
Abstract
Background:
Previous studies detecting mutations in thyroid nodule fine-needle aspiration (FNA) material differed with respect to the cytologic grading applied to the FNAs, the type of FNA material used, and the prevalence of mutations observed in the samples. Therefore, the aim of the present study was to investigate these differences as possible reasons for the discrepant sensitivities and specificities reported for the “ruling-in” approach between the previous studies.
Methods:
RNA and DNA was extracted from 347 routine air-dried FNA smears with available histology. PAX8/PPARG and RET/PTC rearrangements were detected by real-time quantitative polymerase chain reaction, while BRAF and RAS mutations were detected by pyrosequencing.
Results:
BRAF mutations were associated with a carcinoma in 100% of samples; RAS mutations were associated with a carcinoma in 57% of samples. Forty-nine percent of the carcinomas were identified by molecular testing in the group of follicular lesions, which increased the sensitivity from 60% to 80% compared to cytologic FNA evaluation alone. While follicular lesion FNAs had a 28% risk of malignancy, the risk increased to 71% for mutation-positive follicular lesions, and decreased to 18% for mutation-negative follicular lesions.
Conclusion:
Molecular testing of air-dried FNA samples improves presurgical diagnosis. Discrepant sensitivities and specificities reported previously are most likely related to the use of different grading schemes resulting in different compositions of the cytologic categories, interobserver variability to diagnose follicular variant of papillary thyroid carcinomas and a different prevalence of RAS mutations in follicular carcinomas. The knowledge of the molecular testing might support the histologic identification of minimally invasive follicular carcinomas.
Introduction
T
Although molecular diagnostics by the detection of somatic mutations in FNA material (“ruling-in” approach) has led to substantial diagnostic improvements (8,9) major differences with respect to sensitivity and specificity of the ruling-in approach have been reported between the studies of Nikiforov et al. (10,11), Ohori et al. (12), and Cantara et al. (13) and our recent study (14). On the other hand, it is difficult to compare these studies because the cytologic grading in these studies is based on different guidelines (Nikiforov et al. [10]: six-category Bethesda scheme [15] versus four-category American Thyroid Association scheme from 2006 [16] in our study [14]), the studies used different types of FNA material (fresh FNA material [10] versus routine air-dried FNA smears [14]), the prevalence of RAS mutations in FTCs varied between the studies (36% [10] versus 25% [14]), and in Nikiforov et al. (10) the histopathologic diagnosis was established by a pathologist who was not blinded to the results of molecular testing. Therefore, the aim of the present study was to investigate possible reasons for the previous discrepancies for sensitivity and specificity of the ruling-in approach between previous studies, including our recently developed method analyzing routine air-dried FNA smears (14,17,18) in a setting that is closer to the study of Nikiforov et al. (10) thus allowing a better comparison of the different methodologies. For that reason we now analyzed point mutations and rearrangements in a set of 347 routine air-dried FNAs, which were cytologically rated according to the Italian Society for Anatomic Pathology and Cytopathology (SIAPEC)-International Academy of Pathology five-tier reporting system (19,20) superimposable on the British Thyroid Association (BTA) guidelines from 2007 (1) instead of the older four-category scheme used previously. Most importantly, because there is a substantial interobserver and intraobserver variability in the cytopathologic and also the histopathologic evaluation of thyroid nodules (21), the histopathologic diagnosis of mutation-positive and mutation-negative samples was re-evaluated before the impact of molecular FNA testing was assessed. Moreover, the resected tumors were also investigated for the mutations screened in the respective FNA samples to better account for the difficulties to establish a reference or gold standard for these studies.
Materials and Methods
Patients and samples
Air-dried FNA slides from 347 consecutive patients who underwent surgery for thyroid nodules larger than 1 cm after prior FNA at the Arcispedale Santa Maria Nuova Hospital from 2006 to 2013 were retrospectively evaluated in this study. The FNAs were selected for the availability of formalin-fixed paraffin embedded (FFPE) samples to be able to verify the results obtained in the FNA samples and to detect false-negative cases and thus true sensitivity/specificity. All FNAs were graded by an experienced pathologist (S.P.) according to the SIAPEC-International Academy of Pathology five-tier reporting system (19,20), which is superimposable on the 2007 BTA guidelines (1). Cytologic samples included 8 nondiagnostic (Thy1), 106 nonneoplastic (Thy2), 163 follicular lesion/suspected follicular neoplasm (Thy3), 39 suspicious of malignancy (Thy4), and 31 malignant (Thy5) samples. Histologic evaluation of the corresponding FFPEs revealed 137 hyperplastic nodules (HNs), 71 FAs, 24 Hürthle cell adenomas (HCAs), 21 FTCs, 5 Hürthle cell carcinomas (HCCs), 63 classic papillary thyroid carcinomas (cPTCs), 22 follicular variant papillary thyroic carcinomas (fvPTCs), 2 tall cell papillary thyroid carcinomas (tcPTCs), 1 differentiated thyroid carcinoma (DTC), and 1 poorly differentiated thyroid carcinoma (PDC). All cases were classified according to the criteria recommended by the World Health Organization (WHO) (22). The study was approved by the ethics committee of the University of Leipzig.
