
Abstract
Background:
Health registries have become extremely powerful tools for cancer research. Unfortunately, certain details and the ability to adapt to new information are necessarily limited in current registries, and they cannot address many controversial issues in cancer management. This is of particular concern in differentiated thyroid cancer, which is rapidly increasing in incidence and has many unknowns related to optimal treatment and surveillance recommendations.
Summary:
In this study, we review different types of health registries used in cancer research in the United States, with a focus on their advantages and disadvantages as related to the study of thyroid cancer. This analysis includes population-based cancer registries, health systems-based cancer registries, and patient-based disease registries. It is important that clinicians understand the way data are collected in, as well as the composition of, these different registries in order to more critically interpret the clinical research that is conducted using that data. In an attempt to address shortcoming of current databases for thyroid cancer, we present the potential of an innovative web-based disease management tool for thyroid cancer called the Thyroid Cancer Care Collaborative (TCCC) to become a patient-based registry that can be used to evaluate and improve the quality of care delivered to patients with thyroid cancer as well as to answer questions that we have not been able to address with current databases and registries.
Conclusion:
A cancer registry that follows a specific patient, is integrated into physician workflow, and collects data across different treatment sites and different payers does not exist in the current fragmented system of healthcare in the United States. The TCCC offers physicians who treat thyroid cancer numerous time-saving and quality improvement services, and could significantly improve patient care. With rapid adoption across the nation, the TCCC could become a new paradigm for database research in thyroid cancer to improve our understanding of thyroid cancer management.
Introduction
A
However, given the magnitude of data that national registries must collect for all cancer types, certain details and the ability to adapt to new information are necessarily limited. Registry data cannot answer many questions that researchers may have, and cannot address many controversial issues in cancer management. While controversy exists in all fields of cancer management, thyroid cancer is of particular importance because of its rapidly increasing incidence and often young and otherwise healthy patient population. Despite extensive analysis of large cohorts of patients using various registries and databases, there is great debate as to the optimal extent of surgery, postoperative treatment, and surveillance recommendations in the management of patients with differentiated thyroid cancer.
Many clinical practice guidelines defer to “expert opinion” because of the paucity of high-quality data (2 –4). Moreover, “experts” often disagree on optimal treatment and surveillance strategies. Furthermore, the prognostic significance of genetic and molecular markers as well as the importance of various features of pathologically involved lymph nodes require more detailed analysis with large cohorts of patients to help guide disease management. As such, there is a significant need to collect and analyze detailed data to improve thyroid cancer management. These data must be collected over a patient's lifetime in order to understand the impact of therapy, as disease recurrence may occur decades following initial treatment. Unfortunately, a registry that follows a specific patient, is integrated into physician workflow, and collects data across different treatment sites and different payers has been impossible to create and implement in the current fragmented U.S. healthcare system.
In this study, we review different types of health registries used in cancer research in the United States, with a focus on their advantages and disadvantages as related to the study of thyroid cancer. Then, in an attempt to address shortcoming of current registries and databases for thyroid cancer, we present the potential of an innovative web-based disease management tool for thyroid cancer called the Thyroid Cancer Care Collaborative (TCCC), to become a patient-based registry used to evaluate and improve the quality of care delivered to patients with thyroid cancer as well as to answer questions that have not been addressed with current databases and registries. Unique features of the TCCC that overcome some of the shortcomings in current thyroid cancer registries and databases are presented.
Review
Population-based cancer registries
A population-based cancer registry (PBCR) “records all new cases [of cancer] in a defined population (most frequently a geographical area)” (5). The value of a PBCR is in identifying trends in cancer incidence at different geographic locations, as well as providing descriptive statistics such as patient demographics or stratification of outcomes based on a variety of variables. As technology has improved and more resources have been devoted to PBCRs in the United States, they have gone beyond providing only descriptive statistics; they are now being used to study the effects of stage at diagnosis, tumor histology, and the impact of different treatments on survival and recurrence.
While every state in the United States has a PBCR under the umbrella of the National Program on Cancer Registries (NPCR), most publications from PBCRs use data from the SEER program. The SEER database is a group of 20 population-based registries from around the country, held to a specific standard, that have been chosen to be representative of the population of the United States. SEER captures information regarding incident cancers for 26% of the U.S. population. SEER registers information on patient demographics, primary tumor site, tumor morphology, stage at diagnosis, and first course of treatment, and performs follow-up for survival status of each patient as its primary outcome. Data are sent by hospital registries, pathology laboratories, and physicians' offices to the PBCR, where cancer registrars consolidate and validate the information, and remove personal identifiers. Data are sent to SEER from local PBCRs on a regular basis (at least annually).
Benefits of PBCRs and SEER
There are a number of features of the SEER program that make it a powerful tool to study cancer epidemiology and outcomes. First, it captures essentially all new cancer cases diagnosed in a specific geographic location, regardless of the type of treatment setting. Second, SEER requires follow-up for survival status and cause of death for all cancer cases in the program; this is typically done through linkage with other government databases. Third, significant resources are devoted to quality control in SEER, including an annual program conducted by the NCI to evaluate the quality and completeness of the data in which patient cases are re-abstracted to determine the accuracy of the data (6). In addition, training workshops for registry abstractors are conducted at the local level and by the NCI. Fourth, registries contributing to the SEER program collect detailed information on tumor characteristics (including stage of disease at diagnosis), demographic data, surgical intervention, and whether radiation therapy was given.
