
Abstract
Background:
Glucocorticoid (GC) therapy has been shown to prevent Graves' ophthalmopathy (GO) progression following radioactive iodine (RAI) treatment. However, the optimal regimen is controversial, with studies from recent years suggesting the use of lower doses and shorter GC treatment courses.
Methods:
We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) and retrospective controlled trials comparing GC regimens versus placebo, no treatment, or other GC regimens.
Results:
Eight trials evaluating 850 patients fulfilled inclusion criteria. In patients with preexisting GO, standard dose prednisone (0.4–0.5 mg/kg tapered over 3 months) was very effective for prevention of GO progression (OR 0.14 [CI 0.06–0.35], p<0.01) in patients with mild to moderate GO. Two studies evaluated low-dose prednisone (0.2–0.3 mg/kg for 4–6 weeks) in patients with mild GO or risk factors, but were limited by not including patients with preexisting GO in the control groups. Therefore, the two low-dose groups were evaluated using indirect comparisons with control groups matched for age and clinical activity score, showing excellent efficacy versus no treatment or placebo (OR 0.20 [CI 0.07–0.60], p=0.004) and no significant difference compared with standard dose (OR 1.7 [CI 0.52–5.52], p=0.47). In patients without preexisting GO, steroid prophylaxis had no beneficial effect (OR 1.87 [CI 0.81–4.3]), though there were insufficient data regarding patients with risk factors for GO development. GC prophylaxis had no impact on hyperthyroidism resolution (OR 1.05 [CI 0.69–1.58]), and GC side effects were common but mild.
Conclusions:
Current evidence supports a three-tier approach for prevention of GO progression following RAI. Standard dose prednisone is the best validated regimen and should be used in patients with mild to moderate GO who have high risk of progression, while low dose prednisone can be used in patients with mild GO, and in patients without preexisting GO who have risk factors and are selected for GC prophylaxis. Patients without preexisting GO and without risk factors should not be treated with GC prophylaxis.
Introduction
R
The efficacy of corticosteroids in prevention of RAI-induced GO activation was well demonstrated in two randomized controlled trials (RCTs) by Bartalena et al., using prednisone tapered over three months (3,10). Since then, several studies evaluated lower doses of prednisone with shorter treatment duration (11), and some studies found steroid prophylaxis to be ineffective (9,12). According to a treatment consensus of the European Group on Graves' Orbitopathy (EUGOGO) published in 2008, and the management guidelines of the American Thyroid Association (ATA) in association with the American Association of Clinical Endocrinologists (AACE), prednisone prophylaxis 0.4–0.5 mg/kg is recommended in patients recognized to be at risk for GO activation, tapered over three months (13,14). In practice, there is wide variation in when and how glucocorticoids (GCs) are used to prevent GO progression as far as who should be treated, the optimal GC dose, and the duration of treatment (15). To address this challenge, we performed a systematic review and meta-analysis to determine the best validated and effective GC regimen for GO prophylaxis, with an emphasis on lower doses of prednisone, stratified by GO status prior to RAI treatment.
Methods
Data sources
We searched PubMed (January 1966 to January 2014), CENTRAL (The Cochrane Library, up to January 2013), and conference proceedings in endocrinology, ophthalmology, and nuclear medicine. The terms “Graves' ophthalmopathy” and similar, “radioiodine” or “radioactive iodine” and similar, and “steroids” or specific steroid names were crossed. We scanned references of all included trials and reviews identified for additional studies.
Study selection
We included all RCTs, as well as retrospective controlled studies comparing steroid regimens with controls, including placebo, no intervention, or a different steroid regimen for prevention of GO progression. We included trials regardless of publication status and language. Studies in which GO progression was not a primary outcome were included only if they were RCTs, as the risk for selection bias with this design is small. Two reviewers independently inspected each reference identified by the search and applied inclusion criteria.
Data extraction and quality assessment
Two reviewers independently extracted data from the included trials. In the case of any disagreement between the two reviewers, a third reviewer extracted the data. We contacted the authors of trials for missing data, when necessary. Two independent reviewers assessed the trials for methodological quality. We individually assessed the following components: allocation concealment, generation of the allocation sequence, and blinding. We graded allocation concealment and generation as adequate, unclear, or inadequate (16). We also collected data on exclusions after randomization and whether the primary analysis was performed according to the intention-to-treat principle or per protocol.
