
Abstract
Introduction:
Autoimmune thyroiditis (AIT) is a common cause of goiter in children, and sonographic changes have been reported in more than one-third at presentation. The aim of this study was to evaluate the ultrasound (US) characteristics of the thyroid and the prevalence of thyroid nodules in children and adolescents presenting with goiter in the presence or absence of AIT.
Methods:
A retrospective review was conducted of the US characteristics of 154 children and adolescents aged <18 years of age with goiter from July 2008 to December 2010. US characteristics were analyzed according to each patient's age, sex, thyrotropin (TSH) levels, and thyroid peroxidase antibody titer (TPOAb). Heterogeneity and nodule prevalence were compared between antibody-positive and -negative goiter.
Results:
Heterogeneity was more common in TPOAb-positive (59/71, 83%) compared to TPOAb-negative goiter (24/46, 52%; p<0.001), but there was no correlation between the presence of heterogeneity and TPOAb titer within the antibody-positive group. Nodules were equally prevalent in children with (17%) and without (17.4%) TPOAb, and there was no correlation between the serum TSH level or TPOAb titer and the presence of nodules. Papillary thyroid cancer (PTC) was diagnosed in 3/71 with positive TPOAb compared to 1/46 with negative antibodies. Pseudonodules were identified in 11/71 antibody-positive and none of the antibody-negative patients. However, during follow-up, two of these were later identified as nodules and one was PTC.
Conclusion:
The majority of children and adolescents with goiter had positive TPOAb (71/117). Sonographic heterogeneity was more common among TPOAb-positive patients. However, thyroid nodules and PTC were equally common in both groups. Only 15% of the nodules and none of the PTC were palpable. These data support the utility of thyroid US to detect unsuspected thyroid nodules and PTC in children with goiter. Prospective follow-up studies of children with goiter are needed to formulate recommendations for evaluation with US and fine-needle aspiration.
Introduction
T
AIT is a frequent cause of goiter and the most common thyroid disorder in children and adolescents in iodine-replete populations such as the United States (1,10). Thyroid dysfunction in AIT can range from euthyroid goiter to hypothyroidism and, less frequently, hyperthyroidism. The prevalence of AIT increases with age, is more common in females, and varies with iodine status and the criteria used for diagnosis (11). Based on the National Health and Nutrition Examination Survey (NHANES III), antithyroid peroxidase antibodies (TPOAb) are detected in 4.8% of people in the United States, and are significantly associated with thyroid dysfunction. They are therefore commonly used as a surrogate marker of AIT (12). In contrast, antithyroglobulin antibodies are not associated with thyroid dysfunction (12).
US has been increasingly utilized for evaluation of the thyroid structure. It is a useful adjunct to clinical exam to evaluate thyroid size and anatomy and to detect nodules. Diffuse reduction in echogenicity (hypoechoic) or the presence of micronodules are commonly described findings in AIT and are thought to be valid predictors of AIT (13 –15). In adult patients with AIT, US has also been shown to be helpful in identifying patients who are at risk for developing hypothyroidism (16). Pediatric patients with abnormal US findings were found to have higher thyrotropin (TSH) values (17), suggesting that US might also be useful as a noninvasive tool to screen for thyroid dysfunction in children. US is also more sensitive than clinical exam to detect nodules (18,19).
A 2008 study of Italian children with AIT reported thyroid nodules in up to one-third of the patients (6). Importantly, 10% of those nodules were malignant (6). However, Italy is a country with mild to moderate iodine deficiency (20). A 1997 study of European children reported that the median urine iodine excretion in Italy was <10 μg/dL, a threshold level that correlates with goiter formation (21). On the contrary, data from school-age children in the United States from the NHANES 2007–2008 survey showed that only 17% of children had urinary iodine levels <10 μg/dL (10), which according to World Health Organization (WHO) criteria, is classified as iodine insufficient (22). Therefore, the findings from the study in Italy may not be applicable to iodine-sufficient populations such as the United States. Given the paucity of data regarding the utility of neck US from the United States, this study was designed to evaluate ultrasonographic features and nodules in children and adolescents with goiter at the authors' institution.
