
Abstract
Background:
Appropriate management of well-differentiated thyroid cancer requires treating clinicians to have access to critical elements of the patient's presentation, surgical management, postoperative course, and pathologic assessment. Electronic health records (EHRs) provide an effective method for the storage and transmission of patient information, although most commercially available EHRs are not intended to be disease-specific. In addition, there are significant challenges for the sharing of relevant clinical information when providers involved in the care of a patient with thyroid cancer are not connected by a common EHR. In 2012, the American Thyroid Association (ATA) defined the critical elements for optimal interclinician communication in a position paper entitled, “The Essential Elements of Interdisciplinary Communication of Perioperative Information for Patients Undergoing Thyroid Cancer Surgery.”
Summary:
We present a field-by-field comparison of the ATA's essential elements as applied to three contemporary electronic reporting systems: the Thyroid Surgery e-Form from Memorial Sloan-Kettering Cancer Center (MSKCC), the Alberta WebSMR from the University of Calgary, and the Thyroid Cancer Care Collaborative (TCCC). The MSKCC e-form fulfills 21 of 32 intraoperative fields and includes an additional 14 fields not specifically mentioned in the ATA's report. The Alberta WebSMR fulfills 45 of 82 preoperative and intraoperative fields outlined by the ATA and includes 13 additional fields. The TCCC fulfills 117 of 120 fields outlined by the ATA and includes 23 additional fields.
Conclusions:
Effective management of thyroid cancer is a highly collaborative, multidisciplinary effort. The patient information that factors into clinical decisions about thyroid cancer is complex. For these reasons, EHRs are particularly favorable for the management of patients with thyroid cancer. The MSKCC Thyroid Surgery e-Form, the Alberta WebSMR, and the TCCC each meet all of the general recommendations for effective reporting of the specific domains that they cover in the management of thyroid cancer, as recommended by the ATA. However, the TCCC format is the most comprehensive. The TCCC is a new Web-based disease-specific database to enhance communication of patient information between clinicians in a Health Insurance Portability and Accountability Act (HIPAA)-compliant manner. We believe the easy-to-use TCCC format will enhance clinician communication while providing portability of thyroid cancer information for patients.
Introduction
E
The MSKCC Thyroid Surgery e-Form is purely a synoptic operative report and was not designed to act as a stand-alone application. The Alberta WebSMR is composed of two main sections, Preoperative Assessment and Surgical Procedure. The Surgical Procedure section consists of six synoptic operative reports corresponding to the specific procedure type, including: Thyroid Lobectomy and Isthmus, Near Total/Total Thyroidectomy, Subtotal Thyroidectomy, Completion Thyroidectomy, Neck Dissection, Total/Near Total+Ipsilateral Central Lymph Node Dissection.
The Thyroid Cancer Care Collaborative (TCCC) is a comprehensive, Web-based and Health Insurance Portability and Accountability Act (HIPAA)-compliant relational database in which physicians can record information regarding a patient's thyroid cancer. The TCCC is composed of 10 different reporting modules, each of which represents a different phase of a patient's care. The modules include: initial presentation, imaging, surgical management, postoperative hospital course, pathology/staging, nuclear medicine, laboratory results, posttreatment surveillance/surgical follow-up, patient care timeline, and change in health status. The patient care timeline provides a bullet list of the major events in the patient's care that serves as a capsule summary of the major diagnostic findings and therapeutic interventions in a patient's journey with thyroid cancer. The change in health status module communicates essential changes in a patient's health that influences their thyroid cancer management.
