
Abstract
The history of postpartum thyroid dysfunction (PPTD) dates back almost two millennia, when Soranus of Ephesus, who practiced obstetrics and neonatology, observed swelling in the necks (presumably goiters) of women after pregnancy. The next reference to PPTD appeared in artwork more than 1000 years later, with many portraits illustrating women with goiter while holding infants. In the early to mid-19th century, Caleb Hillier Parry and Armand Trousseau described postpartum hyperthyroidism, while in the late 1800s, Sir Horatio Bryan Donkin reported the first patient with postpartum hypothyroidism. The modern era of PPTD began with the description in the late 1940s by H.E.W. Roberton of women after delivery reporting hypothyroid symptoms and responding to thyroid extract. The immunologic influence on PPTD was recognized initially by Parker and Beierwaltes in the early 1960s, and the clinical variability and natural history were carefully documented by numerous investigators in the 1970s–1980s. The past two decades have seen further refinements in understanding the prevalence, etiology, and treatment of PPTD. Yet to be determined is the role of screening as a cost-effective measure.
Introduction
M
Methods
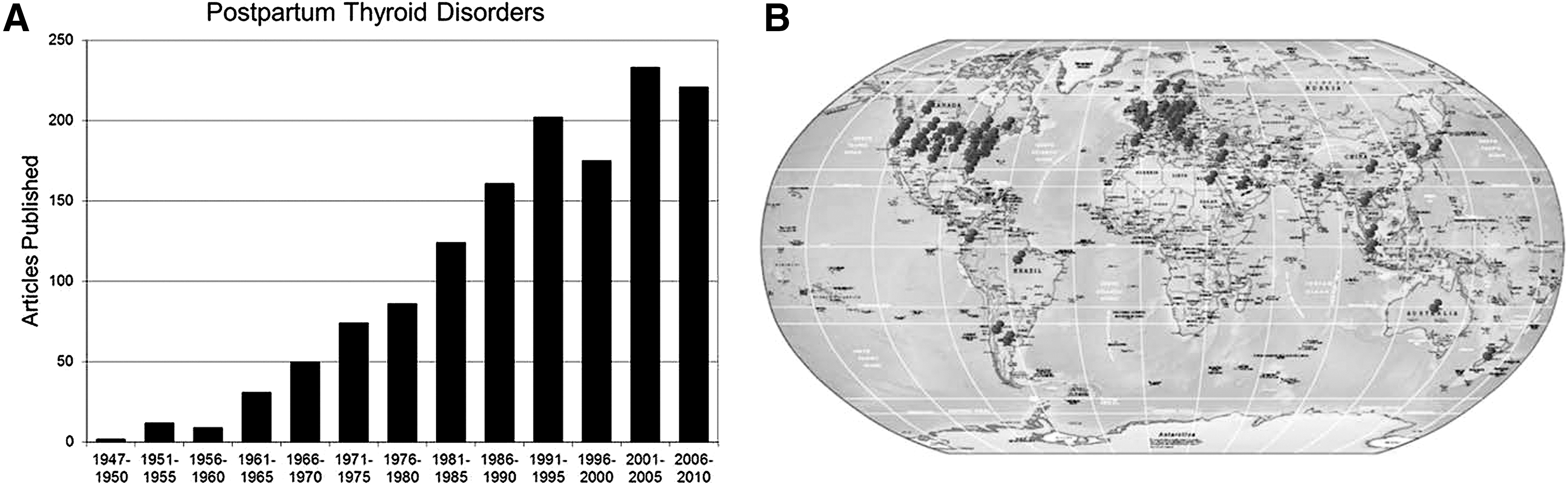
PubMed was searched using the keywords “postpartum thyroiditis” and “postpartum thyroid disorders.” The former identified 372 articles dating from 1971 to present, and the latter identified 1380 publications beginning in 1947 (Fig. 1A). From this modern literature, articles appeared from 38 countries and 30 states plus the District of Columbia within the United States, confirming the international recognition of the importance of this topic (Fig. 1B). The first written evidence of a possible connection between the thyroid and post pregnancy, however, appeared almost two millennia earlier. The results of this review were presented as the Clark T. Sawin Historical Vignette at the annual meeting of the ATA on September 21, 2012, in memory of Dr. Sawin (Fig. 2).
(
Clark T. Sawin, MD (1934–2004), reprinted with permission of Leslie Sawin.