Definition of outcomes
The primary outcome was new or worsening GO following RAI treatment, stratified according to preexisting GO status. Secondary outcomes included resolution of hyperthyroidism and steroid-related adverse events.
Data synthesis and analysis
We analyzed data by calculating the odds ratio (OR) for each trial, with uncertainty expressed using 95% confidence intervals (CI) (Review Manager (RevMan) v5.2 for Windows; The Cochrane Collaboration, Oxford, United Kingdom). We utilized a fixed-effect model using the Mantel–Haenszel method for pooling trial results throughout the review, unless statistically significant heterogeneity was found, in which case we chose a random-effects model using the DerSimonian and Laird method. We assessed the heterogeneity of trial results by inspecting graphical presentations and calculating a chi-square test of heterogeneity and a I 2 measure of inconsistency (17). We explored potential sources of heterogeneity through predefined subgroup analyses.
Results
Description of the studies
The literature search identified 19 manuscripts of GC treatment to prevent GO progression following RAI treatment for Graves' hyperthyroidism. Reasons for exclusion are detailed in Figure 1. Eight studies that were performed between 1986 and 2010 fulfilled inclusion criteria, including five RCTs and three retrospective controlled studies, evaluating 850 patients (Table 1) (3,9 –12,18 –20). GCs used were oral prednisone in five studies, oral betamethasone in two studies, oral prednisolone in one study, and intravenous methylprednisolone in one study.
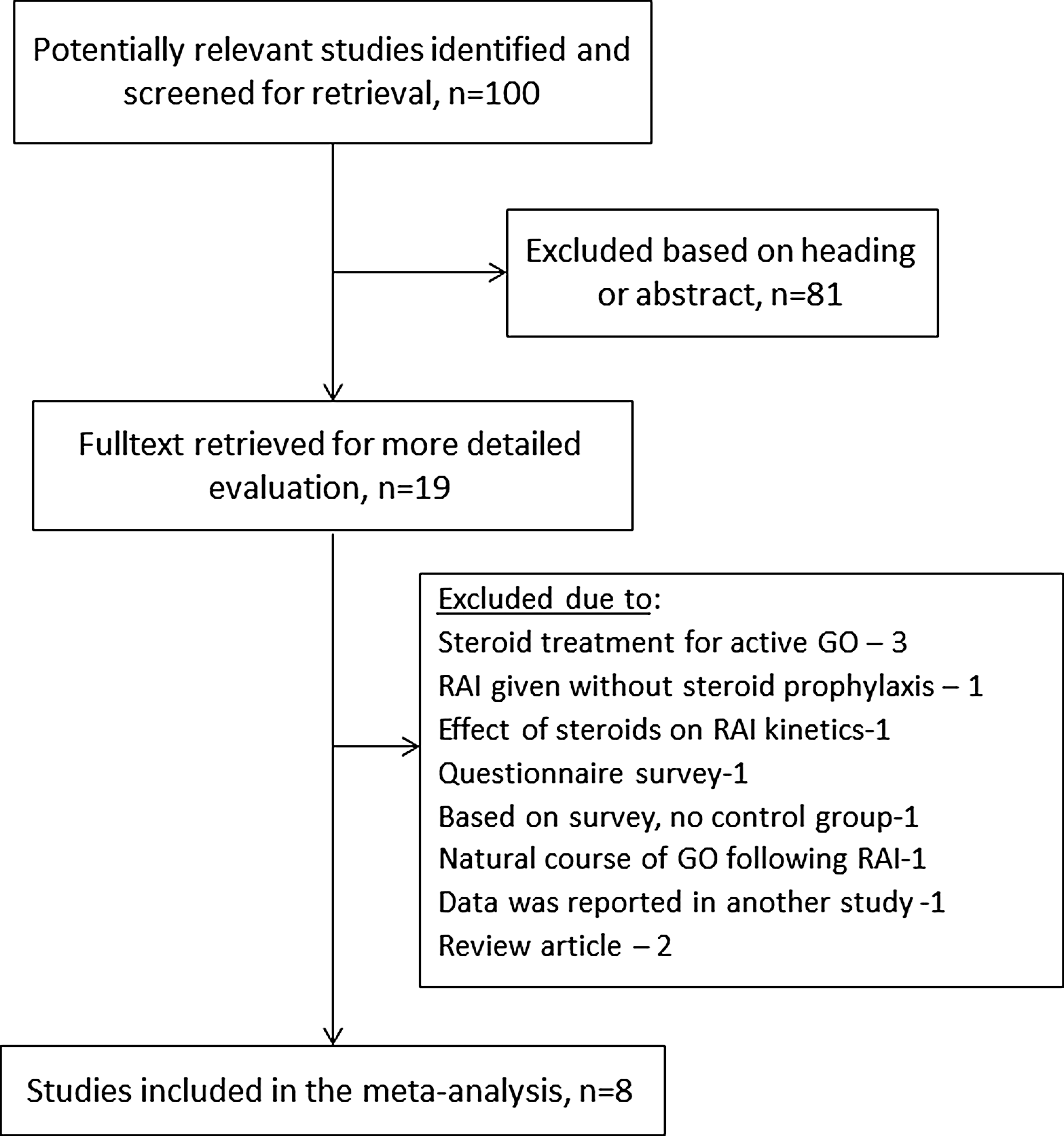