In 2012, the American Thyroid Association (ATA) published a position paper, “The Essential Elements of Interdisciplinary Communication of Perioperative Information for Patients Undergoing Thyroid Cancer Surgery,” defining critical elements for optimal interclinician communication (3). The ATA released this statement in an effort to describe the perioperative details necessary for the effective multidisciplinary management of thyroid cancer and to improve connectivity between the various clinicians involved in the care of a thyroid cancer patient. The article describes the critical data points that the ATA believes must be captured and disseminated to treating physicians. These data points reflect the general requirements necessary to develop “an optimal management plan that will lead to a rational, risk-based approach to initial therapy, adjuvant therapy, and follow-up studies” (3). We performed a comparison of these three disease-specific electronic systems in order to determine which system best achieves the gold standard for disease management data reporting that was established by the ATA. In so doing, we hope to highlight the merits and disadvantages of each system.
Summary
We reviewed the ATA statement on the “The Essential Elements of Interdisciplinary Communication of Perioperative Information for Patients Undergoing Thyroid Cancer Surgery,” from 2012 and catalogued each essential data point into one of three categories: preoperative, intraoperative, and postoperative management of thyroid cancer. We similarly organized each of the data points collected by the TCCC and the Alberta WebSMR. Because the MSKCC Thyroid Surgery e-Form is purely an operative report, it was compared only to the intraoperative section of the ATA's report. The Alberta WebSMR consists of primarily preoperative and intraoperative sections and was thus compared only to those sections of the report. Each instance of overlap between the ATA position paper and the comparative system was recorded. Instances in which the system in question captured additional data not required by the ATA were also recorded.
Preoperative Management
According to the ATA statement on perioperative reporting, seven general categories of information are essential for comprehensive communication of preoperative thyroid cancer patient information: (1) high-risk physical examination findings; (2) high-risk historical features; (3) the results of preoperative scans (e.g., ultrasounds, radiographs, radioactive iodine scans); (4) laryngoscopic findings on preoperative assessment of the laryngopharynx; (5) comorbidities that may affect treatment plan; (6) locations of known or suspected metastases; and (7) laboratory results (3). Within these seven categories, the ATA notes 50 data points, shown in Table 1, which they recommend be included in a comprehensive medical record. With the ATA statement on perioperative reporting as the reference point, the Alberta WebSMR meets all preoperative general requirements and 23 of 50 specific data points outlined by the ATA (Table 1). The TCCC meets all preoperative general requirements and captures all 50 data points mentioned by the ATA. The TCCC collects detailed information on the history of patients who present with recurrent disease, including prior treatment and the status of parathyroid glands. In addition, the TCCC provides an opportunity to report important elements such as genetic mutations related to thyroid cancer as well as the method by which the cancer was discovered (Table 2).
ATA, American Thyroid Association; TCCC, Thyroid Cancer Care Collaborative; EBRT, external beam radiation therapy; RAI, radioactive iodine; CEA, carninoembryonic antigen; TSH, thyrotropin; PET/CT, positron emission tomography/computed tomography; MRI, magnetic resonance imaging.
Intraoperative Management
The ATA position paper defines three general categories that are essential for the comprehensive collection of intraoperative data: extent of thyroid surgery (e.g., completeness of resection, details regarding lymph node dissection); surgical complications (e.g., status of the recurrent laryngeal nerves and parathyroid glands); and operative findings (e.g., presence or absence of gross extrathyroidal extension) (3). Within these three broad categories of intraoperative data collection, the ATA position paper notes 32 data points, shown in Table 3, which they recommend be included to fully capture details about the operative procedure and resected tissues.
ATA, American Thyroid Association; TCCC, Thyroid Cancer Care Collaborative; MSKCC, Memorial Sloan-Kettering Cancer Center; RLN, recurrent laryngeal nerve; PTH, parathyroid hormone.
The ATA also includes some additional recommendations, such as the inclusion of a sketch of operative findings, a dictated narrative, and a synopsis of the patient's history and treatment course for the benefit of clinicians and/or other health care professionals who are not the treating surgeon (3). The intraoperative component of the MSKCC Thyroid Surgery e-Form, the Alberta WebSMR, and the TCCC are compared to the ATA intraoperative recommendation below and in Table 3.