DNA and RNA extraction from FNA smears and FFPE slides
DNA and RNA was extracted from routine air-dried, May-Grünwald-Giemsa (MGG)–stained FNA smears and from the FFPE slides as described recently (17,18).
cDNA synthesis
cDNA was synthesized using the miScript Reverse Transcription Kit (Qiagen, Hilden, Germany) according to the manufacturer's protocol. In brief, 7.5 μL template RNA was added to a master mix consisting of 2 μL 5× miScript RT buffer and 0.5 μL miScript Reverse Transcriptase Mix and incubated for 60 minutes at 37°C. Subsequently, the miScript Reverse Transcriptase Mix was inactivated for 5 minutes at 95°C.
Detection of rearrangements by quantitative polymerase chain reaction
PAX8/PPARG, RET/PTC1, and RET/PTC3 rearrangements were detected in multiplex-qPCRs on a Rotor Gene Q 5Plex (Qiagen) using the QuantiTect SYBR Green PCR kit (Qiagen), one primer pair amplifying an intron spanning 125 bp control fragment of PAX8 mRNA (exon 5–6) (for cDNA quality control), and one rearrangement-specific primer pair as described previously (14). Following the polymerase chain reaction (PCR), a fluorescence melting curve analysis was performed to detect and discriminate the control fragment and the rearrangement specific amplicons by their specific melting points (14).
Detection of point mutations by high-resolution melting peak analysis
BRAF (codons 600/601), KRAS (codons 12/13), HRAS (codon 61), and NRAS (codon 61) point mutations were detected by real-time PCR and high-resolution melting (HRM), using primers flanking the mutation hot spots (14) and the Type-it HRM PCR chemistry (Qiagen) on a Rotor Gene Q 5Plex (Qiagen). Subsequent to the PCR, an HRM curve was analyzed from 75°C to 95°C with an increase of 0.1°C per step and a wait of 2 seconds after each step.
DNA from patient specimens known to carry BRAF, KRAS, and NRAS point mutations were used as positive controls in each analysis. Samples tested positive were subsequently analyzed by pyrosequencing on a PyroMark Q24 (Qiagen) to identify the precise base exchanges and the allelic percentages of the mutations.
Detection of point mutations by pyrosequencing
Point mutations in BRAF, KRAS, and NRAS by pyrosequencing using the therascreen BRAF Pyro Kit, therascreen NRAS Pyro Kit, and PyroMark KRAS Kit (all from Qiagen) according to the manufacturer's instructions. In brief, 5μL of genomic DNA was amplified using template-specific PCR primers (including one biotin-labeled primer) and template-specific PCR conditions. Afterwards, the PCR products were immobilized on streptavidin sepharose beads and single-stranded DNA was prepared allowing subsequent annealing of the sequencing primer to the template DNA. Then, the primed single-stranded DNA was released from the streptavidin surface and transferred to a PyroMark Q24 (Qiagen) for pyrosequencing. HRAS point mutations were detected by pyrosequencing using self-designed primers as described previously (14).
Determination of cutoff values for the pyrosequencing of FNAs
The percentage of mutant BRAF and NRAS alleles determined by pyrosequencing was compared in the corresponding FNA samples of verified mutation-positive FFPEs and mutation-negative FFPEs to determine the optimal cutoff percentage for the FNA samples. The receiver operating characteristic (ROC) analysis revealed an optimal cutoff allele percentage of 11% for the detection of BRAF mutations (Fig. 1A) and of 8% for the detection of NRAS mutations (Fig. 1B). Specific cutoff percentages for HRAS and KRAS mutations could not be calculated because of the small number of detected HRAS and KRAS mutations (7 and 1, respectively). Therefore, a common cutoff percentage of 10% was applied for all FNA mutation screenings: FNAs with a mutant allele percentage less than 10% were deemed mutation-negative, whereas FNAs with a mutant allele percentage 10% or more were deemed mutation-positive.
