
Abstract
Background:
Hypothyroidism has been associated with cognitive and motor impairments that are likely to constitute hazards in the operation of motor vehicles and a public safety risk. However, there is a paucity of data that would provide an evidence basis for recommendations to hypothyroid patients. The purpose of this study was to determine the specific neurological and psychological deficits consequent to hypothyroidism and whether they are of sufficient magnitude to impede the safe operation of motor vehicles.
Methods:
Repeated measurements were obtained in euthyroid, hypothyroid, and euthyroid hormone replaced states of thyroid cancer outpatients, at an academic medical center, who underwent thyroid hormone withdrawal preparation for radioiodine scanning. Study design used a within-subjects longitudinal “A-B-A” with each subject tested at three visits in the same sequence: euthyroid, hypothyroid, and euthyroid for a total of 32 subjects. Data on clinical status and cognitive performance were collected using standard instruments, including ThyDQoL and ThySRQ measures, National Adult Reading Test, Boston Naming Test, Mini-Mental State Exam, Wechsler Adult Intelligence Test-Revised, Letter Fluency FAS, and Beck Depression Inventory. Fine-motor function was measured with an automated assessment panel, and driving performance on a commercial driving simulator.
Results:
In severe hypothyroidism (median thyrotropin 83.2 mIU/L), fine-motor performance of hands and reaction times in emergency braking tests were slowed, as well as subjective slowing reported on structured clinical scales. Depression was present, typified by vegetative and mood alterations, but lacking reported guilt and lowered self-esteem seen in other types of depression. Cognitive impairment was characterized by declines on speeded executive tests. In contrast, episodic memory performance improved over time regardless of thyroid hormone status. Braking times increased in hypothyroidism by 8.5%, equivalent to reports of effects from a blood alcohol level of 0.082 g/100 mL (above the U.S. legal driving limit).
Conclusions:
Transient profound hypothyroidism is characterized by reversible depression, decreased fine-motor performance, slowed reaction times, and decreased processing speed. These data represent new empirical evidence that support the recommendation that complex activities requiring rapid responses, such as operating motor vehicles, should be avoided during hypothyroidism. This has broader implications regarding functional impairments and risk to public health.
Introduction
H
Materials and Methods
Study population and recruitment
Patients were invited to take part in the study if they had been diagnosed with thyroid cancer and had undergone post-thyroidectomy radioiodine ablation therapy at the University of Kentucky Thyroid Oncology Program utilizing hypothyroid preparation. Such patients are typically evaluated with radioiodine whole body scanning (independent of this study) approximately six months later, again utilizing a hypothyroid preparation (off levothyroxine and on liothyronine for four weeks, then off of liothyronine with a low-iodine diet for two weeks prior to radioiodine scanning). For all subjects, recruitment, informed consent (as approved by the University of Kentucky Institutional Review Board), and initial phase of study evaluation were obtained while in a euthyroid state. Additional inclusion criteria included age 18–70 years, at least two years' driving experience, valid driver's license, and normal corrected visual acuity. Subjects were excluded if there were active medical problems other than thyroid cancer requiring new investigation or treatment, cognitive impairment or psychoactive medications likely to cause such impairment, potentially interfering neurologic disorders (epilepsy, head injury with more than a five-minute loss of consciousness), or disabilities that would interfere with assessment of driving and motor performance (e.g., stroke, spinal disease, or Parkinson's disease).
Study design
The experimental design was a within-subjects longitudinal “A-B-A” in which each subject underwent tests at three visits in the same sequential order: euthyroid, hypothyroid, and euthyroid hormone-replaced (recovery) states. Target recruitment was 32 subjects based on a preliminary power analysis, with replacement of dropouts to maintain this target. In all, 40 subjects were recruited; eight subjects completed only the first visit and withdrew due to motion sickness during the driving tasks or for undisclosed personal reasons.
Study measures
Basic clinical data, consisting of serum thyrotropin (TSH) and free thyroxine (fT4) levels, clinical hypothyroidism scores (7,8), and underactive thyroid-dependent quality of life and perceived impact scales (ThyDQoL and ThySRQ) (9), were collected at each visit. TSH was measured using immunochemiluminescence on a Beckman Coulter Unicell Dxi platform. The lower limit of sensitivity of the assay was 0.01 μIU/mL. The intra-assay coefficients of variation for TSH were 4.9% at 0.40 μIU/mL and 4.4% at 32.93 μIU/mL. fT4 was determined using an electrochemiluminescence immunoassay on a Roche Cobas 8000 modular analyzer. The lower limit of sensitivity of the assay was 0.1 ng/dL. The intra-assay coefficients of variation for fT4 were 7% at 0.67 ng/dL and 2.7% at 4.02 ng/dL.