MSKCC Thyroid Surgery e-Form
In comparison to the ATA position paper, the MSKCC Thyroid Surgery e-Form meets all intraoperative general requirements but only captures 21 of 32 data points specifically mentioned by the ATA. The MSKCC Thyroid Surgery e-Form does not incorporate any visual components, such as a sketch of operative findings as recommended by the ATA. In keeping with its intent to serve purely as an operative report, the MSKCC Thyroid Surgery e-Form also does not incorporate a synopsis of the patient's history and treatment course or a detailed record of pathologic findings. However, the MSKCC Thyroid Surgery e-Form does include a free-text “Notes” section and features additional fields such as preoperative, postoperative diagnosis, and prep and position (Table 4).
TCCC, Thyroid Cancer Care Collaborative; MSKCC, Memorial Sloan-Kettering Cancer Center.
Alberta WebSMR
In comparison to the ATA position paper, the Alberta WebSMR operative report meets all general requirements and captures 22 of 32 data points specifically mentioned by the ATA (2). Missing from the fields captured by the Alberta WebSMR are disease characteristics including substernal extent and surrounding fibrosis, and other fields such as placement of incision, estimated blood loss, and patient disposition at the completion of surgery. In addition, the Alberta WebSMR does not include a procedure synopsis or a sketch of operative findings. However, the Alberta WebSMR features additional fields such as nodule mobility and status of the superior laryngeal nerve (Table 4).
TCCC
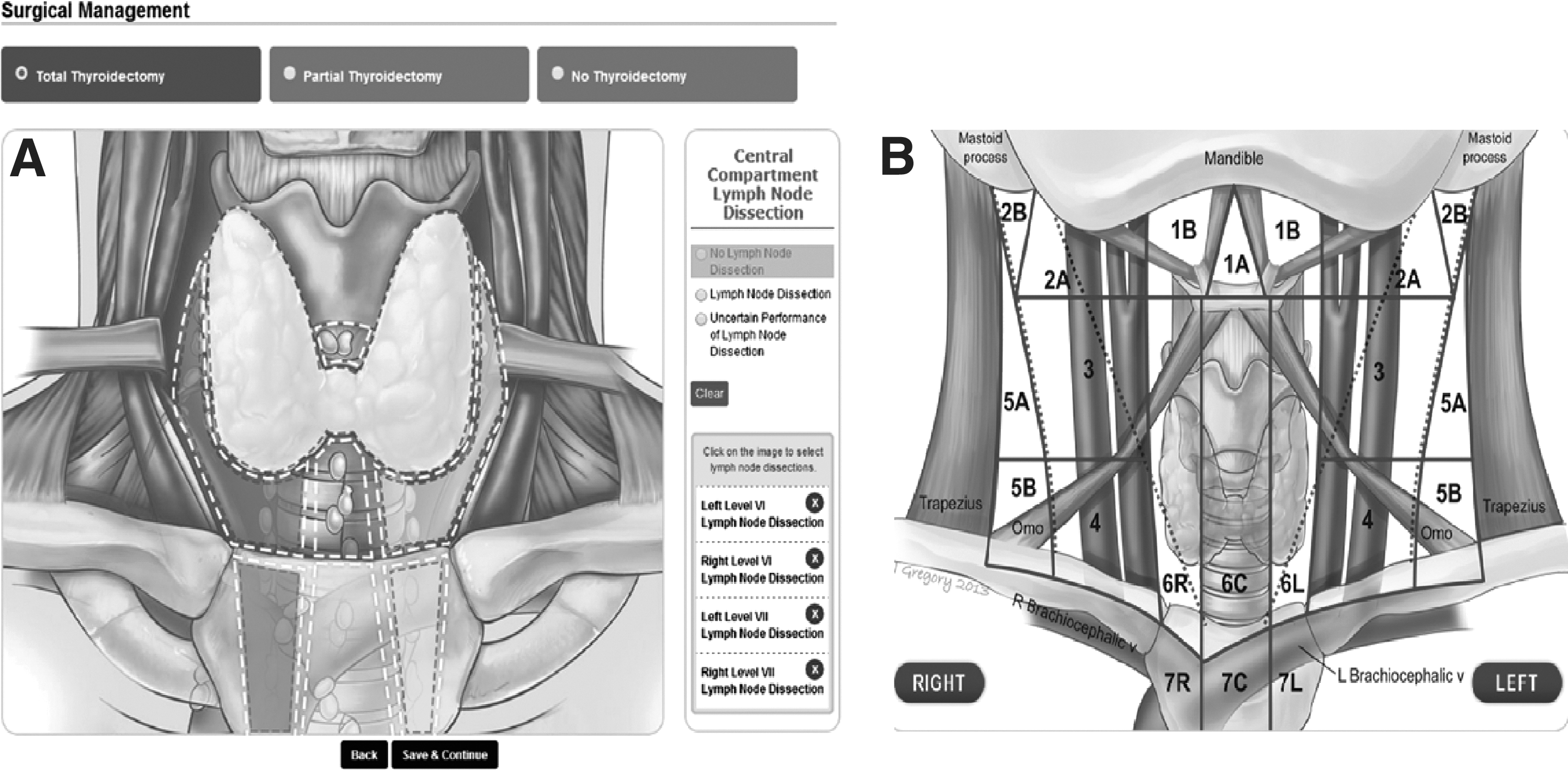
