
Abstract
Background:
Recent studies have shown associations of hypothyroidism with arterial blood pressure, atherosclerosis, and inflammation. Based on these pathways, there might also be an association between hypothyroidism and retinal arteriolar narrowing (RAN), a marker of microvascular damage from hypertension, atherosclerosis, and inflammation. Against this background, the aim of this study was to investigate the putative association between serum thyrotropin (TSH) levels and RAN defined by arterio-venous ratio (AVR) from static vessel analysis.
Methods:
We used data from 3189 individuals from the second population-based cohort of the Study of Health in Pomerania (SHIP-TREND-0). Thyroid function was defined according to serum TSH and serum diiodothyronine (3,5-T2) levels. Low and high serum TSH levels were defined by the cutoffs 0.3 mIU/L and 3.0 mIU/L. Fundus photography of the central retina was recorded with a nonmydriatic camera, and images were evaluated by one experienced reader. An AVR <0.8 was defined as decreased. Serum TSH levels, low and high TSH, and serum 3,5-T2 levels were associated with AVR by linear regression and with AVR <0.8 by Poisson regression, both adjusted for age, sex, cigarette smoking, alcohol consumption, and intake of beta-blockers.
Results:
Serum TSH levels were significantly associated with AVR (β=−0.028 [CI −0.049 to −0.007]; p=0.009) and with a decreased AVR <0.8 (relative risk=2.05 [CI 1.13–3.73]; p=0.019). Individuals with high TSH had a 1.43 higher risk for a decreased AVR ([CI 1.04–1.96]; p=0.027) than individuals with serum TSH levels within the reference range. Serum 3,5-T2 levels were also associated with a decreased AVR (relative risk for an increase of 1 nM=0.45 [CI 0.23–0.87]; p=0.017).
Conclusions:
Our results substantiate evidence for an association between hypothyroidism and RAN. Potential mechanisms explaining this association are long-term hypertension, atherosclerotic processes, and inflammation.
Introduction
P
Previous research on the association between hypothyroidism and retinopathy is sparse. Two animal studies demonstrated a higher frequency of premature retinopathy in neonatal rats with hypothyroidism (15,16). This finding was confirmed by a study in human neonates (17). However, studies investigating possible associations between thyroid dysfunction and RAN in adult humans are lacking. Therefore, our aim was to investigate the putative association between thyroid dysfunctions and RAN in the large population-based Study of Health in Pomerania (SHIP) TREND-0. Thyroid function state was defined by serum TSH and serum diiodothyronine (3,5-T2) levels, and RAN was defined according to central retinal artery equivalent (CRAE), central retinal vein equivalent (CRVE), and the arterio-venous ratio (AVR) taken from static vessel analysis (SVA) with a nonmydriatic camera.
Methods
Study population
SHIP-TREND-0 is a population-based study conducted in the rural Northeast of Germany between 2008 and 2012 (18). For SHIP-TREND-0, a random age- and sex-stratified sample of 8826 eligible subjects was drawn from the population registry of which 4420 subjects participated (net response 50.1%). All participants gave informed written consent. SHIP-TREND-0 followed the recommendations of the Declaration of Helsinki, and was approved by the Ethics Committee of the University of Greifswald.
Of the 4420 participants in SHIP-TREND-0, 486 individuals did not undergo the ophthalmologic examination, mainly because SVA was not part of the mobile section of the study. Mobile examinations were conducted in temporary examination centers to facilitate the recruitment of individuals over a long distance to the main examination center in Greifswald. Images of 691 individuals were not readable because of poor image quality. Optical conditions limited the quality of the examination with advancing age, mainly due to an age-related increase in cataract-induced lens opacity (19). Since there were a further 50 individuals with missing data, the final study population consisted of 3198 individuals.
