
Abstract
Background:
Hyperfunctioning distant metastasis (HFDM) from differentiated thyroid cancer (DTC) is a rare entity. This study aimed to assess the outcomes of DTC patients presenting with HFDM after total thyroidectomy and radioactive iodine therapy.
Methods:
A total of 5367 DTC patients treated with 131I after total thyroidectomy were analyzed retrospectively from January 1991 to June 2013. Therapeutic efficacy was evaluated based on changes in serum thyroglobulin (Tg) and anatomical imaging changes in metastatic lesions. The relationships between survival time and several variables were assessed by univariate and multivariate analyses using the Kaplan–Meier method and Cox's proportional hazards model respectively.
Results:
Thirty-eight patients with HFDM from DTC were diagnosed, including four with hyperthyroidism, four with subclinical hyperthyroidism, and three with subclinical hypothyroidism. The remaining 27 were euthyroid. Of 25 patients with lung metastases, 84% (21/25) showed disappearance or shrinkage of lung nodules; of 24 patients with bone metastases, 66.67% (16/24) exhibited no obvious imaging changes in metastatic bone lesions after 131I therapy. Serum Tg decreased significantly in 81.58% (31/38) and increased in 18.42% (7/38) after 131I therapy. The 10-year survival rate of DTC patients with HFDM was 65.79% (25/38). Multivariate analyses identified age at occurrence of distant metastases (<45 years), only lung metastases, and papillary thyroid cancer (PTC; p=0.032, NA, and 0.043) as independent predictors of survival.
Conclusion:
The response of hyperfunctioning lung metastases to 131I treatment was better than that of non-hyperfunctioning lung metastases in DTC, while hyperfunctioning bone metastases responded similarly compared to non-hyperfunctioning bone metastases. Patients younger than 45 years at occurrence of distant metastases, those with only lung metastases, and patients with PTC had better prognoses.
Introduction
D
DTC is characterized by a slowly progressive course and has a 10-year survival rate as high as 80–95% (2). It usually remains localized to the thyroid gland, and distant metastases occur in a minority of patients, with reported rates of 4–15%. The most common site of distant metastases is the lung, followed by the bone (3,4). Among these, hyperfunctioning distant metastases (HFDM) from DTC after total thyroidectomy are rare, but can result in hyperthyroidism or euthyroidism (5,6). To the best of our knowledge, around 70 cases have been reported in the literature to date (6,7).
Because of their limited occurrence, HFDM from DTC have rarely been reported, mainly as case reports, and their management has not been clearly defined. The aim of this study was to review our experience of HFDM of DTC origin in a large referral center over the last 22 years to analyze the patient characteristics, treatments, and outcomes, and to improve our understanding of this rare entity.
Materials and Methods
Patients
Clinical data for 38 DTC patients with HFDM among a total of 5367 patients enrolled in this study from January 1991 to June 2013 were analyzed retrospectively (Table 1). Patients attended the Department of Nuclear Medicine of Shanghai Sixth People's Hospital, which is a major referral site for 131I treatment in China. The study was approved by the Institutional Review Board. All 38 patients underwent total thyroidectomy before 131I treatment, among whom 15 (39.47%) patients achieved total thyroidectomy after the first operation. The remaining 23 patients required two thyroid operations; they initially underwent thyroid lobectomy for primary DTC, but metastatic lesions were detected during follow-up and then completion thyroidectomy was performed before 131I treatment. Eleven (28.95%) patients underwent central neck dissection, 15 (39.47%) underwent central and lateral neck dissection, and 12 (31.58%) had no neck dissection. Pathological T status was T1 in 11, T2 in 6, T3 in 9, and T4 in 12 patients. Patients with evidence of metastatic disease at the time of or within 12 months of initial diagnosis were considered to have distant metastases at presentation. Distant metastases discovered >12 months after the first thyroid surgery were considered to be delayed distant metastases.
Cumulative 131I activity.
HFDM, hyperfunctioning distant metastases; fT3, free triiodothyronine; fT4, free thyroxine; TSH, thyrotropin; F, female; M, male; PTC, papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; PF, follicular variant of PTC; PR, palliative resection; POP, percutaneous osteoplasty; NO, no other treatment modality.