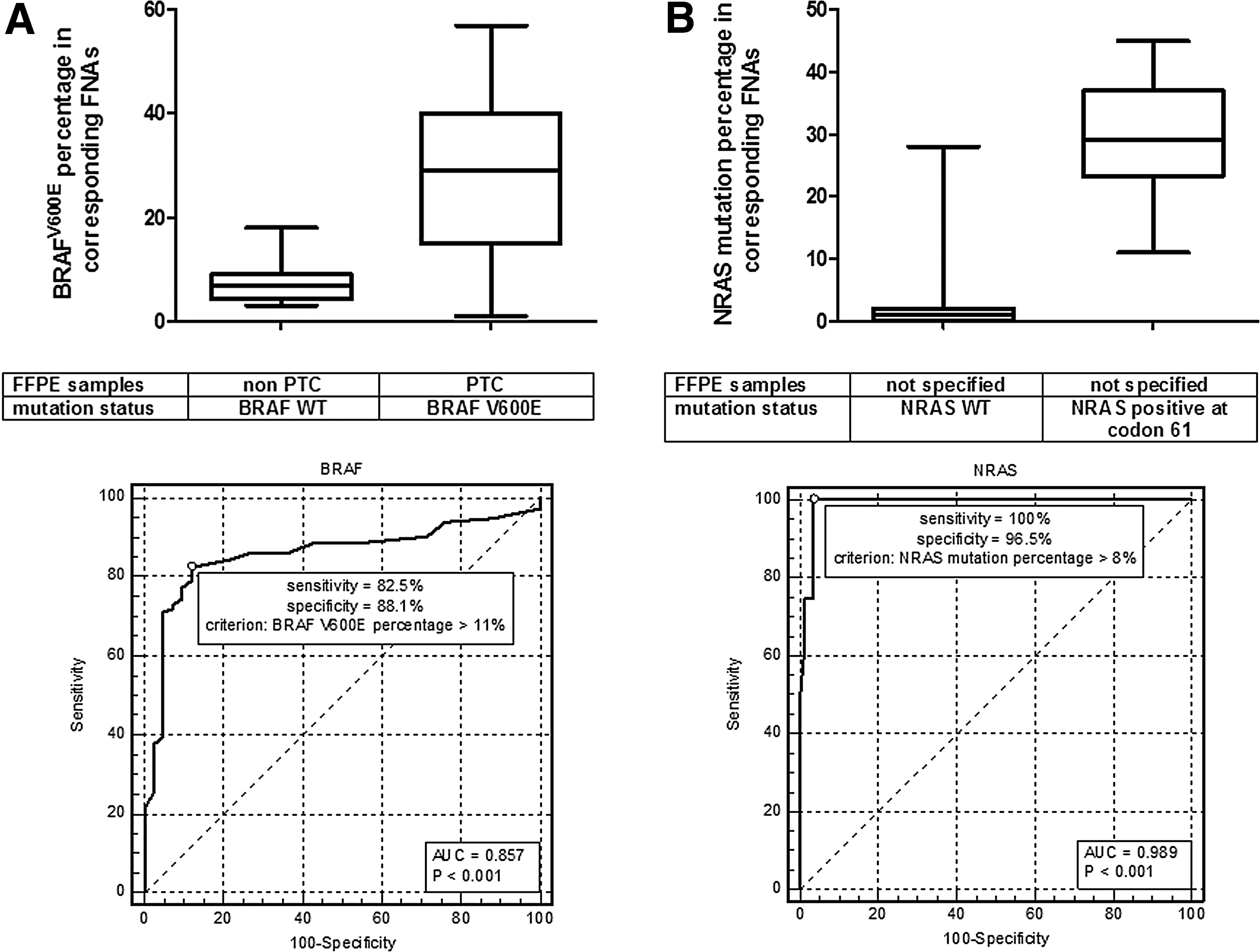
Comparison of the mutation percentage in the fine-needle aspiration (FNA) samples in relation to the mutation status in the corresponding formalin-fixed paraffin embedded (FFPE) samples. (
Histologic re-review of FAs subsequent to molecular testing
Subsequent to the molecular testing of the FNA and FFPE samples the original hematoxylin-eosin stained histology slides of all 98 samples initially diagnosed as FA/HCA were re-reviewed according to the WHO criteria (22) by a pathologist (S.P.) who was aware of the molecular testing results. Statistical analysis was based on these revised histologic diagnoses.
