
Abstract
Background:
Aggressive histopathologic subtypes of differentiated thyroid cancer (DTC) are fluorodeoxyglucose (FDG)-avid tumors and are at high risk for persistent/recurrent disease. In these patients, fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) is performed in cases of suspicion of recurrence based on thyroglobulin (Tg) levels or thyroglobulin antibodies (TgAb). The goals of this study were to evaluate the sensitivity of systematic postoperative FDG-PET/CT and to identify risk factors for abnormal FDG-PET/CT.
Methods:
Single-center retrospective study of 38 consecutive patients (16 males, 22 females; mean age, 57 years) with aggressive histology DTC, without known persistent disease at the time of postoperative radioactive iodine (RAI) ablation. The most frequent aggressive histologic subtypes were tall cell papillary carcinoma (45%) and poorly differentiated carcinoma (42%).
Results:
A total of 86 lesions were found in 20 (53%) patients, distributed in 33 organs. FDG-PET/CT and the postablation whole-body scan (RAI WBS) showed persistent disease in 15 and 12 patients, respectively. FDG-PET/CT was more sensitive than WBS for the detection of individual lesions (69% vs. 59%). Both imaging techniques were complementary with 41% of the lesions detected only by FDG-PET/CT and 31% only by RAI WBS. The only risk factor of abnormal FDG-PET/CT was a stimulated Tg level (Tg/TSH) measured at ablation >10 ng/mL with persistent disease showing FDG uptake in 72% of the patients with a Tg/TSH >10 ng/mL and in 10% of the patients with Tg/TSH ≤10 ng/mL.
Conclusion:
Postoperative FDG-PET/CT should be performed routinely in patients with aggressive histology DTC.
Introduction
D
The serum Tg level above which FDG-PET/CT is recommended during follow-up has empirically been set at 10 ng/mL after thyrotropin (TSH) stimulation, a threshold to be adapted to the DTC pathology subtype (14). More recently, the measurement of the serum Tg at the time of remnant ablation has become more widely used, with the threshold of a thyrotropin-stimulated Tg (Tg/TSH) at 10 ng/mL reported to have the best sensitivity and specificity to predict persistent disease (15). This threshold needs to be adapted to the mode of TSH stimulation, stimulated Tg levels being lower after recombinant human thyrotropin (rhTSH) than after thyroid hormone withdrawal (THW) (16). In all cases, the higher the stimulated Tg level, the greater the risk of persistent disease (17 –19).
Based on the poor prognosis of most aggressive subtypes of DTC, we routinely perform FDG-PET/CT for initial staging after surgery. The aims of this single-center retrospective study performed on consecutive DTC patients with an aggressive histology were, first, to evaluate the sensitivity of postoperative routine FDG-PET/CT and second, to identify risk factors for abnormal FDG-PET/CT.
Patients and Methods
After approval from our Institutional Review Board, the files of consecutive patients with aggressive DTC who underwent FDG-PET/CT after initial surgery between January 2004 and January 2013 were reviewed. Inclusion criteria consisted of patients with an aggressive DTC histology confirmed by our pathologist (A.A.G.); absence of known local disease or distant metastasis at the time of postoperative RAI ablation; and FDG-PET/CT and RAI performed within 3 months of each other. FDG-PET/CT was performed on levothyroxine treatment in 16 (42%) patients and after TSH stimulation in 22 (58%) patients (THW, n=21; rhTSH, n=1) after a mean time of 3.8 months (range, 1.2–7.6 months) after surgery. The mean interval time between FDG-PET/CT and RAI whole-body scan (WBS) was 24 days (range, 64 days before to 85 days after WBS).
RAI ablation and RAI WBS
After surgery (mean interval, 3.5 months; range, 1.4–7.8 months) patients were given a standard activity of RAI (3700 MBq; 100 mCi) after either THW (33 cases; 87%) or rhTSH (0.9 mg intramusclular [IM] per day for 2 consecutive days; 5 cases; 13%). The Tg/TSH level was measured on the day of RAI administration if given after THW, or 3 days after RAI administration if given after rhTSH.