Diagnostic criteria for HFDM
The diagnosis of HFDM from DTC was established based on the residual thyroid tissue after total thyroidectomy, thyroid radioactive iodine uptake, clinical symptoms, thyroid function, free triiodothyronine (fT3), free thyroxine (fT4), thyrotropin TSH, serum thyroglobulin (Tg), and Tg antibody (TgAb) after more than 3–4 weeks of levothyroxine withdrawal, 131I whole-body scan (131I-WBS) after 131I therapy, 131I-single-photon emission computed tomography (SPECT)/computed tomography (CT), X-rays, CT, and magnetic resonance imaging (MRI).
The diagnosis of HFDM due to the overproduction of hormones by metastatic tissue must be based on the following criteria: (a) the existence of hyperthyroidism, subclinical hyperthyroidism, subclinical hypothyroidism, or euthyroidism after total thyroidectomy with at least 3–4 weeks of levothyroxine withdrawal; (b) exclusion of hyperfunctioning diffuse or nodular thyroid gland remnants; (c) low or absent thyroid radioactive iodine uptake in the residual normal thyroid; or no residual thyroid discovered by neck ultrasound after total thyroidectomy; (d) 131I-WBS demonstrates distant lesions with high 131I uptake, at least one imaging method (X-ray, CT, MRI, and 131I-SPECT/CT) showing distant metastasis. Serum Tg levels should also be taken into consideration. In our study, each identified patient met all the above criteria.
Treatment of metastatic disease and follow-up
131I therapy and follow-up
All patients ceased thyroid hormone medication and began a low-iodine diet more than 3–4 weeks before 131I therapy. Before patients received oral 131I, conventional examinations were done, including measurements of fT3, fT4, TSH, Tg, TgAb, and neck ultrasonography, radioactive iodine uptake, X-ray, CT scan, and MRI after 3–4 weeks of levothyroxine withdrawal. 131I-WBS and/or 131I-SPECT/CT fusion imaging was performed five days after 131I oral administration. The first oral dose of 3.7 GBq (100 mCi) of 131I was administered to ablate thyroid remnants. Oral doses of 131I with a standard activity of 5.55–7.4 GBq (150–200 mCi) were administered for the subsequent treatment of hyperfunctioning metastases. The treatment interval ranged from 4–12 months, and the treatment was repeated 3–13 times. The time interval between the first and last radioiodine treatment showed a mean of 19.6 months (1–8 years) and the median follow-up period was 9.63 years (0.5–22 years).
Other treatments for bone metastases
Palliative resection prior to 131I treatment was performed in 10 patients with bone metastases who had orthopedic or neurological complications, or who were at high risk for such complications. External beam radiation therapy was delivered to one patient (case 24) with radiographically visible bone metastases. During 131I therapy, 9 of 38 patients received analgesics to control bone pain. Bisphosphonates, including zolendronic acid, were not used to treat bone metastases in this study. Percutaneous osteoplasty was performed to treat the osteolytic destruction of the left ilium in one patient (case 19).
Evaluation of therapeutic efficacy
The therapeutic effects of 131I were evaluated on the basis of the size of the metastatic lung nodules using CT and serum Tg under TSH stimulation. Lung nodule size was assessed according to the Response Evaluation Criteria in Solid Tumors (RECIST) (8). Serum Tg levels were measured using Roche (Roche Diagnostics GmbH, Mannheim, Germany) or Immulite (Diagnostic Products Corporation, Los Angeles, CA) chemiluminescent immunoassay system. Anatomical images were evaluated based on the responses defined by RECIST v1.1: complete response (CR), disappearance of all target lesions, any pathological lesions (target or non-target) must have a reduction in short axis to <10 mm; partial response (PR), ≥30% decrease in the diameters of target lesions; progressive disease (PD), ≥20% increase in the diameters of target lesions, combined with an absolute increase of ≥5 mm in the sum of diameters (the appearance of one or more new lesions was also considered progression); stable disease (SD), neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD.