Assessments
Fundus photography of the central retina was recorded with a nonmydriatic fundus camera (TRC-NW 200; Topcon Corporation, Tokyo, Japan). A single 45° optic-disc-centered photograph was taken of the right eye. Examinations were conducted by certified staff. All images were processed by the software Visualis (v2.62; Imedos, Jena, Germany). During the whole study period, one single reader (C.J.), who was annually certified, determined CRAE, CRVE, and AVR from SVA according to the Atherosclerosis Risk in Communities protocol using the fundus imaging software Vesselmap 3 (Imedos, Jena, Germany) (20). The reader was blinded for all other data collected for the study. CRAE and CRVE reflect the estimated diameter of the central retinal artery and vein. These parameters were calculated from formulas introduced by Parr and Hubbard (21,22). The AVR is the ratio of CRAE and CRVE. An AVR <0.8 was defined as decreased AVR (23). This threshold is commonly regarded as suitable to separate at-risk patients from healthy subjects (23).
Blood samples were taken fasting between 7 a.m. and 2 p.m. and analyzed in the central laboratory of the University Medicine Greifswald. Serum TSH levels were measured by an immunochemiluminescent procedure (Vista; Siemens, Eschborn, Germany). Low- and high serum TSH levels were defined by the cutoffs 0.3 mIU/L and 3.0 mIU/L according to Baskin et al. (24). In a randomly selected subpopulation of 750 individuals, serum 3,5-T2 levels were measured with a recently developed immunoassay (25). The functional sensitivity of the assay is specified as 0.2 nM. The inter-assay coefficient of variation was between 5.6 and 12.9%.
Smoking status, alcohol consumption, and medication intake were assessed by computer-assisted personal interviews. Smokers were categorized into three categories: lifetime nonsmokers, former smokers, and current smokers. Alcohol consumption was evaluated as beverage-specific alcohol consumption (beer, wine, and distilled spirits) on the last weekend and last weekday preceding the examination, and the mean daily alcohol consumption was calculated using beverage-specific pure ethanol volume proportions (26). All participants were asked to bring their medication to the examination center. Intake of beta-blockers was defined by the anatomic-therapeutical-chemical (ATC) code C07, and intake of thyroid medication by the ATC code H03.
Statistical analyses
Study characteristics are presented stratified by serum TSH levels as absolute numbers and percentages for categorical data and as median, 25th, and 75th percentile for continuous data. A directed acyclic graph was drawn to identify confounders for the association between serum TSH levels and parameters from SVA (Fig. 1). Serum TSH levels were associated with AVR, artery, and vein equivalent by linear regression adjusted for age, sex, cigarette smoking, alcohol consumption, and intake of beta-blockers. Furthermore, serum TSH levels were associated with decreased AVR by Poisson regression with robust standard errors adjusted for age, sex, cigarette smoking, alcohol consumption, and intake of beta-blockers. Since serum TSH levels were associated with missing SVA parameters, we applied inverse probability weighting. The idea behind that approach is to give individuals from groups with a higher likelihood of having missing values a stronger weight in the analyses. For the full TSH range, we applied a power transformation on the TSH values to weaken the effect of outliers on the results of the regression analysis (27). Furthermore, to account for possible nonlinear relationships between TSH and parameters of SVA, fractional polynomials were tested (27). However, in our analysis, we did not detect any nonlinear relationships. Interactions of TSH with sex were tested by a likelihood-ratio test. A p-value of <0.05 was considered as statistical significant. All analyses were carried out with Stata v13.0 (Stata Corp., College Station, TX).