Statistics
Sensitivities, specificities, positive predictive values (PPV), and negative predictive values (NPV) were calculated as follows: sensitivity=true positives/(true positives+false negatives) specificity=true negatives/(true negatives+false positives) PPV=true positives/(true positives+false positives) NPV=true negatives/(true negatives+false negatives).
In the comparisons of cytology versus histology, molecular fine-needle aspiration analysis (mFNA) versus histology, and of cytology and mFNA versus histology, histology is the gold standard. In the comparison of cytology versus histology a cytologic Thy4 and Thy5 test outcome corresponding to a malignant histology is considered as true positive and a cytologic Thy2 test outcome corresponding to a benign histology is considered as true negative. In the comparison of mFNA versus histology and in the comparison of cytology and mFNA versus histology a mutation-negative FA is considered as true negative, while a mutation-positive FA is considered false positive. To investigate the concordance of the mutation analysis for FNA and the corresponding FFPE samples, mFNA was compared to molecular FFPE analysis (mFFPE). Therefore, in this comparison, mFFPE is the gold standard and the decision only depends on whether a mutation present in the FFPE sample was detected in the corresponding FNA sample or not.
The comparison of mutation percentages between FNAs and FFPEs was performed by ROC curves using MedCalc Statistical Software, version 9.6 (Mariakerke, Belgium).
Results
Inadequate PCR product
In the FNAs the average percentage of samples with inadequate PCR products was 2% and 6% per point mutation screening and per rearrangement screening, respectively. Forty-one FNAs characterized by at least one inadequate PCR and that were mutation-negative in all the other screenings, were classified “not evaluable” (NE; Table 1). The percentage of NE-FNAs was highest in the Thy1-FNAs (87.5% NEs), followed by 25% NE-FNAs in the Thy2-FNAs. Significantly lower percentages of NE-FNAs were observed in the Thy3-, Thy4-, and Thy5-FNAs (3.1%, 2.6%, and 3.2%, respectively). FNAs classified as NE were not considered in the calculation of sensitivity and specificity.
Five BRAF mutations were detected in Thy3-fvPTCs: 3 V600E mutations and 2 K601E mutations.
cPTC, classic papillary thyroid carcinoma; DTC, differentiated thyroid carcinoma; FA, follicular adenoma; FTC, follicular thyroid carcinoma; fvPTC, follicular variant of papillary thyroid carcinoma; HCA, Hürthle cell adenoma; HCC, Hürthle cell carcinoma; NE, not evaluable due to failed polymerase chain reaction (PCR); HN, hyperplastic nodule; PDC, poorly differentiated thyroid carcinoma; tcPTC, tall cell papillary thyroid carcinoma.
Detected mutations
Eighty FNAs, which were mutation-positive in at least one analysis (57 BRAF, 15 NRAS, 7 HRAS, and 1 KRAS mutations) were classified mutation-positive. No PAX8/PPARG and no RET/PTC rearrangement could be detected in any FNA sample (Table 1). Only the 226 FNAs, which were mutation negative in all screenings were classified as wild-type (WT).
Eighty-two mutations were detected in the corresponding FFPEs: 56 BRAF, 17 NRAS, 8 HRAS, and 1 KRAS mutation. In 95% the mutation found in the FNA could be confirmed in the FFPE, while 92.6% of the mutations found in the FFPE were detected in the FNA. The correlation between cytology, histology, and mFNA is shown in Table 1. While the presence of a BRAF mutation was associated with carcinoma in 100% of samples, the presence of a RAS mutation was associated with carcinoma in 57% of samples (Table1).
Cytology versus histology
Cytologic evaluation of the FNAs revealed 8 Thy1, 109 Thy2, 163 Thy3, 39 Thy4, and 31 Thy5 results. All 31 cytologically Thy5 samples were carcinomas on histologic analysis (29 cPTCs, 1 fvPTC, and 1 PDC). The final histologic classification of the 39 Thy4-FNAs revealed 27 cPTCs, 2 tcPTCs, 9 fvPTCs, and 1 FA. The final histologic classification of the 163 Thy3-FNAs revealed 7 cPTCs, 11 fvPTCs, 21 FTCs, 5 HCCs, 1 differentiated carcinoma with histologic features of both FTC and PTC, 58 FAs, 23 HCAs, and 37 HNs, while the final histologic classification of the 109 Thy2-FNAs revealed 12 FAs, 1 HCA, and 93 HNs (Table 1). As shown in Table 2, these data result in a sensitivity of 60%, a specificity of 100%, and a PPV and NPV of 99% and 83%, respectively.
