
Abstract
Background:
The aim of our study was to determine central compartment lymph node (LN) characteristics predictive of outcomes in patients with differentiated thyroid cancer (DTC) and pathologically confirmed positive central LNs, in the absence of lateral neck disease or distant metastases at presentation.
Methods:
An institutional database of 3664 previously untreated patients with DTC operated between 1986 and 2010 was reviewed. Six hundred patients with central compartment nodal disease on histopathology were identified. Patient demographics, number of positive LNs, size of largest LN, and presence of extranodal spread (ENS) were recorded for each patient. Variables predictive of recurrence-free survival (RFS) were identified using the Kaplan–Meier method. Univariate analysis was carried out by the log-rank test and multivariable analysis was carried out using cox proportional hazard model.
Results:
The median age of the cohort was 41 years (range 12–91 years). The median follow-up was 61 months (range 1–330 months). Neck recurrence occurred in 43 patients. Recurrence occurred in the central neck in 11 patients, lateral neck in 27 patients, and both compartments in five patients. Factors predictive of neck RFS on univariate analysis were higher T stage (p=0.007), increased number of positive LNs, increased LN diameter, and presence of ENS (p=0.001). Multivariable analysis of LN characteristics showed that the only statistically significant predictor of neck recurrence was the presence of ENS. Neck RFS at five years for patients with and without ENS was 84.7% and 94.5% respectively (p=0.001).
Conclusion:
The LN feature most predictive of neck recurrence appears to be the presence of ENS in the positive central neck.
Introduction
M
The aim of our study was to explore this topic further by determining central compartment LN characteristics predictive of recurrence outcomes in patients with DTC and pathologically confirmed positive central LNs. Size, number of positive nodes, and the presence of extranodal spread (ENS) were analyzed in a large data set of patients treated at a single institution.
Methods
Following approval by the Institutional Review Board, the records of 3664 consecutive patients treated surgically for DTC between 1986 and 2010 were identified from an institutional database. Six hundred pN1a patients on histopathology were identified for review. Patients who were treated at an outside facility prior to referral, had disease confined to the thyroid gland, had evidence of lateral compartment nodal disease, presented with distant metastasis, or were discovered to have distant metastases on postoperative RAI scan (within six months) were excluded from analysis. At our institution, we do not routinely carry out prophylactic central neck dissections but only dissect the central neck whenever nodes are found on palpation, on preoperative imaging, or during surgery. Therefore, the 600 pathologically confirmed patients with central compartment disease consist of patients having a central neck dissection for macroscopic LNs on clinical or radiologic examination. In addition, we also included patients with occult metastases found in perithyroidal LNs included in the thyroidectomy specimen, and included nodes found to be positive on node sampling.
Patient demographic information, surgical details, and histopathological details, including number of positive central LNs, size of largest positive LN, and presence of ENS, were recorded. LN diameter was defined as the diameter of the largest LN containing a focus of metastatic thyroid cancer. The presence of ENS was defined as tumor extension beyond the LN capsule. Details of postoperative use of radioactive iodine (RAI) therapy were recorded and postoperative thyrotropin (TSH) suppression was initiated based on individual risk of recurrence.
As this study includes patients with pathology reports from 1986 to 2010, LN features were not reported in all patients. Figure 1 shows the LN data available for analysis. To maximize statistical power, patients with one or more missing LN feature were censored for the analysis of that LN variable. To ensure there was no selection bias between patients with all LN features reported and patients with one or more missing LN features, Pearson's chi square test was performed comparing these two groups. No difference in sex, age, T stage, or histology was found (data not shown).

Inclusion criteria.
The primary outcome of interest was nodal recurrence-free survival (RFS). Neck LN recurrences were determined by clinical examination supplemented with imaging and fine-needle aspiration. Patients with biochemical recurrences defined by elevated thyroglobulin levels were not considered to be robust endpoints to measure nodal recurrence outcome. Prior to 2000, postoperative serum thyroglobulin (Tg) was not used to detect recurrence. The use of serum Tg measurements and serial ultrasounds has become standard practice at our institution since 2005, and now influence the further investigation of patients in this cohort. The median follow-up for the cohort was 61 months (range 1–330). Outcome data were therefore calculated at five years.