PPTD Through the Ages
The beginning (ab initio c. 98–138 AD)
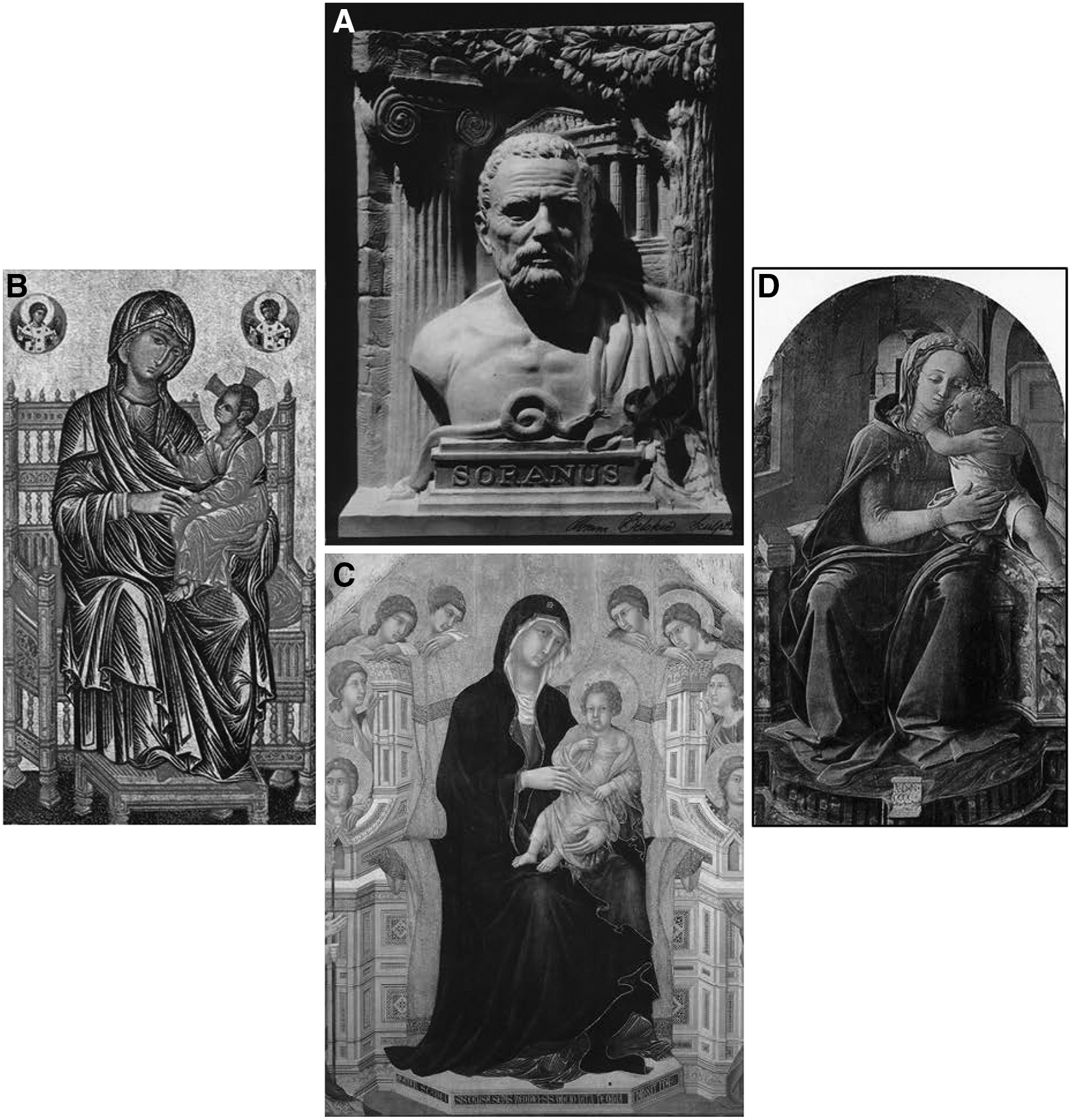
The story begins with Soranus (Fig. 3A), who was born in Ephesus (Asia Minor). He studied medicine in Alexandria, then practiced medicine in Rome. His career was devoted to the care of pregnant women and their babies, and his book Gynaecia, which elaborately described the management of disorders during pregnancy and the care of infants, was used by practitioners for hundreds of years (3,4). Noted medical contributions are that he used the vaginal speculum in his practice, and he wrote a biography of Hippocrates. His importance to the history of PPTD is that he “noted swelling of the neck after pregnancy,” which he thought to be a form of bronchial tumor (5), and was, most likely, a reference to goiter.