Examples of PBCR and SEER database analysis
A number of informative studies in thyroid cancer have come from analysis of SEER data. For example, SEER data have demonstrated the incredible increase in the rate of thyroid cancer diagnosed in the United States, along with descriptive statistics related to this change (7). In addition, the SEER program has identified the characteristics of large populations of patients with very specific conditions such as medullary thyroid cancer (8), pediatric thyroid cancer (9), anaplastic thyroid cancer (10), breast cancer in patients with thyroid cancer (11), and Hashimoto's thyroiditis in patients with thyroid cancer (12). In addition, studies analyzing specific prognostic variables such as lymph node status (13 –15), and the effect of treatment, such as extent of thyroidectomy (16), have been made possible through analysis of the SEER data.
Limitations of PBCRs and SEER
Investigators who are adept at review and analysis of population-based cancer registries such as SEER are skilled at asking very specific, focused questions based on the data available. However, these authors understand the limitations of the information this research can provide.
Most importantly, SEER does not, and cannot, capture the necessary relevant data that could help improve care. For example, there is no information included in the SEER registry to retrospectively influence diagnostic recommendations, including results and trends of diagnostic testing. Furthermore, for treatment, the magnitude of thyroid hormone suppression and the corresponding TSH levels are not available. Though information regarding radioactive iodine (RAI) therapy is available, the details of therapy including use of thyroid hormone withdrawal or recombinant thyrotropin (TSH) injections are not reported. Also, SEER only captures data on the first course of treatment; subsequent treatment, as is common in thyroid cancer, is not included in this database.
In terms of pathology, many details about nodal disease in patients with thyroid cancer are not recorded. Unfortunately, details about size of nodes, whether they are clinically evident, and features of nodes (such as extranodal extension) are simply not available for analysis using SEER data and therefore cannot shed light on the active controversies regarding the impact of lymph nodes in thyroid cancer. In fact, the conclusions about the influence of lymph nodes in well-differentiated thyroid cancer from SEER data have been conflicting, with one study showing that lymph node involvement did not impact survival in differentiated thyroid cancer (13), another one showing a significant difference in 14-year overall survival between node-negative and node-positive cancers (14), and another study that concluded that the presence of lymph node metastases affected survival in all patients with follicular carcinoma and only patients with papillary thyroid cancer over the age of 45 (15). This type of contradictory data from the same database, but over differing years, implies that there might be something more than just the presence or absence of positive lymph nodes that can act as a prognostic variable; unfortunately, SEER does not have any further details about lymph nodes in these patients. In their study analyzing outcomes based on extent of thyroidectomy, Haigh et al. note that SEER lacks the clinical detail that might help to explain some of the differences in survival observed between groups treated with different extents of thyroidectomy (16).
In SEER, data are collected primarily from the pathology report, hospital or outpatient surgical center record, and nuclear medicine facilities, but physicians' offices are not routinely visited (6). This is of particular concern for thyroid cancer in which the majority of patients are followed in physician's offices where data are difficult to access. Related to data collection, the SEER coding rules are sometimes confusing and overlapping, leading to problems with accurate analysis. This is particularly true in the way that extensive local tumor extension and metastatic disease for thyroid cancer were coded from 1988 to 2003 (15,17).
As new information becomes available, such as genetic and molecular markers, a major investment of resources is required to add or change variables to the database.
In terms of timeliness, SEER is required to report complete counts of new cases to the NCI only within 22 months of the end of the year in which the diagnosis is made, thereby allowing registrars time to gather information on first course of treatment, but making data analysis at all times almost 2 years old.
Finally, active follow-up is limited to survival status and cause of death as recorded in government databases, thereby limiting the analysis of patterns of recurrence and subsequent treatment over a patient's lifetime.
Health systems-based cancer registries
In contradistinction to PBCRs, health systems-based cancer registries collect incident cases in a specific setting. This could be a single-institution, multi-institution, payer-based, or hospital-based health registry.
Single-institution databases have provided valuable data in understanding thyroid cancer. In particular, single institution reviews have had a major impact on predicting prognosis and creating risk group stratifications in thyroid cancer based on factors such as Age (A), Gender (G), Invasion (I), Size (S), Extent (E), Distant Metastases (M) and Completeness of Resection (C) in systems such as MACIS (18), AMES (19), AGES (20), and GAMES (21). They have also led to the stratification of thyroid cancer patients into groups that include low risk, intermediate risk, and high risk of recurrence and/or death from cancer (21).
The Thyroid Tumor and Cancer Collaborative Registry at the University of Nebraska is a single-institution registry that goes beyond collecting clinical data. The Thyroid Tumor and Cancer Collaborative Registry questionnaire collects extensive demographic information, including family history; occupational and exposure analysis; dietary habits; smoking, alcohol, and caffeine ingestion; medications; previous medical history; and treatment. It is coupled with a biospecimen bank for blood, urine, and tissue on each person. Data are supplemented retrospectively with electronic medical records from the University of Nebraska when necessary. While a biospecimen bank and exposure history are important supplements, this health system-based cancer registry suffers the same limitations of other single-institution researcher-driven databases: low numbers, selection bias, and potential issues with generalizability.
The National Thyroid Cancer Treatment Collaborative (NTCTC) is a multi-institution system-based health registry that was established in 1986 at the University of Cincinnati that includes 14 major academic medical centers. The NTCTC registers patients prospectively at the time of diagnosis of thyroid cancer. Information is obtained by review of patients' charts, including physician notes and letters; surgical notes; and radiographic, laboratory, and pathology reports. Initial case reports are to be completed within three months of initial disease diagnosis, and follow-up is conducted annually. From 2001 to 2010, the number of registered cases in the NTCTC increased from 2936 to 4767, and median length of follow-up increased from 3 to 5.3 years (22).
The goals of this prospective, multicenter registry are (a) to establish a broadly applicable staging classification for predicting outcome in patients with thyroid carcinoma, (b) to define contemporary clinical practice in the management of these patients, and (c) to determine the impact of different therapeutic approaches on the morbidity and mortality of this disease. A number of excellent studies have been generated from this multi-institutional database, including a staging classification that provides a prospectively validated scheme for predicting short-term prognosis for patients with thyroid carcinoma (23). The major limitations of this multi-institutional collaborative are as follows: (a) it is limited to a select few major academic medical centers; (b) data are abstracted first from each institution's charting system retrospectively into a five-page word processor form, which is then entered into the central registry by another data abstractor; and (c) the data collection sheet was last updated in 2001. This results in a bias toward types of patients and diseases going to major academic medical centers, quality and completeness issues inherent to retrospective chart reviews by data abstractors, and timely and relevant data points
The premier multi-institution health systems-based database used for cancer research is the National Cancer Database (NCDB). The NCDB is a joint program of the American Cancer Society and the American College of Surgeons' Commission on Cancer (ACS CoC). Data are collected at the institutional level by 1506 ACS CoC–accredited cancer programs in all 50 states as well as Puerto Rico. Data on all types of cancer are recorded, including thyroid cancer. The NCDB collects very detailed data on all new cases of cancer diagnosed or first treated at a CoC-accredited cancer facility (analytic cases). The NCDB is estimated to capture approximately 67.4% of new cancer cases in the United States, with a range of 27.1% (Arizona) to 88.7% (Delaware) (24). For thyroid cancer, case ascertainment by NCDB is between 76% (24) to 92% (25) of incident cases in the United States, depending on the PBCR used to estimate incidence. Each CoC-accredited facility has a central tumor registry in which professional tumor registrars abstract data from medical charts into a computer program and data are then periodically sent to the NCDB. The number of new thyroid cancer cases in the NCDB from all CoC-accredited hospitals from 2000 to 2011 is shown in Figure 1.
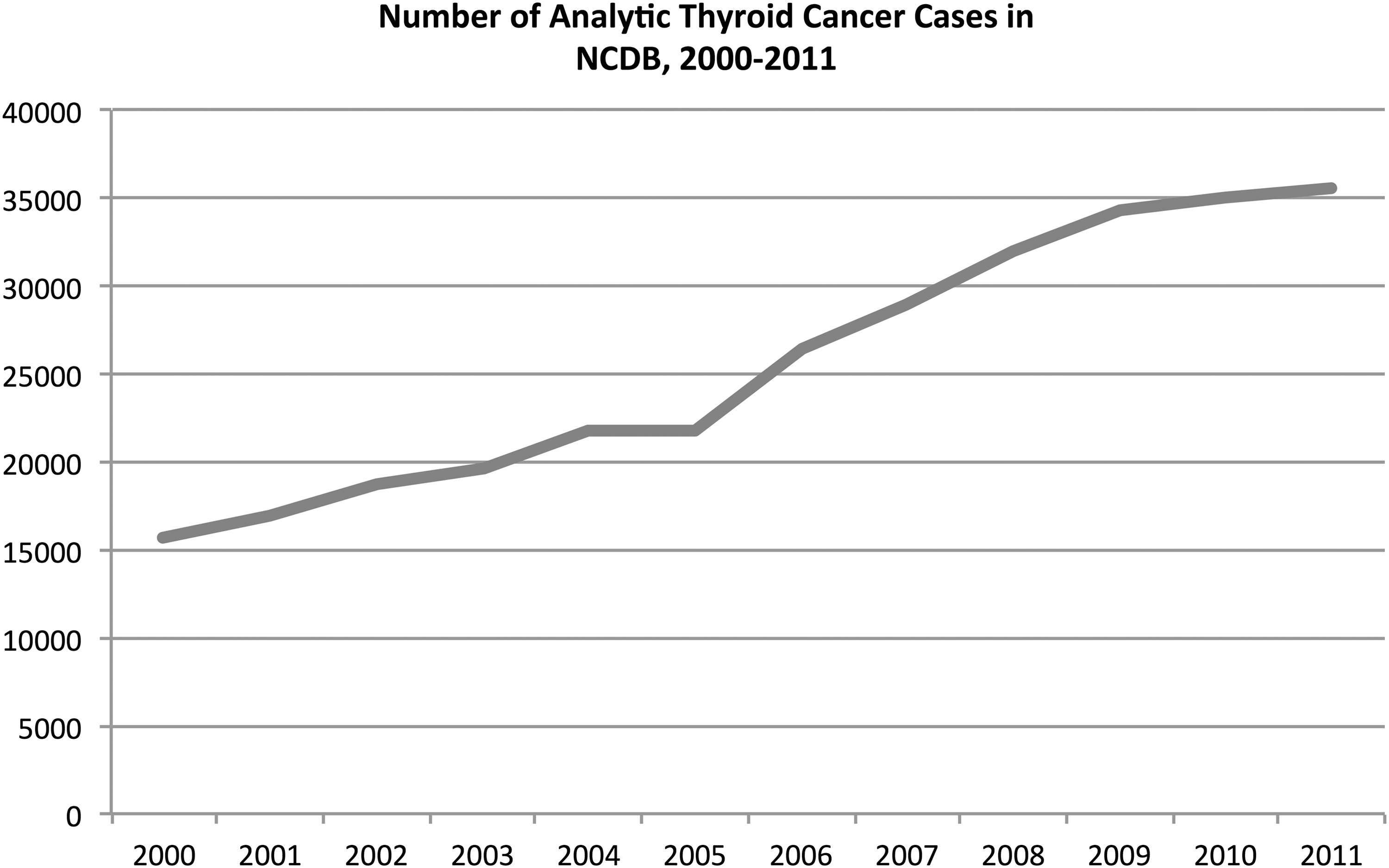
Number of newly diagnosed thyroid cancer in the National Cancer Database (NCDB) from 2000 (n=15,653) to 2011 (n=35,473). Prior to 2006, thyroid cancer had under 24,000 annual cases diagnosed in the database and was not in the top-11 NCDB cancer sites (26).
Benefits of the NCDB
There are numerous favorable characteristics of the NCDB in studying cancer epidemiology and outcomes. First, there is a broad range of the types of hospitals reporting data to the NCDB from diverse geographic locations. This permits analysis of the variability in care across the country not only in geography, but also based on hospital type and patient volume (25).
Although the NCDB is a tremendous repository of oncologic data, some researchers believe that the most important benefit is its ability to benchmark hospitals and feed information back to the public and to participating hospitals. The NCDB offers public benchmark reports for the 11 most commonly diagnosed solid-organ tumors in the United States. These reports currently provide data on more than 5.9 million patients, allowing users to define queries based on patient sex, age, ethnicity, histology, stage, first-course therapy, type of surgical resection, hospital type, and geographic location. The NCDB also offers five-year survival reports based on patient stratification using the American Joint Commission on Cancer (AJCC) staging system.
In addition, the NCDB can designate special data requests for certain tumor types, which must then be collected by cancer registrars. Known as a Collaborative Stage, these unique fields are specific to the type of cancer. According to the Collaborative Staging manual for thyroid cancer, the only specific data point collected is whether the cancer is multifocal within the thyroid gland.
Also, because of the large representation of patients with a specific type of cancer and particular patient and tumor characteristics, the large sample size allows researchers to draw statistically significant inferences in rare cancers as well as a subset of more common cancers (e.g., 1–2 cm papillary thyroid cancers) (25). NCDB data have provided valuable information about important questions that are essentially impossible to address in a clinical trial in which a large cohort of patients is required to detect a small difference in survival as described below.
Examples of NCDB analysis in thyroid cancer
Because of these advantages, the NCDB has been used in a number of interesting ways to find trends among large numbers of patients. For example, in 1998 Hundahl et al. published the NCDB report on over 53,000 cases of thyroid carcinoma treated between 1985 and 1995 (27). The authors reported demographic and survival statistics stratified by stage for the major histologic subtypes of thyroid cancer. A limitation of this study was that, halfway through the period of data collection, the AJCC staging system for thyroid carcinoma changed and the authors noted that reliable re-staging of patients was not feasible.
In September 2013, NCDB released Participant User Files to researchers at CoC-approved hospitals. As Bilimoria et al. from the NCDB explain, “this file will provide the opportunity to examine a large dataset containing a number of data points that are not available through other cancer registries including surgical margin status, systemic therapy (chemotherapy and hormonal therapy), detailed radiation treatment data, and clinical and pathological AJCC staging” (25).
While the Participant User Files are a major dataset to study, the completeness of the information and the utility for thyroid cancer is limited. Items such as hormone therapy are recorded in all patients who are on levothyroxine, but TSH levels and therefore the level of thyroid hormone suppression are not available. Dosages of RAI are sparsely included, and must be abstracted from office notes in the physician charts and are incomplete if patients are seen by doctors at a number of different sites. Also, this dataset cannot evaluate the importance of some aspects of thyroid cancer that are not recorded, such as more detailed characteristics of metastatic lymph nodes that have been shown to be important (28).
Limitations of health systems-based registries and NCDB
Despite the insightful work that has come from single-/multi-institution databases, as well as the large amount of data available from the NCDB, health systems-based registries do have some drawbacks.
One of the major problems in current databases is the depth of data collected. Hospital registries at CoC-accredited hospitals must follow the FORDS Manual for data abstraction from medical charts for all new cancer types. This includes patient factors, tumor factors, treatment factors, and outcomes. Data points required to complete the TNM stage must be included, as well as some site-specific items as identified in the Collaborative Stage manual. For thyroid cancer, the only additional item required in the collaborative stage is unifocal versus multifocal carcinoma within the thyroid. While protocols in pathologic reporting (e.g., College of American Pathologists protocols) have simplified data collection by tumor registrars, the database only contains information requested by the registry. For example, in thyroid cancer, most registries report lymph nodes simply as N0, N1a, or N1b even though pathology reports often contain data such as number of positive lymph nodes, size of lymph nodes, and the presence of extranodal extension, as indicated in the updated version of the College of American Pathologists thyroid cancer protocol released in 2014 (29). Furthermore, items such as level of thyroid hormone suppression or dose (activity) of RAI are variables that are not consistently collected in NCDB datasets.
The effort to gather a great level of detail in large national databases has proven to be a significant challenge, and according to Veeranki et al., some experts have urged central and hospital registries to collect minimal data, cease collection of data items that are essentially never used, and focus on case finding (i.e., ensuring that all incident cases are captured) in order to be more prudent and cost-effective (30). Registrars must balance the information that can be obtained from the medical charts at various treatment sites with what is deemed to be most important given a finite amount of resources.
Second, these types of databases suffer from bias in the types of patients who are treated at such facilities. For example, there are over 5000 hospitals in the country, and the NCDB captures patient data at approximately 1500 of them, all those being CoC accredited. There may be an inherent difference in the types of patients who receive their initial care at non-CoC-accredited hospitals, and thereby introducing an important selection bias.
Third, cancer statistics can be greatly impacted by the quality of the data collected in a large database. For example, a study on breast cancer found that improved ascertainment of breast cancer registrations was associated with a drop in overall five-year survival (31). Problems in data quality may be related to the way in which they are collected. NCDB data are abstracted by cancer registrars utilizing page-by-page review of physician charts and hospital notes, similar to the method used in SEER.
Fourth is the extent of a “complete” dataset. The NCDB uses the term “analytic cases” as those patients who are either diagnosed and/or first treated at a CoC facility. Only analytic cases must be reported to the NCDB. Therefore, a patient who is diagnosed and undergoes initial treatment in the form of a hemithyroidectomy at a non-CoC facility, and then undergoes evaluation and further treatment at a CoC facility, will not be included in the NCDB. Similarly, patients with recurrent cancer who come to a CoC-accredited facility are considered nonanalytic and do not have to be reported to the NCDB.
Finally, the issue of follow-up represents a significant challenge. The facility in which the diagnosis or first treatment occurs (i.e., an analytic case) is responsible for life-long follow-up. If the patient stays within the same treating facility, cancer registrars are able to perform chart reviews and find required information from doctors' notes for additional treatment courses. However, if patients move location or change doctors, the process is more cumbersome and the registrars are responsible for contacting those doctors for follow-up. This occurs by contacting the patient, finding his/her current doctor's information, and then sending a letter to the new doctor with questions about follow-up. In these situations, because of low response rates, registrars have found the ability to obtain follow-up data to be quite limited.
Patient registries
Another type of registry, with a much looser definition, is the patient registry. In most cases, patient registries are created to answer a very specific question for a group of patients with a particular exposure or disease, or who have undergone a particular treatment. Patients are actively followed regardless of where they are treated. Large-scale patient registries have long been the domain of pharmaceutical and device manufacturers who track long-term postdrug or device release data on side effects and safety.
In 2010, Navaneethan et al. (32) developed an innovative electronic health record (EHR)-based patient registry for chronic kidney disease (CKD) at the Cleveland Clinic, which included over 57,000 patients within the Cleveland Clinic main hospital and 15 community-based health centers with mild to moderate CKD. This was unique in that data from the registry were pulled directly from the EHR (which was shared among all practice sites), and the data points available for analysis were extremely detailed including a range of comorbid conditions, laboratory values, imaging (renal ultrasound), and anthropometric details (32). One of the major drawbacks of the health systems-based cancer registries as well as the population-based cancer registries described above is the need for data abstraction by individuals who are not involved in the patient's care. In this case, by virtue of its integration into the clinician workflow at the Cleveland Clinic, there is a great amount of data available without the unnecessary burden of chart abstraction. The authors of that study (also the developers of the CKD registry) recognized that the major drawback to their EHR-based patient registry is that, for patients who seek part or all subsequent care outside of the Cleveland Clinic Health System, their detailed clinical data will not be available for analysis.
To our knowledge, a registry that actively follows cancer patients irrespective of location and/or practice site of the diagnostic and/or treating physicians does not exist, particularly one that has disease-specific details that are maintained through a mechanism that obviates the need for data abstraction.
A patient registry for thyroid cancer
For a multitude of reasons, thyroid cancer is an ideal disease to embrace such a system. First, the diagnosis and care of patients with thyroid cancer involves coordination between multiple specialists, which include endocrinologists, surgeons, nuclear medicine physicians, radiologists, radiation oncologists, pathologists, cytopathologists, and medical oncologists. These physicians are often located in different practice settings that are not connected by a common EHR and are forced to communicate via letters and telephone calls or more often by the patient collecting all of their important records and serving as the messenger to each treating physician (Fig. 2).

Thyroid cancer care requires significant coordination between various physicians and care sites, making communication and maintaining a complete dataset a major challenge. Figure adapted from (35).
Second, thyroid cancer has been recognized as one of seven cancers that are increasing in incidence (33), occurring at a remarkable rate as shown in Figure 3.
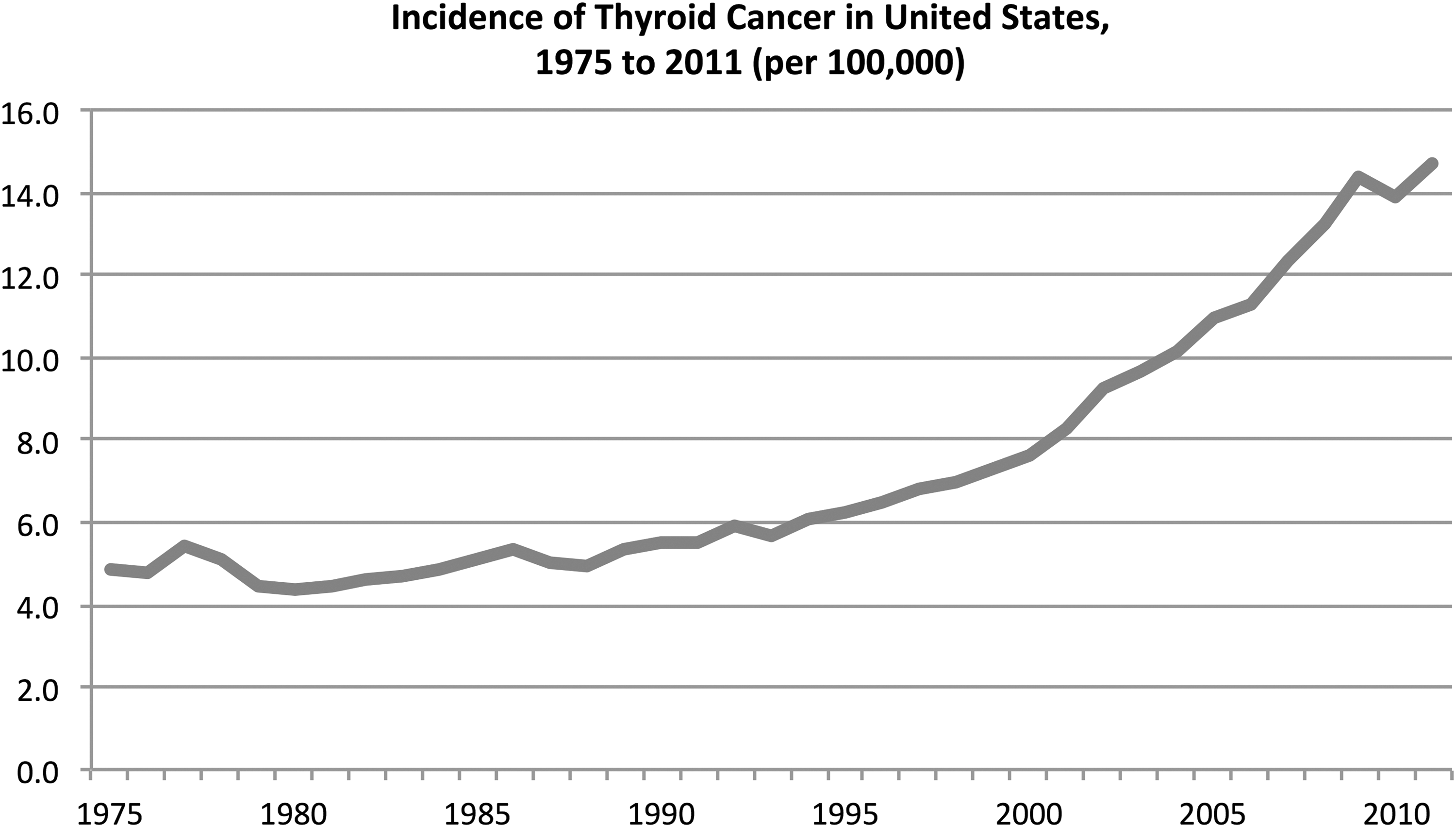
Incidence of thyroid cancer in the United States from 1975 to 2011, according to Surveillance, Epidemiology, and End Results data (34).
Third, patients with thyroid cancer are often young and otherwise healthy. It is not uncommon for such individuals to change jobs, insurances, locations, and practitioners, and need to be followed over long periods of time in order to gain meaningful data especially regarding disease recurrence. Survival statistics alone are not a sufficient outcome data point in the management of thyroid cancer.
Fourth, as discussed above, there are significant controversies and lack of strong clinical evidence related to certain key areas in the management of patients with thyroid cancer. In light of the number of clinical practice guidelines dependent on “expert opinion” (in which experts often disagree) and those that are intentionally nonspecific, there is an imperative to collect and analyze data to improve thyroid cancer management (3). There is a necessity to capture disease details over extended periods of time in order to identify significant prognostic variables that will help to guide important disease management controversies such as the role of central neck dissection, extent of thyroidectomy required, and optimal use and dosage of RAI, which will otherwise remain in the realm of expert opinion.
The TCCC: a new paradigm for database research in thyroid cancer
In an attempt to improve quality, the TCCC was created by a group of key opinion leaders in thyroid cancer from across the country as described in detail in a previous review (35). The TCCC was developed to be a comprehensive web-based program for patients and clinicians to report and store all data related to a patient's thyroid cancer care. Physician participation is completely voluntary, with a number of features such as patient education videos, clinical decision-making modules with the latest guidelines, and enhanced cancer care communication, which will benefit patients, community physicians, and academic physicians alike.
Each thyroid cancer patient is given a TCCC profile within which they can identify his or her thyroid cancer team of clinicians, irrespective of any specific practice group. Data entry is performed by the clinician (or her/his designee) at the point of care into the web-based interface. There are nine distinct modules: initial presentation, imaging, surgical management, postoperative hospital course, postsurgical follow-up/-treatment surveillance, pathology and staging, laboratory results, nuclear medicine, and change in health status in which to enter data. For example, following an operation, the surgeon would complete the “Surgical Management” module, which takes less than two minutes to complete, and will autogenerate a narrative operative report that meets all American Thyroid Association guidelines for high-quality operative reporting in thyroid cancer (36,37).