Mutation-positive adenomas considered as false positives.
Mutation-positive adenomas considered as true positives.
The comparison of molecular fine-needle aspiration (mFNA) and molecular formalin-fixed paraffin embedded analysis (mFFPE) results gives a measure of the concordance of the mutation analysis between FNA and corresponding FFPE samples.
PPV, positive predictive value; NPV, negative predictive value.
mFNA versus histology
mFNA revealed 80 mutations in total. Fifty-seven BRAF mutations (55 BRAF V600E and 2 BRAF K601E ) were detected. Forty-seven cPTCs, 9 fvPTCs, and 2 tcPTCs harbored a BRAF V600E mutation, while in 2 fvPTC a BRAF K601E mutation was found. Furthermore, 15 NRAS mutations were detected in the FNAs representing 7 FTCs, 1 cPTC, 1 differentiated carcinoma with histologic features of both FTC and PTC, 3 FAs, and 3 HNs in the final histology. In addition, 7 HRAS mutations could be detected in the FNAs (3 FTCs, 1 HCC, and 3 FAs). Finally, 1 KRAS mutation was detected in an FNA representing a HCA in the histology. Two hundred twenty-six FNAs were mutation-negative, representing 1 PDC, 17 PTCs, 10 fvPTCs, 11 FTCs, 4 HCCs, 58 FAs, 22 HCAs, and 103 HNs at final histology. These data result in a sensitivity of 62%, a specificity of 95%, and a PPV and NPV of 88% and 81%, respectively (Table 2).
Cytology and mFNA versus histology
In addition to the 70 cytologically malignant (Thy5) and suspicious of malignancy (Thy4) samples, mFNA detected 31 mutations (10 BRAF [8 V600E, and 2 K601E], 13 NRAS, 7 HRAS, and 1 KRAS) in the 163 Thy3 samples representing 5 cPTCs, 5 fvPTCs, 10 FTCs, 1 HCC, 6 FAs, 1 HCA, and 2 HNs, 1 NRAS mutation in the Thy2 group representing 1 HN, and 1 BRAF mutation in the Thy1 group representing a fvPTC (Table 1). One hundred twenty-seven FNAs were mutation-negative in the Thy3 group representing 2 cPTCs, 6 fvPTCs, 11 FTCs, 4 HCCs, 49 FAs, 21 HCAs, and 34 HNs in the final histology. In the Thy2 group, 78 FNAs were mutation-negative representing 8 FAs, 1 HCA, and 69 HNs in the final histology. Based on these data the combination of cytologic evaluation and mFNA allowed the detection of 22 additional carcinomas in the Thy3 category, while 23 carcinomas could not be identified, revealing overall a sensitivity of 80%, a specificity of 95%, and a PPV and NPV of 89% and 91%, respectively, if mutation-positive FAs were considered as false positives (Table 2). In an additional analysis, we considered mutation-positive FAs as (pre-)malignant tumors and thus as true positives. Based on this assumption, the sensitivity is 82%, specificity is 100%, and the PPV and the NPV is 100% and 91%, respectively (Table 2).
mFNA versus mFFPE
The direct comparison of mFNA and mFFPE results is not of diagnostic relevance in this retrospective study, but gives a measure of the concordance and the true sensitivity/specificity of the mutation detection by comparing FNA and corresponding FFPE samples. Eighty mutations were detected in the FNAs. Seventy-six of these 80 mutations could be confirmed in the FFPEs. Two hundred twenty-six FNAs were mutation-negative. While the molecular screening of the corresponding FFPEs confirmed the mutation-negative result in 217 FFPEs, 5 FFPEs were mutation-positive (2 BRAF, 2 NRAS, and 1 HRAS mutation) and 4 FFPEs were NE. This corresponds to a sensitivity of mFNA of 94%, and a specificity of 100% (Table 2).
Histologic re-review of FAs subsequent to molecular testing
For 10 FAs, RAS mutations were detected in FNA and FFPE material. The histology of these samples was re-evaluated after the results of the molecular screening thus leading to the reclassification of three FAs into minimally invasive FTCs. In addition, all the remaining (mutation-negative) FAs were re-evaluated and the original histologic diagnosis was confirmed. Figure 2 shows a representative case of a deceptive minimally invasive FTC, which was initially underdiagnosed as an FA.