Methods
The medical records of 221 children and adolescents aged <18 years who were diagnosed with goiter (diffuse thyromegaly (23)) from July 2008 to December 2010 at the Pediatric Endocrinology Clinic at the Children's Hospital of Richmond of Virginia Commonwealth University were retrospectively analyzed. This is a tertiary referral center for children throughout central Virginia. The study was approved by the Institutional Review Board at Virginia Commonwealth University. Children included in the study were referred either due to the presence of goiter or because they were found to have goiter during evaluation for hypothyroidism. Children with a history of radioactive iodine therapy or head and neck radiation were excluded. Although not prospectively excluded, there were no children with Down syndrome or Turner syndrome in this study.
Data collected included age, sex, thyroid medication use, presence of palpable nodule on examination, palpable lymph nodes, TPOAb status and titers, TSH levels, free thyroxine (fT4) levels, and US features of the thyroid gland. Serum TSH and fT4 levels were measured by direct chemiluminescence using Siemens Centaur kits. TPOAb measurement was done by enzyme immunoassay on the Siemens Immulite 2000 until June 2009 and then moved to Roche Elecsys E-170. Those with titers greater than the upper limit of the reference range (negative <35 IU/mL) were considered antibody positive. Neck US was requested at the discretion of the clinician evaluating the patient in those with a considerably enlarged, firm thyroid gland that was difficult to palpate on exam. US exams were performed by physicians trained in performing neck US in children, and all abnormal US findings were reviewed and confirmed by one of the study authors who was blinded to the initial findings (U.P.).
US characteristics were reported, including (a) thyroid volume, (b) echographic pattern, (c) presence of heterogeneity, (d) presence and size of nodules, (e) presence of pseudonodules and cysts, and (f) presence of abnormal cervical lymph nodes. The volume (V) of each thyroid lobe (in milliliters) was estimated by the modified formula of the rotation ellipsoid (V=0.479×d×w×l). The thyroid volume was defined as the sum of the volumes of both lobes, without including the isthmus (24). Areas of focal abnormality were further assessed for the presence of microcalcifications and cervical lymphadenopathy and by Doppler imaging to evaluate the blood-flow pattern. These additional features were also used to differentiate between true nodules and areas of heterogeneity. Follow-up US exams were performed as indicated on those with concerning findings on initial examination. US-guided fine needle aspiration (FNA) was performed in children who had a concerning nodule >1 cm.
Definitions
A nodule was defined as a distinct hypo-, hyper-, or isoechoic focal area within the thyroid gland noted on US, with vascularity different from the surrounding parenchyma. Lesions that had irregular margins were also classified as nodules if they were sonographically distinct from the surrounding parenchyma. A pseudonodule was defined as a poorly demarcated hypo- or hyperechoic focal area (25). A cyst was defined as an anechoic focal area with no solid component.
US characteristics, including presence of heterogeneity, nodules, and pseudonodules, were compared between antibody-positive and antibody-negative patients. In those who were positive TPOAb, the relationship between TSH levels, TPOAb titers, and the presence of heterogeneity and nodule were assessed. The number of patients who underwent FNA and subsequent surgery and who had a final histological diagnosis was also assessed.
Statistical analysis
Data are reported as mean±standard deviation (SD) for linear variables with normal distribution, median, and interquartile range (IQR) for non-normally distributed variables, and as proportions for categorical variables. TSH and TPOAb titer values were log-transformed due to non-normal distribution of data. Parametric and nonparametric tests were used for linear and categorical variables as applicable. Logistic regression analysis was performed to assess the relationship of log TSH levels and log TPOAb titer with the presence of nodule or heterogeneity of the gland. A p-value of <0.05 was considered significant. All data summaries and analyses were performed using JMP® statistical software v10.