(
Late Byzantine/Early Renaissance (c. 1260–1473)
PPTD next appeared more than 1000 years later and was not depicted by the written word. Rather, this period could be referred to as the Visual Era of PPTD. There are many examples of paintings in galleries throughout the world that illustrate (usually as a religious work of Madonna and child) young women with goiters holding infants in their laps. Representative works include “Virgin and Child Enthroned with Angels in Medallions” in the National Gallery of Art, Washington, DC (artist unknown, c. 1260–1285; Fig. 3B); one by Duccio (1308), which resides in Siena Cathedral, Siena, Italy (Fig. 3C); “Virgin (with goiter) and Child” by van der Weyden (1399–1464) in the Prado, Madrid; a Madonna and child by Fra Filippo Lippi (1437) situated at the Palazzo Barberini, Rome (Fig. 3D); and Leonardo da Vinci's “Madonna and Child” (1473), Munich. Many of the models for these pictures may have had iodine deficiency goiter exacerbated by pregnancy, while others may have had underlying thyroid autoimmunity (6).
19th century
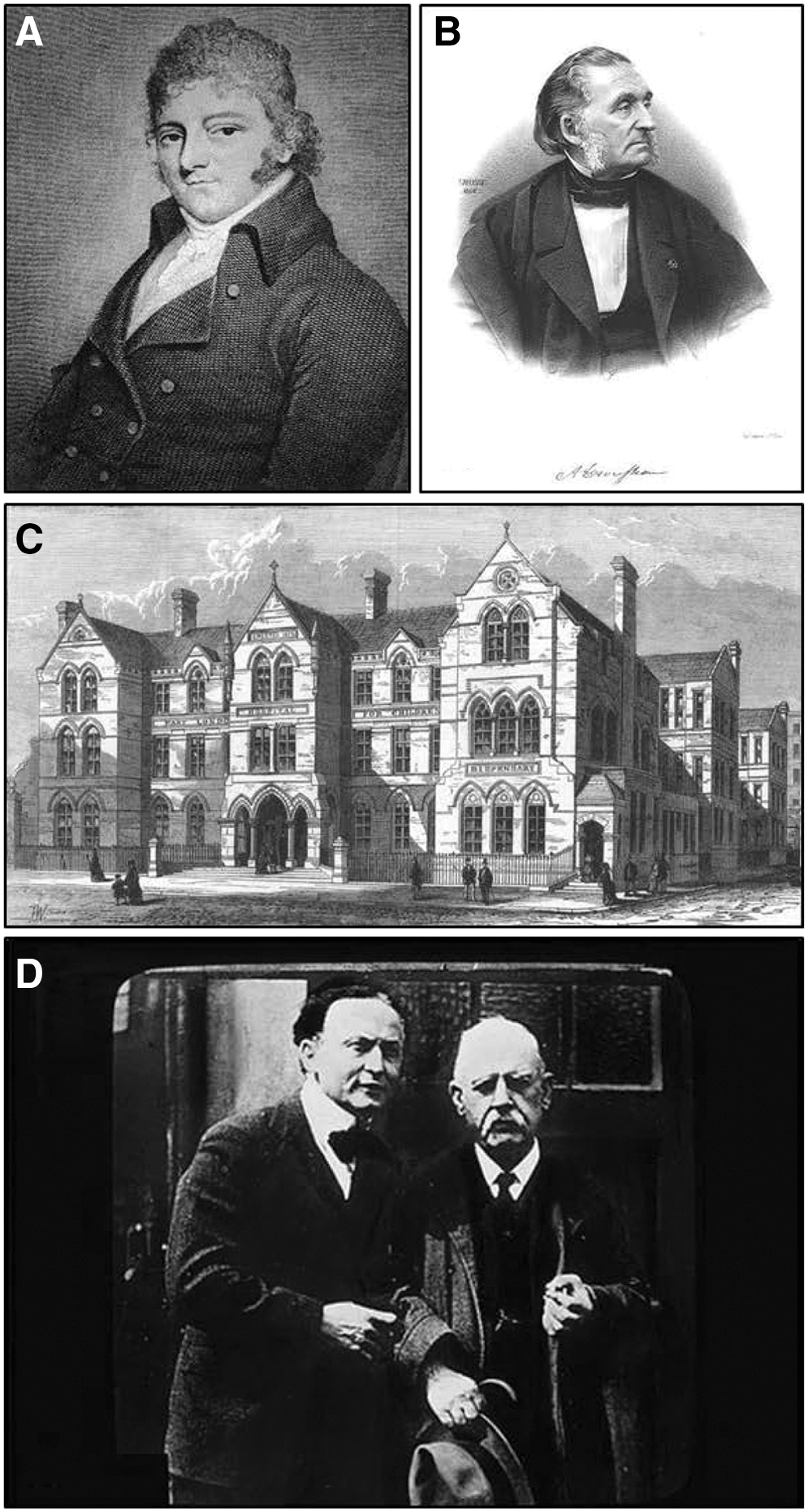
Another 500 years elapsed before we see descriptions of women suffering from thyroid disorders after delivery. The first case was a woman with probable Graves' disease (before Graves described hyperthyroidism) and was reported by Caleb Hillier Parry (1755–1822; Fig. 4A). Parry was a schoolmate of Edward Jenner, and while not eligible to attend Oxford or Cambridge due to his religion, he studied medicine in Edinburgh. Parry was a successful practitioner in Bath, United Kingdom, and was the father of Admiral Sir Edward Parry. In the posthumous publication of his writings (7), he describes a 37-year-old woman whom he saw in 1786 when she was three months postpartum. He described a lump that “continued to enlarge…occupied both sides of her neck…reached an enormous size…the part swelled was the thyroid gland…the eyes were protruded from their sockets…an appearance of agitation and distress, especially on any muscular exertion…a considerable degree of loss of appetite and thirst…edematous swelling of her legs…night sweats…each systole of the heart shook the whole trunk of the body” (7).
PPTD in the 19th century. (