Statistical analysis was carried out using SPSS Statistics for Windows v21 (IBM Corp., Armonk, NY). Categorical cutoffs for size and number of positive LNs were based on frequently used cutoff from the literature as well as by receiver operating characteristic (ROC) curves. ROC curves were plotted for all LN number and size cut-points. The value at which sensitivity and specificity was maximized for nodal RFS was also selected for analysis. Pearson's chi-square test was used to compare variables within groups. Survival outcomes were analyzed using the Kaplan–Meier method. Univariable analysis was carried out by the log-rank test, and multivariable analysis was carried out using the Cox proportional hazard model. A p-value <0.05 was considered significant.
Results
The median age of the cohort was 41 years (range 12–91 years). The median time to regional nodal recurrence was 50.5 months (range 1–330 months). Nodal recurrence occurred in 43 patients. Recurrence occurred in the central neck in 11 patients, lateral neck in 27 patients, and both compartments in five patients. Distant recurrence developed in 10 patients, and disease-specific death occurred in five patients.
Predictors of neck RFS on univariable analysis
Factors predictive for neck RFS were increasing LN diameter and the presence of ENS (Table 1). Although T stage was predictive (p=0.007), sex, age, histology, and postoperative RAI administration were not predictive.
Bold indicates significant values.
RFS, recurrence-free survival; RAI, radioactive iodine.
LN diameter (n=446)
Patients with central LN micrometastases of ≤0.2 cm had similar five-year neck RFS compared to patients with LNs >0.2 cm (93.6% vs. 92.6%; p=0.603). At a LN cutoff of 0.75 cm, determined by ROC analysis, patients with LN≤0.75 cm had a small but statistically significant superior five-year neck RFS (96.8% vs. 90.2%; p=0.040). Similarly, patients with a LN diameter ≤1 cm and ≤2 cm had superior five-year neck RFS compared to patients with LNs >1 cm and >2 cm respectively (Table 1).
Number of positive LNs (n=597)
Comparison of five-year neck RFS for patients with three or fewer and more than three positive LNs (94.1% vs. 88.2%, p=0.043), five or fewer and more than five positive LNs (93.5% vs. 87.6%; p=0.070) as well eight or fewer and more than eight positive LN patients (93.5% vs. 80.7%; p=0.001; Table 1) showed a general trend toward poorer neck RFS with increasing number of positive central LNs. A cutoff of eight or fewer positive LN was determined by ROC analysis.
ENS (n=415)
A total of 23.4% of patients with N1a disease had evidence of ENS reported on histopathology. Patients with ENS had a significantly poorer five-year neck RFS survival compared to patients without ENS (84.7% vs. 94.5%; p=0.001; Table 1 and Fig. 2). When stratified by age >45 and <45 years, the presence of ENS remained significant in both age cohorts (p=0.044 and p=0.005 respectively).
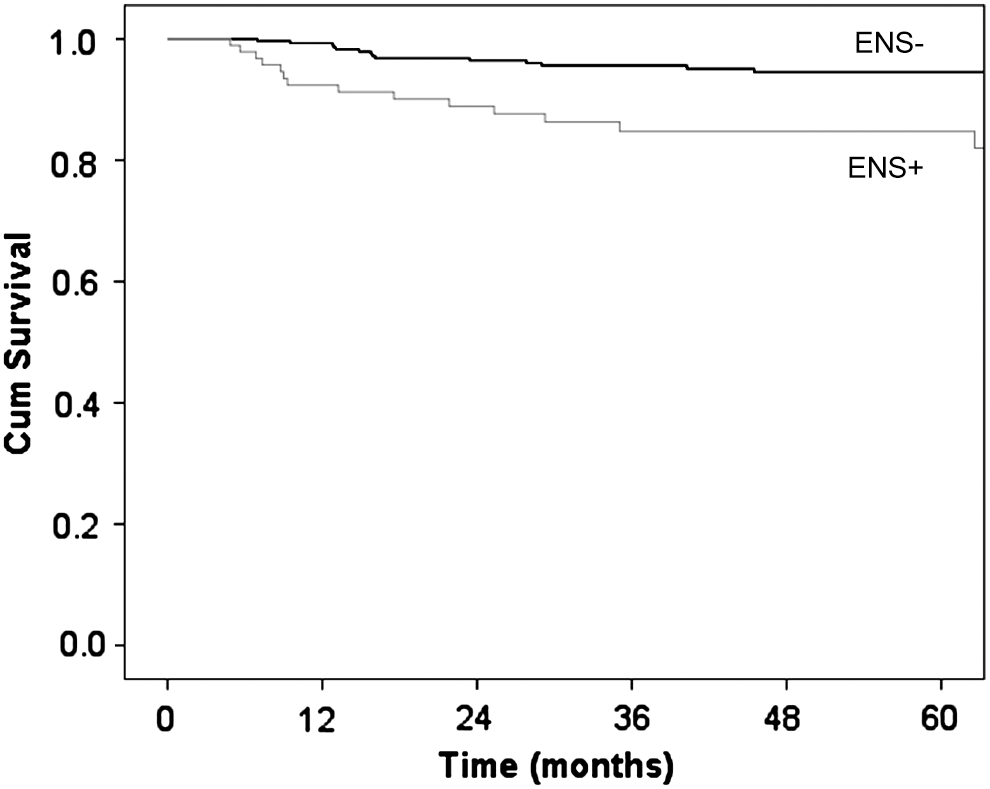
Neck recurrence-free survival in patients with and without extranodal spread.