The pathology/staging module is designed to report the most up-to-date CAP protocol for thyroid cancer and includes important lymph node-related information about the number, size of metastatic focus, and the presence of extranodal extension. In addition, the TCCC captures information about whether pathologic nodes were clinically evident prior to or during surgery. For office visits, the Post-Surgical Follow-up/-Treatment Surveillance module has a simple point-and-click interface that inputs data directly into the database. This point-of-service data entry will improve the quality and completeness of data available for research, which is a known disadvantage of retrospective data abstraction methods used in current cancer databases. Accuracy of data entry is high because data are entered at the point-of-service by the clinical team, automatic alerts are generated for outlying data, data are immediately available for review by all practitioners involved in the care of the patient, and patients themselves can review their clinical data and identify inconsistencies and errors. Therefore, patients will be strong drivers to maintain up-to-date, replete, and accurate clinical information.
Currently, with the synoptic and/or graphical nature of each module, data entry takes only a few minutes. Also, detailed and highly illustrated patient education and informed consent videos save the physician and their clinical staff time, thereby providing an opportunity to enter data into the appropriate module(s). Furthermore, integration of the TCCC into provider EHRs using a universal language is in active development, as is autopopulation from synoptic pathology and laboratory reports, and opportunities to “cut and paste” information from the TCCC into EHRs can facilitate record keeping. Representative screenshots of the user interface are shown in Figure 4.
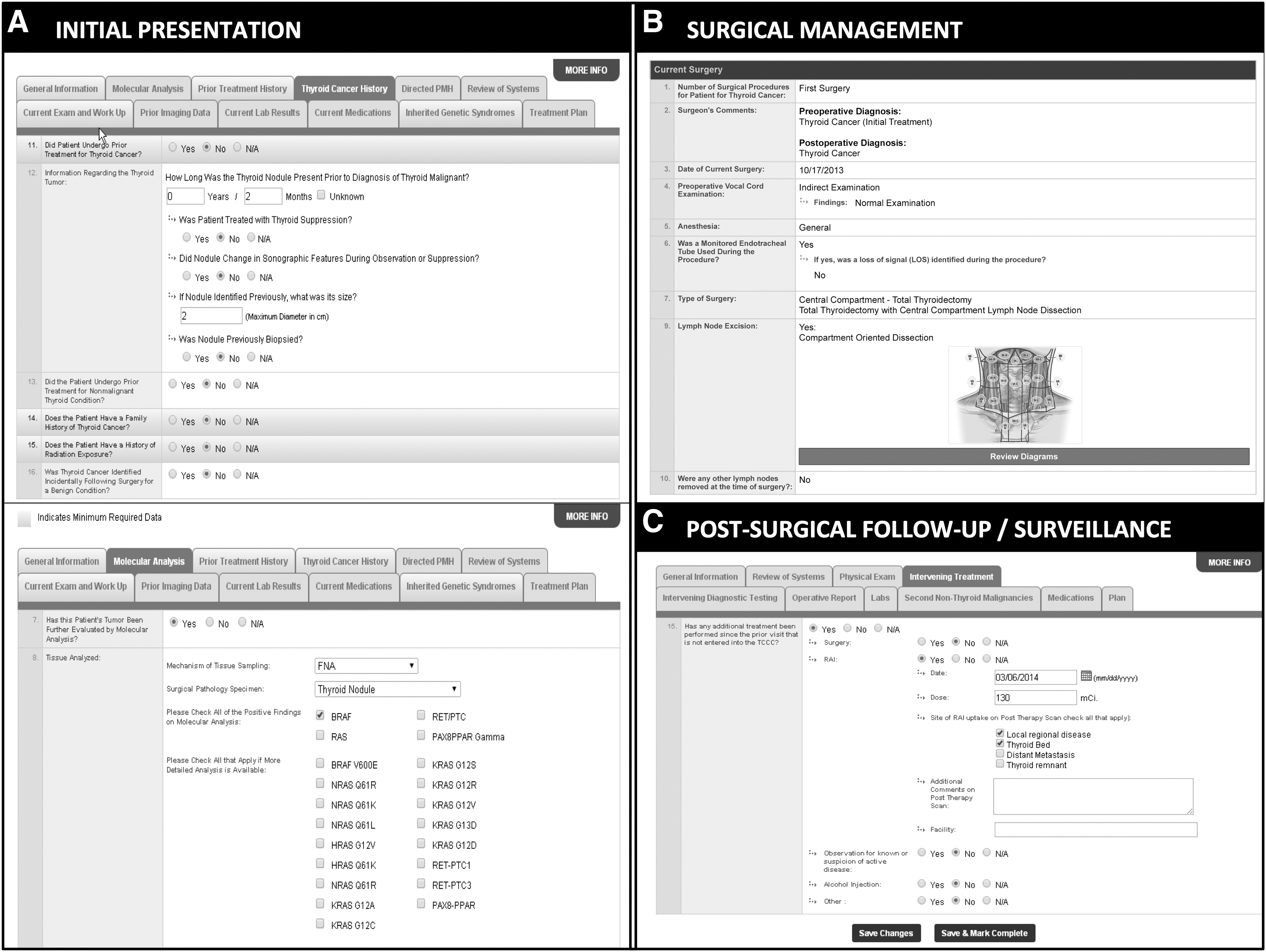
Representative screen shots of web-based graphical user interface for patients and clinicians to perform synoptic data entry. There are nine distinct modules: initial presentation
In addition to being an online repository of clinical information, the TCCC provides education and evidence-based clinical decision-making support services to patients and physicians within the framework of both the American Thyroid Association and National Comprehensive Cancer Network clinical practice guidelines for thyroid cancer (2,3). These latter features were designed into the system in order to enhance user adoption, with the secondary advantage of increasing utilization of clinical practice guidelines by bringing them directly to physicians at the point of care. It is believed that this will enhance the quality of care administered across the entire spectrum of healthcare in the United States.