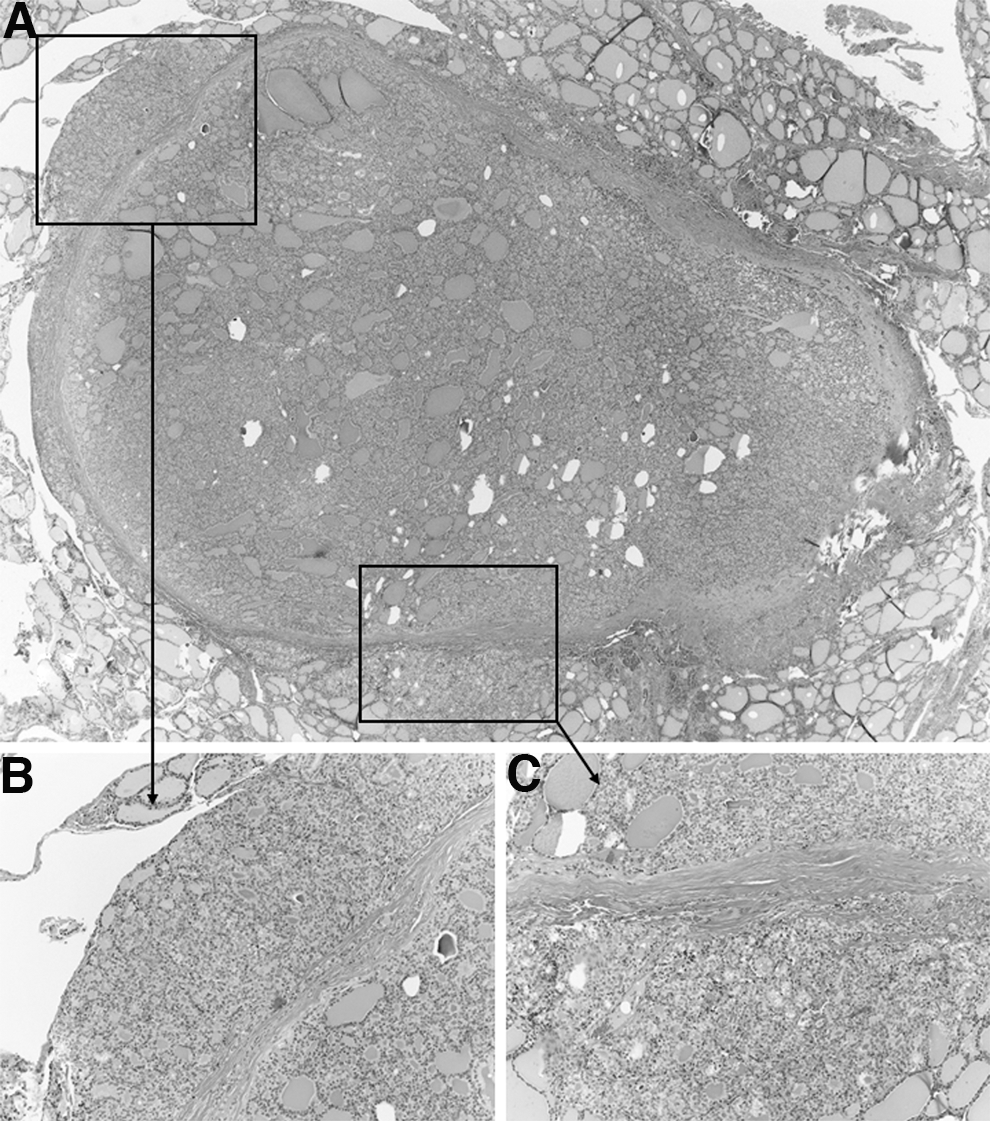
A representative case of a deceptive, minimally invasive follicular carcinoma originally reported as follicular adenoma. At low power view (
Discussion
The molecular screening of FNA material from the same routine air-dried FNA smear, which is used for cytologic analysis, offers major advantages (23). Therefore, we established a methodology to extract both DNA and RNA from these FNA smears for the analysis of point mutations and rearrangements (17,18,24). For a better comparison of this methodology with the so far most important study using fresh FNA material (10), this report analyzes the impact of the molecular panel screening in a set of 347 samples from a single institution, which were cytologically graded according to the SIAPEC-International Academy of Pathology five-tier reporting system (19,20), superimposable to the BTA guidelines from 2007 (1).