Postablation WBS was performed 3 to 4 days after RAI administration. Before 2012, RAI WBS planar images were acquired using a dual-head camera (DHD-SMV, Sopha Medical, Buc, France) equipped with high-energy collimators and thick crystals at a scanning speed of 8 cm/min followed by a static neck scan. After 2012, the WBS was performed using a double-head camera equipped with 1.59 cm (5/8-inch) sodium iodide crystals and a multidetector (2 rows) spiral CT (Discovery NM/CT 670, General Electric Medical Systems, Waukesha, WI) after which single-photon emission computed tomography (SPECT)-CT was performed. The SPECT volume session included the neck and thorax with an axial field of view of 53.3×38.7 cm. For SPECT acquisition of tomographic images, a 128×128 matrix was used, and sixty-four 30-second projections were acquired over 360 degrees. SPECT data were reconstructed using a three-dimensional iterative algorithm (ordered-subsets expectation maximization with 4 iterations and 8 subsets). Images were smoothed with a three-dimensional spatial Gaussian filter. Immediately after SPECT acquisition, a CT tomogram was acquired followed by a spiral CT acquisition performed on a volume session similar to that of SPECT acquisition. CT acquisition parameters were as follows: tube current, 60 mA; collimation, 2–2.5 mm; pitch, 2. For CT data reconstruction, a 3-mm slice thickness with 2-mm slice increment and a B70 kernel filter were used. No contrast medium was injected during the procedure.
FDG-PET/CT
Before July 2011, FDG-PET/CT were performed using a Biograph LSO PET/CT (Siemens Medical System, Malvern, PA) with an activity of 4–6 MBq/kg of FDG and after July 2011 using a Discovery 690 (General Electric Medical Systems) with an activity of 3–4 MBq/Kg of FDG. Patients fasted for at least 6 hours and had glycemia <10 mmol/L. Image acquisitions were obtained 60 minutes after FDG injection with a three-dimensional mode. PET data on the Siemens Biograph were reconstructed on a 2562 matrix, using an iterative algorithm (FORE and AWOSEM) with 2 iterations, 8 subsets, and a 5-mm FWHM Gaussian postfilter and images were analyzed on an e.soft workstation (Siemens). PET data on the Discovery 690 were reconstructed on a 2562 matrix, using an iterative algorithm (FORE and AWOSEM) with 2 iterations, 24 subsets, a PSF-based reconstruction and a two-dimensional Gaussian postfilter with a 6.4-mm FWHM, and images were analyzed on an Advantage workstation (General Electric).
Image analysis
An initial independent visual analysis of both imaging tests was performed by two expert nuclear medicine physicians (D.D. and S.L.). For RAI WBS, any nonphysiologic iodine uptake was considered as abnormal. For FDG-PET/CT, lesions were classified as probably benign, suspicious, and malignant, the last two being considered as abnormal findings; they consisted in either those lesions with FDG uptake or lesions without FDG uptake that were seen on the CT scan. Lesions were considered as true positive based on cytology, histology, or follow-up. Otherwise they were considered as false positive.
In a second analysis performed by an expert nuclear medicine physician (C.N.), the RAI WBS and FDG-PET/CT images were correlated, the abnormal uptakes of RAI and FDG were compared and the patients were classified as: RAI−/FDG−; RAI+/FDG+; RAI+/FDG−; and RAI−/FDG+.
In RAI+/FDG+ patients, FDG-PET/CT and RAI WBS were considered concordant when all lesions showed both RAI and FDG uptake. They were considered complementary if at least one lesion was detected by only one of the two imaging tests.
