
Abstract
Background:
Thyroid nodules are less common in children than adults, but the risk of malignancy in thyroid nodules is much higher in children. The ability to characterize pediatric thyroid nodules has improved with the use of ultrasound-guided fine-needle aspiration, the Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) classification system, and expanded molecular testing. Nevertheless, stratification criteria to predict thyroid malignancy in children are poorly defined. Our objective was to determine if clinical presentation and molecular genetics could predict malignancy in pediatric thyroid nodules.
Methods:
Retrospective chart review of patients ≤18 years of age at the Children's Hospital of Pittsburgh of the University of Pittsburgh Medical Center with the diagnosis of a thyroid nodule from January 2007 to January 2012 was conducted. Eighty-nine subjects fulfilled the inclusion criteria: 1) thyroid nodule ≥0.8 cm and biopsy (n=76), or 2) thyroid nodule ≥0.8 cm, no biopsy, and ultrasound follow-up for at least 2 years (n=13).
Results:
Twenty-four (27%) of 89 patients were diagnosed with thyroid cancer (50% papillary thyroid carcinoma [PTC], 50% follicular variant of papillary thyroid carcinoma [FVPTC]). Features associated with malignancy included larger nodule size, palpable nodule, or palpable lymphadenopathy. There were no differences in presenting features between patients with PTC and those with FVPTC. Thyroid malignancy was diagnosed in all nine patients with a molecular abnormality (BRAF, RAS, RET/PTC, PAX8/PPARγ).
Conclusions:
Clinical features, FNA cytology, and molecular genetics are valuable tools to discriminate benign from malignant nodules in pediatric patients. This information is important to direct subsequent clinical management.
Introduction
T
Ultrasound-guided fine-needle aspiration (FNA) has been demonstrated to have a high sensitivity and specificity in identifying malignancy in pediatric thyroid nodules (11). Molecular analysis may further improve the positive predictive value in those cases with indeterminate FNA cytology (12,13) and may be useful in guiding subsequent management (14,15). Despite improved imaging and molecular techniques, the ability to discriminate between malignant and benign nodules on clinical grounds alone, and thus avoid anxiety and prolonged evaluations, has not been possible in the pediatric population. Most previous case series of children and adolescents with thyroid nodules report only a small number of patients or are limited by ascertainment bias, such as including only patients who had undergone a surgical procedure.
Our goal was to determine if clinical presentation, biopsy findings (16), and/or molecular markers could predict thyroid malignancy in children ≤18 years of age who presented with a thyroid nodule measuring ≥0.8 cm.
Materials and Methods
Study design
We reviewed consecutive outpatient clinic records for pediatric patients (≤18 years of age) referred to our tertiary care center pediatric endocrinology clinic at the Children's Hospital of Pittsburgh of the University of Pittsburgh Medical Center (UPMC) between January 2007 and January 2012. Our initial chart search was performed using all diagnostic codes that could encompass thyroid nodule, including thyroid nodule, thyroid cancer, thyroid cyst, goiter, and multinodular goiter. Charts were then reviewed by one member (M.B.) of the study team for appropriate inclusion based on the criteria listed below. In the absence of a uniform standardized protocol for pediatric thyroid nodule evaluation, specific patient management was based on physician preferences. Multidisciplinary care for patients encompassed pediatric subspecialty services including otolaryngology, nuclear medicine, pathology, interventional radiology, surgery, and in some cases oncology. This protocol was approved by the Institutional Review Board at the University of Pittsburgh.
Eighty-nine subjects fulfilled the inclusion criteria: 1) thyroid nodule ≥0.8 cm and biopsy (either FNA or core biopsy), (n=76) or 2) thyroid nodule ≥0.8 cm and no biopsy and either initial surgery or ultrasound follow-up for at least 2 years from time of initial evaluation (n=13). Thyroid nodules measuring <0.8 cm or those occurring in young adults over the age of 18 years old were excluded. Patients with prior irradiation, previous malignancy, or a predisposing genetic cancer syndrome were also excluded. The size criteria were chosen according to the ability of interventional radiology to accurately perform the FNA procedure. Generally, physicians at our institution obtain FNA on nodules ≥1 cm. FNA is attempted on nodules between 0.8 and 1.0 cm if concerning features are observed on ultrasound.