The TCCC meets all intraoperative general requirements and captures 29 of 32 data points outlined by the ATA. For example, the TCCC features many visual components, including intraoperative anatomic diagrams on which surgeons can tap and click to record any visceral, vascular, or muscular structures that were removed in the process of resecting invasive disease. Surgeons can also tap and click to identify and record the specific lymph node compartments of the central and lateral neck that were resected as well as the portions of the thyroid that were removed (Fig. 1).
The TCCC also features the automatic generation of narrative operative reports. Data entered into the surgical management module are used to automatically create a narrative operative report that can be customized for each physician and institution.
The TCCC also includes drop-down menus and radio buttons for ease of data entry as shown in Figure 2, as well as free-text “Notes” sections in which clinicians can record further information regarding intraoperative findings and unusual anatomic details.
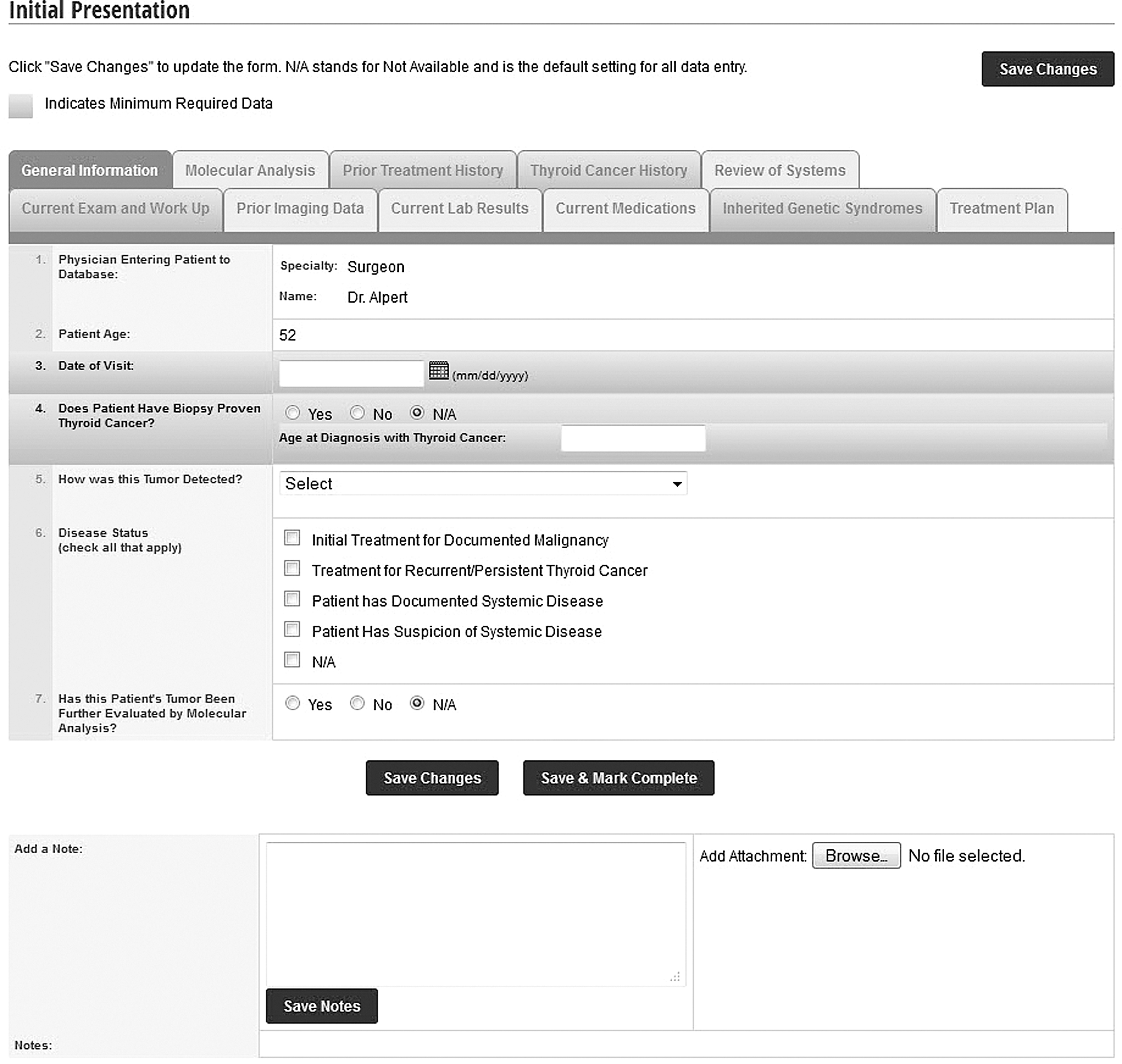
The first tab of the Initial Presentation module of the Thyroid Cancer Care Collaborative (TCCC).
Postoperative Management
According to the ATA position paper, 6 general categories are essential for the comprehensive reporting of postoperative data: operative complications; hypocalcemia and hypoparathyroidism; final pathologic results and staging; replacement therapy (i.e., calcium, levothyroxine); use of iodinated contrast computed tomography scans; and postoperative treatment plan (3). Within these 6 categories of postoperative data collection, the ATA notes 38 fields, shown in Table 5, which they recommend be included to fully capture details about the postoperative period.
ATA, American Thyroid Association; TCCC, Thyroid Cancer Care Collaborative; CEA, carninoembryonic antigen; T4, thyroxine.
The TCCC meets all postoperative general requirements and captures all 38 data points defined by the ATA (Table 5). In a comparison between the basic dataset for pathology recommended by the ATA and the Pathology/Staging module of the TCCC, we found that the TCCC was in complete compliance with the ATA guidelines. The TCCC captures all 10 data fields relating to pathologic results deemed essential by the ATA. The pathology module of the TCCC is consistent with the College of American Pathologists (CAP) Protocol and captures additional critical details such as the presence of extranodal extension, the number of positive nodes identified in the sample, and the size of the largest positive lymph node. It is important to note that the TCCC automatically feeds the pathology data into the staging module to calculate each patient's MACIS score, as well as assigning the stage of disease according to the American Joint Committee on Cancer (AJCC) prognostic staging systems. The TCCC also automatically assigns a level of risk of recurrence—low, intermediate, or high—based on the ATA clinical practice guidelines. The TCCC features a “banner” that discretely lists patient information essential for a comprehensive understanding of the patient's thyroid cancer history and the current status of his or her disease. Shown in Figure 3, the banner is located at the top of each surveillance module of the TCCC after therapy has been initiated. It is designed to increase the efficiency and accuracy of postoperative clinical decisions that are made in the care of this rapidly growing population of patients.