Tg and TSH level measurements
Before 2006, serum Tg was measured using an immunoradiometric assay (SELco® Tg, Medipan Diagnostica, Selchow, Germany). The analytical sensitivity was 0.3 ng/mL and the Tg level was considered as not measured accurately when the routine recovery test (performed in all serum samples) was less than 80%. Since 2006, Tg is measured using a chemiluminescent immunoenzymatic “sandwich” assay (Access® Thyroglobulin, automated on UniCel® DxI 800 instruments, Beckman Coulter, Villepinte, France) with an analytical sensitivity of 0.1 ng/mL. The Tg level was considered as not measured measured in the presence of Tg antibodies using the Access® Thyroglobulin Antibody II assay (Beckman Coulter).
Serum TSH was measured using the Access hypersensitive human thyroid-stimulating hormone (hTSH) assay, a third-generation two-site immunoenzymatic (“sandwich”) assay automated on Access II Immunoassay System instrument (Beckman Coulter, Fullerton, CA), with a reference range of 0.34–5.60 mIU/L.
Statistical Analysis
Quantitative data are expressed as mean and standard deviation and qualitative data are expressed in percentage.
Risk factors for abnormal FDG-PET/CT were analyzed by univariate logistic regression and included the following characteristics: sex, age (≤45 vs. >45 years), tumor size (≤20 mm, 20–40 mm, >40 mm), bilaterality of the tumor, extension beyond the thyroid capsule (pT3–T4), neck dissection at initial surgery, presence of metastatic lymph node (N1 vs. N0-Nx), and Tg/TSH level (Tg/TSH ≤/> 10 ng/mL).
All reported p values are two-sided and the significance level was 0.05. Analyses were performed using SAS statistical software (version 9.1, SAS Institute Inc., Cary, NC).
Results
Patients
Thirty-eight patients (16 males, 22 females; mean age, 57 year; range, 18–84 years) form the basis of this study. Their clinical characteristics are reported in Table 1.
All patients underwent total thyroidectomy and 22 (58%) underwent neck lymph node dissection. Tumors were papillary in 20 (53%) cases, well-differentiated follicular carcinoma in 2 (5%) cases, and poorly differentiated in 16 (42%) cases (Table 1).
According to the 2010 pTNM scoring system for DTC (8), tumors were pT1 in 2 cases (5%), pT2 in 6 cases (16%), pT3 in 25 cases (66%), and pT4 in 5 cases (13%). Lymph node status was pN1 in 20 (53%) cases, pN0 in 2 (5%) cases and unknown (pNx) in 16 (42%) cases (Table 1). Mean size of the primary thyroid tumor was 41 mm (range, 10–100 mm). Among patients with lymph node metastases, the mean number of lymph node metastases (N1) was 10 (range, 1–42) and the mean number of N1 with extracapsular extension was 2 (range, 0–12).
The mean postoperative Tg/TSH level was 213 ng/mL (range, 0–2825; median, 5 ng/mL). The Tg/TSH level was >10 ng/mL in 18 patients (mean, 44.8 ng/mL; range, 12.3–2825) and ≤10 ng/mL in 20 patients (mean, 1.4 ng/mL; range, 0–6.4). TgAb were detectable and above the upper limit range in 5 cases.
Imaging results
Per patient analysis
Persistent disease was detected on FDG-PET/CT and/or RAI WBS in 20 (53%) patients (Table 2). Initial pathology was tall cell papillary carcinoma in 10 cases, diffuse sclerosing and trabecular papillary carcinoma in 2 cases, poorly differentiated carcinoma in 7 cases, and oncocytic follicular thyroid cancer in 1 case. Tumors were pT1 in 2 cases (10%), pT2 in 3 cases (15%), pT3 in 11 cases (55%), and pT4 in 4 cases (20%). Lymph node status was pN1 in 9 (45%) cases, pN0 in 2 (10%) cases, and pNx in 9 (45%) cases. The patients with detectable persistent disease at ablation had detectable Tg/TSH (mean, 422.5 ng/mL; range, 1.4–2825; median, 75 ng/mL) in all cases except 1 who had elevated TgAb at 1688 IU/mL. The 18 patients without FDG-PET/CT and/or RAI WBS persistent disease at ablation had a mean Tg/TSH level of 3.5 ng/mL (range, 0–32; median, 1 ng/mL).