The therapeutic effects of 131I therapy on bone metastases of DTC were evaluated based on two indicators, including changes in serum Tg levels and alterations in anatomical imaging of bone metastatic lesions. Anatomical images were evaluated using the methods established by MDA criteria (9): (a) CR: complete sclerotic fill-in of lytic lesions on X-ray or CT; normalization of bone density on X-ray or CT; normalization of signal intensity on MRI. (b) PR: development of a sclerotic rim or partial sclerotic fill-in of lytic lesions on X-ray or CT; interval visualization of lesions with sclerotic rims or new sclerotic lesions in the setting of other signs of PR and absence of progressive bony disease; ≥50% decrease in measurable lesions on X-ray, CT, or MRI; ≥50% subjective decrease in the size of ill-defined lesions on X-ray, CT, or MRI. (c) SD: no change; <25% increase or <50% decrease in size of measurable lesions; <25% subjective increase or <50% decrease in size of ill-defined lesions; no new bone metastases. (d) PD: ≥25% increase in size of measurable lesions on X-ray, CT, or MRI; ≥25% subjective increase in the size of ill-defined lesions on X-ray, CT, or MRI; new bone metastases.
Statistical analysis
Data were analyzed statistically using SPSS Statistics for Windows v10.0 (SPSS, Inc., Chicago, IL) and SAS v13.0 (SAS Institute, Inc., Cary, NC). Kaplan–Meier survival analysis was applied to evaluate the effects of different variables on survival rates, and differences between groups were compared using log-rank tests. Multivariate analysis was performed to assess the relationships between survival time and several variables simultaneously using Cox's proportional hazards model.
Results
Patient characteristics
The clinical characteristics of the 38 patients with HFDM of DTC are summarized in Table 2. In our cohort of 5367 patients with DTC, 38 (0.71%) presented with HFDM. The median age of the 38 patients was 47.7 years (range 17–82 years), with 24 subjects ≥45 years of age and 14 subjects <45 years of age. The male:female ratio was 1:2.2. Twenty-three patients had follicular thyroid cancer (FTC), 11 had papillary thyroid cancer (PTC), and four had follicular variant of PTC. Distant metastases at presentation of DTC were discovered in 12 (31.6%) patients. These included six patients with bone metastases as an initial presentation of DTC, while the distant metastases in the remaining six asymptomatic patients (including three lung, two bone, and one lung combined with bone and mediastinum) were detected at first postsurgical 131I ablation. Delayed metastases in 26 (68.4%) patients were detected in the following 1.8–22.5 years (M=9.5 years) after first thyroidectomy. Among these 38 patients, four had hyperthyroidism (cases 7, 10, 17, and 35), four had subclinical hyperthyroidism (cases 13, 22, 29, and 33), three had subclinical hypothyroidism (cases 28, 30, and 38), and the remaining 27 were euthyroid after thyroid levothyroxine withdrawal for at least 3–4 weeks. Of the total 38 patients, four had weight loss, malaise, heat intolerance, insomnia, and hypoxia caused by hyperthyroidism, two of whom changed from hyperthyroidism to hypothyroidism after one course of 131I treatment; one became hypothyroid after two courses, and the remaining patient after four courses. The 34 patients with subclinical hyperthyroidism, subclinical hypothyroidism, and euthyroidism became hypothyroid after one course of 131I treatment. After repeating 131I treatment, no patient with HFDM lost responsiveness to 131I during the period of the study, but the ability of 131I uptake wore off on the 131I-WBS in 22 (57.9%) patents.
DTC, differentiated thyroid cancer.
Clinical features and distribution of metastases
Among all 38 patients, 14 (36.8%) were classified as having pulmonary metastases alone, with a mean of 12 lung metastases (range 3–18). Thirteen (34.2%) DTC patients only had bone metastases, with a solitary metastatic bone lesion in one case, and a mean of six bone metastases (range 1–17). Eleven patients (29%) had synchronous bone and lung metastases, including a mediastinal and a renal metastasis. The mean number of distant metastases was 12 (range 8–20), the mean number of lung metastases was 10 (range 4–18), and the mean number of bone metastases was four (range 1–9). Seventeen patients with distant metastases were asymptomatic while 21 had clinical symptoms relating to metastatic lesions, including 14 patients with bone pain, seven with pathologic fractures, five with spinal cord compression, three with breathing difficulties, and two with hemoptysis.
