageous for assessing atypical nuclear changes, architectural alterations in follicular structures and borders, in addition to adjacent normal tissue, because CNB can obtain tissue cores containing the nodular margin, tumor capsule and, adjacent normal tissue in nodules that are suspicious for FN (16,22 –24) (Figs. 2 and 3). Hence, if nodular parenchyma, extranodular tissue, and the fibrous capsule of a nodule are present in CNB specimens, pathologists can more readily obtain an accurate diagnosis of FN, regardless of the presence of a primarily macrofollicular growth pattern. Therefore, based on the results of previous studies and our present findings, FNA has a fundamental limitation in differentiating FN and CNB can provide more accurate diagnostic information in this regard. For this reason, our current study contributes to our understanding of the usefulness of CNB and to the best strategies for managing thyroid nodules with FN.

Core-needle biopsy (CNB) histology and surgical pathology of a thyroid nodule confirmed as follicular adenoma.
Our study has several limitations to note. First, its retrospective design may have caused a selection bias. As our hospital has used the Bethesda System for FNA cytology diagnoses since 2012, we have replaced all cytology readings made prior to 2012 using this system instead of reclassifying these findings via a review of FNA cytology slides by a pathologist. Hence, the prevalence of nodules with an FN reading might have been underestimated. Although our current study findings demonstrate that CNB produces fewer false-positive results than FNA when assessing FN, further investigations are needed to validate the diagnostic performance of CNB. Second, the lack of a standardized diagnostic category for the histologic diagnosis of FN on CNB may have influenced our results. Finally, the involvement of multiple operators for both the FNA and CNB procedures can be the source of a further bias in terms of our current study findings. However, all of the operators on our present patient series performed FNA or CNB under the supervision of two experienced operators.
In conclusion, our study demonstrates that CNB shows a significantly lower false-positive rate and a higher malignancy rate than FNA in diagnosing FN. Therefore, CNB could minimize unnecessary surgery and provide diagnostic confidence when managing patients with FN to perform surgery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.