With a maximum percentage of 3% NE-FNAs in the diagnostically relevant categories (Thy3-Thy5), and with an accuracy of 98% (sensitivity of 94%, specificity of 100%) for the direct comparison of the molecular FNA screening and the molecular screening of the corresponding FFPE samples, we could clearly confirm the feasibility of molecular screening of routine air-dried FNA smears for point mutations and rearrangements. The significantly higher NE rate in the Thy2 category (25%) in comparison to the Thy3-Thy5 categories (3%) is most likely due to the fact that in a reliable clinical setting, a cystic lesion on ultrasound was considered benign if abundant colloid and macrophages were found on cytology, even if the follicular cells were very scanty. This advantage derives from a strict clinico-cytologic correlation that also explains the low rate of Thy3 FNAs. In fact, due to this approach it is possible to find selected cases containing less cells than Thy1, for which the clinical information of a cystic lesion allows to consider those lesions as benign (Thy2).
The molecular screening of both FNAs and corresponding FFPE samples (that was so far performed only by Cantara et al. [13] and in our recent study [14]), allowed the definition of a precise cutoff value by the application of ROC statistics for the allelic percentage of the point mutations, which has to be exceeded to consider a FNA sample mutation-positive (Fig. 1). This definition of a precise cutoff value led to an accuracy of 98% for our molecular FNA testing versus the molecular testing of the corresponding FFPE samples, resulting in a true sensitivity and specificity of the mutation detection of 94% and 100%, respectively. Previous studies without cutoff value determination reported sensitivities of 88% and 76%, and specificities of 100% and 98%, respectively (13,14).
A significant 20% gain of sensitivity from 60% (cytology alone) to 80% (cytology and mFNA combined) could be observed by combining cytologic evaluation and mFNA (Table 2), while the specificity slightly decreased from 100% to 95% (if RAS-positive FAs were considered as false positives) (McNemar test, p<0.05). However, there are several previously discussed reasons (8) that could justify the consideration of RAS-positive FAs as true positives (which would result in a sensitivity of 82% and a specificity of 100%). In addition, one point is of particular interest, especially with regard to the comparison of our present data with the data published by Nikiforov et al. (10). RAS-positive FAs may represent tumors for which capsular or vascular invasion was not detected by histologic examination because of sampling bias. This assumption is supported by a recent prospective study defining the limitations of histologic thyroid nodule evaluation by Cibas et al. (21). While a disagreement between benign and malignant histologic diagnoses occurred in 9.7% of histopathologic assessments, the highest percentage of discordant histologic assessments involved minimally invasive FTCs and HCCs, which are diagnosed by evidence of capsular or vascular invasion (21). In 61% of FTCs/HCCs with capsular invasion and in 50% of FTCs/HCCs with vascular invasion, discordant diagnoses (benign versus malignant) were established by expert histopathologists (21). Similar results have previously been published by others (25 –27). This high rate of histopathologic discordance is a dilemma for translational studies of molecular markers aiming to improve the presurgical diagnosis because the histologic reference for these studies is obviously imprecise. In the studies of Nikiforov et al. (10,11) the histopathologic diagnosis was established by a pathologist, who was aware of the results of the molecular testing, thus this knowledge has most likely directly influenced the histopathologic diagnosis of FAs/FTCs/fvPTCs. This issue adds to the well-known interobserver variability in the diagnosis of fvPTC (28). In our series, we followed stringent morphologic criteria, being completely unaware of the molecular status.
Indeed, for our data set the histologic re-evaluation of 10 RAS-positive cases originally diagnosed as FAs/HCAs revealed (by the identification of capsular invasion) a revised diagnosis of minimally invasive FTCs for 3 NRAS-positive samples initially classified as FAs while none of the RAS-negative adenomas was reclassified. This revised histologic classification resulted in both an increased sensitivity and specificity of the molecular panel screening. Hence, the problem is that while in the evaluation of molecular markers a precise histologic reference is mandatory, the knowledge of the molecular testing (especially the presence of RAS mutations) may also lead to the revision and improvement of histologic diagnoses by the histologic identification of minimally invasive FTCs.
In comparison to our previous study in which RAS-positive adenomas did not undergo histologic re-evaluation (14), the sensitivity of detecting malignant tumors in the cytologically indeterminate group increased from 18% (86% specificity) to 61% (92% specificity; combining the Thy3 and Thy4 groups) and is comparable to the study by Nikiforov et al. (10) with a sensitivity of 61% and a specificity of 98% (combining the Bethesda categories (15) atypia of undetermined significance/follicular lesions of undetermined significance, follicular or Hürthle cell neoplasm/suspicious for follicular neoplasm, and suspicious for malignant cells). Because we did not change the methodology of point mutation and rearrangement detection in routine air-dried FNA smears in comparison to our previous study, our present data show that the awareness of the mutation status by the pathologist as described above, and as evident in previous publications (10,11), is an aspect influencing the outcome of the molecular panel screening.