131I scintigraphic and radiological findings
Among the 14 patients with pulmonary metastases alone, 12 were diagnosed by lung CT and 131I-WBS after oral administration of 131I, and two were diagnosed by 131I-WBS combined with 131I-SPECT/CT. Among 13 patients with bone metastases alone, three cases were identified by puncturing or pathological results before total thyroidectomy, 10 were detected by 131I-WBS combined with other imaging modalities after oral administration of 131I (four were detected by 131I-WBS combined with CT, four by 131I-WBS combined with 131I-SPECT/CT, and two by 131I-WBS combined with MRI). Among the 11 patients with lung, bone, and/or other distant metastases, two were detected by bone pathological results and lung CT before total thyroidectomy, three by 131I-WBS combined with 131I-SPECT/CT after 131I treatment, and six by 131I-WBS combined with lung CT and bone MRI. In our study, other distant metastases such as liver and brain were not detected, and ectopic thyroid tissue (sublingual or thyroglossal thyroid tissue) was ruled out by post-therapy scans after treatment with 131I.
Responses to therapy
Among 25 patients with lung metastases, 84% (21/25) showed disappearance or shrinkage of lung nodules, including 10 patients (40%) with CR and 11 with PR. Of the 24 patients with bone metastases, 66.67% (16/24) exhibited no obvious anatomical imaging changes in metastatic bone lesions after 131I therapy. Serum Tg decreased significantly in 81.58% of patients (31/38), and increased in the remaining 18.42% of patients (7/38) after 131I therapy.
Group of patients with only lung metastasis
Among 14 patients with lung metastasis alone, the mean lung nodule size was significantly smaller before the last 131I treatment compared with before the initial 131I treatment. Seven patients presented with CR, with a reduction in nodule size from 11.4±6.5 mm to being undetectable on lung CT scan. In five patients with PR, the mean size of the lung nodules decreased on CT scan from 15.4±7.8 mm to 5.9±3.4 mm. Two patients exhibited SD. Serum Tg decreased from 567 ng/mL (range 234–1059) to 14 ng/mL (range 36–5.8) in the CR group, from 651 ng/mL (range 117–925) to 78 ng/mL (range 21–125) in the PR group, and from 893 ng/mL (307–1539) to 143 ng/mL (87–129) in the SD group.
Group of patients with only bone metastasis
Of the 13 cases with bone metastases alone, none obtained CR, one (7.7%) presented with PR, and nine (69.2%) exhibited SD. Bone metastases progressed in three patients (23.1%), indicating PD. Mean serum Tg levels fell from 324 ng/mL to 21 ng/mL in the patient with PR and from 1735 ng/mL (range 74–11,258) to 507 ng/mL (range 21–4652) in the SD group, and increased from 11,324 ng/mL (range 307–15,324) to 12,729 ng/mL (range 369–17,974) in the PD group.
Group of patients with lung, bone and other distant metastases
Of 11 patients with lung metastases, three presented with CR, with the size of the lung nodules decreasing from 9.3±4.5 mm to becoming undetectable on lung CT scan. In six patients who achieved PR, the lung nodules decreased on lung CT from 18.4±9.2 mm to 6.7±3.8 mm. Two patients exhibited SD. Of the 10 cases with bone metastases, no patients obtained CR or PR, seven presented with SD, and four exhibited PD. Mediastinal metastasis in case 6 and renal metastasis in case 25 showed SD. Serum Tg levels gradually declined in 63.64% (7/11) of these patients, changing from 2748 ng/mL (range 409–17,685) to 987 ng/mL (range 122–9467), and increased significantly in the remaining 36.36% (4/11), changing from 2147 ng/mL (range 578–12,493) to 4285 ng/mL (range 1032–16,794).
Survival rates and prognostic factors
The 10-year survival rates and prognostic factors in the 38 patients with HFDM are listed in Table 3. Distant metastasis–free survival was 0.5–22 years (median 13.6 years) at the end of the follow-up period. At the time of follow-up, 12 patients had died of metastatic lesions, and one had died of a traffic accident after a diagnosis of distant metastases from DTC. The remaining 25 patients were alive and disease free, giving a 10-year survival rate for DTC patients with distant metastases of 65.79% (25/38). Univariate analysis identified a significant association between the site of distant metastasis and 10-year survival rate (p=0.001; Fig. 1). However, there was no significant association between 10-year survival rate and sex, T stage, number of thyroid surgeries, pathological type, age at occurrence of distant metastases, presenting symptoms and whether distant metastasis as at presentation of DTC, or other treatment prior to 131I therapy (p>0.05; Table 3).
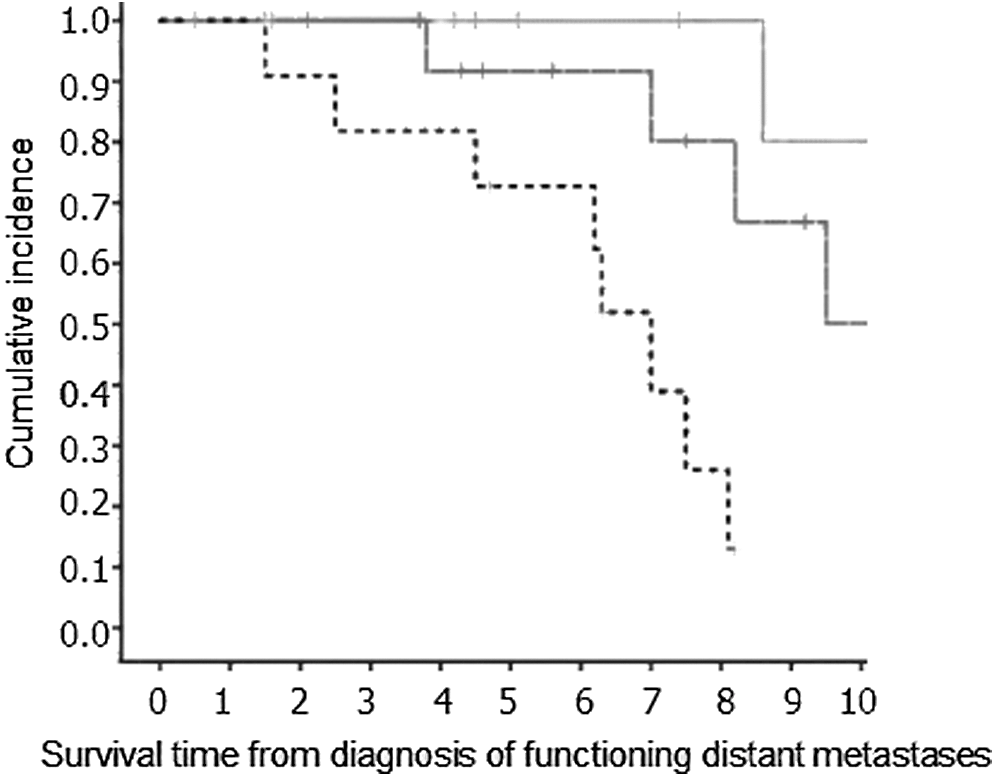
Comparison of survival curves between differentiated thyroid cancer (DTC) patients with only lung metastases (upper line), only bone metastases (middle line), and lung, bone, and/or other distant metastases (lower line).
Multivariate analyses to evaluate the simultaneous effects of variables on survival identified being aged <45 years at occurrence of distant metastases, only lung metastases, and PTC as independent factors associated with better prognosis (p=0.032, NA, and 0.043 respectively; Table 4). Other factors, including sex, T stage, number of thyroid surgeries, presenting symptoms and whether distant metastasis as at presentation of DTC, and other treatment prior to 131I therapy, were not prognostic factors (p>0.05).