Selection process for included studies.
Based on supplementary data provided by the authors.
Allocation grading: A, adequate; B, unclear.
NA, not available; Y, yes; N, no.
Preexisting GO was present in >50% of patients in five studies, in <50% in one study, and in none of the patients in two studies. Steroid administration was initiated before RAI in three studies, on the day of RAI treatment in one study, one to three days after RAI treatment in four studies, and a week after RAI treatment in one study (Tables 1 and 2).
Patients with preexisting GO
Six studies reported GO outcome following RAI treatment in patients with preexisting GO (3,10 –12,18,19). In one study, the entire patient population had preexisting GO (20), while in others, data were extracted from the treatment and control groups. The clinical activity score (CAS) before treatment was reported in three studies (Table 1) correlating with mild to moderately active GO, and in three studies, the GO severity was described in the text as mild, or mild to moderate. Overall, GCs were very effective in preventing GO progression in patients with preexisting GO (OR 0.14 [CI 0.06–0.35], 378 patients; Fig. 2). The most studied drug was prednisone, which was evaluated in three RCTs and three retrospective studies, with doses ranging from 0.2 mg/kg to 0.5 mg/kg, and duration ranging from 1 to 10–12 months. Standard dose prednisone, 0.4–0.5 mg/kg a day for three or more months, was evaluated in five studies (three RCTs and two retrospective studies) in patients with mild to moderate GO, with excellent efficacy (OR 0.16 [CI 0.06–0.37], p<0.01). Sensitivity analysis by study type showed higher effects estimates in RCTs compared with retrospective studies (Fig. 2).