Physician banner listing all critical elements of a patient's history, diagnostic, and therapeutic interventions as well as stage and response to therapy.
Thyroid cancer surgery, in particular, is highly conducive to electronic reporting (1). Effective management of thyroid cancer is a highly collaborative effort between physicians of different specialties. The patient information communicated between physicians and the way in which it factors into clinical decisions is complex. For these reasons, the method of interphysician communication is extremely relevant in the optimization of patient care. Electronic reporting can promote efficiency and portability, which allows physicians to deliver a high level of care to a large number of patients (4). Accurate and efficient communication between physicians is also essential for effective, individualized treatment planning, which allows for a better understanding of the particular patient's disease biology and may better detect and manage advanced disease. Effective treatment planning may also minimize the likelihood of recurrent disease, and may maximize the chances for an optimal outcome. It can also reduce the risk of excessive or unnecessary testing for those patients who achieve a favorable response to therapy.
According to a study by Iyer et al. (1) in 2011, an interinstitutional electronic reporting system for the capture of perioperative information regarding thyroid cancer had yet to be developed. The American Thyroid Association's statement on “The Essential Elements of Interdisciplinary Communication of Perioperative Information for Patients Undergoing Thyroid Cancer Surgery,” defines a clear gold standard that new electronic medical records should emulate.
The MSKCC Thyroid Surgery e-Form, Alberta WebSMR, and TCCC are electronic medical records designed specifically to capture the data set needed for thyroid cancer management. Based on the field-by-field analysis conducted in this study, the TCCC is the most comprehensive. To our knowledge, the TCCC is also the only system designed specifically to facilitate interinstitutional and interclinician communication in a HIPAA-compliant manner. The TCCC promotes effective interinstitutional communication among physicians by centralizing all patient information regarding thyroid cancer care in an immediately accessible online platform. TCCC also features unique anatomic diagrams that allow for efficient and accurate data entry as well as a highly visual mechanism for reporting results (Fig. 1). Finally, by prompting physicians to determine each patient's “response to therapy” at the end of each follow-up module, the goal of individualizing surveillance strategies and adjuvant therapy can be achieved.
Challenges Ahead
All interinstitutional reporting systems face significant challenges in their implementation. The primary challenge is achieving interoperability between the new reporting system and existing hospital based EHRs as well software reporting for pathology and laboratory data. This is true in particular for the TCCC, which has been designed to facilitate interinstitutional communication of perioperative data for enhanced thyroid cancer management. Achieving smooth information flow from different systems and institutions into the TCCC, to avoid duplication of effort, is a recognized and universal challenge plaguing all patient registries. It is essential that patient information be transferred accurately. This is facilitated in the TCCC by virtue of the fact that multiple clinicians, involved in the care of a specific patient, are given access to all information entered into the system in a rapid fashion that allows for questions, challenges and ultimately, edits to data entry when needed. The integration of these disparate systems with the TCCC is in active development.
Conclusion
Effective management of thyroid cancer is a highly collaborative, multidisciplinary effort. The patient information which factors into clinical decisions about thyroid cancer is complex. For these reasons, electronic health records are particularly favorable for the management of patients with thyroid cancer. The MSKCC Thyroid Surgery e-Form, the Alberta WebSMR, and the TCCC each meet all of the general recommendations for effective reporting of the specific domains that they cover in the management of thyroid cancer, as recommended by the ATA. However, the TCCC format is the most comprehensive. The TCCC is a new Web-based disease specific database to enhance communication of patient information between clinicians in a HIPAA compliant manner. We believe the easy to use TCCC format will enhance clinician communication while providing portability of thyroid cancer information for patients.
Footnotes
Acknowledgment
We would like to acknowledge the Mount Sinai Health System for their generous support of this research project.
Author Disclosure Statement
No competing financial interests exist.