Predictors of neck RFS on multivariable analysis
A total of 354 patients had all LN variables (maximal LN diameter, number of positive LNs, and ENS) available for analysis and were therefore included in the multivariable analysis of significant LN characteristics predictive for neck recurrence. We were limited to three variables for multivariable analysis due to the limited number of neck recurrences. Table 2 shows nine models of multivariable analysis of LN variables, including all combinations of LN diameters (<0.75 cm/≥0.75 cam, <1 cm/≥1 cm, and <2 cm/≥2 cm), number of positive LNs (three or fewer/more than three, five or fewer/more than five, eight or fewer/more than eight) and presence of ENS. In all nine models, the presence of ENS was independently predictive for neck RFS.
Bold indicates significant values.
CI, confidence interval; LN, lymph node; ENS, extranodal spread.
When we controlled for T stage, ENS remained a significant predictor for neck recurrence conferring a hazard ratio of 3.1 ([confidence interval (CI) 1.491–6.515], p=0.003).
Distant recurrence and disease-specific survival
No central compartment LN features were predictive of distant RFS or disease-specific survival (DSS) on univariable analysis.
Discussion
Metastases to the central compartment LNs (levels 6 and 7) in patients with DTC are common. In the majority of patients, these are subclinical micrometastases, and the prognostic significance of them is very controversial. Recent data suggest that the size and number of positive LNs are prognostic (4 –8). The American Thyroid Association recently published a detailed systematic review quantifying thyroid cancer nodal volume and its relationship to prognosis. In this review, it was recommended that patients be classified into “lower and higher risk N1” categories based on volume of nodal disease (9). The definition of micrometastases being ≤0.2 cm was based on data from breast cancer staging. No recommendation at the time was made for stratification of patients with evidence of ENS. To explore this controversial subject further, we sought to analyze our own results using a data set of 600 patients with central compartment nodal disease. We analyzed size of LNs, number of positive nodes, and the presence of ENS using this data set, and report that all three characteristics are significant. However, it is the presence of ENS that appears to be the most prognostic in the central compartment.
With regards to the size of the metastatic LN, several studies have reported larger LN size and metastatic foci diameter to be prognostic in DTC. Ito et al. have published several studies on the prognostic implications of central neck metastatic LN size in papillary thyroid cancer (4,10). That group reported on 626 patients with papillary thyroid cancer >1 cm undergoing prophylactic central neck dissection with or without lateral neck dissection. On multivariable analysis, in addition to other predictors, central LN features associated with a significantly worse RFS were LN diameter >1.5 cm and more than 10 positive LNs (4). In a similar study by Sugitani et al., patients with papillary thyroid cancer >1 cm with central and/or lateral neck disease were examined. Multivariable analysis suggested that LN metastases >3 cm were predictive of DSS and RFS in patients aged 50 years or older but not in younger patients (5). In a case control study by Yamashita et al., large LN deposits >1 cm in size as well as ENS were significantly higher in the metastatic group on univariable analysis. LN size, however, was not significant on multivariable analysis when controlling for other LN variables. A more recent study reported central LN metastases of >0.2 cm to be prognostic of recurrence. However, presence of ENS was not controlled for in this study (8). Data from this current study suggest that increasing size of positive central compartment LNs is associated with a trend toward poorer RFS: 96.1% for those with LNs≤0.75 cm in contrast to 75.8% for patients with LN >2 cm (Table 1). However, at no size was LN diameter independently predictive of nodal recurrence when controlling for presence of ENS (Table 2).