WBS, whole body scan; FDG-PET/CT, fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography; NA, not attributed.
FDG-PET/CT was abnormal in 17 patients among whom 2 were considered as false positive because FDG uptake was located in the thyroid bed, there was no abnormality on cross-sectional imaging or on RAI WBS, and no recurrence occurred during follow-up (5 and 60 months length). In both false-positive cases, the ablation Tg/TSH levels were <1 ng/mL in the absence of TgAb. Initial pathology of these 2 patients was pT3N1 papillary TC (diffuse sclerosing variant and tall cell variant in 1 case each).
RAI WBS was abnormal in 12 patients. No false-positive result was observed. The median iodine uptake in the thyroid bed on RAI WBS, available in 32 cases, was 0.32% (mean, 1.2%; range, <0.1 to 14%).
Among the 20 patients with persistent disease, disease was detected only by FDG-PET/CT in 8 (40%) cases, only by RAI WBS in 5 (25%) cases, and by both imaging techniques in 7 (35%) cases (Fig. 1 and Table 2). Among these 7 cases, FDG-PET/CT and RAI WBS were complementary (i.e., at least one lesion was detected by only one of the imaging methods) in 6 cases. FDG-PET/CT was the only abnormal imaging technique (8/20) or showed lesions not seen on RAI WBS (6/20) in 14 cases (70%). The sensitivity of FDG-PET/CT for the detection of persistent disease was 75% (confidence interval [CI] 56%–94%) and the sensitivity of RAI WBS was 60% (CI 39%–82%; p=0.50).
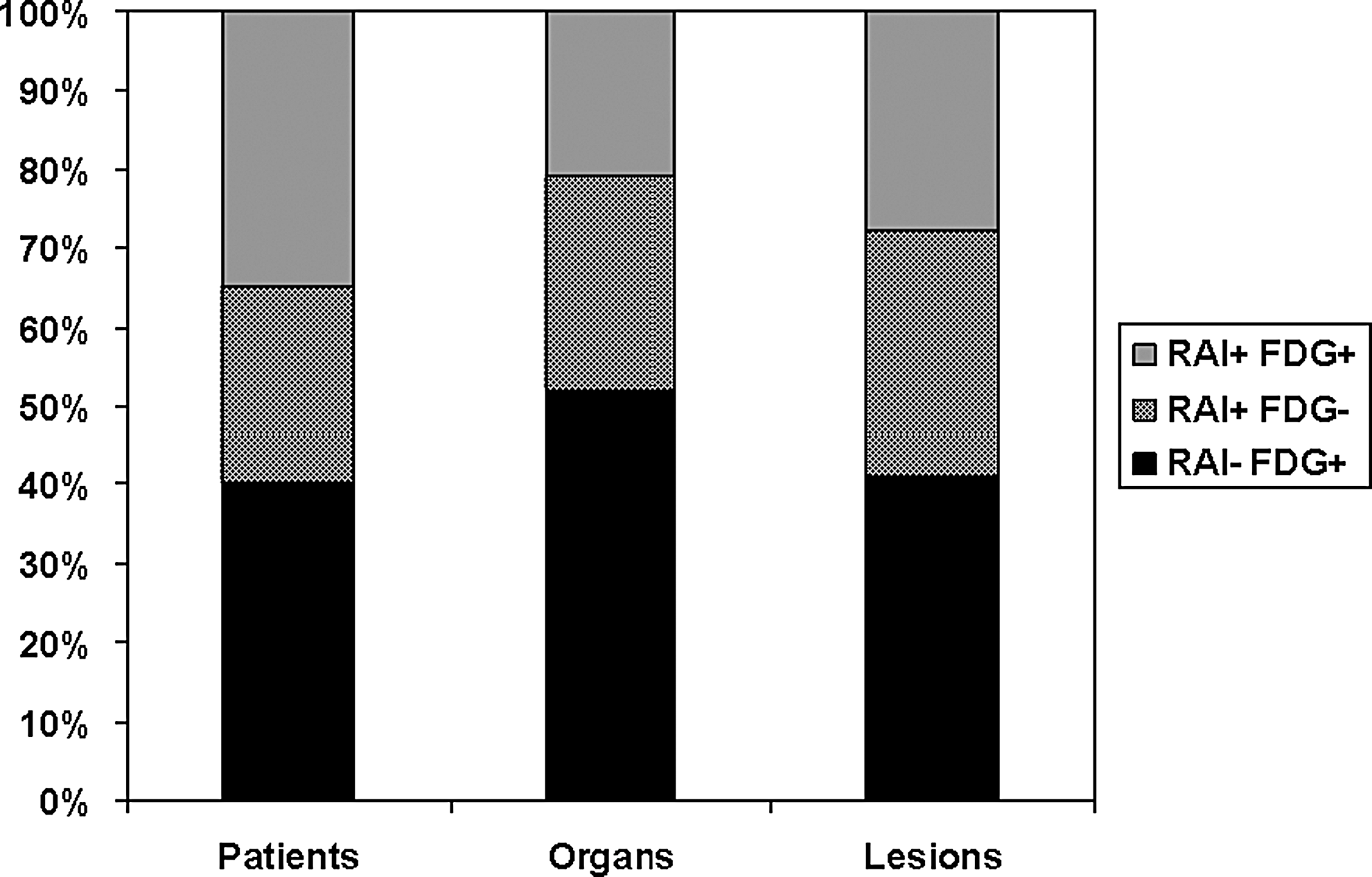
WBS and FDG-PET/CT for disease detection by patient, organ, and lesion. WBS, whole-body scan; RAI: radioactive iodine; FDG: fluorine-18-fluorodeoxyglucose; FDG-PET/CT, fluorodeoxyglucose positron emission tomography/computed tomography.
