
Abstract

In 2009, the American Thyroid Association (ATA) for the first time explicitly recommended against postoperative radioactive iodine for well-differentiated thyroid tumors ≤1.0 cm without high-risk features (1). The recommendations for tumors ≥1.1 cm did not substantively change, effectively advising physicians' discretion and selective use. Use of radioactive iodine in patients with tumors ≤1.0 cm has not shown benefit, while the costs and harms of radioactive iodine may be significant. Haymart et al. (2) demonstrated that use of radioactive iodine increased over time for patients with all tumor sizes. Their sample included patients in the National Cancer Database (NCDB) treated through 2008. We examined the use of radioactive iodine before and after 2009 to determine whether the ATA guidelines influenced practice.
Following Haymart et al. (2), we used the NCDB to identify 160,976 patients who underwent total thyroidectomy for papillary, follicular, or Hürthle cell carcinoma during 2004–2011. We performed a quasi-experimental difference-in-differences analysis to assess whether there were differences in radioactive iodine use between the exposed group (patients with tumors ≤1.0 cm) and an unexposed group (patients with tumors ≥1.1 cm) before and after 2009. The amount of radioactive iodine used was not available. We excluded data from 2009 (n=24,305) to avoid misclassification of the timing of treatment relative to the guideline's release. The null hypothesis was that any temporal difference was due to trends affecting tumor sizes equally. We used linear regression because its estimates are directly interpretable in marginal probability terms (3). We clustered standard errors to account for intrahospital correlation.
We performed two sensitivity analyses. First, we limited the unexposed group to patients with tumors 1.1–2.0 cm to test whether the guidelines influenced the tumor size closest to the exposed group. Second, we excluded patients treated at hospitals that did not contribute data to the NCDB every year during 2004–2011 in case hospitals with different levels of radioactive iodine use joined or left the database (n=10,818).
The proportion of patients with tumors ≤1.0 cm receiving radioactive iodine dropped from 42% [CI 40–44%] before 2009 to 32% [CI 30–34%] after 2009, a decrease of 10 percentage points [CI 9–12] compared to tumors ≥1.1 cm, which dropped from 69% [CI 68–71%] to 68% [CI 66–69%], a decrease of 2 percentage points [CI 0–3] (difference-in-differences 8 percentage points [CI 7–10]; p<0.0001; Fig. 1). Results were comparable in sensitivity analyses comparing tumors ≤1.0 cm to tumors 1.1–2.0 cm (unexposed group pre to post: 4 percentage point decrease [CI 2–6]; difference-in-differences 6 percentage points [CI 4–8]; p<0.0001), and excluding patients from non-constant hospitals (p<0.0001).