Results
Clinical diagnosis of goiter was made in 221 children between July 2008 and December 2010. The mean age was 13.8±3.3 years (IQR 6.4–18), and the majority were female (85%). Thyroid US was performed in 154 of these children at the discretion of the treating clinician. Of these 154 patients, 71 were antibody positive, 46 antibody negative, and 37 patients did not have antibody status available. There were no differences in the mean age or sex between the groups (Table 1). There were significantly more patients on levothyroxine treatment in the antibody-positive group (37/71, 52%) compared to the antibody-negative group (16/46, 35%; p=0.0256). US characteristics of TPOAb-positive and -negative patients and those with antibody status not available are summarized in Table 2. Patients with positive TPOAb were more likely to have heterogenous US features (59/71, 83%) compared to those with negative TPOAb (24/46, 52%; p=0.0007). However, within the antibody-positive group, there was no correlation between the presence of heterogeneity with increasing TPOAb or TSH levels, as shown in Figure 1A and B. There were 20 (13%) nodules identified in the 154 patients with goiter who underwent US. The prevalence of thyroid nodules was similar in TPOAb-positive (12/71, 17%) and -negative children (8/46, 17%; p=0.61). Furthermore, within the TPOAb-positive group, there was no correlation between TSH levels or TPOAb titer and the presence of nodules, as shown in Figure 2A and B.