Follow-up of patients with normal imaging
Among the 18 patients without evidence of disease at the time of investigation (16 patients with both normal imaging methods and 2 patients with false-positive FDG uptake), after a mean follow-up of 19 months (range, 2.5–71 months; median, 8 months), 1 patient relapsed. This patient had a pT4b Nx M0 poorly differentiated thyroid cancer and recurrence was detected 33 months after surgery, by an increase of the nonstimulated Tg level. FDG uptake, but not RAI imaging, revealed the recurrence.
Per organ analysis location of persistent/recurrent disease
Eighty-six lesions were detected in 33 organs defined as neck, mediastinum, lung, and bone. Six patients (30%) had neck disease only and 14 (70%) had distant metastases (lung, n=8; mediastinal lymph nodes, n=6; bone, n=3).
FDG-PET/CT detected lesions in 24 organs and RAI WBS in 16 organs (Table 2). Organs with metastases were diagnosed only by FDG-PET/CT in 17 (52%) cases, only by RAI WBS in 9 (27%) cases, and by both imaging techniques in 7 (21%) cases (Fig. 1). The sensitivity of FDG-PET/CT for the diagnosis of organs with metastases was 73% (CI 56%–85%) and the sensitivity of RAI WBS was 48% (CI 32%–65%; p=0.23).
Per lesion analysis
The 86 detected lesions were located in the neck (n=26), lungs (n=46), mediastinum (n=7), and in bones (n=7). FDG-PET/CT detected 59 of these lesions and RAI WBS detected 51. Lesions were detected only by FDG-PET/CT in 35 cases (41%), only by RAI WBS in 27 cases (31%), and by both FDG and RAI WBS in 24 cases (28%; Fig.1). The sensitivity of FDG-PET/CT for the diagnosis of lesions was 69% (CI 59%–78%) and the sensitivity of RAI WBS was 59% (CI 49%–70%; p=0.009). Of note, 6 of the 7 bone lesions were detected only by RAI WBS.