The TCCC meets the strictest standards for HIPAA compliance with appropriate data encryption and site-wide security at the browser and server level, ensuring that no unauthorized users have access to patient data. Furthermore, patients have a clear understanding that, in addition to the quality and communication advantages of the TCCC, research is a cornerstone of the TCCC and is part of the informed consent presented to patients at the initial visit.
While individual physicians have the ability to query aggregate data about their own patients, multiple-provider or multi-institution data queries using anonymous data require review and approval by a multidisciplinary research committee and either an independent or institution-linked ethics review board. The infrastructure for data queries is otherwise similar to current anonymous multi-institution cancer databases and the questions that can be answered are as limitless as the data points available for analysis. Retrospective clinical research can provide valuable information about treatment outcomes that require long-term longitudinal follow-up as well as the ability to identify unique cohorts of patients who require more intensive therapy, as well as de-intensified therapy.
Additional unique features of the TCCC as a new paradigm for patient-based cancer registry research are presented in Table 1.
AJCC, American Joint Commission on Cancer; CoC, Commission on Cancer; EHR, electronic health record; NCDB, National Cancer database; RAI, radioactive iodine; TCCC, Thyroid Cancer Care Collaborative; TSH, thyrotropin.
The TCCC model is particularly suited for disease processes that require a high level of coordination between different specialists at different practice locations over a long period of time. It offers a solution for maintaining comprehensive data on patients if they move to a new geographic location or change their physicians; patients can simply request that new clinicians be provided access to their records, and thereby continue to maintain a more complete dataset.
Future directions
The future of the TCCC as a national database will evolve with more widespread adoption beyond the walls of academic institutions and large hospital systems. All physicians in all practice settings who treat patients with thyroid cancer are invited and encouraged to participate. A list of TCCC-participating physicians will be available within a particular patient's geographic location. Physician participation is voluntary, and will be partly patient driven. The TCCC is more than just a registry: offering patient education, enhanced physician communication, and clinical decision-making support using the latest guidelines to all users with numerous time-saving and quality improvement services. While not a replacement for the work of NCDB and SEER, which are powerful tools to capture national trends in thyroid cancer, the TCCC has the potential to answer questions in thyroid cancer that these large-scale cancer databases simply cannot. With a more comprehensive disease-specific dataset and the commitment to provide continuous updates to the TCCC as new information becomes available, the TCCC holds promise to serve as a very valuable research tool. Also, future linkage of TCCC data with other databases might give researchers the ability to carry out health services and outcomes analysis in thyroid cancer that is not yet possible. In addition, with large-scale adoption, the TCCC presents an opportunity to direct appropriate patients into clinical trials.
Summary
Though extremely powerful tools for cancer research, certain details and the ability to adapt to new information are necessarily limited in current cancer registries, hence greatly limiting their ability to address many controversial issues in cancer management despite huge cohorts of patients. This is of particular concern in differentiated thyroid cancer because it is rapidly increasing in incidence and there is great debate as to the optimal extent of surgery, postoperative treatment, and surveillance recommendations.
It is imperative that clinicians understand the nature of these databases in order to more critically interpret the numerous clinical research studies that appear in the literature. Here, we review different types of health registries used in thyroid cancer research, including a discussion of advantages and disadvantages of each. This analysis includes (a) population-based cancer registries, particularly those that contribute data to the SEER Program; (b) health systems-based cancer registries, such as single-institution, multi-institution, and the NCDB; and (c) patient-based registries used in other areas of healthcare. A cancer registry that follows a specific patient, is integrated into physician workflow, and collects data across different treatment sites and different payers does not exist in the current fragmented system of healthcare in the United States.
To overcome the shortcomings of current registries and databases for thyroid cancer, an innovative web-based disease management tool for thyroid cancer called the Thyroid Cancer Care Collaborative (TCCC) is presented. The TCCC has the potential to become a patient-based registry used to evaluate and improve the quality of care delivered to patients with thyroid cancer as well as to answer questions that current databases and registries cannot. Unique features of the TCCC that address some of the shortcomings in current thyroid cancer registries and databases include (a) detailed data fields that are dynamic and can change as new information becomes available; (b) seamless integration of data entry into physician workflow; (c) patient-driven life-time follow-up on disease status, diagnostic tests, additional treatments, and treatment-related complications regardless of practice site; (d) representation across the entire spectrum of disease presentation and sites of care; and (e) private analysis of physician outcomes against regional or national benchmarks. In Table 2, the TCCC is compared to the major population-based and health systems-based cancer registries currently in use for cancer care in the United States.
Actual performance will be dependent upon adoption by physicians and patients. SEER, Surveillance, Epidemiology, and End Results; TBD, to be determined depending on speed of adoption across the country.
The hope is for rapid adoption of the TCCC into the healthcare landscape by physicians who treat thyroid cancer that will be driven by the numerous time-saving and quality improvement services it offers patients and care providers.
Conclusions
Cancer registries and databases are powerful tools to analyze epidemiology and basic outcomes in thyroid cancer and to generate hypotheses. A number of unique features of the TCCC give it the potential to become a new and improved patient registration database to analyze outcomes in thyroid cancer at a depth that is not possible in any current cancer registry. A demonstration of the TCCC is available to view online.
Footnotes
Acknowledgments
The preparation of this article was supported by a generous grant from the Mount Sinai Health System and the Thyroid Head and Neck Cancer (THANC) Foundation.
Author Disclosure Statement
No competing financial interests exist.