Relationship between presence of heterogeneity of the thyroid gland and log10 thyroid peroxidase antibody titer (TPOAb) titer
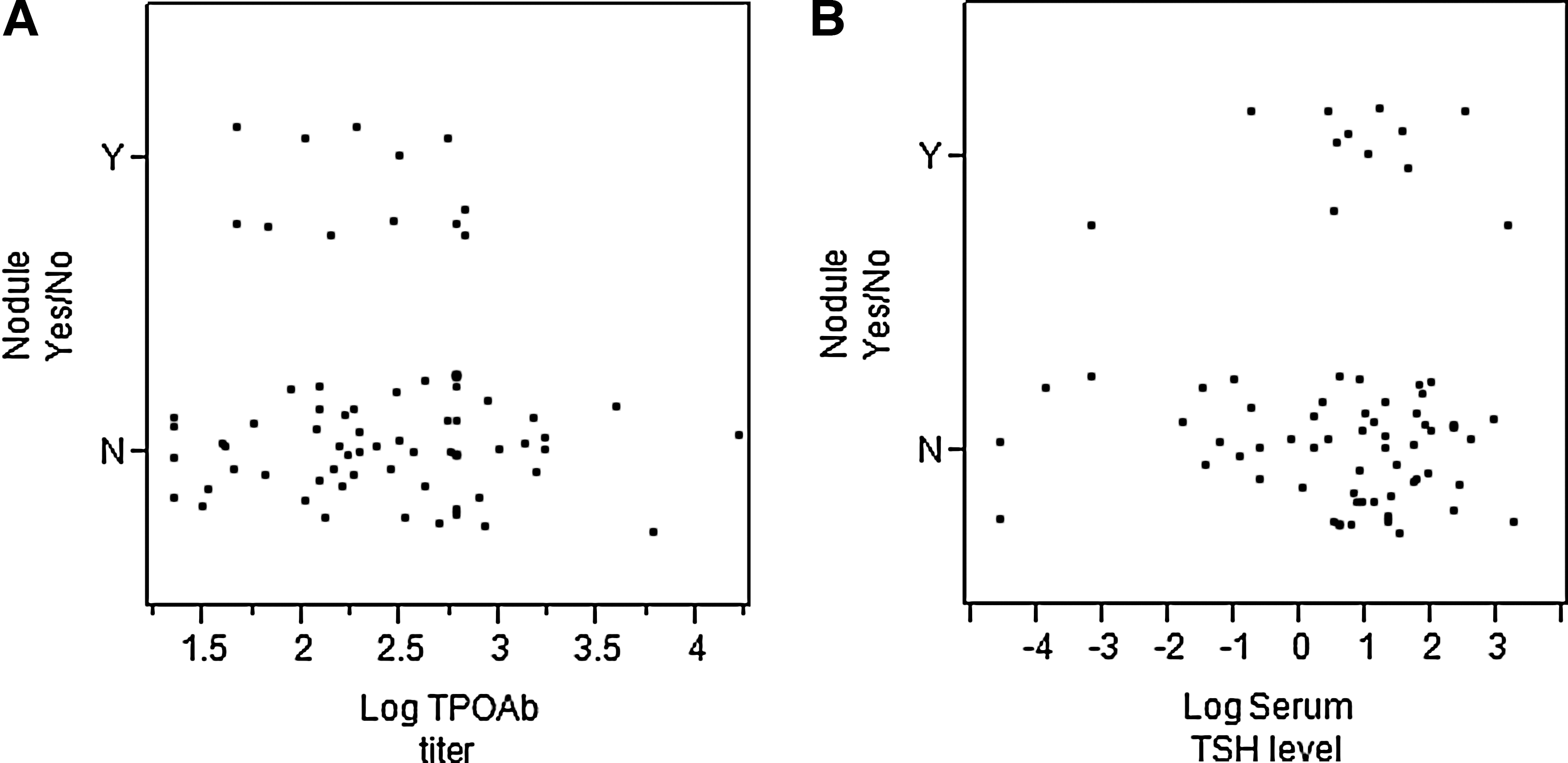
Relationship between presence of thyroid nodule with log10 TPOAb titer
Values are given as mean±standard deviation (SD).
Values within 2 months of the US study.
p-Value comparing TPOAb-positive and -negative groups.
TPOAb, thyroid peroxidase antibody; TSH, thyrotropin; fT4, free thyroxine.
Values are given as mean±SD.
p-Value comparing TPOAb positive and negative groups.
US, ultrasound.
Thyroid nodules were detected at a slightly younger age in children with positive antibodies (Mdn age=3.8 years, IQR 8.8–18 years) compared to those with negative antibodies, (Mdn age=17.3 years, IQR 9.9–18 years; p=0.06), as shown in Figure 3A and B. Nodule diameter was not significantly different between the two groups (0.3–4.8 cm in the antibody-positive and 0.3–3.7 cm in the antibody-negative group). In the antibody-positive group, there were five nodules <1 cm and seven nodules >1 cm. None of the five subcentimeter nodules had any other suspicious US features to warrant FNA as a part of clinical care. Therefore, cytological diagnosis was not available. Furthermore, at follow-up US, these five nodules did not increase in size or develop any suspicious US features. Five of the seven nodules >1 cm were further assessed by FNA, of which two were diagnosed as papillary thyroid cancer (PTC; Table 3) and confirmed on surgical pathology. Three were found to have a benign histology. The remaining two of the seven were lost to follow-up.