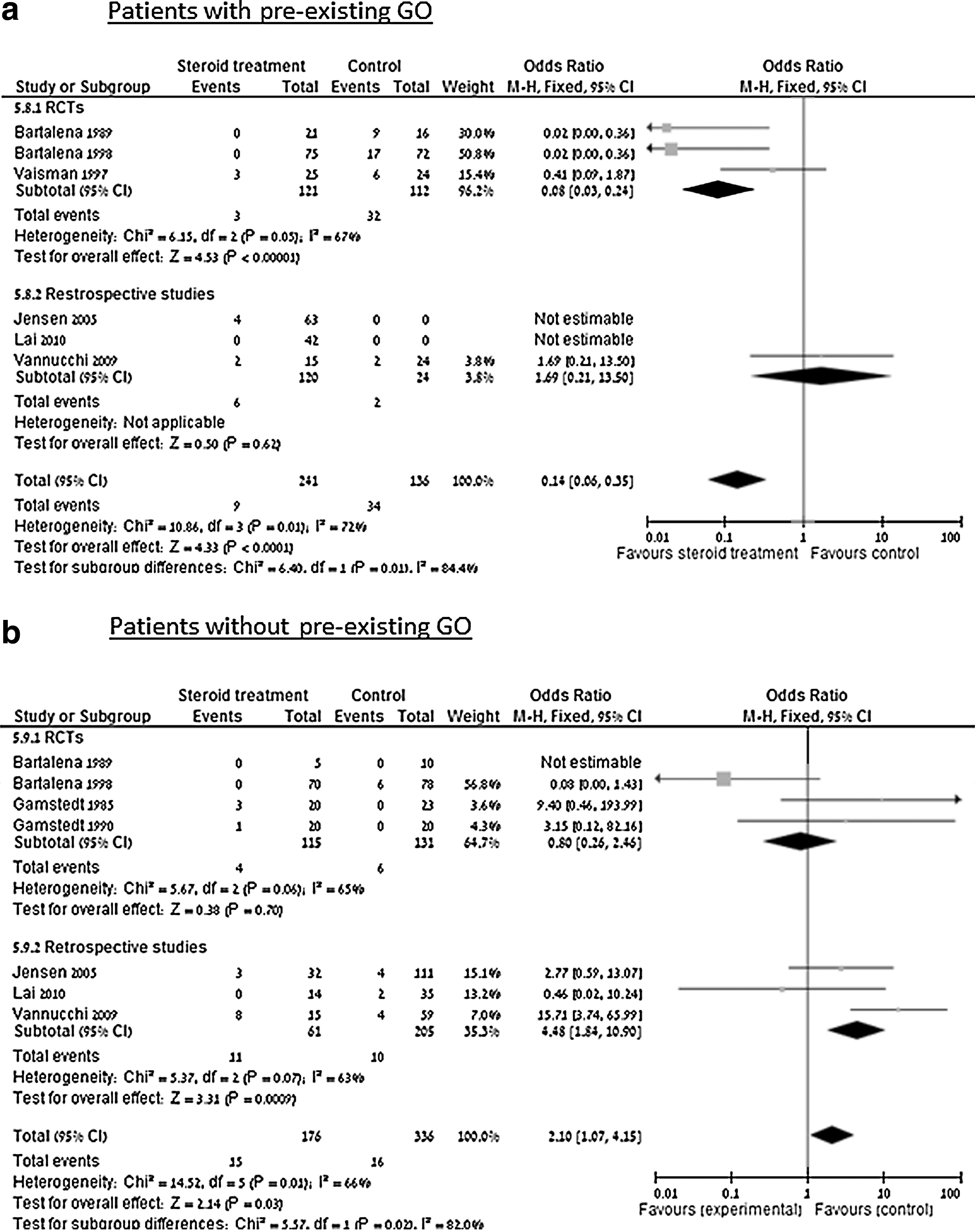
Graves' ophthalmopathy (GO) progression stratified according to preexisting GO status.
Low-dose prednisone, 0.2–0.3 mg/kg tapered over four to six weeks, was evaluated in two retrospective studies in patients with mild GO (11,12). In both studies, the intervention arm included patients with mild or mild to moderate GO, while the control group included patients without preexisting GO, making the groups incomparable due to different patient populations. Therefore, to evaluate the efficacy of low-dose prednisone, an indirect comparison was made between the intervention groups and matched control groups from the studies included in the meta-analysis, which were matched for sex, age, and disease activity (females 80% vs. 81%, age 45.5 vs. 43.6 years, and CAS 0.9 (SD=0.8) vs. 1.1 (SD=0.7) respectively, n.s.) (3,9,20). Low-dose prednisone was effective in preventing GO progression compared to no treatment or placebo (OR 0.20 [CI 0.07–0.60], p=0.004) (3,9,20) (Fig. 3), and was not significantly different from standard dose prednisone (OR 1.7 [CI 0.52–5.52], p=0.47) (3,9 –11,20).

GO progression stratified by drug.
Intravenous methylprednisolone was evaluated in one retrospective study, in which five patients with preexisting GO were treated once weekly for one month (Table 2), and none had disease progression. This was compared to no treatment and to standard dose prednisone, but the sample size was insufficient to prove efficacy or noninferiority when a noninferiority limit (d) of 25% was used.
