
Abstract
Objective:
The goal was to determine if there was a relation between the introduction of evidence-based radioactive iodine (RAI) treatment guidelines for differentiated thyroid cancer (DTC) at Cedars-Sinai Medical Center (CSMC) and subsequent RAI use. In addition, we compared RAI treatment rates for DTC at CSMC to data from the National Cancer Database (NCDB) to see if the trends in RAI use at CSMC differed from the national trends.
Methods:
RAI data from the CSMC Thyroid Cancer Center were reviewed to determine if RAI treatment was given appropriately. Kaplan-Meier curves were used to estimate disease-free survival for patients who received or did not receive treatment. RAI data from the NCDB were also used to compare how CSMC treatment rates compare nationally.
Results:
There were 444 CSMC patients identified with DTC between 2009 and 2012. Approximately 95% of the patients had papillary thyroid cancer (n=423) with 65% in the stage I risk group (n=290). Kaplan-Meier curves for stages I–III show that those who did not receive RAI treatment had 100% disease-free survival, which was better than those who had received RAI. However, given that the total population in both stages II and III is quite small, having received RAI ablation was not found to be statistically significant. Stage I patients who received RAI had a significantly increased incidence of recurrent disease. The NCDB RAI rates for all DTC stages in each year have consistently been over 50% with an overall treatment rate of 57%. There were significant differences in the treatment rates between CSMC and NCDB, with a decrease in the use of RAI in low-risk patients with stage I tumors at CSMC following institution of the guidelines.
Conclusion:
Prudent use of RAI treatment should be considered for low-risk patients. Ablation rates have been decreasing steadily at CSMC, particularly among low-risk patients, with the adoption of more stringent RAI treatment guidelines. It is apparent from our data that physician practices can change with the implementation and dissemination of evidence-based guidelines for the treatment of DTC with RAI.
Introduction
R
The incidence of thyroid carcinomas has increased with the majority consisting of American Joint Committee on Cancer (AJCC)/TNM stage I disease and microscopic well-differentiated thyroid carcinomas (4). Multiple studies have shown that RAI treatment for all tumor sizes has increased and particularly for low-risk thyroid cancers (TC), such as stage I and II (without distant metastases), many of these patients are probably being overtreated (5 –13). Between 1973 and 2006, the overall rate of RAI increased from 6.1% to a high of 48.7%. Among low-risk patients, RAI use went from 3.3% in 1973 to 38.1% in 2006 (7). While RAI can improve overall survival and decrease recurrence rates for high-risk patients with extensive locoregional disease or distant metastases, many studies have shown that postoperative RAI ablation does not change an already excellent outcome for patients with low-risk thyroid cancers (stage I and II without distant metastases).
RAI ablation has been well supported for aggressive disease including distant metastasis and gross extrathyroidal invasion but there have not been any randomized prospective treatment trials demonstrating that RAI reduces the risk of recurrence among patients whose disease-specific survival is high and whose risk for disease recurrence is relatively low. Indeed, other studies report unclear and inconsistent outcomes from RAI for low-risk patients (5,8 –18). Analysis of Mayo Clinic data found that there was no benefit to RAI ablation for low-risk tumors (19). Additionally, the potential for side effects exist and may exceed the benefits of RAI (7,8,11 –14,18,20 –23). Short- and long-term side effects include but are not limited to nausea, sialadenitis, leukopenia, parotiditis, dry eyes, and loss of taste and can occur in up to 10–30% of patients undergoing treatment (24). Additionally, overtreating these patients may also increase the risk of secondary primary malignancies (7,24,25). Given the lack of consensus regarding the benefits, if any, of treating low-risk patients with RAI and the potential for side effects and possibly secondary malignancies, it is prudent that clinicians conservatively manage very-low- and low-risk tumors.
Because of the lack of prospective data, definitive recommendations for any individual patient for RAI ablation is left up to the discretion of the treating physician according to the 2009 American Thyroid Association (ATA) guidelines (26). Furthermore, the recommendations for RAI ablation for low-risk DTC can be conflicting (27), however, the 2009 ATA guidelines provided for the first time a definitive recommendation against RAI use for well-differentiated papillary thyroid cancer (PTC)≤1cm without high-risk features (26). Using the National Cancer Database (NCDB), Roman et al. (28) report a change in practice after publication of the 2009 ATA guidelines reporting a 10% decrease in RAI use for this very low-risk subgroup of patients. As previously reported, guidelines for RAI use at our institution are relatively more stringent, particularly for stage I and II patients (20). This study explores the Cedars-Sinai Medical Center's (CSMC) RAI guidelines published in 2010 compared to the ATA RAI guidelines (updated in 2009) (Table 1) to determine how appropriately DTC patients were treated at CSMC and whether the dissemination of guidelines influenced the overall use of RAI (20,26). Additionally, we used RAI ablation rates from the National Cancer Database (NCDB) to see how the change in our RAI rates compare nationally, and whether there was a temporal relationship between education about the guidelines and subsequent RAI use.
RAI, radioactive iodine; ATA, American Thyroid Association; CSMC, Cedars-Sinai Medical Center.