Discussion
HFDM occurring in DTC is rare, and no studies have reported on the clinical management and outcomes of patients with HFDM from DTC. Most published studies have been either individual case reports or small case series of patients with hyperthyroidism or euthyroidism. DTC associated with distant metastases thus represents a challenge because of a lack of definitive clinical data. In the current cohort of 5367 patients with DTC, 38 (0.71%) presented with HFDM, including four with hyperthyroidism, four with subclinical hyperthyroidism, three with subclinical hypothyroidism, and 27 (71.05%) with euthyroidism after levothyroxine withdrawal for at least 3–4 weeks. The possible mechanisms responsible for HFDM in DTC are unclear. There are some potential reasons that might be involved in the rare situations where physiological or supraphysiological amounts of thyroid hormone are produced by HFDM. Thyroid-stimulating immunoglobulins, which could stimulate and increase the thyrotropin receptors (TSHR), may promote the growth of DTC cells, ultimately allowing metastatic tumors to function autonomously and synthesize thyroid hormones, thus causing the distant metastases to become functional (10 –12). Alternatively, some HFDM from follicular thyroid carcinoma can express 5′-iodothyronine deiodinase. When patients with these HFDM receive levothyroxine, it could increase the conversion of levothyroxine to T3 in the metastatic tumor tissues (13,14). In addition, activating mutations of the TSHR or the stimulatory guanine nucleotide-binding protein subunit (Gsα) in the primary tumor or metastatic lesions of DTC can lead to constitutive activation of the cyclic adenosine monophosphate-protein kinase A (cAMP-PKA) pathway and result in clinical and biochemical hyperthyroidism (15 –20). For example, Russo et al. described a 42-year-old female patient with an autonomously functioning Hürthle cell thyroid carcinoma causing thyrotoxicosis (18). The tumor contained a somatic gain-of-function mutation in the TSHR (L677V) (18). In another case, these authors identified a constitutively active TSHR mutation (A623V) both in the primary tumor as well as in a lung metastasis (15).
The median age of the 38 patients with HFDM was 47.7 years (range 17–82 years), which was lower than that reported in patients with non-HFDM from DTC by Sampson et al. (21) (M=68 years), and similar to the findings of Huang et al. (22) (M=46.4 years). Univariate analysis identified age as a strong predictive factor in all DTC patients with distant metastases, with younger patents (<45 years) having better cancer-specific survival rates than older patients (≥45 years) (4,21 –24). In this study, 24 of the subjects with HFDM in DTC were ≥45 years of age, and 14 were <45 years, with 10-year survival rates of 54.2% and 85.7% respectively. Being aged <45 years had a significant impact on survival, as identified by multivariate analysis, which supported the above finding that age is a strong predictive factor in DTC patients with non-HFDM in DTC.
FTC has been considered to be the most common type of thyroid cancer associated with this kind of hyperthyroidism to date (12,25 –28), and there have been few reports of hyperthyroidism caused by metastatic PTC or follicular variant of PTC (7,29,30). Girelli et al. noted a case of hyperthyroidism with a functioning pelvic metastasis of PTC (29), and Basaria and Salvatori described a 74-year-old man with conventional PTC with functional lung metastases causing severe hyperthyroidism complicated by Graves' disease (30). Lee et al. described a 49-year-old woman with metastatic clear cell variant of PTC who presented in a euthyroid state, despite having discontinued levothyroxine after undergoing a total thyroidectomy (7). In our study, the ratio of PTC with follicular variant to FTC was about 1:1.53. It showed that PTC was not extremely rarer than FTC in terms of HFDM in DTC, but PTC was associated with a better outcome, similar to previously reported outcomes in DTC patients with non-HFDM (4,22,24).
The most common sites of distant metastases from DTC are the lungs and bones (1). The site of metastasis has been reported to be a significant prognostic factor in DTC (5,31). This was in accordance with the findings of our study, which showed improved survival in patients with distant metastases limited to the lung, though the 10-year cause-specific survival was 92.9%, which was higher than in other studies. It is possible that this discrepancy may be because HFDM has an excellent avidity for 131I.
The presence of distant metastatic disease at presentation is relatively rare, with rates of 3–15%. In our series, the presence of distant metastatic disease at presentation was higher than that reported for non-HFDM in DTC (28,29). The 10-year survival rates of patients with distant metastases at presentation and delayed distant metastases were 75.0% and 61.5% respectively, indicating that the time of appearance of distant metastases did not significantly affect survival in patients with DTC. These results are higher than those reported by Shoup et al. (31), who found 10-year survival rates of 62% and 41% respectively, possibly because this study had a few patients who were not treated with 131I or who were not radioiodine avid on 131I treatment (5,21,22). Alternatively, this might also suggest differences in the studied populations (based on genetic or environmental factors), and/or in the screening methods used in the referral population of our Center, and/or in the clinical management of the patients after DTC diagnosis; all that affected the survival of DTC patents.