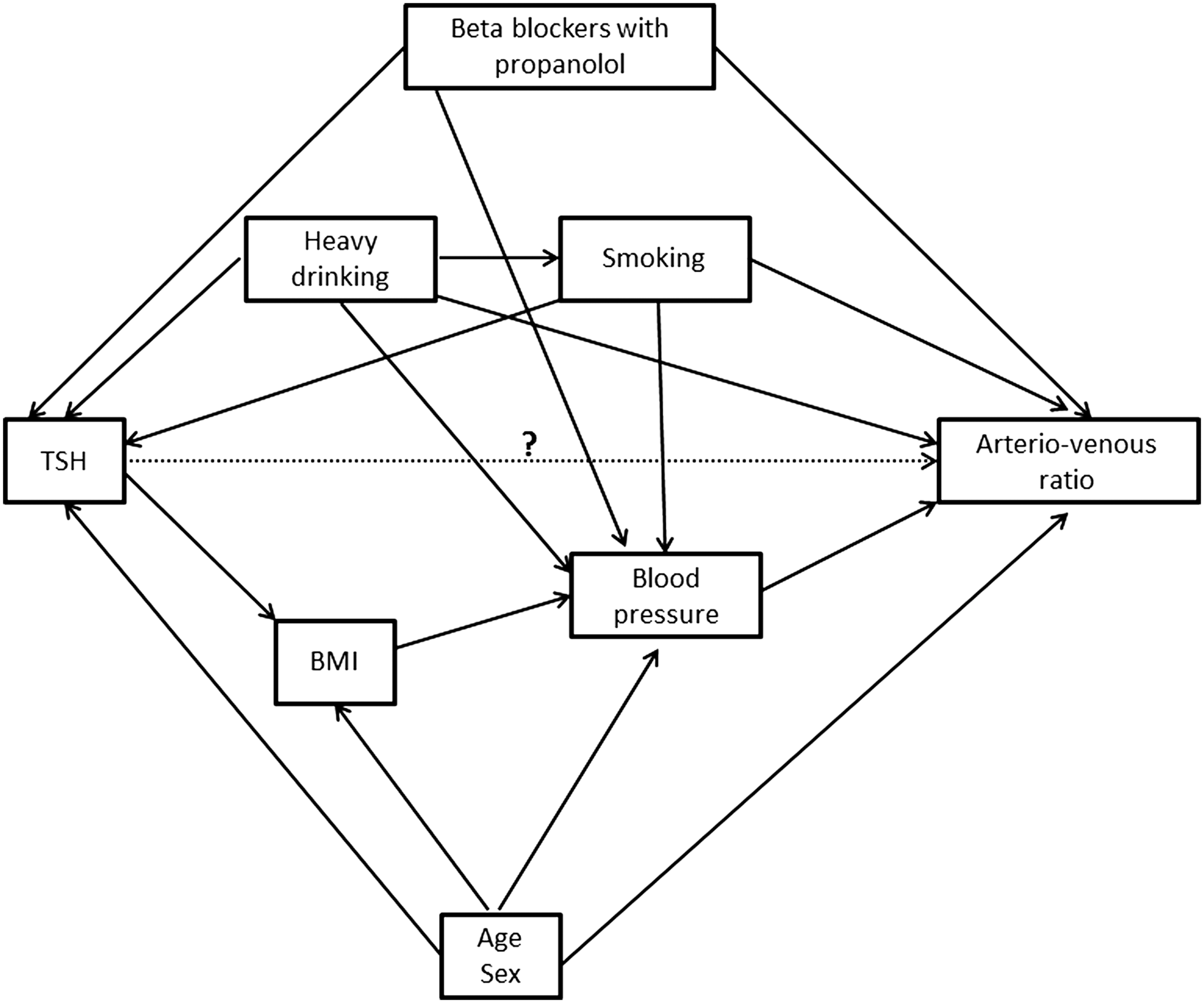
Directed acyclic graph for the association between thyrotropin (TSH) and arterio-venous ratio (AVR).
Results
There were 2964 subjects with serum TSH levels within the reference range, 86 subjects with low TSH, and 148 subjects with high TSH (Table 1). Participants with low TSH were older and participants with high TSH were younger than participants with serum TSH levels within the reference range. Among groups of low and high TSH, the frequency of males was lower than in individuals with serum TSH levels within the reference range. Frequency of individuals with a decreased AVR was highest in the group with high serum TSH levels.
Data are expressed as median (25th and 75th percentile) for continuous data and as absolute numbers (percentages) for categorical data.
AVR, arterio-venous ratio.