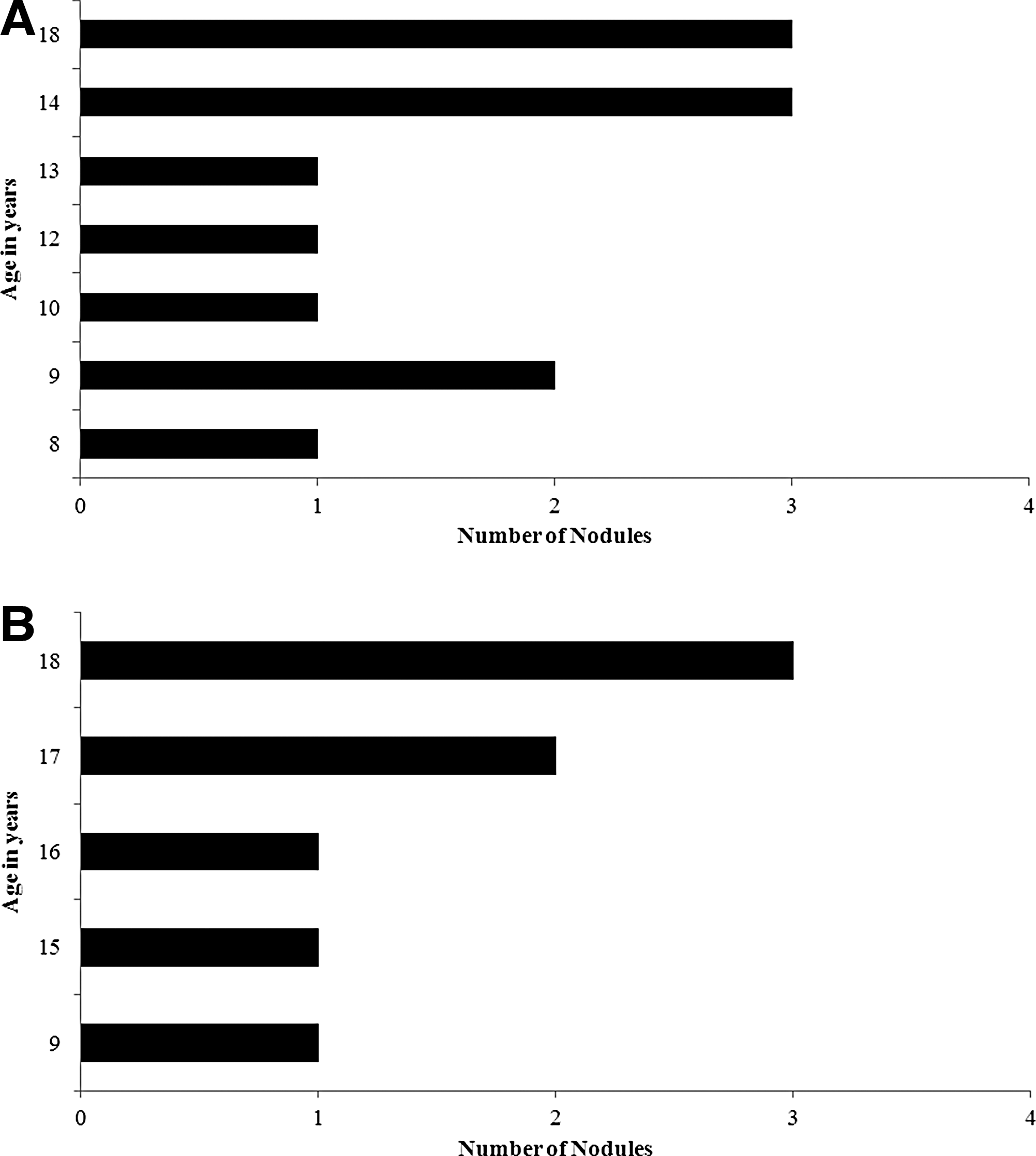
Distribution of number of nodules in each age group based on antibody status.
TNM, tumor–node–metastasis.
Four of the TPOAb-negative patients had nodules <1 cm with no suspicious US features. The remaining four nodules in the antibody-negative group were >1 cm, and FNA was performed in three. One was diagnosed as PTC (Table 3), two had a benign histology, and one was lost to follow-up. PTC was diagnosed in 3/71 (4%) with positive TPOAb compared to 1/46 (2%) with negative TPOAb (p=1.00). The overall incidence of PTC was not significantly different between the two groups. Of the total 20 nodules, only three (15%) were palpable on clinical exam, and none of the PTCs were palpable. Five of the 20 patients with nodules had multiple nodules, and none of these was malignant. All four PTC in this study presented as solitary nodules, and none of them had microcalcifications, but one had increased vascularity (Table 3).