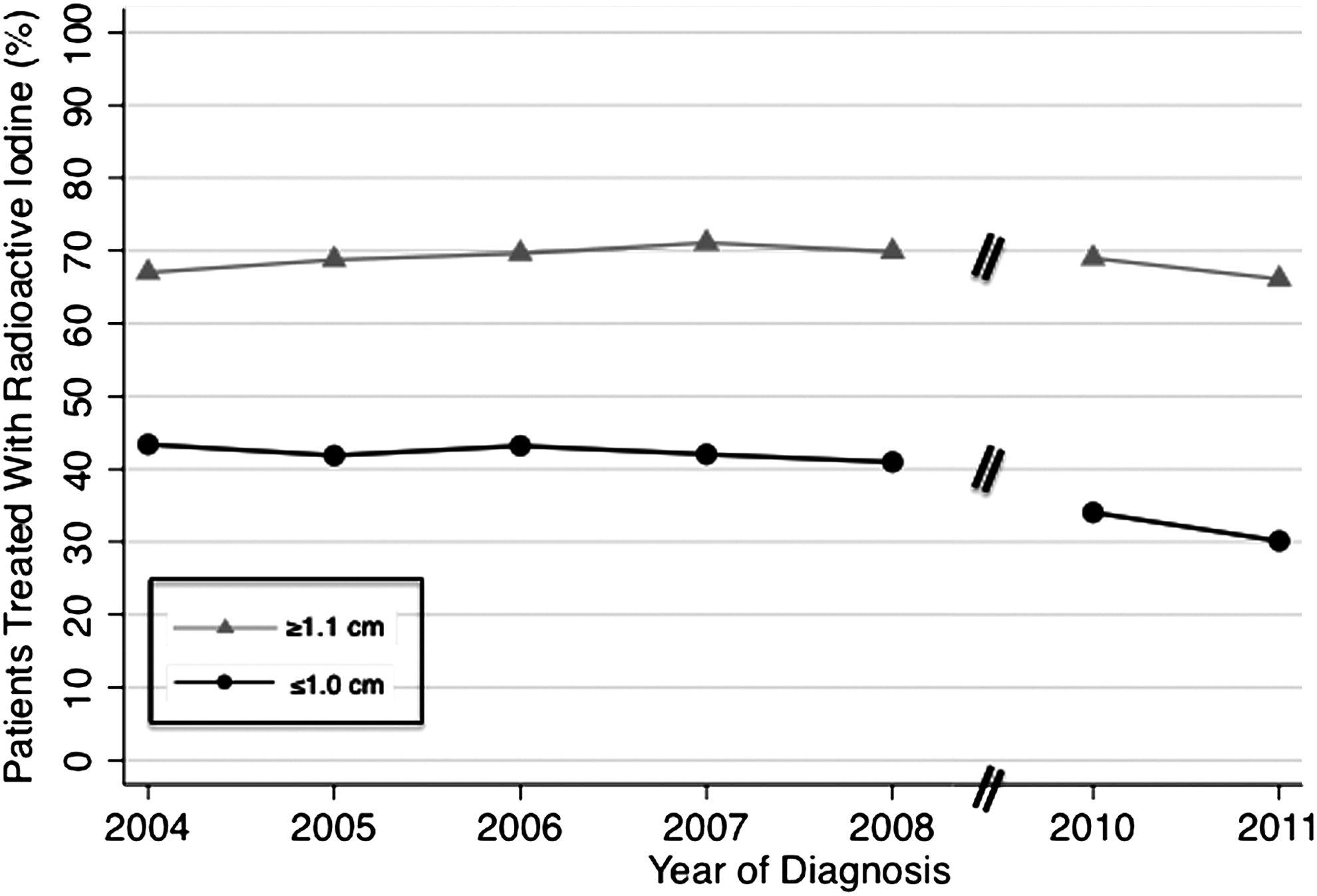
Percentage of patients treated with radioactive iodine according to tumor size; ≤1.0 cm vs. ≥1.1 cm. There were 50,339 patients with tumors ≤1.0 cm and 87,017 patients with tumors ≥1.1 cm (41,876 patients with tumors 1.1–2.0 cm, 32,675 patients with tumors 2.1–4.0 cm, and 12,466 patients with tumors >4.0 cm). For the primary analysis with control group of all tumors larger than 1.1 cm, there were 87,605 patients in the pre-period (2004–2008) and 49,751 patients in the post-period (2010–2011). For the sensitivity analysis with control group of tumors 1.1–2.0 cm, there were 57,758 patients in the pre-period and 34,457 patients in the post-period.
After publication of new guidelines in 2009, radioactive iodine use declined significantly for ≤1.0 cm tumors compared to larger tumors, suggesting that guidelines addressing overuse may play an important role in changing practice. This is important because most guidelines and quality measures address only what to do (4).
Despite decreased use, more than 30% of patients with tumors ≤1.0 cm were treated with radioactive iodine after 2009. Continued use may be driven by financial incentives, a lack of knowledge or disagreement with the guidelines (5), or continued belief that the service has benefit (6). For example, although there is no evidence of improved outcomes, beliefs may persist that benefit may be derived from ablating remnant thyroid tissue to improve the sensitivity of surveillance thyroglobulin or 131I scans, and from the possibility of ablating occult lymph node or distant micro-metastases.
Given this debate, further reductions in use may require multimodal efforts, including changes in reimbursement and additional evidence examining the benefit of radioactive iodine for ≤1.0 cm tumors. Additional guideline implementation strategies could also be employed. Since post-publication dissemination efforts are often complex, costly, and ineffective, future efforts to improve adherence to guidelines should focus on improving the implementability (e.g., usability, perceived validity, clarity, applicability, and communicability) of the recommendations (7).
Using observational data entails important limitations, including the omission of potentially relevant information about indications for radioactive iodine. In addition, causation between guideline publication and changing practice patterns cannot be proven. Finally, two years of post-guideline data may underestimate the effect, since practice is known to change slowly (8). Nevertheless, our analysis offers some hope about physicians' willingness to reduce overuse when guideline recommendations are made clear.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest.