
Abstract
Background:
Genetic mutations have been found to be associated with thyroid cancer. Previous studies have been focused on the relation between genetic mutations and thyroid cancer. We sought to evaluate the prognostic value of the three most common genetic mutations (BRAF, RAS, and RET) in patients with thyroid cancer.
Methods:
Sources from MEDLINE (inception to December 2013) and EMBASE (inception to December 2013) were searched. Studies of thyroid cancer with results of genetic mutations and studies that reported survival data were included and two authors performed the data extraction independently. Any discrepancies were resolved by a consensus.
Results:
Fourteen studies assessing BRAF mutations, 6 RAS mutations, 4 RET mutations, and 1 with analysis of both BRAF and RAS mutations were included in this meta-analysis. Patients with papillary thyroid cancer with BRAF mutations showed a 1.59-fold higher risk of events or a 2.66-fold higher risk of death than patients with papillary thyroid cancer without a BRAF mutation. Also, patients with RAS mutations showed a 2.90-fold higher risk of death by thyroid cancer than patients without a RAS mutation. In addition, patients with medullary thyroid cancer with RET mutations showed a 5.82-fold higher risk of death by the disease than without a RET mutation.
Conclusions:
Genetic mutations should be considered as a poor prognostic marker in thyroid cancer and may lead to better management of individual patients. However, the use of genetic mutations as prognostic markers should not be generalized, but individualized in the specific clinic setting.
Introduction
T
Thyroid carcinomas commonly contain one of a small number of recurrent genetic mutations (4). Previous studies revealed the pathogenetic, diagnostic, prognostic, and therapeutic roles of these mutations in thyroid tumors. These mutations have emerged as promising prognostic factors for thyroid cancer. Much effort has focused on identifying the association between genetic mutations and the outcome of thyroid cancer. However, the clinical significance of mutations as potential prognostic markers in papillary thyroid cancer (PTC) remains controversial, and scientific debate is ongoing (5). Previous meta-analyses (6 –8) revealed an association between BRAF mutations and the clinical outcome of PTC. However, these studies have several limitations, and no studies regarding the prognostic value of RAS and RET mutations have been performed. Therefore, we performed a meta-analysis to assess the prognostic value of the three most common genetic mutations (BRAF, RAS, and RET) in patients with thyroid cancer.
Materials and Methods
Data search and study selection
We performed a systematic search of MEDLINE (from inception to December 2013) and EMBASE (from inception to December 2013) for English-language publications using the keywords “thyroid,” “BRAF,” “RAS,” “RET,” and “prognosis.” All searches were limited to human studies. The inclusion criteria were studies of thyroid cancer that reported the results of genetic mutations and survival data. Reviews, abstracts, and editorial materials were excluded, and duplicate data were removed. If there was more than one study from the same center, the report with the information most relevant to this study was included. Two authors performed the searches and screening independently, and discrepancies were resolved by consensus.
Data extraction and statistical analysis
Data were extracted from the publications independently by two reviewers, and the following information was recorded: first author, year of publication, country, genetic mutation analyzed, number of patients, staging, mutation rate, and end points. The primary outcome was event-free survival (EFS). Data regarding disease-free survival (DFS), recurrence-free survival (RFS), disease-free interval (DFI), and progression-free survival (PFS) were obtained from the included studies, and were redefined as EFS, which was measured from the date of initiation of therapy to the date of recurrence or metastasis (9). The secondary end point was disease-specific survival (DSS), which included tumor-specific survival (TSS), cause-specific survival (CSS), papillary thyroid cancer-related mortality (PRM), survival from cancer (SFC), death from thyroid cancer (DFT), and tumor-related death (TRD). Only deaths from disease were included in DSS. The tertiary outcome was overall survival (OS), which was defined as the time from the initiation of therapy until death from any cause.
The effects of genetic mutations on survival were assessed using hazard ratios (HRs). Survival data were extracted following a methodology suggested previously (10). A univariate HR estimate and 95% confidence intervals (CIs) were extracted directly from each study, if provided by the authors. Otherwise, p values of the log-rank tests, 95% confidence intervals, numbers of events, and numbers of patients at risk were extracted to estimate the HR indirectly. Survival rates calculated from Kaplan-Meier curves were read using Engauge Digitizer version 3.0 (
Results
Study characteristics
The electronic search identified 2,128 articles. Non-English–language articles (n=172), conference abstracts (n=687), and 846 studies that did not meet the inclusion criteria based on their title and abstract were excluded. After reviewing the full text of 102 articles, 25 studies including 5,854 patients were eligible for inclusion in the study. The detailed procedure is shown in Figure 1.
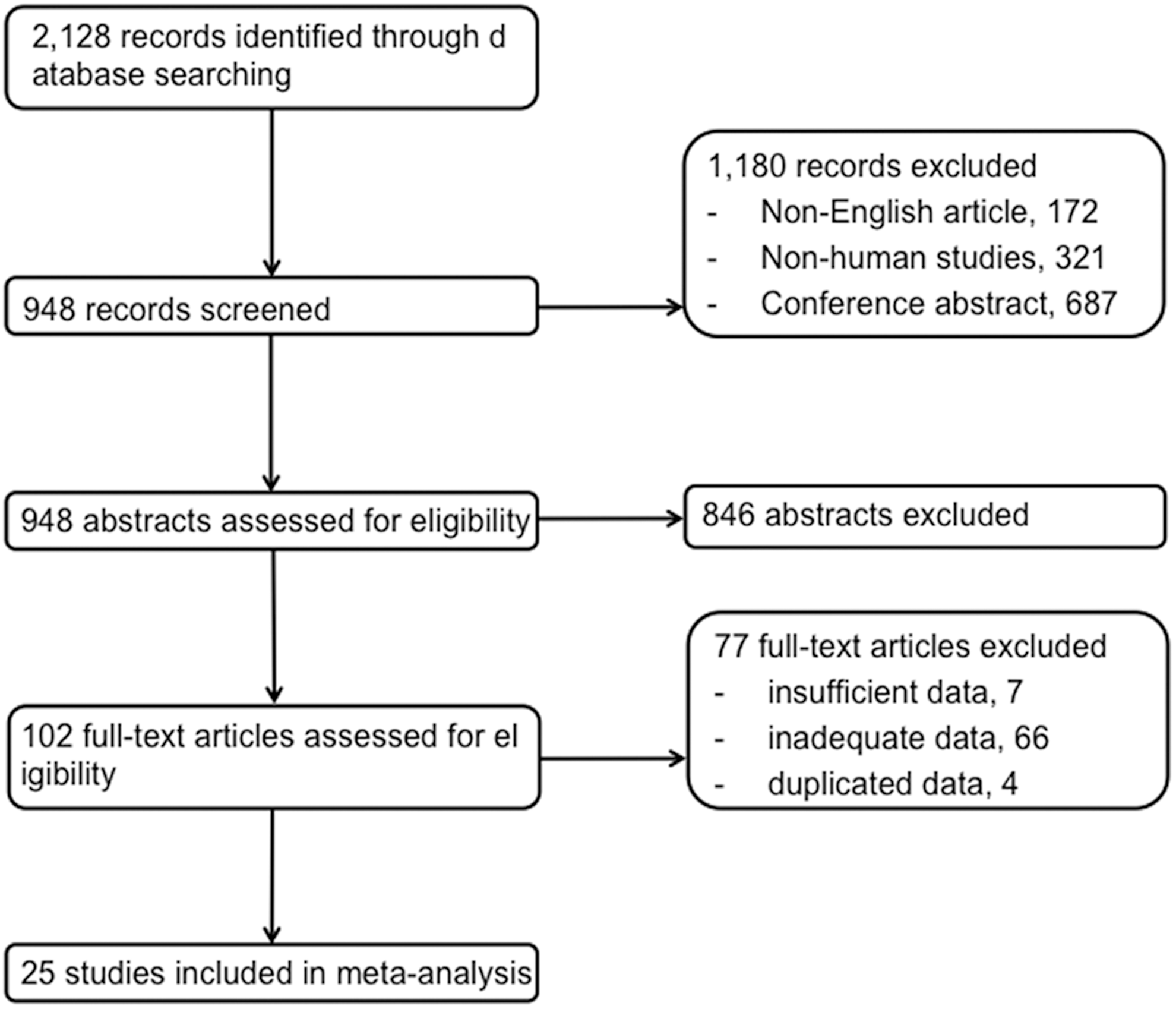
Flowchart of the study selection process.
Fourteen studies assessing BRAF mutations (13 –26) six with RAS mutations (27 –32), four analyzing somatic RET mutations (33 –36), and one reporting both BRAF and RAS mutations (37) were included in the meta-analysis. The prognostic value of BRAF mutations was assessed by analyzing DSS in 2,913 patients and EFS in 2,264. The prognostic potential of RAS mutations was analyzed according to DSS, EFS, and OS in 294, 173, and 131 patients, respectively. The prognostic value of RET mutations was assessed according to DSS in 300 individuals. The percentage of patients with the mutation in each study ranged from 36.7–73.4 for BRAF, 14.3–56.9 for RAS, and 16.0–61.8 for RET. All studies of BRAF mutations included patients with PTC (13 –26,37). Patients with MTC were included in three of four studies analyzing RET mutations (33,34,36). Visual inspection of the funnel plot suggested no evidence of publication bias. The study characteristics are summarized in Table 1.
Follow-up; amedian, bmean.
PRM, papillary thyroid cancer-related mortality; TSS, tumor-specific survival; CSS, cause-specific survival; PFS, progression free survival; DFI, disease-free interval; DSS, disease-specific survival; DSD, disease-specific death; SFC, survival from cancer; DFT, death from thyroid cancer; TRD, tumor-related death; PDTC, poorly differentiated thyroid cancer; ATC, anaplastic thyroid cancer; MTC, medullary thyroid cancer.
BRAF mutations
All patients included in the meta-analysis of BRAF mutations had PTC. EFS was analyzed based on 12 studies (13 –18,20,21,23 –25,37). The pooled HR for adverse events was 1.59 (95% confidence interval [CI] 1.24–2.04, p=0.0002), and the test for heterogeneity gave no significant results (χ2=14.49, p=0.21; I2=24%). Subgroup meta-analyses were assessed according to region (European, Korea/Japan, United States, and others), number of patients (<100, ≥100, <200, and ≥200), patient age (<45 and ≥45 years), the prevalence of BRAF mutations (<50 and ≥50%), and follow-up period (<60 and ≥60 months) (Table 2). Studies with a BRAF mutation rate <50% had a HR of 1.81 (1.12–2.93, p=0.02), whereas those with a BRAF mutation rate ≥50% had a HR of 1.52 (1.14–2.03, p=0.004). The effect sizes of HRs were similar among the subgroups analyzed. DSS was analyzed based on four studies (19,22,26,37), and the combined HR for deaths from thyroid cancer was 2.66 (1.34–5.27, p=0.005). The forest plots for EFS and DSS are shown in Figure 2.
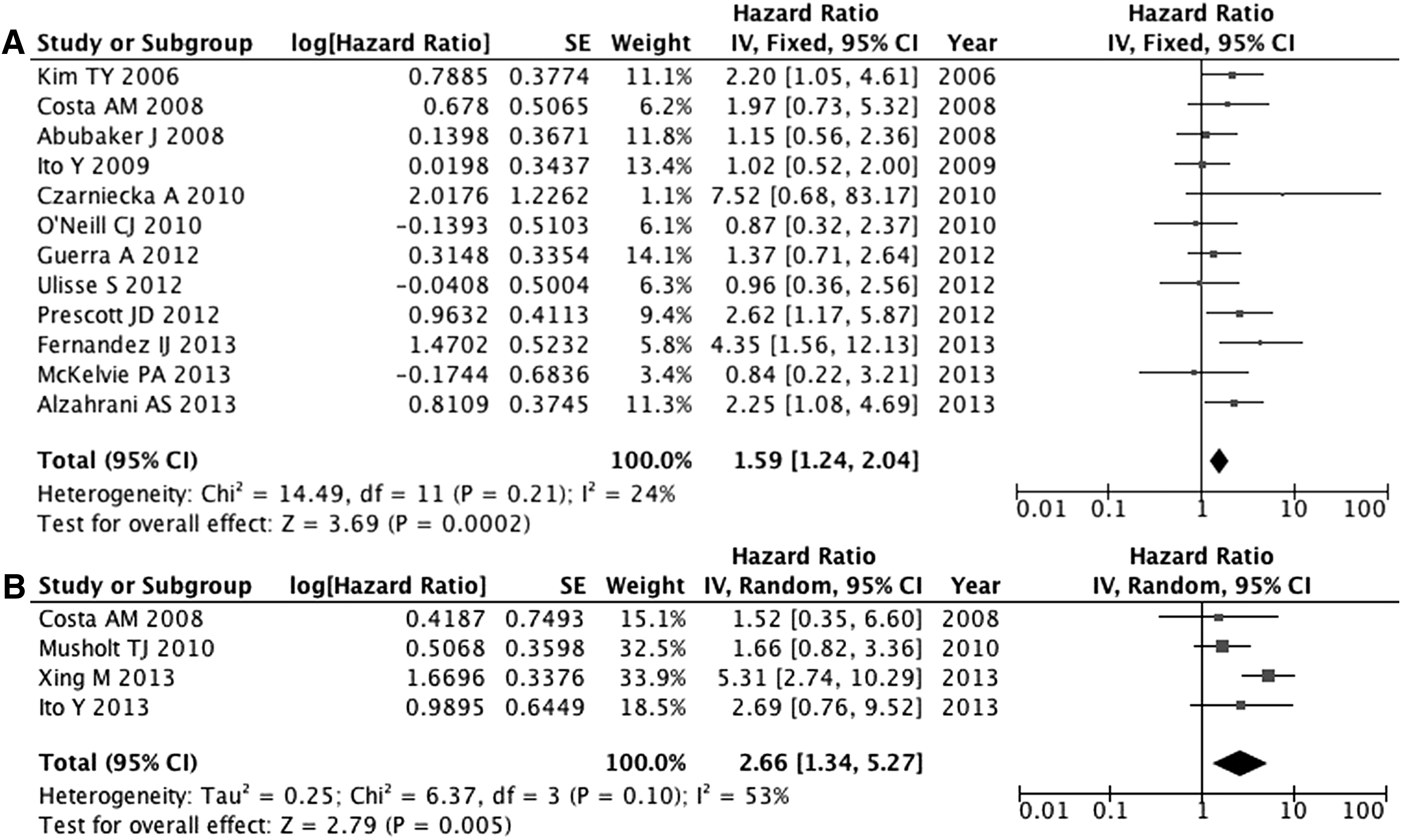
Forest plots of the hazard ratios for events
EFS, event-free survival; HR, hazard ratio; CI, confidence interval.
RAS mutations
Two studies (27,37) analyzed EFS in 173 patients, and three studies (28,31,32) containing 131 patients that reported OS were included to calculate the combined HRs. However, RAS mutations were not associated with an increased risk of events (HR 1.80; 0.95–3.43, p=0.07) or a higher risk of death from any cause (HR 2.18; 0.45–10.64, p=0.33). To measure the HR of DSS, three studies containing 294 patients were included (27,29,30). The combined HR of deaths from thyroid cancer was 2.90 (1.66–5.07, p=0.0002). The forest plots for EFS, OS, and DSS are shown in Figure 3.
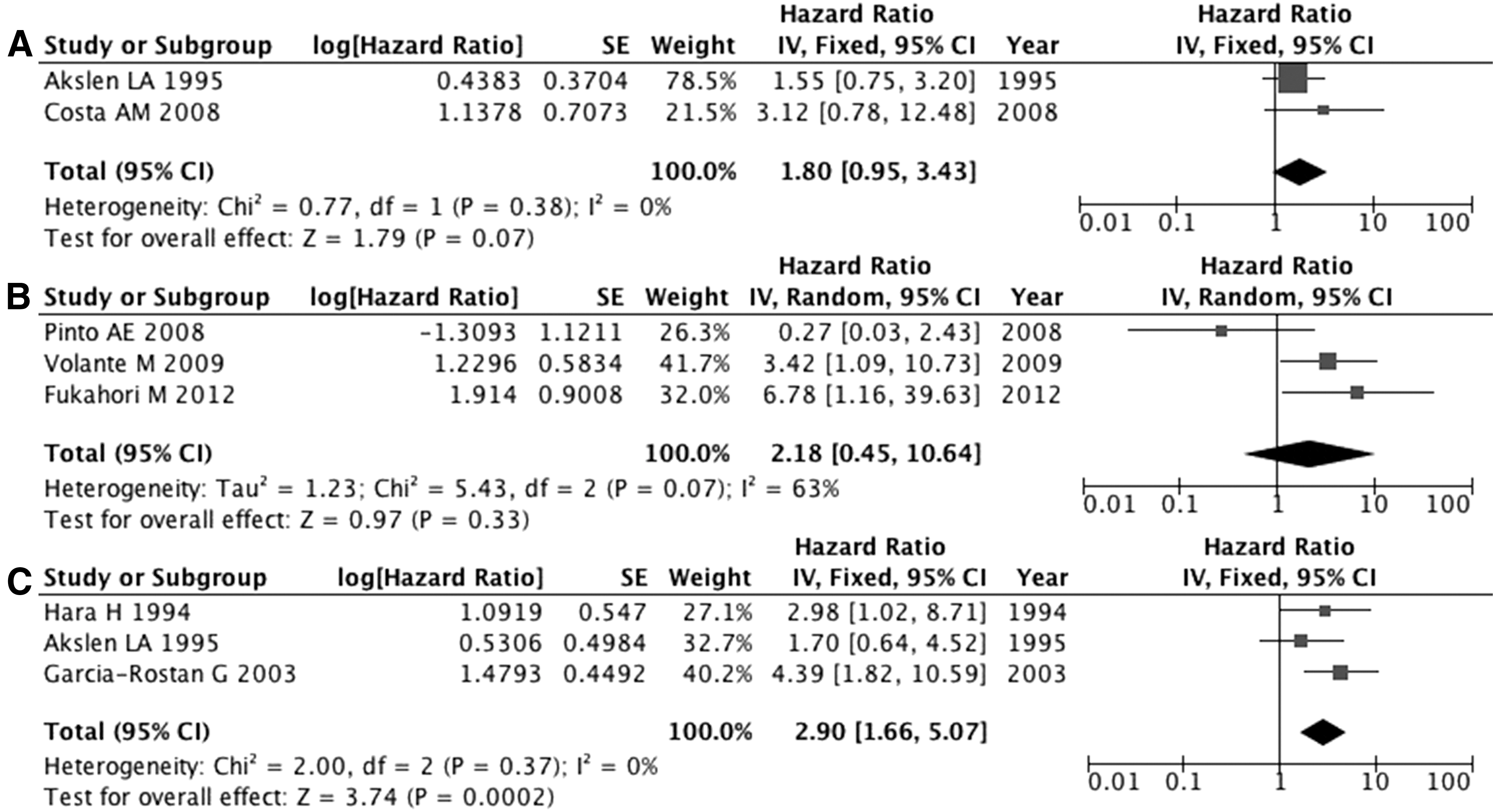
Forest plots of hazard ratios for events
RET mutations
DSS was analyzed based on four studies including 300 patients (33 –36). After excluding one study of patients with PTC (35), three studies analyzing MTC showed a combined HR of 5.82 (2.53–13.38, p<0.0001). The forest plot for DSS is presented in Figure 4.

Forest plots of the hazard ratio for death from thyroid cancer in patients with RET mutations.
Discussion
This meta-analysis evaluated the prognostic value of genetic mutations in patients with thyroid cancer. In combined results, PTC patients with BRAF mutations had a 1.59-fold higher risk of events and a 2.66-fold higher risk of death than those without BRAF mutations. In addition, patients with RAS mutations had a 2.90-fold higher risk of thyroid cancer-related death than those without a RAS mutation. Finally, MTC patients with RET mutations had a 5.82-fold higher risk of death due to the disease compared with patients without RET mutations.
The present study is consistent with recent meta-analyses reporting that BRAF mutations are closely related to the presence of high-risk clinicopathologic factors and poorer outcome in patients with PTC (6 –8). Our results are compatible with a clinical study reporting that preoperative knowledge of BRAF mutations might alter the initial PTC surgical management strategy, and also prevent the increased rate of morbidity that has been associated with preoperative neck exploration (38). An explanation for the role of BRAF mutations in PTC-related mortality lies in the molecular mechanisms by which BRAF mutations promote the aggressive pathogenesis of thyroid cancer. For example, BRAF mutations cause the dedifferentiation of PTC, resulting in the loss of expression of the thyroidal genes that regulate thyroid iodide concentration and hence the failure of radioiodine treatment (7,39). BRAF mutations also strongly upregulate several classic angiogenic and tumor-promoting molecules, and are associated with the hypermethylation and inactivation of tumor suppressor genes (7,39). It is likely that, through these unique molecular mechanisms, BRAF mutations promote aggressive tumor behavior such as lymph node metastasis (LNM), tumor invasion, distant metastasis, silencing of thyroidal genes involved in iodide handling thereby rendering tumors resistant to radioiodine treatment, and expedite tumor progression. In combination, these effects increase the risk of PTC-related mortality. However, the presence of a BRAF mutation cannot be interpreted independent of tumor behaviors that can affect patient mortality. In fact, when Xing et al. (26) adjusted for these tumor behaviors, the association of outcomes with the presence of a BRAF mutation was no longer statistically significant. These results from Xing et al. (26) are consistent with another study (20) demonstrating that the presence of a BRAF mutation has a significant impact on PTC-related deaths in high-risk categories.