In multivariable linear regression, power-transformed TSH was significantly associated with both absolute AVR values and a decreased AVR, but not with retinal artery and vein equivalent (Table 2). AVR values decreased significantly with increasing serum TSH levels. Individuals with low TSH had no significantly different AVR, retinal artery, or vein equivalent compared to individuals with serum TSH levels within the reference range. High TSH was inversely associated with retinal artery equivalent and positively associated with a decreased AVR. There was no association between high TSH and retinal vein equivalent, but the retinal vein equivalent increased significantly with increasing serum TSH levels within the reference range. Serum TSH levels within the reference range were not significantly associated with AVR and retinal artery equivalent.
Linear regression (continuous outcomes) or Poisson regression with robust standard errors (dichotomous outcomes) adjusted for age, sex, smoking status, alcohol consumption, and intake of beta-blockers, and weighted by inverse probability weights for missing SVA variables. TSH was power-transformed for analysis with TSH over the full range.
p<0.05.
In comparison to TSH within the reference range.
TSH, thyrotropin.
Serum 3,5-T2 levels were not associated with the continuous AVR variable (β=0.002 [CI −0.012–0.017]; p=0.759), but significantly associated with a decreased AVR (relative risk=0.45; [CI 0.23–0.87]; p=0.016).
In the model with AVR <0.8 as a dependent variable, there was a significant interaction of TSH with sex on the multiplicative scale (p=0.043). Stratified analyses revealed significant associations between TSH and AVR in females but not in males (Table 3 and Fig. 2).
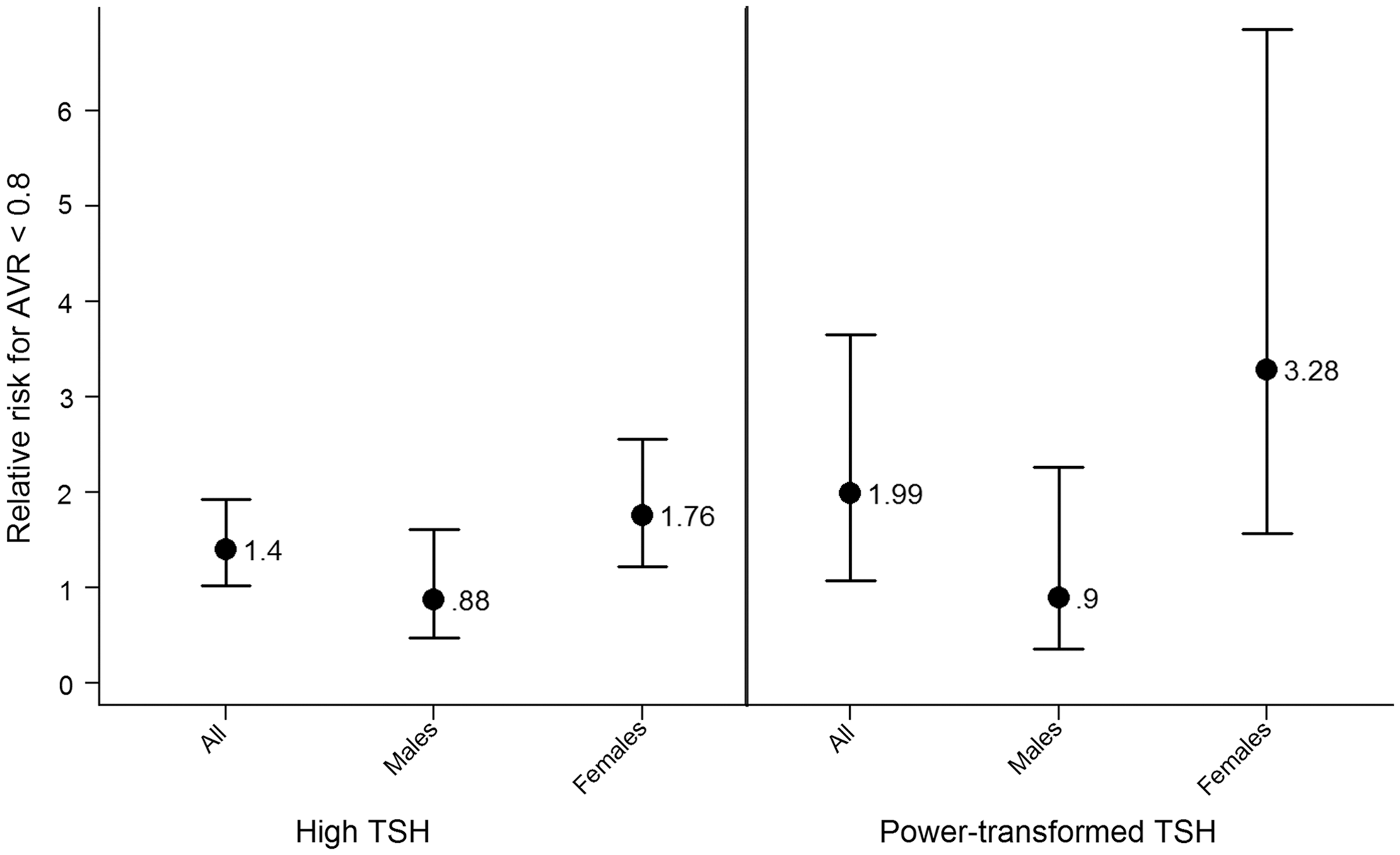
Association between serum TSH levels and AVR.
Linear regression (continuous outcomes) or Poisson regression with robust standard errors (dichotomous outcomes) adjusted for age, sex, smoking status, alcohol consumption, and intake of beta-blockers, and weighted by inverse probability weights for missing SVA variables. TSH was power-transformed for analysis with TSH over the full range.
p<0.05.
In comparison to TSH within the reference range.
Even though we used inverse probability weighting to account for missing SVA variables, this method is only adequate for missing at random (28). In our data, the number of evaluable SVA images decreases with increasing age with a frequency of 91% of evaluable images in the age group <60 years and a frequency of 65% in the age group ≥60 years. Therefore, we reanalyzed our data in subjects <60 years of age. Regarding statistical significance, these analyses revealed similar results as in the total