Methods
In 2007, Cedars-Sinai Medical Center in Los Angeles, California, established a multidisciplinary Thyroid Cancer Center (TCC). An evidence-based review of the literature regarding the effectiveness of 131I ablation of DTC was carried out and the results were discussed among the group and eventually published (20). After approval by the CSMC Institutional Review Board, a thyroid cancer database was established for patients treated at this institution. Data collected include many variables such as patient demographics, operative and pathologic details, imaging studies, treatment information as well as serum thyroglobulin levels. The study population identified for the appropriateness of RAI treatment included patients who underwent total thyroidectomy at CSMC's TCC between the years 2009 (when the CSMC RAI guidelines were in practice) and 2012 and included patients who were diagnosed with either papillary or follicular thyroid carcinoma (FTC; n=444). Pathologic data were reviewed in detail and staged according to the TNM system, sixth edition, established in 2002. A retrospective review of medical records was performed to determine if patients received RAI ablation. When these data were unknown, follow-up with the referring endocrinologist was made to determine if RAI was given elsewhere as well as any other corresponding information. Based upon patient age, primary tumor size, tumor characteristics including extrathyroidal invasion, lymph node (LN) and distant metastatic involvement, and TNM stage, patients were classified as either being appropriately or not appropriately treated with RAI based on both CSMC and ATA RAI guidelines (Table 2) (20,26). Seven patients did not follow their physician's recommendation for or against RAI. Five patients with stage I PTC preferred RAI despite physician recommendation against it, and two patients with stage III/IV disease refused RAI despite physician recommendation for RAI. These patients are also included in Table 2 despite not being appropriately treated because of nonphysician-dependent issues. Kaplan-Meier curves using SAS 9.3 (SAS Institute, Cary, NC) were used to estimate disease-free survival among all stages of DTC for patients who received or did not receive RAI (Figs. 1 –4). Recurrent disease was defined as the presence of clinical disease by imaging or surgical pathology (i.e., lymph node metastasis) 6 months or more after initial thyroidectomy, having positive thyroglobulin levels 6 months after initial RAI treatment, or persistence of antithyroglobulin antibodies 3 years after initial RAI ablation.
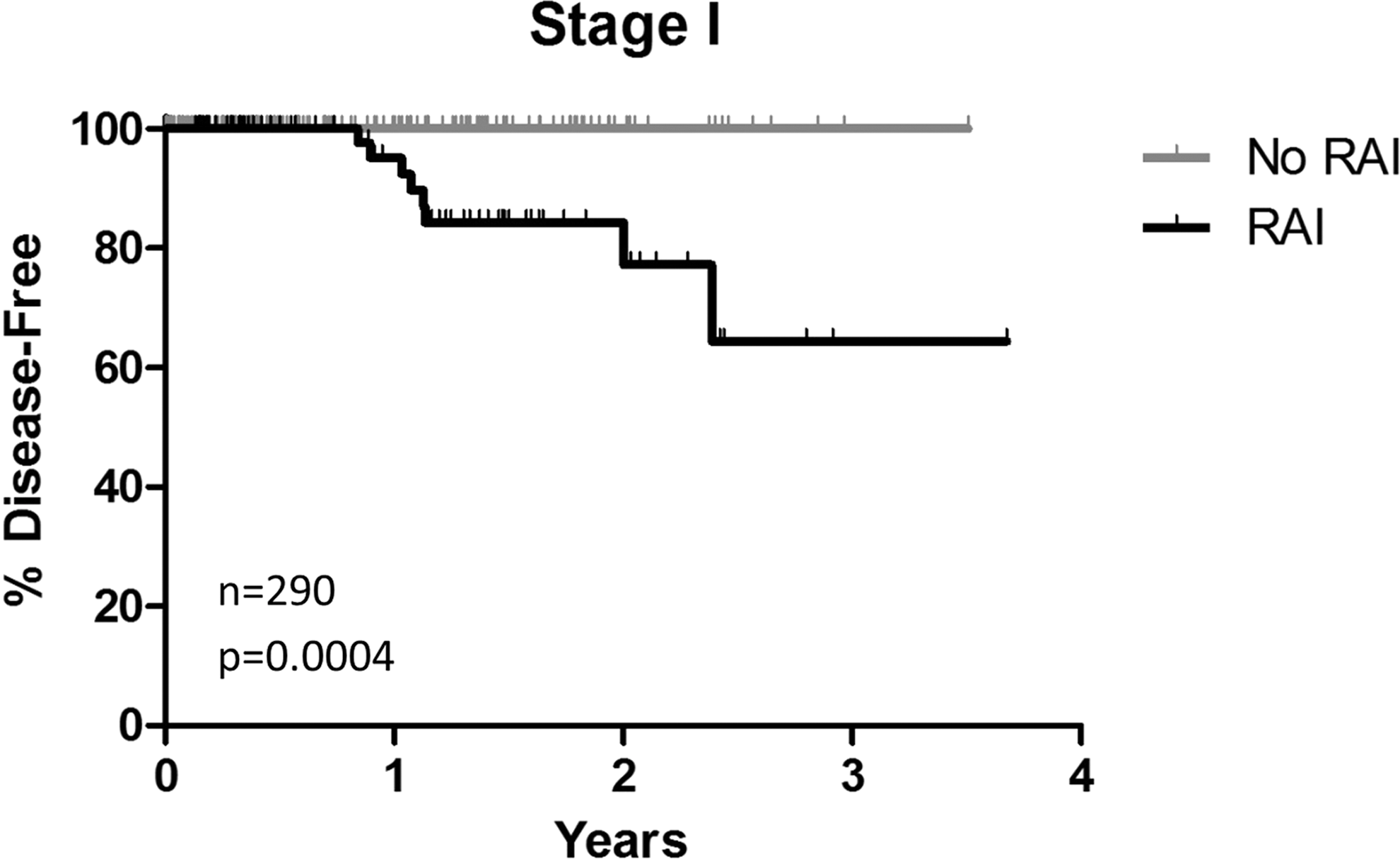
Kaplan-Meier disease-free curves for stage I differentiated thyroid cancer (DTC) patients seen at Cedars-Sinai Medical Center (CSMC) between 2009–2012.
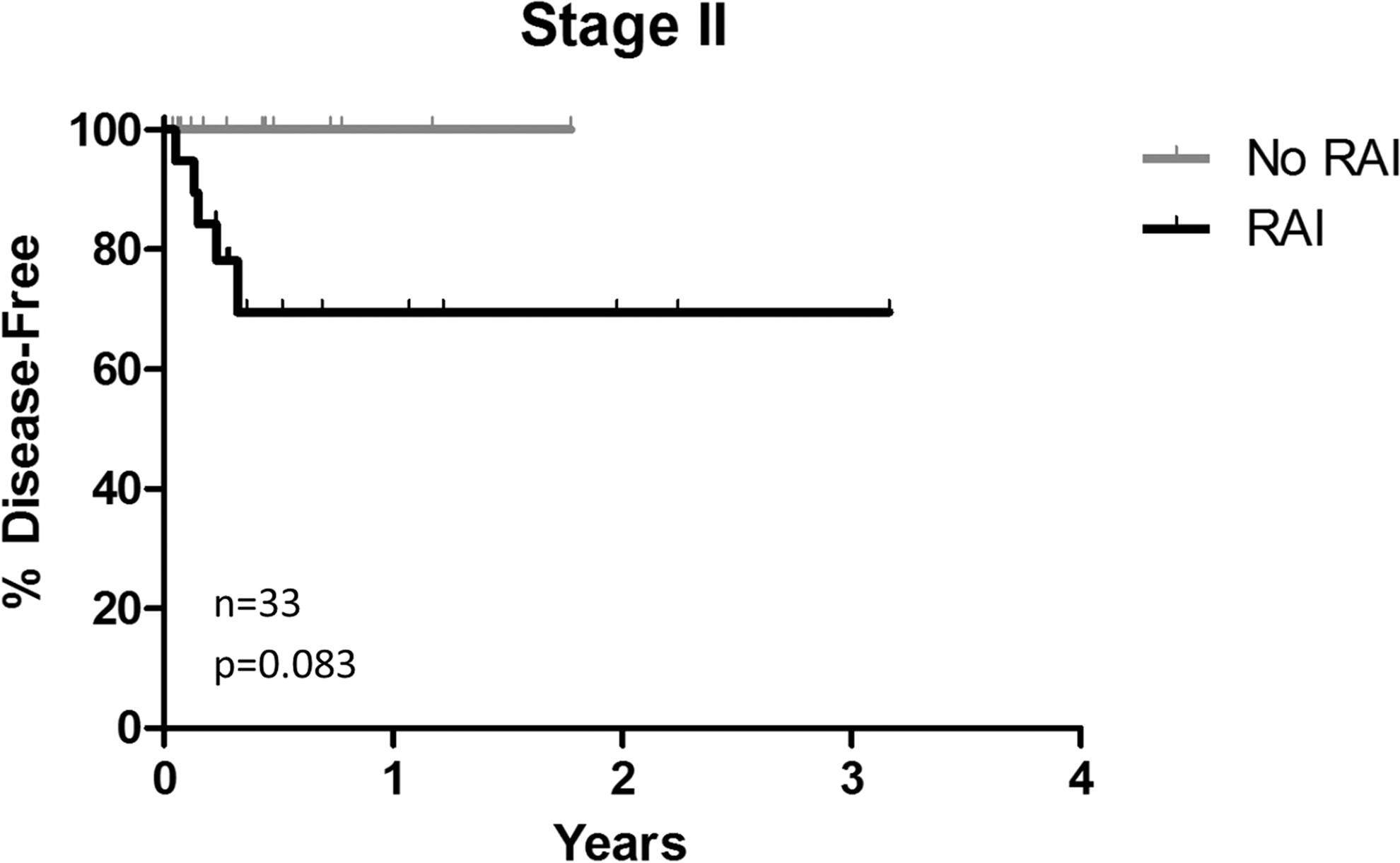
Kaplan-Meier disease-free curves for stage II differentiated thyroid cancer (DTC) patients seen at Cedars-Sinai Medical Center (CSMC) between 2009–2012.
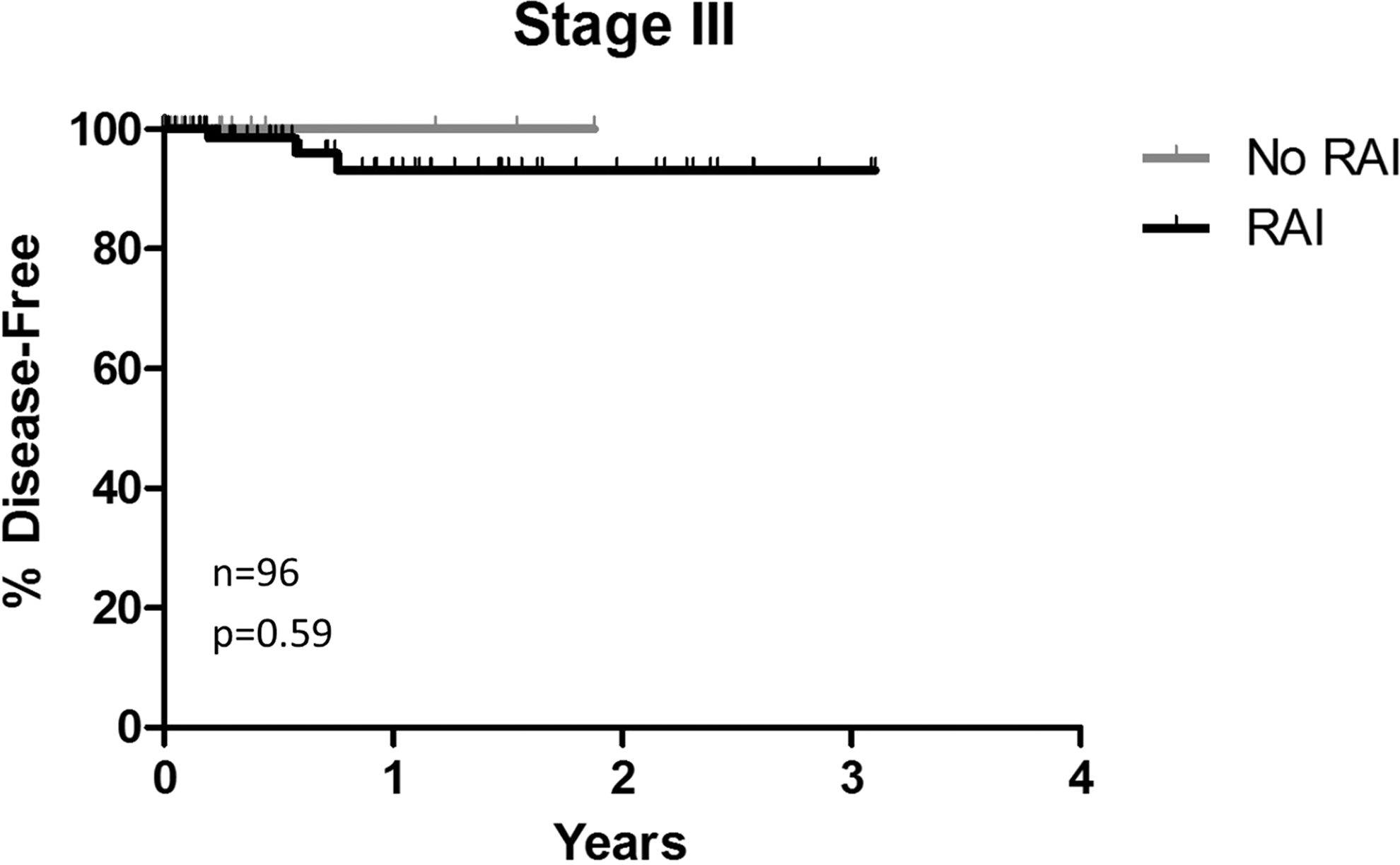
Kaplan-Meier disease-free curves for stage III differentiated thyroid cancer (DTC) patients seen at Cedars-Sinai Medical Center (CSMC) between 2009–2012.
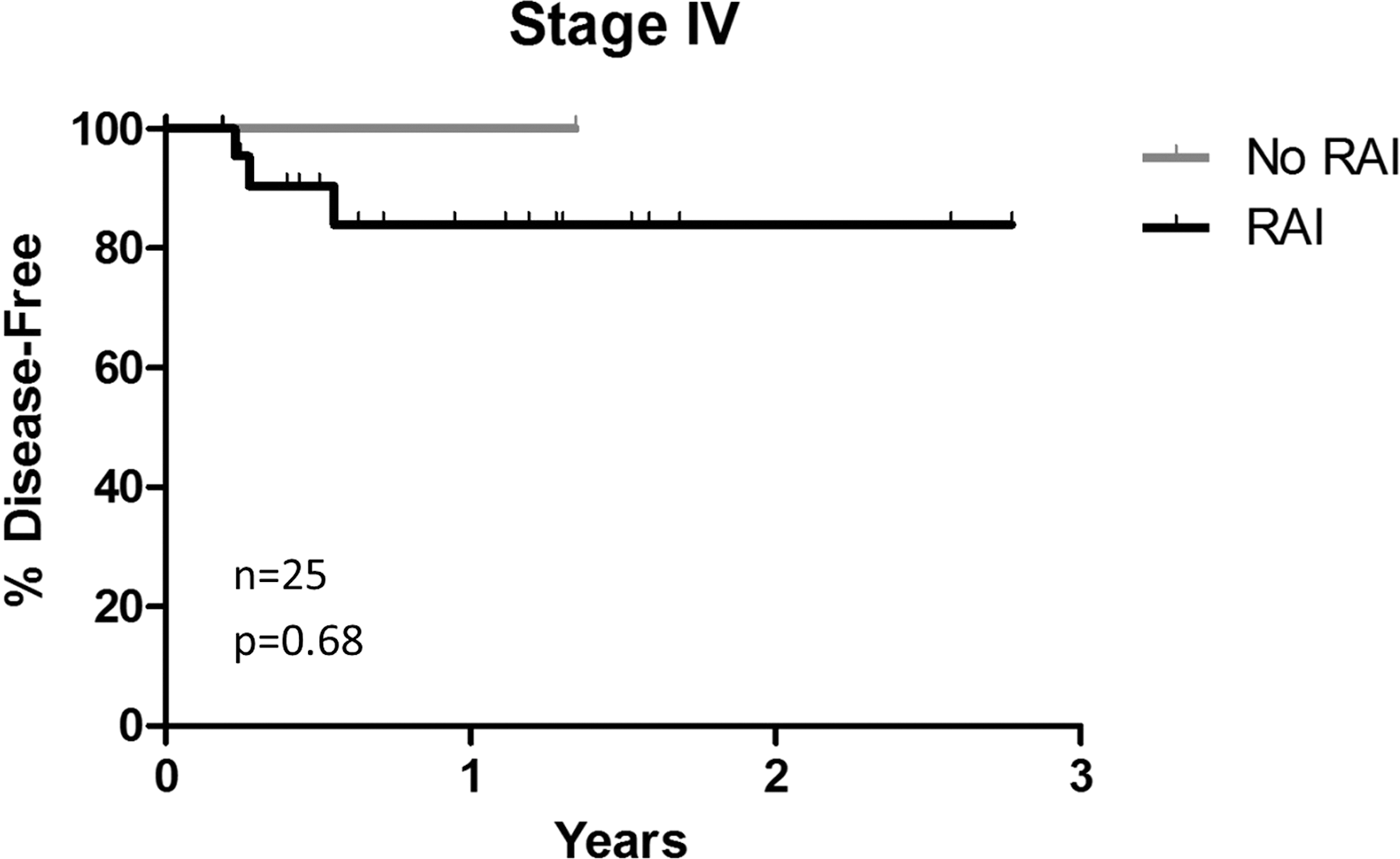
Kaplan-Meier disease-free curves for stage IV differentiated thyroid cancer (DTC) patients seen at Cedars-Sinai Medical Center (CSMC) between 2009–2012.
CSMC, Cedars-Sinai Medical Center; RAI, radioactive iodine; ATA, American Thyroid Association.
The CSMC RAI treatment rates from 1998–2011 were also compared to the NCDB RAI rates during the same period, irrespective of appropriateness of treatment, to determine how our rates compare nationally. The NCDB is a nationwide oncology outcomes database and clinical surveillance tool and is jointly supported by the Commission on Cancer of the American College of Surgeons and the American Cancer Society. Established in 1989, it includes more than 1,500 cancer programs and 29 million records from cancer registries in the United States and Puerto Rico (29). Data from approximately 180,000 DTC patients who underwent total thyroidectomy between the years 1998–2011 were included in the comparison. Differences in RAI rates over time between CSMC and the NCDB were tested using logistic regression, which included a Wald χ2 test of trend for the interaction of group with time. Multiple point wise comparisons between groups were adjusted using Tukey-Kramer multiple comparison procedures. All patients treated with RAI at Cedars-Sinai were included in these comparisons.
Results
There were 444 CSMC patients identified with PTC or FTC between the years 2009–2012 with a mean follow-up of 0.8 years (range, 0–3.7 years). Recurrent disease was found in approximately 4.5% of DTC patients (n=20). A majority of CSMC patients, approximately 95%, had PTC (n=423) with 65% in the stage I risk group (n=290). Women represented 74% (n=329) of the population. Mean age at surgery was 48 years and mean tumor size was 1.4 cm.
The CSMC RAI guidelines for DTC treatment are more stringent compared to the ATA in which many of the disease factors leave the decision to treat with RAI up to the physician. The overall percentage of patients appropriately treated between the years 2009 and 2012 for stages I to IV are comparable (Table 2). The seven patients who were inappropriately treated due to patient preference have been included in Table 2, however, there was no change in overall results due to the low number.
Kaplan-Meier curves for stages I–III show that those who did not receive RAI had a 100% disease-free survival rate that was greater than for those who had received RAI (Figs. 1 –4). As seen in Figure 1, stage I patients who received 131I had a significantly increased incidence of recurrent disease indicating a probable selection bias with patients having extensive LN involvement, especially those with lateral compartment disease being more likely to receive radioactive iodine than those with disease confined to the thyroid or with minimal central compartment LN involvement. Patients with stage II disease approached significance (Fig. 2), however, given the total population in both stages II and III is quite small (n=33 and 97, respectively), having received RAI ablation was not found to be statistically significant. Among stage IV patients (n=26), there was only one patient who did not receive RAI and consequently, it is not possible to draw any conclusions.
Between 1998 and 2011, more than 100,000 patients nationally received RAI ablation. The breakdown for each year is shown in Table 3. The NCDB RAI rates for all DTC stages in each year have consistently been over 50% with an overall treatment rate of 57%. In the regression analysis, the RAI rate decreased more among CSMC patients over time than observed at the national level (p<0.0001) (Fig. 5). Furthermore, beginning in 2007, CSMC data shows a significantly lower RAI ablation rate compared to the NCDB data. There were significant differences in the treatment rates between CSMC and NCDB driven by stage I patients (Table 4, Fig. 6). Interestingly, the CSMC RAI guidelines were in practice in 2007 when the decline in RAI was noted to be significantly lower when compared to the national rate. Subsequently, RAI rates among all thyroid cancer cases decreased from 50% in 2009 to 36% in 2012. Additionally, for stage I disease specifically, the rate among CSMC also decreased more over time compared to the NCDB data with CSMC having a significantly lower RAI rate starting in 2005. While rates of RAI among stage II and III also decreased (71% and 85% in 2009 to 67% and 70% in 2012, respectively), the CSMC sample sizes are very small and therefore there is no statistically significant difference between CSMC and NCDB RAI rates.
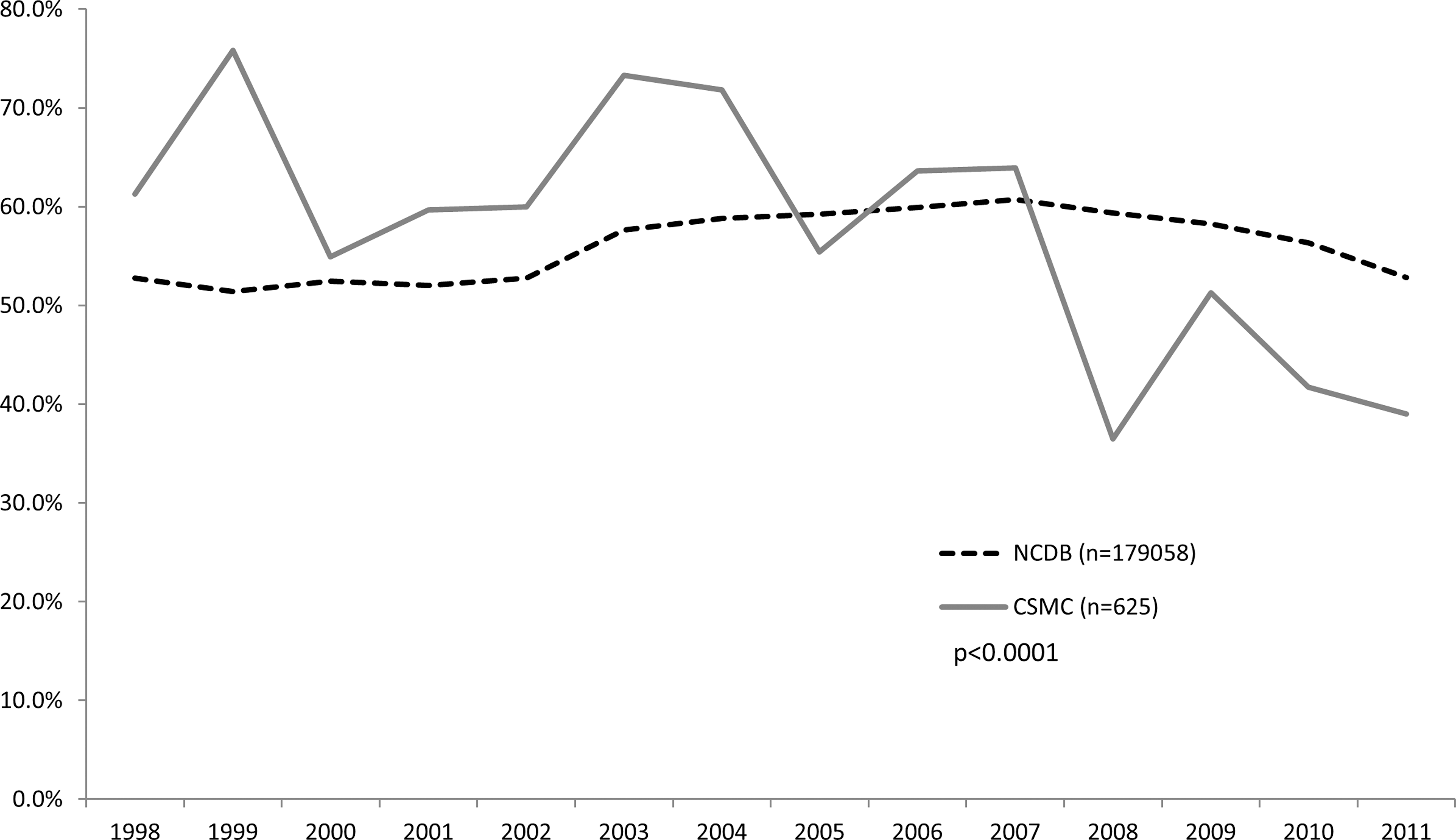
Radioactive iodine (RAI) treatment trends among all differentiated thyroid cancer (DTC) cases. n=total number of patients with DTC, %=number of patients treated with RAI. p Values represent the test of trend over time.
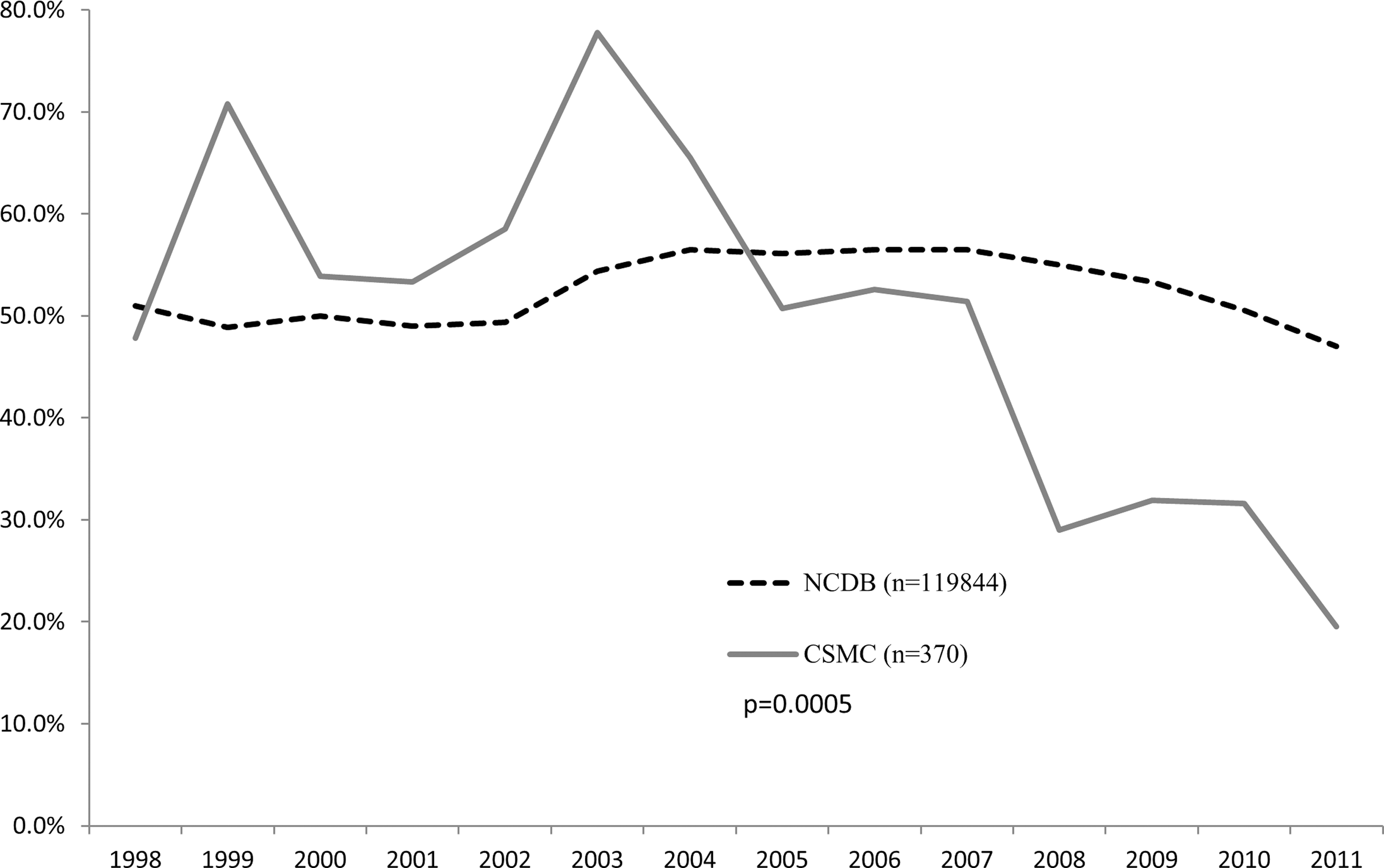
Radioactive iodine (RAI) treatment trends among stage I differentiated thyroid cancer (DTC) cases. n=total number of patients with DTC, %=number of patients treated with RAI. p Values represent the test of trend over time.
DTC, differentiated thyroid cancer; NCDB, National Cancer Database; CSMC, Cedars-Sinai Medical Center; pts, patients; RAI, radioactive iodine.
Discussion
Few studies have demonstrated significant differences in outcomes in low-risk DTC patients who received RAI (30). Among 704 patients with papillary thyroid microcarcinoma, no significant difference was seen in recurrence rates between those who received and did not receive RAI (p=0.17) followed over a median of 64 months (range, 1–185 months) (9). Furthermore, among 729 DTC patients treated between 1958–1998 (median follow-up of 11.3 years; range, 0.3–39.8 years), no difference was demonstrated in the 10-year local recurrence-free rate among low-risk patients stage I younger than 45 years of age (p=0.32), nor were there any deaths among patients who did and did not receive RAI (31). Recent studies by Schvartz et al. (12,13) demonstrated similar results among 1,298 low-risk DTC patients who received and did not receive RAI treatment followed for a mean of 10.3 years (95% confidence interval [CI] 9.8–10.7 years). Two large studies with long-term outcome data published in 2002 (n=2444) and 2006 (n=2936) also concluded that survival rates did not change among stage I (AJCC/TNM) or low-risk (MACIS<6) patients with or without treatment followed for 10,994 and 43,000 patient-years, respectively (32,33). Our data show that patients with stage I disease who received RAI actually had a significantly higher recurrence rate than those who did not and those with stage II disease had a nonsignificant trend toward higher recurrence in those who received RAI. These data are very similar to that reported by Hay et al. (19) who found that among 1,163 PTC patients with a MACIS score<6, the 20-year recurrence rate was significantly higher among those who received RAI (14% vs. 9%, p=0.008). These findings undoubtedly reflect a selection bias whereby patients with bulky nodal disease, especially in the lateral compartments or those with minor soft tissue invasion are more likely to receive RAI than those with no obvious invasion or nodal involvement. The recurrence rate in the former is higher than in the latter irrespective of treatment. It is acknowledged that patients who have not received RAI may have detectable levels of thyroglobulin while on thyroid hormone, presumably coming from normal thyroid remnant tissue. In those instances, disease-free survival was assumed if there was no increase in the thyroglobulin levels over time. Similarly, thyroglobulin that is detectable after RAI may not be coming from persistent disease but may be from residual normal thyroid tissue. These factors may lead to an underestimation of persistent disease in those who have not received RAI and overestimation of persistent disease in those who have received RAI. With the possible increased risk of secondary primary malignancies, acute and subacute side effects and unclear benefits of RAI ablation for low-risk DTC outcomes, including overall and disease-free survival, it is prudent that use of RAI be reconsidered for low-risk patients.