The histologic composition of the indeterminate samples is an additional important characteristic for a better comparison of our approach using air-dried FNA material with previous studies using fresh FNA material. While in our previous study the percentage of fvPTCs and PTCs in the indeterminate category was rather low (3%), this percentage is 12% in the indeterminate category of this study and thus compares better to a percentage of 21% in the study of Nikiforov et al. (10), eliminating a low percentage of fvPTCs and PTCs in this cytologic category as likely reasons for different sensitivities or specificities. However, the prevalence of BRAF and RAS mutations in the fvPTCs significantly differs between the study of Nikiforov et al. (10) and our present study. While the most prevalent mutations in fvPTCs are RAS mutations (54%) in the study by Nikiforov et al. (10), followed by PAX8/PPARG (4%), and BRAF (3%) mutations, we did not find any RAS and PAX8/PPARG mutation, but 50% (11/22) of fvPTCs harbored a BRAF mutation (9 V600E, 2 K601E). Furthermore, in the present study we observed a higher percentage of RAS mutations in the FTCs compared to the study of Nikiforov et al. (48% vs. 36%). Based on these differences, one could suppose that the histologic criteria for the differential diagnosis of fvPTCs and FTC might differ slightly (i.e., we classified PTCs as follicular variants only when showing exclusively or almost exclusively a follicular pattern of growth, with no papillary structure but typical nuclear features), it is possible that the diagnostic criteria in the study by Nikiforov et al. are broader. It is also possible that, being aware of the presence of a RAS mutation, the pathologist is prompted to emphasize ambiguous morphologic features. As for FTC, variability in the diagnosis of fvPTCs has also been reported previously (28). These findings demonstrate that the gold standard (i.e., histology) can be improved by incorporating molecular findings, which need to be adjusted to variations of diagnostic criteria for specific histologic diagnoses. In any case, our data demonstrate that routine air-dried FNA smears are as adequate as fresh FNA material used by Nikiforov et al. (10,11) and others (12,13) for molecular screening.
In the diagnostically most important Thy3 group representing follicular lesions, the molecular panel screening revealed an increase of the risk of malignancy from 28% before the molecular screening to 71% for mutation-positive samples, and a decrease to 18% for mutation-negative samples (Table 3). Our data show that this improvement is achieved by the screening for both BRAF and RAS mutations, while we did not observe any PAX8/PPARG rearrangement. Although the latter finding is at variance to our previous study (14), it confirms the rather low prevalence of PAX8/PPARG rearrangements observed in previous studies (10,11,13). The lack of RET/PTC rearrangements in this study is also at variance to previous studies (11,13) thus suggesting regional differences in the prevalence of this rearrangement. Because of the 97% risk of malignancy in the Thy4 group, there is no significant potential to improve the cancer diagnosis by the molecular screening in this group. Moreover, this high cancer prevalence is also responsible for the low NPV in the Thy4 group.
ROM, risk of malignancy.
Nevertheless, despite the low diagnostic potential, the knowledge of the mutational status is likely to provide additional prognostic information. Our data also show that the current mutation panel does not cover a sufficiently broad range of mutations to identify all thyroid carcinomas in the cytologic indeterminate categories because 48 of 118 carcinomas detected by histology were mutation-negative.
In conclusion, our data suggest that molecular FNA testing improves presurgical diagnosis using air-dried smears. The discrepant sensitivities and specificities reported in previous studies are most likely related to the use of different grading schemes resulting in a different composition of the cytologic categories, and a different prevalence of RAS mutations in follicular carcinomas. Moreover, the knowledge of the molecular testing (especially the presence of RAS mutations) supports the histologic identification of minimally invasive follicular carcinomas, which is characterized by a well-known high interobserver variation and sampling bias.
Footnotes
Acknowledgments
This research was supported by a Deutsche Krebshilfe grant (109994) to Markus Eszlinger. Ralf Paschke is supported by DFG and Krebshilfe and Wilhelm Sander Stiftung project 2013.010.1. Furthermore, this research was supported by Qiagen GmbH (Hilden, Germany) by providing kits and technical equipment.
Author Disclosure Statement
No competing financial interests exist.