Risk factors for abnormal FDG-PET/CT
Potential risk factors for abnormal FDG-PET/CT analyzed are shown in Table 3. The only significant risk factor was a Tg/TSH level >10 ng/mL.
FDG-PET/CT, fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography; LN, lymph nodes; OR, odds ratio; CI, confidence interval; Tg, thyroglobulin; TSH, thyrotropin.
Among the 20 patients with Tg/TSH level ≤10 ng/mL, 5 had elevated TgAb. Persistent disease was detected in 4 of 20 cases (20%), among whom 1 had elevated TgAb. In these patients persistent disease was identified only by RAI WBS in 2 cases and only by FDG-PET/CT in 2 cases (Table 4).
Two RAI−/FDG+ patients with false-positive FDG uptake excluded.
RAI, radioactive iodine; FDG, fluorine-18-fluorodeoxyglucose; Tg, thyroglubulin.
Among the 18 patients with a Tg/TSH level >10 ng/mL, none had positive TgAb. Persistent disease was detected in 16 of 18 cases (89%), identified only by RAI WBS in 3 (17%) cases, only by FDG-PET/CT in 6 (33%) cases, and by both RAI WBS and FDG-PET/CT in 7 (38%) cases (Fig. 2). FDG-PET/CT was abnormal in 10% of patients with Tg/TSH levels ≤10 ng/mL and in 72% of patients with Tg/TSH levels >10 ng/mL (p<0.001). The frequency of truly abnormal FDG-PET/CT with normal RAI WBS or showing at least one lesion not detected by RAI WBS was 10% (n=2) when serum Tg/TSH was ≤10 ng/mL (with or without TgAb) and 67% (n=12) when serum Tg/TSH was >10 ng/mL. Of note, among the 2 patients with a Tg/TSH level >10 ng/mL and normal imaging, the follow-up, available in 1 case, showed complete remission with a subsequent stimulated Tg of 0.1 ng/mL and a normal RAI WBS.

This 63-year-old woman underwent total thyroidectomy and bilateral central and lateral neck dissection for a pT3 N1b tall cell variant of papillary thyroid carcinoma. The postoperative stimulated serum Tg was 18.3 ng/mL. (
Among the 17 (45%) patients with tall cell papillary carcinoma and the 16 (45%) patients with poorly differentiated carcinoma, persistent disease was detected in 10 patients with TCC (59%) and in 7 (43%) with poorly differentiated carcinoma. The detection rates of FDG-PET and RAI WBS are shown in Table 5. No statistical test was performed considering the small sample sizes.
WBS, whole body scan; FDG-PET, fluorine-18-fluorodeoxyglucose positron emission tomography.
Discussion
Aggressive histologic variants with poorly differentiated carcinomas represent only a minority of DTC (1). According to the American Thyroid Association classification, they have an intermediate to high risk of persistent/recurrent disease, depending on the pTNM system and the completeness of surgical resection. According to the European Thyroid Association classification, they are at high risk of persistent disease (8,20). To our knowledge, our study is the first focusing on the use of postoperative FDG-PET/CT in patients with DTC with aggressive histology (21 –23). Persistent disease was found in more than half of the patients (53%), most of them with distant metastases. FDG uptake was found in 75%, and RAI uptake in 60%. FDG-PET/CT was the only imaging technique demonstrating abnormal findings or lesions not seen on RAI WBS in 70% of these patients. Our numbers are higher than previously reported, where persistent disease detected on preablation FDG-PET/CT was found in 13% to 33% of patients with intermediate risk of persistent disease (21 –23). These higher figures can be explained by the selection of patients with aggressive histology. However, we cannot eliminate a bias due to the type of referrals to our institution as a tertiary medical care center concentrating on patients with more advanced tumors.