Pseudonodules were identified in 11/71 (16%) antibody-positive patients, but none was found in antibody-negative patients (0/46, p=0.003). Importantly, on one-year follow-up US, two of the lesions initially thought to reflect pseudonodules were now identified as nodules >2 cm size, one of which was a PTC (Table 3).
Small cysts between 0.2 and 0.5 cm were identified in the two groups, with a similar prevalence in antibody-positive (7/71, 10%) and antibody-negative (4/46, 9%; p=1.00) patients. The group with antibody status unavailable had no nodules, but two of them had pseudonodules.
Discussion
Goiter is a common reason for referral of children and adolescents to pediatric endocrine centers, and US is a widely used diagnostic tool in patients with goiter. It is a useful adjunct to clinical exam in evaluating thyroid size and anatomy and detecting nodules. AIT is the most common cause of thyroid dysfunction in children and adolescents in iodine-sufficient populations (1). US changes and the interval between diagnosis and US abnormalities are variable in AIT in both children and adults (26,27). However, there is a paucity of data regarding US findings in children with goiter from the United States.
In this study, 20 of the 154 patients with goiter were found to have thyroid nodules by US. Eight of the 20 underwent FNA evaluation, resulting in the identification of four (20%) with PTC. None of these was detected by palpation prior to US, and only one had increased vascularity.
A previous study from Italy analyzed the relationship between AIT, thyroid nodules, and thyroid cancer in a large series of children and adolescents from six centers (6). Thyroid nodules were found in 115 of 365 patients with AIT (31.5%) of which only 38 nodules (one-third) were palpable by clinical examination. In contrast, the present study found a lower prevalence of thyroid nodules than the Italian study (6), but the prevalence of nodules in this study was similar in patients with TPOAb-positive goiter (17%) compared to patients with goiter and negative antibodies (17%). It was also found that heterogeneity of the thyroid gland was common in patients with TPOAb-positive goiter, as has been shown in adults with AIT (14).
One possible explanation for the difference in prevalence of thyroid nodules between the Italian study and the present study could be the difference in iodine intake. Italy is a country with mild to moderate iodine deficiency, while the United States is iodine sufficient (10,20). Iodine deficiency is a risk factor for thyroid nodule formation, but the relationship between iodine deficiency and AIT is not yet clear. Recent studies from Greece reported goiter in 28% and nodules in 14% of children with AIT and an increase in their prevalence after elimination of iodine deficiency (28,29). The differing study designs (different definitions of AIT and the difference in iodine intake) might have contributed to the differences in results, as would selection bias in all these studies, which were performed in tertiary care centers.
In contrast to all of these studies, a recent study from Japan (an iodine-sufficient region) found nodules detectable by US in only 1.6% of healthy children. The lower prevalence of nodules in this study is most likely explained by the cross-sectional evaluation of unselected school-age children with or without goiter (3).
Pseudo-nodular appearance due to fibrosis and scarring is seen in some AIT patients, making distinction from nodules rather difficult (25). In the present study, focal abnormalities were subclassified into nodules and pseudonodules based on the similar work of others (25) in efforts to identify which patients needed further evaluation. Pseudonodules were reported in 11/71 (16%) of antibody-positive patients with goiter in the current study. Of these, five did not have any change at follow-up, four did not have a follow-up US, and two were identified as nodules on follow-up US. One of these two nodules was ultimately found to be a PTC. Although these are small numbers, this is concerning and underscores the need for follow-up when any focal abnormality is identified on US. Newer techniques such as sono-elastography may help in differentiating nodules from pseudonodules, as shown in recent studies of adults (25).
No relationship was found between US characteristics (heterogeneity and presence of nodules) and thyroid function (as represented by TSH). Heterogeneity was more likely to be noted in patients with TPOAb-positive status versus those who were antibody negative. This is consistent with previous reports on AIT in adults (14). However, within the antibody-positive group, no significant correlation was detected between increasing TPOAb levels and the presence of heterogeneity on US. It is speculated that in the antibody-negative subgroup, patients who had heterogeneity may have AIT, since antibody levels are known to fluctuate over time and may become negative (30). Some of the antibody-negative goiter patients may have had an enlarged thyroid gland related to puberty (31).