Patients with no preexisting GO
GC treatment for the prevention of GO progression in patients without GO was evaluated in seven studies, of which four were RCTs and three were retrospective studies (3,9 –12,18,19) (Table 1). In two studies, no participant had preexisting GO (18,19), while in others, these patients represented 20–68% of the study population. Prednisone was evaluated in four studies (two RCTs and two retrospective), betamethasone in two RCTs, prednisolone in one retrospective study, and intravenous methylprednisolone in one retrospective study (Table 1).
In patients without preexisting GO, standard dose prednisone (0.4–0.5 mg/kg for three months) was evaluated in two RCTs and two retrospective studies, and was ineffective (OR 1.87 [CI 0.81–4.3]). Betamethasone was evaluated in two RCTs, and was also found to be ineffective (OR 6 [CI 0.68–52.9]).
When subgroup analysis was performed according to study type, there was a clear difference between RCTs showing steroid prophylaxis to be ineffective (OR 0.8 [CI 0.26–2.46]), and retrospective studies that surprisingly found steroid prophylaxis to be harmful. However, in these three retrospective studies, the intervention and control groups were uneven, with all patients in the intervention group having one or more risk factors, while all patients in the control group had no risk factors, and thus a significantly lower risk of progression. The risk factors included smoking and/or thyrotropin receptor antibody (TRAb) levels (9,11,12). Even after carefully inspecting all included studies in the meta-analysis, none of the control groups were comparable to the intervention groups of patients with risk factors, and therefore the retrospective studies cannot guide treatment in patients without preexisting GO who have risk factors for GO progression.
Hyperthyroidism resolution
Four studies reported rates of hyperthyroidism resolution following RAI treatment with concomitant steroids compared to those treated with RAI alone (3,12,18,19). GC administration had no impact on treatment success rates (OR 1.05 [CI 0.69–1.58]). In a study by Bartalena et al., the rate of hyperthyroidism resolution was not reported, but was described as “similar” (10).
GC-related side effects
Four studies reported side effects of GC treatment, and all were described as minor (3,9 –11). These side effects included Cushingoid features, weight gain (average 2.8 kg with regular-dose prednisone and 1.8 kg with low-dose prednisone), anxiety, hyperglycemia, and insomnia. Side effects were reported in 62% with prednisone 0.4–0.5 mg/kg, in 43% with low-dose prednisone (0.2–0.3 mg/kg), and in 48% with intravenous methylprednisolone.
Discussion
To guide the optimal use of GC to prevent GO progression following RAI treatment, we performed a systematic review and meta-analysis evaluating 850 patients with Graves' disease. Our work stratified patients, for the first time to our knowledge, according to GO status prior to RAI treatment. Our results show that GCs are very effective in preventing GO progression in patients with preexisting GO, but not in patients without preexisting eye involvement (Fig. 2). The most validated regimen is prednisone 0.4–0.5 mg/kg given for three months or more in patients with preexisting eye disease, as recommended by both the ATA/ACEE management guidelines from 2011 and the EUGOGO consensus statement from 2008. While this regimen was evaluated in patients with mild or moderate GO, newer studies evaluated low-dose prednisone (0.2–0.3 mg/kg for four to six weeks) in patients with mild GO or risk factors, which was found to be an effective alternative with significantly less adverse effects. In patients without preexisting GO, steroid prophylaxis was ineffective in preventing GO development.
The need for an evidence-based approach to GC prophylaxis was well demonstrated by a survey among members of the European Thyroid Association (15). In that survey, there was a wide variation in the decision of who to treat and what regimen to use. Some respondents did not prescribe GC in any clinical scenario, others gave GCs to all patients receiving RAI therapy, while the majority only gave GCs to patients with some degree of ocular involvement or if risk factors, such as smoking, were present. This heterogeneity is understandable in light of the currently available studies included in our meta-analysis. These studies included heterogeneous patient populations (with active GO, nonactive GO, patients with risk factors only, and patients without known eye disease), and used multiple treatment regimens (Table 2). While several tools are available to evaluate for severity and activity of GO (CAS, measured proptosis, diplopia assessment, etc.), there is not a single tool that comprehensively describes GO disease status. Our goal was to stratify patients according to both severity of structural disease and disease activity, but most outcome data from included studies stratified patients only according to the presence or absence of preexisting GO, with most treated patients having some degree of active disease. Although grouping according to preexisting GO may not represent the full complexity of GO pathology, it reflects the currently available data and is effective in guiding clinical decision making.