Ablation rates have been steadily decreasing at CSMC, particularly among low-risk patients, with the adoption of more stringent RAI treatment guidelines. Additionally, RAI treatment at CSMC was shown to be decreasing more rapidly compared to the NCDB national rates. While the NCDB rates for each year hovers at or above 50%, this implies that many patients are being overtreated because a majority of DTC patients are in the very-low- to low-risk category. The increase could be explained by many factors such as patient preference, the extensive variation in hospital protocol, and varying levels of physician expertise. Completeness of surgery also plays a major role in thyroid cancer outcomes and can be a factor in the decision to use RAI for ablation. Several studies have demonstrated that stage I patients who had surgery at facilities that focus on thyroid cancer had a much lower rate of RAI use compared to other facilities (5,10,30). For example, Haymart et al. (5) demonstrated increased RAI use associated with general surgeons with less than 10 years experience (52%) compared to endocrine surgeons with 10 years or more experience (p<0.001) (30%). Such specialized facilities provide more surgeon training and have better surgical outcomes from total thyroidectomy that resulted in less RAI use (5,10). Endocrinologists practicing alongside surgeons with an expertise in thyroid surgeries are also less likely to use RAI in part because the likelihood of a substantial amount of residual thyroid tissue remaining is decreased.
With the increased detection of DTC, the majority being low-risk cases, there is a need for a prospective randomized controlled study that looks specifically at the long-term effects of RAI on recurrence in this group of patients. Such a study involving 32 hospitals in France has been initiated to determine if the administration of 30 μCi of RAI with recombinant human thyroid stimulating hormone followed by monitoring for 5 years compared with simply monitoring for 5 years of low-risk patients not treated with RAI have a similar proportion of outcomes. The study's goals are to compare short- and long-term complications, disease-free survival during the first 3 years, quality of life, estimated costs of treatment and follow up for low-risk patients treated with RAI to determine the best course of therapy (34).
Limitations of using NCDB data include the lack of thorough review of each individual case and the specific reason for recommending RAI ablation, which may include factors such as the extent of LN involvement and family history. Additionally, it is also unknown how patient preference and physician recommendation were accounted for. Nevertheless, implementing an evidence-based treatment guideline did demonstrate a decrease in overall use of RAI ablation at our institution and we advocate for risk stratification of patients in the postoperative period to guide the physician toward or against RAI with the goal to decrease overtreating low risk patients. Our data demonstrate that RAI was given appropriately according to both CSMC and ATA guidelines. Patients with very low-risk or low-risk disease have an excellent prognosis and low risk of recurrence regardless of intervention or further treatment.
Limitations to our database include a relatively small sample size, low recurrence rate, and selection bias. While the outcome data are limited by short-term follow-up, our current disease-free survival rate is excellent with a 1.5% mortality rate, which is similar to data from other studies (12,17,32,33). However, longer follow-up is needed to determine the impact of RAI on recurrence rates. Additional limitations to this study include detection bias for low-risk thyroid cancer and selection bias for RAI use at our institution. Last, a sampling bias also must be acknowledged in this single institution and as a result, it may be difficult to apply this patient population and these findings to other DTC populations.
The dose of RAI used was not factored into this study and it is not known how dose may affect outcome. Histologic subtype was also not considered. For example, tall cell and insular variants of PTC are thought to act more aggressively, and therefore may warrant RAI treatment in some cases. Thus, it is difficult to generalize our results for all DTC patients because each case has unique factors that are considered in the decision to treat with RAI. Appropriate surgical management including total thyroidectomy with therapeutic central compartment dissection or potential prophylactic LN dissection or even lobectomy and thyroid hormone suppression/replacement seem to be sufficient for low-risk patients, particularly for younger patients without aggressive pathologic features. Long-term follow-up to include structural imaging and thyroglobulin monitoring is needed to determine whether withholding RAI therapy is indeed justified and may be associated with improved disease-specific survival (35). Roman et al. (28) demonstrated a 10% decrease in RAI use in stage I patients from 2004 to 2011, while we showed a 41% decrease in RAI use consistent with our guidelines being more stringent than the 2009 ATA guidelines (26). It is apparent from our data as well as other sets (28,35) that physician practices can change with the implementation and dissemination of evidence-based guidelines for the treatment of well-differentiated thyroid cancer with radioactive iodine.
Footnotes
Author Disclosure Statement
No competing financial interests exist.