The current study also reveals that patients with RAS mutations had a 2.90-fold higher risk of death due to thyroid cancer. Constitutively activating RAS mutations are probably the most common mutations in cancer biology (4). Previous studies revealed correlations between RAS mutations and bone metastases, increased aggressiveness, and higher mortality in all types of thyroid cancer (27,29,30,40). A retrospective study also found that RAS mutations are overrepresented in differentiated thyroid carcinomas in patients with radioiodine-avid pulmonary metastases (41). Radioiodine-avid lung metastases are rarely cured by radioiodine therapy, resulting in a impaired prognosis. PTCs usually contain an activating mutation in the RAS/MAPK cascade: most commonly in BRAF, and less frequently in RAS. A recent study (42) reported that the rapid increase in thyroid cancer incidence over the last four decades was accompanied by an increased frequency of BRAF mutations and a marked increase in RAS mutations. Consistent with this finding, we confirm the prognostic value of BRAF and RAS mutations in patients with PTC. The current study is the first meta-analysis of the prognostic value of RAS mutations in thyroid carcinoma. The association of BRAF and RAS in thyroid cancer combined with the diverse effects of BRAF/RAS presents many potential therapeutic targets.
The current meta-analysis also found that MTC patients with RET mutations had a 5.82-fold higher risk of death. RET is a cell–surface receptor tyrosine kinase that transmits environmental cues to RAS and the downstream MAPK pathway. RET itself is not expressed in normal thyroid follicular cells, but the juxtaposition of the two kinase domains of RET and its promoter leads to the expression of a fusion oncoprotein and aberrant kinase activity (4). The biologic behavior of MTC is much less favorable compared with other well-differentiated thyroid carcinomas (43). Currently, the only effective clinical tools for gauging the progressive or stable nature of an MTC tumor are the calcitonin and carcinoembryonic antigen doubling times during follow-up (43). Previous studies demonstrated that RET gene mutations, which are present in approximately 40–50% of MTC tumors, are a poor prognostic factor for the outcome of MTC patients (33,34,36). However, this observation was not confirmed by several other reports (44,45). These analyses were performed in small MTC series with short-term follow-ups. In addition, the data were not always homogeneous in terms of the frequency, type, and site of the somatic RET gene mutation, or their association with clinical and pathologic features. Our data confirm that somatic RET mutations are molecular markers of more aggressive MTC subtypes. This might facilitate the planning of appropriate surgical interventions, determination of the extent of surgery, and tailored patient follow-up from the beginning of treatment.
The major strength of this study consists in the fact that it is the largest meta-analysis performed to date that includes the most recent studies. We analyzed the association of the three most common genetic mutations and with the prognosis (EFS, DSS, and OS) of thyroid cancer patients, but not with clinico-pathological features. Six previous meta-analyses were identified by searching the electronic MEDLINE and EMBASE databases (Table 3). Each study analyzed the effect size of risk ratios (RRs) or odds ratios (ORs). However, because RRs or ORs are measured at a single point in time, they are not recommended as surrogate methods for analyzing time-to-event outcomes (46); instead, HR is the most appropriate measurement. Therefore, we calculated HRs as the effect size in the current study. Nevertheless, this study also has several limitations. Because we were unable to access individual patient data, there is a risk of bias. Studies with different treatments, follow-up periods, and surveillance protocols were included in this study, which is a weakness for meta-analysis. Although funnel plots did not reveal clear evidence of publication bias, it could not be excluded. In addition, even though two reviewers read survival curves independently, this strategy could not ensure complete accuracy of the extracted data. Finally, although we included studies of RAS mutations, we were unable to subanalyze these according to RAS isoforms due to the insufficient number of studies.
PTC, papillary thyroid cancer; LN, lymph node; EE, extrathyroidal extension.
Cancer is a disease of accumulated DNA damage the progression of which is in part driven by the acquisition of additional genetic abnormalities. Understanding how these changes contribute to the disease process is essential for the development of novel prognostic and therapeutic strategies. Targeting these recurrent mutations singly can result in transient relief from disease progression. Combination therapies that address a more comprehensive catalogue of driving mutations might achieve more durable responses, and perhaps cures. Finally, the epigenetic control of the tumor genome is also an attractive target for reversal of disease progression. In conclusion, genetic mutations should be considered to be poor prognostic markers in thyroid cancer; such knowledge might improve the management of individual patients. However, the use of a BRAF mutation or other mutations as prognostic markers should not be generalized, but individualized in the specific clinic setting. Further studies of risk assessment establishing strategies for aggressive postoperative therapies and follow-up are needed.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.