SHIP-TREND-0 population with one exception. Serum TSH levels in the reference range were not significantly associated with the retinal vein equivalent (β=1.12; [CI −0.16–2.41]; p=0.087) in the population aged <60 years. Of note, the association between power-transformed TSH levels over the full range (relative risk (RR)=2.74; [CI 1.46–5.14]; p=0.002) and high serum TSH levels (RR=1.58; [CI 1.14–2.18]; p=0.006) with a decreased AVR <0.8 was stronger than in the main analyses over the full age range. In addition, we analyzed the data in the age groups 20–45 years and 46–82 years. These analyses showed similar mean effect sizes as already seen in the main analyses for the association between power-transformed TSH and AVR (β=−0.025 in the younger age group and β=−0.022 in the older age group) and for the association between power-transformed TSH and decreased AVR (RR=2.26 in the younger age group and RR=2.10 in the older age group). In the younger age group, these associations were statistically significant, while in the older age group these associations were not. This difference in significance is related to the lower statistical power in the older age group because this group consists of fewer subjects (n=1448) than the younger age group (n=1750). In further sensitivity analyses, we also adjusted for body mass index (BMI), since the association between TSH and BMI might be bidirectional (29,30), and excluded 307 individuals taking thyroid medication. Results of these analyses did not differ substantially from those presented in Table 2.
Discussion
This is the first study investigating the putative association between serum TSH levels and RAN in the general population. We detected significant associations between serum TSH levels and AVR. Particularly, individuals with high serum TSH levels >3.0 mIU/L had a 40% increased risk for a decreased AVR in comparison to individuals with serum TSH levels within the reference range. The higher risk for a decreased AVR in individuals with low 3,5-T2 levels substantiates this finding. 3,5-T2, a potential metabolite of triiodothyronine (T3), exerts marked thyromimetic actions without the undesirable cardiac and central side effects of T3. Animal studies showed a reduction of serum TSH levels by 3,5-T2 treatment in hypothyroid rats, indicating a link between low 3,5-T2 levels and hypothyroidism (31,32). Previous studies in hypothyroid rats furthermore showed that 3,5-T2 treatment results in prevention of fat accumulation (33) and reduced adiposity (31,34). Hence, one might speculate that low 3,5-T2 levels induce increased body weight, leading to a higher risk for hypertension and atherosclerosis. Through this pathway, 3,5-T2 levels might be associated with RAN.
RAN is a manifestation of long-term hypertension, atherosclerotic processes, and inflammation (11 –14). Recent data from large cross-sectional population-based studies showed positive associations of high serum TSH levels with arterial blood pressure (1 –4), atherosclerotic processes (7,35), and inflammation (10,36,37). Interestingly, in one of the studies that investigated the association with hypertension (2), the association with high TSH levels was only present in females not in males, which fits well with the results of our study. However, reasons for the discrepancy between the sexes are currently unclear and need further investigation. It may be speculated that sexual hormones as well as genetic differences influence associations of thyroid hormones with blood pressure, atherosclerotic processes, and inflammation. Overall, our finding of an inverse association between serum TSH levels and AVR corresponds well with the results of most studies (1 –4,7,10,36,37). On a population-based level, we could thereby substantiate evidence for an association between hypothyroidism and early vascular changes.
In contrast to our findings for high TSH levels, we did not find a significant association between serum TSH levels within the reference range and RAN. Contrary to this result, previous cross-sectional population-based studies reported a positive association between serum TSH levels within the reference range and arterial blood pressure (1,2,4). Perhaps individuals with normal high serum TSH levels at a particular time do not maintain their serum TSH level, so that current high normal TSH is associated with prevalent hypertension but does not predict incident hypertension. Thus, a change in serum TSH levels would result in an altered risk for hypertension, and individuals may only be hypertensive for a short period of time. Consequently, prevalent high normal TSH would not be associated with RAN, since RAN is not a manifestation of short-term but of long-term hypertension. In agreement with this hypothesis, a recent pooled analysis of four population-based cohort studies with 10,048 individuals reported no significant association between baseline serum TSH levels and incident hypertension (4). In addition, another study demonstrated a positive association between changes in TSH during follow-up and changes in arterial blood pressure during follow-up (3). In that study (3), however, baseline TSH levels were also associated with blood pressure at follow-up, but this association might be explained by the strong correlation of baseline and follow-up values of hypertension.
Strengths of our study are its population-based design, the large number of examined individuals, and the intensive quality control during the study. All examiners were certified before start of the study and afterwards semi-annually. Furthermore, examiner differences were evaluated every three months during the study, and no relevant deviations were detected for the SVA. In addition, all fundus images were evaluated by one experienced reader, who had an intra-reader variation <2% during the course of the study.
Limitations of our study include the cross-sectional design, allowing only limited insight into causal mechanisms, and the high frequency of non-readable images in the elderly, which might have introduced a selection bias. Therefore, we applied inverse probability weighting in our analyses. In addition, we reanalyzed our data in the <60 years population, which gave similar results compared to those in the whole study population. A further limitation is the missing determination of T3 and T4 in our study. However, 3,5-T2 levels were measured in a subpopulation and demonstrated an association with decreased AVR values.
Our results substantiate evidence for an association between hypothyroidism and RAN. Potential mechanisms explaining this association are long-term hypertension, atherosclerotic processes, and inflammation.
Footnotes
Acknowledgments
The Study of Health in Pomerania is part of the Community Medicine Research Network of the University Medicine Greifswald, which was funded by the German Federal Ministry for Education and Research, the Ministry for Education, Research and Cultural Affairs, and the Ministry for Social Affairs of the State Mecklenburg-West Pomerania. Analyses were further supported by the German Research Foundation (DFG VO955/10-1 and DFG-SPP 1629 ThyroidTransAct: DFG VO955/12-1 and DFG KO 922/16-1) and the BMELV.
Author Disclosure Statement
No competing financial interests exist.