In agreement with previously published studies and one meta-analysis, we found a high risk for GO progression following RAI in patients with preexisting GO (25%), and a much lower risk in patients without known eye involvement, with or without risk factors (6%) (3 –7). In patients with preexisting eye disease, who are at a high risk for progression, the risk was reduced from 25% to 4% by the use of prednisone or prednisolone (Table 3). However, in patients who had no preexisting GO in whom the risk of de novo GO development is relatively low, a larger sample size is required to prove the efficacy of preventive treatment. For example, to prove a 50% risk reduction in patients who have no preexisting GO, a sample size of approximately 300 patients is required. Therefore, current recommendations on preventive treatment for patients, who do not have GO but have risk factors for progression, is supported by limited evidence, and are mostly based on expert opinion and our understanding of the disease.
This group includes patients both with and without risk factors for GO occurrence.
RCT, randomized controlled trial.
While treatment with GCs is effective in preventing GO progression following RAI, it is not risk-free. The recommended dose of 0.4–0.5 mg/kg for three months may cause significant side effects, including elevated blood glucose levels, hypertension, weight gain, mood changes, and acne, among others. Thus, assessment of the risk–benefit ratio should be performed for each patient, considering the treatment alternatives for hyperthyroidism. For patients with preexisting GO who failed medical treatment and who are otherwise healthy, treatment with RAI with concurrent GC prophylaxis is reasonable and evidence-based. However, in patients who are at risk for GC-related side effects (patients with metabolic syndrome, mental disease, etc.), an individualized risk assessment should be performed, weighing the risk of GO progression according to GO severity and activity versus the risk for GC-related adverse effects. The use of low-dose prednisone or referral to thyroid surgery can be effective options in these cases.
Our systematic review is limited by several factors. First, most studies did not clearly define preexisting GO, which may include both active and inactive disease. While most included patients had active disease according to CAS scores and as described in the text, it is unclear whether these conclusions can be generalized to patients with inactive GO given previous studies showing low risk for progression in patients with inactive disease (21). Further studies should evaluate the value of GC prophylaxis in patients with inactive disease, and especially in patients with long duration of disease who have lower risk of activation (9). Second, studies included in our meta-analysis provided insufficient data regarding risk factors for GO occurrence and progression. Smoking and post-RAI hypothyroidism are known risk factors for GO, whereas a high TRAb autoantibody titer is a known risk factor for GO progression (22 –24). Currently, the role of GC prophylaxis in patients with risk factors who do not have preexisting GO remains unclear. Moreover, previous studies have shown that post-RAI hypothyroidism may contribute to GO progression, which was prevented or blunted by early administration of levothyroxine (21). We have no data regarding this risk factor, which may have affected the risk of GO progression or the efficacy of steroid therapy. Third, most trials evaluated multiple outcome measures, without a clear definition of a primary outcome. This, in combination with the relatively small sample sizes, increased the risk for alpha-type errors of finding false statistical differences between treatment groups. Finally, the natural history of GO is incompletely defined, and may remit or improve spontaneously, which might affect results in an unpredictable manner (25,26). The use of a meta-analysis may partially overcome the methodological difficulties mentioned above by enlarging the sample size.
In conclusion, current evidence supports a three-tier, risk-adjusted approach for prevention of GO progression. Standard dose prednisone (0.4–0.5 mg/kg tapered over three months) is the best validated regimen and should be used in patients with mild to moderate GO who have high risk of progression, while low-dose prednisone (0.2–0.3 mg/kg tapered over four to five weeks) can be used in patients with mild GO and in patients without preexisting GO who have risk factors and are selected for GC prophylaxis. Future research should further substantiate the efficacy of low-dose prednisone, and evaluate the role of GC prophylaxis in patients with risk factors for GO development and in patients with inactive GO.
Footnotes
Acknowledgments
We would like to thank Prof. Mario Vaisman and Dott.ssa Guia Vannucchi for kindly providing additional information regarding their studies, which were included in the meta-analysis.
Author Disclosure Statement
No competing financial interests exist.