Although thyroid nodules are less common in children, they are more likely to be malignant compared to adults (4,5). The prevalence of thyroid cancer in patients with AIT is not clear, with reports ranging from 1% to 30%, with most of these studies being of adults (32 –34). Thyroid cancer was diagnosed in a significant number of young patients, even in this study's small cohort (3/71, 4%, with positive antibodies compared to 1/46, 2% with negative antibodies), but none of these were palpable on physical exam. This is similar to the incidence of thyroid cancer in the Italian study (11 cases of PTC, 3%) (6). In the Italian study, lymphadenopathy and a progressive increase of nodule diameter on levothyroxine therapy were more common in patients with thyroid cancer compared to patients with a benign lesion. There were insufficient patients with PTC in the present study to examine these relationships, but there was one patient with a pseudonodule, which on subsequent examination was reclassified as a nodule and diagnosed as PTC. Despite the fact that none of these PTC were palpable, one PTC was >2 cm in diameter and two had microscopic spread to regional lymph nodes (N1) indicating a biological capacity to metastasize. This suggests that had they not been discovered, these two PTC might have spread further, resulting in more widespread regional and possible pulmonary metastases that would have required more extensive treatment. It is the authors' opinion that early discovery of these PTC was of clinical benefit to these few patients, as they did not require extensive surgery or radioactive iodine ablation. Caution is, however, urged in attempting to extrapolate these data to all children with goiter or AIT. First, the small number of patients in this study with PTC and the lack of long-term follow-up make it impossible to determine the impact of early identification of PTC on outcome. Second, had they not been detected by US, these PTC would likely have become clinically apparent, and it is possible that treatment at that later time would still have resulted in a favorable outcome. To the authors' knowledge, there are few published data that support the hypothesis that a delay in treatment has no impact on metastasis or recurrence risks. A retrospective review by Welch Dinauer et al. found no relationship between the time between first symptom to initial therapy and outcome, but the number of patients was also small, limiting the power of this observation (35). That study did find that recurrence risk was greater for larger and metastatic tumors. Large multicenter studies of the natural history of thyroid nodules in children will be required to determine if routine US examination is a cost-effective screening procedure for PTC in children and adolescents, and whether treatment of nonpalpable PTC will offer any benefit in terms of the extent of treatment and risk of recurrence for this age group.
The limitations of the study are the relatively small number of patients, the retrospective nature of the study design, possible ascertainment bias at a tertiary care center, and lack of data on the individual iodine excretion. In addition, interobserver variation in reading the US could have had an impact on the identified characteristics. This challenge is also integral to prospective studies, particularly when larger numbers of subjects are recruited at multiple centers involving several observers. Standardized reporting protocols in clinical practice might be helpful in minimizing these issues. Large prospective studies looking at US appearance in goiter, along with measurement of TPOAb, assessment of urinary iodine status, and thyroglobulin, and a standardized clinical description of goiter may be helpful in minimizing these issues.
Conclusion
The majority of children and adolescents with goiter had positive TPOAb (71/117). Sonographic heterogeneity was more common among TPOAb-positive patients. However, thyroid nodules and PTC were equally common in both groups. Only 15% of the nodules and none of the PTC were palpable. These data support the utility of thyroid US to detect unsuspected thyroid nodules and PTC in children with goiter. Prospective follow-up studies of children with goiter are needed to formulate recommendations for evaluation with US and FNA.
Footnotes
Acknowledgments
The opinions expressed here are solely of the authors and do not reflect the views of National Institutes of Health. NIH KL2TR000057 (AG).
Author Disclosure Statement
The authors declare that they have no competing interests.