We evaluated the therapeutic efficacy of 131I therapy for distant metastases in DTC based on two indicators: changes in serum Tg, and alterations in anatomical imaging of metastatic lesions.
Among the 25 patients with lung metastases, no patients showed PD, 10 (40%) obtained CR, 11 achieved PR (44%), and four (16.67%) exhibited SD. Patient outcomes in this study were thus better than those of other reports of non-HFDM from DTC. Okamto et al. (32) reviewed 62 patients with lung metastases, including 28 131I uptake-positive and 31 131I uptake-negative patients. None of the 131I uptake-positive patients showed CR or PD, 21 presented with SD, and seven showed PR. These results suggest that hyperfunctioning lung metastases respond better to 131I treatment than non-hyperfunctioning lung metastases in DTC. Moreover, serum Tg levels in all these patients showed a gradual decline during the course of 131I treatment. This study also showed that CT provides a reliable method for evaluating response to 131I in DTC patients with hyperfunctioning lung metastases.
Of the 24 patients with bone metastases, none showed CR, one (4.1%) presented with PR revealed by MRI, 16 obtained SD (66.67%), and seven (29.17%) exhibited PD. The PR patient may be because the lesion was at an early stage and still remained small (33). Qiu et al. (3) reported imaging responses to 131I in 81 patients (76.4%) with non-hyperfunctioning bone metastases showing SD and in 22 patients (10.8%) showing PD, indicating that hyperfunctioning bone metastases responded less well to 131I treatment than non-hyperfunctioning bone metastases in DTC. These results also revealed that anatomical imaging (such as CT or MRI) cannot truly evaluate the efficacy of 131I therapy for DTC hyperfunctioning bone metastases.
Serum Tg is not only a highly sensitive and specific monitor of DTC metastasis and recurrence, but also reflects tumor burden (34). However, the detected values of Tg may be disturbed by TgAb, and we therefore measured serum levels of Tg and TgAb simultaneously in all patients. Although TgAb levels were increased to some extent as a result of stimulation by high serum Tg levels, serum Tg was pronouncedly elevated in DTC patients with HFDM, and serum Tg was obviously higher than serum TgAb. Therefore, changes in serum Tg may serve as an indicator of 131I treatment efficacy for HFDM. CT is a reliable method for evaluating 131I response in DTC patents with only hyperfunctioning lung metastases, but given that serum Tg was obviously decreased in these patients, Tg can be used as a secondary indicator measuring 131I treatment efficacy. In bone-only metastases, however, anatomical imaging (such as CT or MRI) cannot truly evaluate the efficacy of 131I therapy, and Tg may thus be the main indicator of 131I treatment efficacy in these patients. As far as bone and lung metastases are concerned, assessing the efficacy of 131I treatment for DTC is difficult: decreasing Tg in association with shrinkage or stable lung nodules by CT indicates effective bone metastasis treatment, while rising Tg in association with shrinkage or stable lung nodules by CT indicates ineffective bone metastasis treatment.
In summary, HFDM represents an extremely rare pattern of invasion from DTC with an incidence of 0.71%. PTC was not extremely rarer than FDC in terms of HFDM in DTC. Most HFDM patients (71.05%) keep euthyroid status after levothyroxine withdrawal before 131I treatment. Of the 38 patients with HFDM from DTC, 12 died of disease, one died of other causes, and the remaining 25 remained alive, giving a 10-year survival rate of 65.79%. The site of distant metastases, pathological type, and age at occurrence of distant metastases had major, independent impacts on survival. Lung metastases can be effectively treated by 131I, with a CR rate as high as 40%, which was better than the response of non-hyperfunctioning lung metastases in DTC. Bone metastases could be kept stable by 131I in most DTC patients (66.67%), which was similar to the situation seen in patients with non-hyperfunctioning bone metastases.
Footnotes
Acknowledgment
This study was sponsored by the National Natural Science Foundation of China (No: 81201115 & 81271611).
Author Disclosure Statement
None declared.