Many international groups have also reported on the prognostic significance of increasing number and ratio of positive LNs in DTC. The cutoffs considered to be prognostic have differed significantly between groups from more than two positive LNs in the central or lateral compartment (6) to more than five LNs in younger but not older patients (5). Others have found >10 LNs in the central or lateral compartment (7) and >10 LNs in the central compartment alone (4) to be prognostic of recurrence when adjusting for the presence of ENS. In our own study, we explored various cutoffs for the number of central LNs that were predictive of recurrence. We did not find a clear cutoff for the number of positive LNs. For this reason, systematic multivariable analysis for three or fewer or more than three LNs, five or fewer or more than five LNs as well as eight or fewer or more than eight LNs, adjusting for LN diameter and presence of ENS, was performed (Table 2). Whilst an increasing number of positive central LNs increases risk of recurrence on univariable analysis (Table 1), this risk would seem to be secondary to its association with ENS rather than an independent predictor.
With regards to ENS, many studies have shown ENS to be an important predictor of outcome in other head and neck cancers (11,12), and it is widely accepted as an indication for additional adjuvant therapy in squamous cell carcinoma (13). However, there are few studies on the impact of ENS on outcome in patients with thyroid cancer. Earlier studies were unable to detect an association between ENS and outcome, possibly due to the small sample size (14). However, several recent international groups have observed ENS to be prognostic of outcome (7,15 –17). More recently, a review of 111 PTC patients with total thyroidectomy and positive central LN metastases by Lee et al. suggested that the rate of ENS in PTC patients was higher with younger age, large tumor size, and increased number of central neck LN metastasis. However, due to the short follow-up period in this study, the impact on outcome could not be determined (18).
The extent of ENS on prognosis has also been investigated. Several Japanese groups have demonstrated poorer outcomes in patients with evidence of macroscopic ENS (17,19) in central or lateral neck LNs. Macroscopic ENS was defined as LN invasion of cervical organs, vessels, or nerves that required partial or full excision. The same group investigated the role of ENS in central compartment LNs and found no association between ENS and outcome (4). Other studies have reported microscopic ENS alone is predictive of RFS and DSS outcome (20,21). Yamashita et al. performed a matched pair analysis of 50 patients with distant metastatic DTC disease with 50 control patients without distant disease, together with histological review of pathology slides. Univariable analyses demonstrated that among other tumor and patient factors, LN deposits >1 cm and presence of microscopic ENS were significantly higher in the distant metastatic group. However, on multivariable analyses, ENS was the only statistically significant LN predictor of outcome (20).
It is important to note that our study has several limitations. Due to its retrospective nature, our study is susceptible to all the limitations associated with such studies. First, our institutional policy is to perform neck dissections only in patients with palpable or ultrasound evidence of cervical neck metastases. It is therefore possible that some N1a patients included in this study had subclinical lateral neck disease not detected at the time of preoperative work-up. Lateral neck recurrence events in this cohort may therefore represent persistent disease rather than recurrent disease and thus neck recurrence events may have been overestimated. Nevertheless, the impact of microscopic disease on outcome has not been demonstrated. A second limitation is that the quality and detail of histopathology reporting of both the primary tumor and the LN features has improved significantly in the modern era. Of the 600 patients, only 354 (59.0%) patients had all three LN features (size of largest LN, number of positive LNs, and presence of ENS) available for analysis. Our multivariable analysis is therefore based upon this smaller number of patients.
In conclusion, in patients with positive central compartment nodes, we have found LN diameter, number of LN metastasis, and LN ENS to be predictive for neck recurrence. We report that the strongest predictor appears to be the presence of ENS. Management guidelines may consider these data when recommending adjuvant therapy for patients with differentiated thyroid cancer. However, further studies on larger data sets with complete synoptic reporting of all of these LN characteristics is required to support the impact that ENS has on outcome definitively.
Footnotes
Author Disclosure Statement
The authors have no commercial associations or potential conflicts of interests to declare.