The question whether FDG-PET/CT should be performed postoperatively in all patients with intermediate risk of persistent disease or according to serum Tg level measured at ablation is a matter of debate. We found that 40% of the patients with persistent disease after surgery had disease detected only by FDG-PET/CT. Among all patients, the only predictive factor of abnormal FDG-PET/CT was a stimulated Tg level, with abnormal FDG-PET/CT in 10% of patients with Tg/TSH levels ≤10 ng/mL and in 72% of patients with Tg/TSH levels >10 ng/mL (p<0.001). The relations between Tg/TSH and the risk of abnormal FDG-PET/CT was also reported in a previous study (21), and was suggested in two others (22,23). The absence of large thyroid remnants after total thyroidectomy, with RAI uptake in the thyroid bed <1% of the administered activity in most cases, allows a better evaluation of the origin of elevated Tg levels: in these patients, an elevated serum Tg level is highly suspicious of persistent disease, in which RAI uptake may be absent because of the aggressive histology (9,24); furthermore, poorly differentiated thyroid cancer may not produce high levels of Tg in the serum.
The recommendation of performing FDG-PET/CT for aggressive DTC can be based on the Tg/TSH level, the only risk factor predicting an abnormal FDG-PET/CT. It may be suggested in patients with a Tg/TSH <10 ng/mL, but it is really useful in those with a Tg/TSH >10 ng/mL. In these cases, FDG-PET/CT frequently allows the identification of residual disease not detected on the RAI WBS, which may be amenable to other treatment options, including local treatment, such as cryoablation or radiofrenquency ablation, or targeted therapy in case of RECIST progression as first-line treatment (8,25). Also, when the disease is considered as refractory to RAI, usually no additional RAI treatment is performed (25). The small sample size in this study did not allow determining whether the benefit of FDG-PET/CT is increased in a particular histotype.
The advantages of performing FDG-PET/CT systematically, even when the Tg/TSH is <10 ng/mL, consist in the benefit of the TSH stimulation associated with the RAI treatment (26) and the complementarity between FDG-PET/CT and WBS, with 41% of the lesions only detected with FDG-PET/CT and 31% only detected with RAI WBS. On the contrary, the disadvantage of performing FDG-PET/CT postoperatively is the risk of a false-positive FDG-PET/CT because of postoperative inflammation (27). We indeed found two patients with false-positive FDG uptake in the thyroid bed but both had low Tg/TSH levels. Physicians should be aware of this risk and interpret FDG-PET/CT with caution in patients with Tg/TSH <10 ng/mL.
The study is limited by its retrospective design and the low number of included patients, which is because of the rarity of the disease. Also, we were not able to biopsy all lesions detected on FDG-PET/CT or RAI WBS because this was not medically or ethically possible. Furthermore, as the SPECT-CT camera was not available in our center until 2012, we did not perform RAI WBS with neck SPECT-CT in all patients, which was shown to increase the number of detected lesions and to decrease the number of doubtful lesions (28). We performed FDG-PET/CT under TSH stimulation in only 58%, which might have decreased the sensitivity of FDG-PET/CT (26). Finally, the interval time between RAI WBS and FDG-PET/CT might have introduced bias. We allowed in our inclusion criteria a maximum of a 3-month interval because we are dealing with DTCs, which are usually slow-growing tumors. The mean interval time was, however, much shorter: only 24 days, possibly introducing a minor bias.
In conclusion, early postoperative FDG-PET/CT performed concomitantly with RAI WBS in patients with aggressive DTC histology showed persistent disease in a high number of patients and should be performed routinely.
Footnotes
Acknowledgment
C. Nascimento received a grant from DUERTECC/EURONCO (Diplôme Universitaire Européen de Recherche Translationnelle Et Clinique en Cancérologie).
Author Disclosure Statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.