Subsequent descriptions of postpartum hyperthyroidism were provided by Dr. Armand Trousseau (1801–1867; Fig. 4B). Trousseau received his Doctorate in Paris in 1825 and worked in the Hôtel Dieu. He was the first to perform tracheotomy in France, and he described the Trousseau sign of latent tetany (8). Trousseau's Lectures on Clinical Medicine were published in 1868 (9). He discussed two cases that were similar to the one reported earlier by Parry. The first was a 29-year-old woman seen in October 1861 when four and a half months postpartum. She had “palpitations of the heart…eyes had a strange restless look…dyspnea…thyroid gland very prominent…slight murmur over it…felt her goiter pulsate, and stated that her throat began to swell six weeks ago, that is, three months after delivery.” The second case, seen a year later, was a 25-year-old woman who “after birth of her last child…was violently moved on finding out that she had been right in suspecting her husband was unfaithful to her. From that time, violent palpitation of the heart; her eyes…now remarkably prominent…throat became gradually larger while her appetite increased extraordinarily…pulsations were 110–130” (9).
Perhaps the most interesting discovery of Dr. Sawin's was most likely the first report of postpartum hypothyroidism, which appeared as case #16 in a Table in the seminal 1888 report on myxedema (10). The contributing physician was Sir Horatio Bryan Donkin (1845–1927). Donkin was educated at Queen's College, Oxford, and was trained in medicine at St. Thomas' Hospital. He was a Lecturer at The London School of Medicine for Women, and from 1874 to 1898 served as Physician to the East London Hospital for Children (11) (Fig. 4C). He undoubtedly saw many young women and babies, and described a 38-year-old woman whose “last pregnancy was seven months ago, since then, symptoms of myxedema appeared; skin-cool, clammy, waxy, edema (hands, face); unpleasant dreams, nightmares, drowsy; memory very bad for recent events; profuse menses” (10).
Donkin changed careers in 1898, giving up clinical practice to become Commissioner of Prisons. He was appointed to the Royal Commission on the Care and Control of the Feeble-Minded, and in 1911 was knighted by King George V (12). Another interesting sidelight of Donkin's career was that in 1876, while a medical student, he and Edwin Ray Lankester, a laboratory assistant, attended a séance and exposed the American psychic Henry Slade (13). For this, he received international recognition in the news, and many years later, in 1920, was photographed with the magician Harry Houdini, another skeptic of spiritualism (Fig. 4D).