Procedures
With the exception of FNAs performed at outside hospitals prior to referral to our facility, ultrasound-guided FNA biopsies were performed either at the Children's Hospital of Pittsburgh of UPMC (CHP), UPMC Presbyterian Hospital (UPMC-PUH), or UPMC Shadyside Hospital (UPMC-SHY) in Pittsburgh, Pennsylvania, depending on patient age and preference (n=70). All FNAs within the UPMC system were performed using ultrasound guidance with or without anesthesia, based on patient age and preference. Standard technique includes a 25- to 27-gauge FNA needle and three to five passes at each site performed depending on the ability to obtain adequate tissue and the ability of the patient to tolerate the procedure. Six subjects had FNA at an outside hospital prior to referral; details regarding these procedures were not available.
Core biopsies (using 20- to 22-gauge needles) were performed in rare cases (n=4) with a suboptimal FNA, or without concurrent FNA. Aspirated material was used for smear preparation, including air-dried smears stained with a Romanowsky-based stain, and alcohol-fixed slides stained with the Papanicolaou stain. All FNA specimens starting in September 2008 were classified by the Bethesda System for Reporting Thyroid Cytopathology (TBSRTC), which is a six-tier graded classification system that provides a reporting scheme for FNA cytology. The categories are 1) nondiagnostic/unsatisfactory (ND); 2) benign (BEN); 3) atypia/follicular lesion of undetermined significance (AUS/FLUS); 4) suspicious for follicular or oncocytic neoplasm (SFON); 5) suspicious for malignancy (SM), and 6) positive for malignant cells (PM) (15). A previous study from our institution confirmed that the TBSRTC system can be applied to children (11). Cases prior to September 2008 were retrospectively categorized based on cytology reports.
Material was also obtained for potential molecular marker studies on all patients after April 2007 and only submitted for testing if indeterminate (AUS/FLUS, SFON, SM), positive for malignant cells, or from large nodules (≥4 cm) with an FNA diagnosis of negative for malignancy. All specimens were evaluated by pathologists specializing in cytopathology and/or pediatric pathology as previously described (11,16).
Mutational analysis for the BRAF, NRAS codon 61, HRAS codon 61, and KRAS codons 12 and 13 was performed using real-time polymerase chain reaction (PCR) and post-PCR fluorescence melting curve analysis on the LightCycler (Roche Applied Science). RET/PTC1, RET/PTC3, and PAX/PPARγ variants were detected by real-time reverse transcriptase PCR with primers designed to flank the respective fusion point on ABI7500 (Applied Biosystems). A subset had the above chromosomal rearrangements evaluated with florescence in situ hybridization techniques. These techniques have been previously described (13).
Statistical analysis
Patient information including age, race/ethnicity, sex, body mass index (BMI), laboratory data, radiographic data, pathology results, and surgical procedures were obtained from hospital records and recorded in a secure database with patient identifiers removed. Demographics were summarized using medians and interquartile ranges (IQRs) for nonparametric or mean and standard deviation for parametrically distributed data. Frequencies are displayed as percentages. Comparisons of continuous variables between two groups of parametric and nonparametric data were performed using t-test or Wilcoxon-rank sum as appropriate. Chi-square test or Fisher's exact test (expected values <5) were used as appropriate for comparisons of proportions or categorical variables. Associations were tested using linear regression analysis and Pearson or Spearman correlation as appropriate. SAS software was used to perform the statistical analysis (SAS Institute).
Results
Subject population
A total of 357 patient charts were identified by our search criteria. Of these patients, 50% (180/357) had been referred for evaluation of another thyroid condition and did not fulfill our inclusion criteria. Of the remaining 177 (50%) patients, 88 patients did not have a thyroid nodule on further evaluation, the nodule was <0.8 cm, or the patient did not have sufficient follow-up (e.g., <2 years follow-up without biopsy or repeat ultrasound) to determine the status of the nodule. One patient was excluded due to previous neck irradiation for prior malignancy. All subjects with known cancer syndromes or other conditions that would predispose them to increased risk of malignancy were excluded. A total of 89/357 (25%) patients were then included in our analysis (Fig. 1).
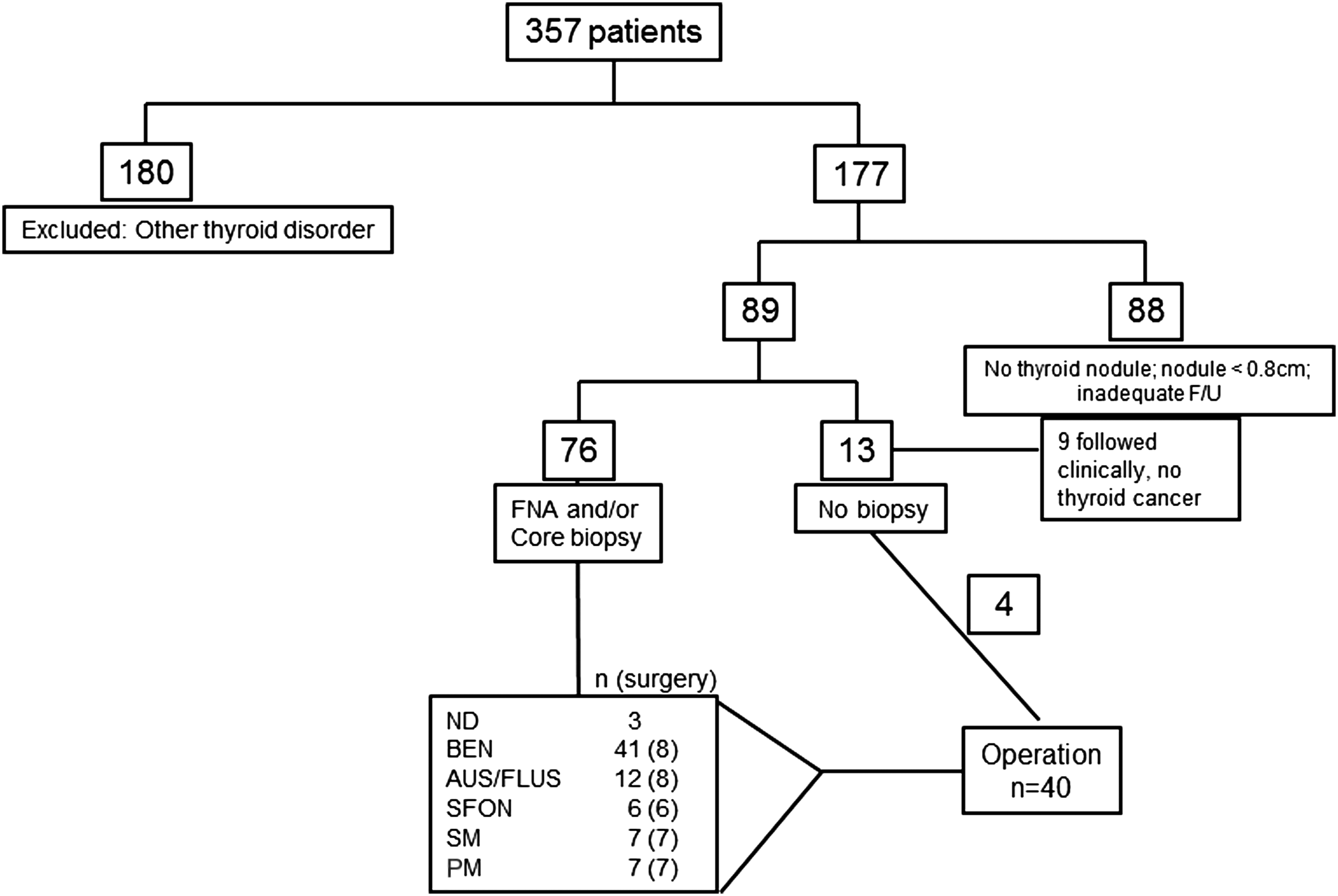
Patient selection flowchart. BEN, benign; ND, nondiagnostic; AUS/FLUS, atypia of undetermined significance/follicular lesion of undetermined significance; SFON, suspicious for follicular neoplasm; SM, suspicious for malignancy; PM, positive for malignant cells.
Description of 89 subjects with thyroid nodule criteria
The median age was 15.1 years (IQR 12.6–16.1 years), median BMI percentile was 85th (IQR 50–92), and median thyrotropin (TSH) 1.3 μIU/mL (IQR 0.75–5.1 μIU/mL). Eighty-one percent were female and 68% were Caucasian. The majority of our patients were 12–18 years old (80%, 71/89); only two patients were <6 years. The reasons for referral included palpable nodule (63%, 56/89), incidental nodule on imaging (17%, 15/89), and “neck/thyroid enlargement” or “goiter” (20%, 18/89). Subsequent workup at our center was physician dependent and included thyroid function tests in 78 (87%) and thyroid ultrasound in 75 patients (84%). Imaging studies in remaining subjects included computed tomography scan in two (2.2%), magnetic resonance imaging in two (2.2%), or radioiodine scan in three (3.4%). The indications for thyroid scan and uptake were hyperthyroidism in one patient and hypothyroidism in two patients. Prior to referral to CHP, six subjects (6%) had an FNA biopsy performed at an outside hospital without repeat FNA at CHP. As per our standard protocol, the results were verified by our pathologists in three of these specimens. Thyroid ultrasound had been performed at an outside hospital in 10 patients and was not repeated at our institution.
A total of 76/89 (85%) patients had pathologic assessment of their nodule. The majority had an FNA biopsy, with four patients undergoing core needle biopsy. The remaining 13 patients did not have a preoperative pathologic evaluation; these patients either went directly for an operation without having an FNA performed (n=4) or had follow-up (n=9) over a minimum time period of 2 years with regression in size of nodule and “benign findings” on ultrasound, thus foregoing an FNA. The decision to perform FNA was physician dependent and was based on imaging findings, size, and clinical judgment. None of the nine patients followed for 2 years developed thyroid malignancy.
Forty of 89 (45%) patients underwent surgical procedures. Final pathologic diagnoses were conventional papillary thyroid carcinoma (PTC) (n=12), follicular variant of papillary thyroid carcinoma (FVPTC) (n=12), benign follicular adenoma (n=12), or multinodular goiter (n=4). To summarize, 24/89 (27%) of our patients were diagnosed with thyroid cancer. No thyroid cancers were detected in the nodules that measured between 0.8 and 1.0 cm on ultrasound.
Comparison of characteristics between benign and malignant nodule groups
To identify features distinguishing between benign and malignant nodules, patient and nodule characteristics were compared between the two groups. Age, BMI, and sex did not differ between the groups (Table 1). Significant differences between the two groups were the presence of a palpable nodule (rather than incidental finding), larger nodule size in those with malignancy, palpable lymphadenopathy (LAD), the presence of both palpable nodule and LAD, and presence of a molecular mutation (Table 1). Historical features such as family history of thyroid cancer did not differ between groups. There was no statistical difference between the two groups regarding report of compressive symptoms, and 3/24 (12%) of those with thyroid cancer and 2/65 (3%) of those without thyroid cancer reported symptoms; however, more than 50% (3/5) of those who reported compressive symptoms had thyroid cancer. There were no differences in clinical features between those diagnosed with conventional PTC compared with those diagnosed with FVPTC (Table 2). The presence of palpable lymphadenopathy in evaluation of a thyroid nodule had a high specificity for malignancy (95%) with a low sensitivity (33%) (Table 3). A palpable nodule had a sensitivity of 87% in identifying malignancy; this feature had a negative predictive value of 90% (Table 3).
p<0.05.
BMI, body mass index; IQR, interquartile range; LAD, lymphadenopathy; TSH, thyrotropin; U/S, ultrasound.
FVPTC, follicular variant of papillary thyroid carcinoma; PTC, papillary thyroid carcinoma.
The sensitivity, specificity, and positive and negative predictive values of the ultrasound features of the nodules are reported in Table 3. These results must be interpreted with caution because multiple ultrasonongraphers performed the imaging in the absence of a standard reporting protocol, which likely resulted in greater variability in the reports. Thus, reports regarding regional lymph nodes were inconsistent and dependent on practitioner requests. When reported, the presence of calcifications, increased vascularity and hypoechogenicity of nodules were all sensitive findings (88%, 90%, 80% respectively) with a high level of negative predictive value (85%, 89%, 89%). At least one of these features was present in 19/24 patients with thyroid cancer. Preoperative ultrasound identified lymph node metastases in only three of nine patients in whom lymph node metastases were detected after surgical excision. The diagnosis of thyroid cancer was not made solely on lymph node biopsy results in any patient in this study.
Final cytology and patient outcome
The most common cytology result was BEN found in 41/76 (54%) patients undergoing FNA. Notwithstanding the reassuring FNA results of BEN, nine of these patients subsequently underwent an operation for removal of the nodule. The reasons for surgery included family preference (n=5), symptomatic nodule (n=3), and surgeon preference (n=1). Four of the nine patients with benign FNA undergoing surgery had a malignant pathology. These included two patients who had an FNA done only at outside hospitals without repeat FNA at our institution. Despite being offered the opportunity to repeat the FNA, two families elected to proceed with operations without repeat FNA. The final pathology was PTC in both cases.
The other two patients with malignancies elected operations because of large nodule size (4.4 cm on ultrasound, 1.8 cm in largest dimension on final pathology) and family preference; the final histological diagnoses were PTC and FVPTC, respectively. Retrospective review of these FNA biopsy cases confirmed the original diagnoses, and thus, likely represent sampling error. Other than size, ultrasonographic features did not specifically influence the decision for surgery in these two individuals, although one patient was noted to have a solid, vascular nodule on ultrasound. Apart from size, no specific concerning features were mentioned in ultrasound report for the other patient. The remaining 32 patients with a BEN cytology deferred surgery and agreed to long-term surveillance; none developed thyroid cancer in the follow-up period. Three patients with FNA interpreted as ND, elected to be followed clinically; none have been found to have thyroid malignancy.
All subjects with FNA cytology finding of SFON, SM, or PM underwent either lobectomy or complete thyroidectomy (Table 4). In those with an FNA cytology of AUS/FLUS, surgical intervention was performed in 67% (8/12) with reasons for surgical intervention including increase in nodule size (n=2), repeat FNA diagnosis of SFON (n=1), nodule failed to decrease in size (n=1), or family or surgeon chose surgical intervention (n=4). All eight nodules were benign on final pathology. The fact that all of our AUS/FLUS nodules were benign on final pathology may be due to low sample size.
FNA, fine-needle aspiration.
Surgical interventions
Specific surgical interventions included initial total thyroidectomy in 7/7 (100%) subjects with a preoperative FNA diagnosis of PM, 6/7 (71%) patients with SM, and 2/6 (33%) patients with SFON (Table 4). All other subjects (25/40) undergoing an operation underwent an initial thyroid lobectomy with subsequent completion thyroidectomy if malignancy was diagnosed from initial lobectomy (5/25). No patient developed vocal cord dysfunction or paralysis. Temporary postoperative calcium supplementation was necessary in eight patients. One patient with multifocal PTC (RET/PTC-positive), extensive lymph node disease, and aggressive neck dissection required long-term calcium and calcitriol supplementation. At operation, 15/24 (58%) patients with thyroid cancer had at least one lymph node resected with 10/15 (64%) patients having lymph nodes metastases (range 1–50). Distant metastases (e.g., pulmonary metastases) were not present in any of the patients in this study. TNM staging for those with molecular mutations is listed in Table 5. With the exception of one patient, all remaining patients were either T1 or T2 and Nx, N0, or N1a. The four N1a patients had two (n=3) or three (n=4) positive nodes. The remaining patient, a 14-year-old boy with no significant medical history, had T4aN1bM0 stage disease with 46/104 nodes sampled positive for metastatic disease.
LN, lymph node.
Molecular mutations and correlation with clinical findings
Excluding the FNA cases with BEN or ND results, molecular mutation testing was performed in 35 subjects. Nine patients (Table 5) were positive for a molecular marker known to be associated with thyroid cancer: BRAFV600E (n=2), RAS (NRAS61, n=1 and HRAS61, n=2), RET/PTC (n=3), and PAX8/PPARγ (n=1). In one case (NRAS) testing was positive at resection, but had not been performed on the FNA specimen. All nine mutation-positive subjects were found to have either conventional PTC (n=5) or FVPTC (n=4). FNA results in six of these nine mutation-positive subjects were interpreted as SM or PM. Two of the nine patients had an FNA result of SFON. One patient had a BEN FNA result and a large nodule (4 cm); mutation analysis was performed postoperatively rather than at the time of FNA. The RAS mutation was present in these latter three subjects. Conversely, a mutation was not identified in 61% of children with thyroid cancer.
One of the three patients with a RAS mutation underwent initial lobectomy followed by completion thyroidectomy. Patients positive for RET/PTC and PAX8/PPARγ underwent total thyroidectomy, despite indeterminate pathology on FNA in two cases (SFON, n=1 and SM, n=1). All five patients with BRAF or RET/PTC mutations had lymph node metastases at the initial surgery and underwent central neck (n=3) or central and unilateral, lateral neck (n=2) dissections. Patients with RAS or PAX8/PPARγ mutations had no regional lymph node metastases; however, fewer lymph nodes were resected in these patients (zero or one in RAS-positive patients and eight in PAX8/PPARγ-positive patients). The characteristics of the mutation-positive patients are summarized in Table 5; however, there were too few patients with specific mutations to perform statistical comparisons.
Discussion
Thyroid nodules and thyroid cancer are uncommon among children. Discovery of a thyroid nodule in a child warrants thorough evaluation because the incidence of thyroid cancer in a nodule is higher in children than among adults (1). Most published guidelines for management of thyroid nodules are tailored to adults (18). Evidence-based guidelines directly aimed at the pediatric population are not yet available. Currently available algorithms for pediatric patients are based on expert opinion, small case series, or data extrapolated from studies largely done in adult populations (7). Our results provide potentially useful data for the evaluation and management of thyroid nodules in the pediatric population.
This study found that 27% of children presenting to our institution with a thyroid nodule ≥0.8 cm had thyroid cancer. No cancers were identified in nodules <1 cm on ultrasound evaluation. This percentage is higher than the reported rates of thyroid cancer in adults with thyroid nodules (5%–10%) (3). Our results are comparable to the previously reported prevalence of thyroid cancer in children with thyroid nodules (2,3). Many of the studies reporting higher percentages of malignancy were surgical case series with malignancy rates of 36%–43% (19 –21). Surgical case series studies are subject to verification bias and inherently overestimate the risk of cancer by excluding subjects managed solely with observation. For example, if we included only our surgical patients, we would have estimated the prevalence of thyroid cancer in pediatric thyroid nodules to be 60%. The prevalence of thyroid malignancy in our population may have been influenced by our status as a tertiary care center; therefore, nodules that had been evaluated and determined to be benign at an outside institution are likely underrepresented in our population.
The reason for referrals differed between those with and without malignancy. Patients referred for incidentally found nodules were less likely to have malignancy compared to patients referred for a nodule palpated by a clinician. This difference has not been previously reported in other case series, although reasons for referrals to our center were similar to other studies (1,3,21). It has been speculated that the improved resolution of thyroid imaging with detection of smaller nodules is one reason for the increasing incidence of pediatric thyroid cancer. With the exception of 1/24 (4%) patients, our findings indicate that incidentally found lesions did not substantially contribute to the overall pediatric thyroid cancer incidence in our population (19). Nevertheless, incidental nodules still warrant careful clinical evaluation and follow-up imaging (17,22).
Thyroid nodules that were palpable on exam were more likely to be malignant, and a palpable nodule was a sensitive (87%) physical exam characteristic. Twenty of 24 (83%) patients in our study with thyroid cancer had a palpable thyroid nodule at presentation. Nevertheless, 58% of the patients in the group without cancer also had palpable nodules. Palpable lymphadenopathy and larger nodule size were associated with an increased risk for malignancy (p=0.001 and 0.046). Furthermore, the combination of palpable lymphadenopathy and a thyroid nodule was highly specific for a diagnosis of thyroid cancer (95%). Over 50% of our patients with thyroid cancer had regional lymph node metastases at the time of initial surgery, much higher than the typical rate of lymph node involvement in adults (3). Hence, an examiner should be concerned about the increased risk of malignancy in the presence of a thyroid nodule accompanied by lymphadenopathy. This finding emphasizes the importance of physical examination in these young patients by all health care professionals (1,19,21,23).
The relationship of nodule size to cancer risk has been debated. While some studies have not found a relationship between size and the presence of malignancy (1,19,24), a recent study did report a correlation (3). Our finding may be biased based on the fact that the majority of our malignant cases were palpable nodules, and therefore likely to be larger in size than those detectable only by imaging. Additionally, the difference in nodule size between the groups may be due to the inclusion of subcentimeter nodules in our design, all of which were benign.
The role of autoimmune thyroid disease (ATD) as a risk factor for pediatric thyroid cancer and the necessity of screening patients with ATD for thyroid cancer has been deliberated (25 –27). Two subjects had a prior diagnosis of Hashimoto's thyroiditis; the majority of antibody-positive subjects were identified during the thyroid nodule evaluation. Our study was not designed, and was therefore underpowered, to address this question; we found no difference in median TSH level or presence of positive antibody titers (anti-thyroglobulin and anti-thyroid peroxidase antibodies) in benign versus malignant groups.
We found an excellent (100%) correlation between the presence of a molecular marker and malignancy in our patients. However, absence of positivity for a mutation certainly did not exclude thyroid cancer. Therefore, the molecular testing used at our institution can be helpful to “rule-in” malignancy, particularly in indeterminate nodules, but a negative result does not exclude malignancy. Similar to findings in adults, BRAF and RET/PTC were associated with conventional papillary carcinomas and RAS and PAX8/PPARγ mutations were associated with follicular variant of papillary pathology (28,29). Although the number of mutation/rearrangement-positive cases was too low to make statistical inferences, all patients with BRAF and RET/PTC had regional lymph node metastases, while none of the patients with RAS and PAX8/PPARγ had reported lymph node metastases. The caveat is that directed lymph node sampling was performed less frequently in the latter group. FNA evaluation also stratified these patients, with 95% (38/40) of patients with malignancy detected by FNA as SFON or above (only two false negatives). However, molecular genetic analysis as performed here cannot be relied upon in isolation because depending on molecular testing alone would have missed nearly 60% of cancers. Nevertheless, when mutations or rearrangements are present, particularly BRAF mutations which are known to be more commonly associated with PTC, the risk for a malignant diagnosis is increased in an indeterminate FNA case, and there is an impetus for a total thyroidectomy rather than a two-stage procedure, (i.e., initial lobectomy followed by completion thyroidectomy) (14,30).
While the majority of patients with a mutation would have undergone surgical removal of their nodule regardless of the results of the mutational analysis, the one patient with benign cytopathology who was subsequently found to have thyroid cancer might have been identified earlier had the molecular mutation panel been performed on FNA. Therefore, this mutation panel may be worthwhile for children with large nodules or other suspicious ultrasound features, which are reported as benign on FNA; however, sampling issues can confound evaluation of larger nodules. Additionally, the presence of mutations known to be associated with more aggressive lymph node metastasis may lead towards more extensive lymph node dissection.
The overall prevalence of molecular mutations in our patients with thyroid cancer (39%) is similar to a previous report in children (11), but lower than that reported in adults (29). The gap between the percentage of mutation-positive pediatric thyroid cancers and mutation-positive adult thyroid cancers is likely due to the presence of other mutations not tested for on the mutation panel used during the time frame of this study and adds further evidence that pediatric thyroid cancer is likely biologically different than adult thyroid cancer. Next generation sequencing (NGS) offers a cost-effective approach with high throughput and parallel sequencing to analyze for a larger number of genetic variations in small-volume samples. This technique has recently been adopted as the standard for molecular testing of thyroid nodules at our institution (31). Use of NGS for pediatric thyroid cancer will likely discover novel genetic markers and provide more accurate prognostic information (32). Whereas the identification of a positive molecular marker can be a useful adjunct in those patients with indeterminate cytology, a negative result on mutation testing does not exclude the possibility of malignancy (14,33,34).
We were able to confirm the findings of similar previous case series of pediatric thyroid nodule patients with a thyroid cancer prevalence of 27% in this group. Our study affirms that a child with a clinically palpable nodule or palpable lymphadenopathy is more likely to have malignancy than the child with a nonpalpable nodule or lack of lymphadenopathy. Furthermore, the presence of both lymphadenopathy and a palpable nodule provided even greater discrimination between malignant and nonmalignant nodules. Nevertheless, our findings suggest that even incidentally found lesions warrant evaluation. We found that FNA of thyroid nodules provided a high level of discrimination between malignant and nonmalignant lesions. Our data confirm the impact of adjunct molecular testing on aspirate material and its supportive role in the management of pediatric patients with thyroid nodules. The advent of NGS testing will most likely help to distinguish benign from malignant lesions in the face of indeterminate cytology results in the future. Thorough evaluation of each patient that includes clinical exam, imaging, FNA cytology, and molecular testing is collectively important to establish a diagnosis and to direct subsequent therapy, while minimizing patient discomfort and surgical procedures in children and adolescents with thyroid nodules. In addition, this report highlights the importance of a multidisciplinary approach given that no parameter by itself is has sufficient sensitivity and specificity, and thus all contribute to the optimal care of a pediatric patient. The multifaceted care necessary for these patients is emphasized and may help in creating diagnostic algorithms specific for pediatric patients with thyroid nodules.
Footnotes
Author Disclosure Statement
MB: The views expressed in this publication are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States government. All other authors have no disclosures.