In 1891, Dr. George R. Murray described a woman who, after a miscarriage, developed typical symptoms of myxedema and who responded clinically to injections of an extract of sheep thyroid gland (14). He subsequently noted that “excessive child-bearing seems to be another predisposing cause [of myxedema], as the majority of cases occur in women who have borne children” (1865–1939) was an English physician, born in Newcastle-upon-Tyne, Northumberland, and educated at Eton and Trinity College, Cambridge.
The dawn of PPTD (1946–1953)
Another half century passed before physicians began to associate thyroid dysfunction with pregnancy and the postpartum period. The first to recognize a connection was Dr. H.E.W. Roberton (1904–1991; Fig. 5A). Educated at Emmanuel College, Cambridge, and St. Bartholomew's Hospital, London, he returned to Christchurch, New Zealand, as a general practitioner. He was awarded the Sir Charles Hastings Prize for his essay in 1946, and this was followed by two other publications (16,17). In the latter, he stated that “it is common in Christchurch, New Zealand, to find mothers of young babies in a poor state of health and suffering from fatigue out of all proportion to the work they do…[there is] also intense irritability, undue coldness, and dryness of the hair…treatment with thyroid extract gives complete relief” (17).
Recognition of postpartum thyroid dysfunction. (
During this time, there was also interest in the role hormones might play in lactation. Dr. Margaret Robinson published a series of articles showing that lactation could be improved using crude anterior-pituitary extract (18), iodine (19), or dried thyroid gland (20). Dr. Charlotte Naish, a general practitioner, also reported success using thyroid for lactation (21).
In the United States, Dr. Thaddeus S. Danowski (1914–1987) and colleagues measured protein-bound iodine (PBI) in a group of women during and for a year following delivery. They noted that PBI increased during pregnancy and returned to nongravid levels shortly after delivery. However, PBI levels were down in a small number of women for at least a year, suggesting relative hypothyroiodism (22). Dr. Danowski was born in Wallington, NJ, trained at Yale, and was Professor of Research Medicine and Chief of Endocrinology at the University of Pittsburgh. He also served as an Associate Editor of Metabolism.
The infancy of immunology (1960s)
The now-accepted critical role of thyroid autoimmunity in pregnancy-related and postpartum thyroid dysfunction was reported by Parker and Beierwaltes in 1961. They measured antithyroid antibody (AAB) in 23 pregnancies and found that “maternal AAB titers began to fall as early as the first trimester, tended to strike a plateau at a low level in the third trimester, and rose again during the first few months after the termination of pregnancy” (23). Dr. Beierwaltes was a native of Saginaw, MI, and Chief of Nuclear Medicine at the University of Michigan (Fig. 5B). He is known for developing 131I-MIBG imaging for adrenal tumors, and he received the Scientific Achievement Award from the American Medical Association and the Distinguished Service Award from the ATA.
Contemporaneously, Dr. R.T. Cooke reported three women who had typical hypothyroid symptoms at 3, 4, 18, and 20 months postpartum (24). All had positive thyroid antibodies, and all were treated with thyroid extract.
Early case series (1976–1982)
Fourteen more years elapsed before the beginnings of intensive study and numerous publications. The initial papers were descriptive. Amino et al. reported six women with autoimmune thyroiditis who developed transient hypothyroidism three to six months postpartum associated with goiter and their highest titer of antithyroid microsomal hemagglutination antibodies (25). The following year, they described one patient with Graves' disease who became transiently hyperthyroid one month after delivery and transiently hypothyroid for two months (26). Shortly thereafter, Ginsberg and Walfish first documented the biphasic response of postpartum thyroid dysfunction in five women with transient thyrotoxicosis associated with a low radioactive iodine uptake at one to six months postpartum, which spontaneously evolved to transient or permanent hypothyroidism (27). Amino et al. confirmed the occurrence of both postpartum thyrotoxicosis due to painless thyroiditis and Graves' disease (28 –32). Subsequently, Woolf (33), Eckel and Green (34), and Fein et al. (35) also reported on the biphasic thyrotoxic followed by hypothyroid phases in thyroid function in postpartum thyroiditis syndrome.
PPTD: coming of age (1982–1990)
The 1980s was a decade of rapid expansion of studies on PPTD spanning many continents. Amino et al. reported prevalence figures when they published that 5.5% of 505 Japanese women developed transient thyrotoxicosis and hypothyroidism after delivery (36). Shortly thereafter, Jansson et al. reported similar findings due to autoimmune thyroid dysfunction in 460 Swedish women (37). The second half of the decade included additional large studies from the United States (1,38,39), Canada (40) Wales (41), Denmark (42,43), and Thailand (44).
From these and many other studies emerged an appreciation of the broader natural history of PPTD, which included the classic biphasic thyrotoxic/hypothyroid thyroiditis, transient or permanent hypothyroidism, transient thyrotoxicosis (either thyroiditis or Graves' disease), or permanent hyperthyroidism. Studies also expanded the understanding of the HLA system and the roles of humoral and cellular autoimmunity in driving the phenotypic expressions of PPTD (45).
PPTD: refinement (1990–2012)
The past two decades have seen many articles devoted to refining further our understanding of the etiology, clinical manifestations, and management of PPTD. The group from Cardiff, Wales, has made sustained contributions to the PPTD literature. One of the early frequent senior investigators was Professor Reginald Hall (1931–1994; Fig. 5C) who was born in Belmont, County Durham, United Kingdom, trained at the Medical School in Newcastle-upon-Tyne, and practiced at the University of Wales College of Medicine (1980–1989). He was awarded the honor of Commander of the British Empire (CBE). Joining Dr. Hall et al. after their initial report (41), Dr. John Lazarus and his group have published extensively on the subject of PPTD for more than 20 years. Studies have described the long-term follow-up of these patients (46), the association of thyroid antibodies with depression in postpartum women (47), as well as the clinical spectrum of disease and role of complement in pathogenesis.
A second clinical investigator who has made numerous contributions is Dr. Alex Stagnaro-Green. His interest began as a fellow with Dr. Terry Davies when they reported an increased rate of miscarriage in thyroid autoantibody positive women (48) and described the changes in T-cell function (49).
Other important papers from Dr. Stagnaro-Green et al. include the observation that PPTD incidence increased threefold in insulin-dependent diabetic women (50) (confirming the report of Bech et al. (51)) and the recent ATA guidelines (52). Other authors have furnished additional insights. As examples, levothyroxine (L-T4), but not iodide, successfully treated postpartum hypothyroid symptoms (53), antibody titer predicts the clinical course (49,54), and PPTD or thyroid antibodies may be related to depression (55,56). Studies examined various aspects of immunologic regulation, and recently Negro et al. showed in a prospective, randomized trial that selenium given during and after pregnancy reduced thyroid peroxidase (TPO) antibody levels and postpartum hypothyroidism (57). Finally, there have been several clinical guidelines on the subject of pregnancy and PPTD in the past three years (52,58).
The future (ad finem)
The end of the story of PPTD is hopefully in the not too distant future, and it is inextricably intertwined with the recent and rapidly expanding literature on thyroid disease during pregnancy (52,58). In 2010, the number of live births was around four million in the United States, and, in 2011, there were approximately 134 million live births worldwide. We know that an estimated 10% of women during and after pregnancy have a positive TPO antibody. The presence of thyroid autoimmunity and mild to moderate iodine deficiency in pregnant women are the two principal forces that lead to thyroid dysfunction, both in the mother and the fetus. The clinical impact of chronic thyroiditis on mother and child, both during pregnancy and postpartum, have been extensively studied. In some circumstances, either L-T4 or iodine supplementation are clearly beneficial, and for milder degrees of thyroid dysfunction, many investigators have proposed L-T4 therapy during pregnancy. However, randomized clinical trials have not yet confirmed that maternal and fetal outcomes in the many women with mild TSH elevations will be improved by L-T4, and so guidelines have not yet recommended universal screening during pregnancy (52). If and when the benefits of screening are confirmed and shown to be cost-effective, then the risk of postpartum hypothyroidism will markedly diminish, as the women at risk will have been identified before delivery.
In conclusion, the answer to the question posed in the title of this vignette is Horatio Donkin. It was he who made a career change to become Commissioner of Prisons and which later led to his being knighted by King George V. And it was he, who as a result of his early experiences exposing the psychic Henry Slade, later in his career met Harry Houdini.
Footnotes
Author Disclosure Statement
No competing financial interests exist.