The Human Motor Assessment Panel (HuMAP) was utilized to assess fine-motor function. The HuMAP (10) is an automated measurement apparatus for assessing speed of proximal and distal movements of the upper extremities. The apparatus comprises a transparent plastic vertical plate equipped with left- and right-arm portals through which the individual reaches to gain entry to an inner chamber divided into left and right halves. In separate tasks of increasing difficulty, the patients were instructed to retrieve a steel nut from one of four inserts including a level platform (level one), a straight rod (level two), a question-mark-shaped rod (level three), and a double-S-shaped rod (level four). There were five trial repetitions completed per hand per task before proceeding to the next level of difficulty (n=10 trials/task). Participants began each repetition when a randomly timed light flashed to indicate when to start. Based on previous experience, performance times for the two lower levels of fine-motor difficulty and for the two higher difficulty levels were combined by averaging, and further combined by averaging for the left and right hands. This procedure results in two automated measures: a simple and a complex average fine-motor performance time for each subject at each visit. Reaction time, the interval between the start of the task, and hand entry through the outer portal, were measured and combined in the same way as for the fine-motor performance time, resulting in a simple and complex average reaction time for each subject visit.
Psychometric testing was performed to assess cognitive function. At each visit, subjects completed a psychometric battery designed to detect changes in cognition and mood. These tests included standard measures of baseline estimated IQ (North American version of the National Adult Reading Test), naming (Boston Naming Test), global cognition (Mini-Mental State Examination; MMSE), immediate recall (Wechsler Adult Intelligence Test—Revised; WAIS-R Logical Memory A and B), working memory (digits forward and backward), processing speed (WAIS-R Digit Symbol Substitution), attention and sequencing (Trials A and B), lexical retrieval (Letter fluency FAS), delayed recall (WAIS-R Logical Memory II), and mood (Beck Depression Inventory; BDI (11)).
Driving performance was assessed using a driving simulator. At each visit, subjects performed three driving tasks using a simulator (STISIM Drive M400): (a) braking on and off, (b) divided attention to a distracting arrow in the peripheral field, and (c) a driving navigation task to and from a target location using a guide map. In the first task, the subject was told to step on the foot brake as quickly as possible in response to a random flashing stop signal. Time to brake and time to release the brake were recorded for each of three repetitions. In the second simulation, the subject was instructed to drive steadily in their lane along a straight road, and indicate by pressing a corresponding button the direction of an arrow that randomly appeared and disappeared in the upper left peripheral field. Frequency and accuracy of arrow appearance and direction, and any out of lane deviations, speeding, and collisions were recorded. The third task involved driving to a target location and back to the starting point using a provided map. Completion time for each leg of the drive and number of traffic violations (e.g., wrong way on a one-way street, striking a pedestrian) were recorded. Driving simulation testing has been shown to be a sensitive reflection of true road driving performance (12).
Statistical analyses
A within-subjects analyses, across all three visits, were performed using a standard multivariate analysis of variance repeated-measures model (JMP 9.0, SAS Institute). Paired t-tests were performed when comparing data from two visits. A p-value of <0.05 was considered significant for these planned comparisons.
Results
Clinical data
The entire group of 32 subjects was verified as euthyroid at visit 1 and hypothyroid at visit 2. Data from each of these 32 subjects were included in the analyses comparing data from visits at time-point one versus time-point two. However, at the completion of data collection, several of these 32 participants were identified who were tested at the third visit too soon after beginning thyroid hormone replacement. Thus, a subgroup of 20 subjects was formed with verified euthyroid state at visit 3 by clinical and laboratory criteria (Recovery subgroup) for inclusion in analyses comparing each of the three time points (i.e., the A-B-A design). Basic demographic data for the whole group and the Recovery subgroup are given in Table 1. Most subjects were postsecondary-educated, right-handed, middle-aged females with at least a decade of driving experience. All were native English speakers. The intervals from initial euthyroid state to hypothyroid nadir, and from hypothyroid nadir to a restored euthyroid state, were about two months on average.
Table 2 characterizes the Recovery subgroup at visits 1 (euthyroid), 2 (hypothyroid), and 3 (euthyroid recovery). These data include TSH and fT4 levels, scores from the Zulewski clinical hypothyroid scale, and Quality of Life assessment scores. For the whole group visits 1 and 2, respectively, median TSH was 0.82±0.28 versus 95.4±8.4 mIU/L (p<0.0001), and there were significantly worsening ThyDQoL and Clinical cores similar to the first two visits in the Recovery subgroup. The full data table for the whole group is available upon request (see Supplementary Tables; Supplementary Data are available online at
ThySRQ was rated at the hypothyroid second visit only (t-test for mean of zero). F- and p-values were computed from a standard multivariate analysis of variance (MANOVA) repeated measures analysis of each variable. Visit 1—Three p-values were computed from a paired t-test. Clinical scores are from the Zulewski Scale (7).
Mean±SEM for quality of life. Scores: excellent, 3; very good, 2; good, 1; okay, 0; bad, −1; very bad, −2; extremely bad, −3.
Mean±SEM for expected quality of life if euthyroid (assessed at time of hypothyroidism). Scores: very much better, 3; much better, 2; a little better, 1; the same, 0; worse, −1.
Missing values made the total n<20.
Shape of the trend line connecting data points for the three visits was classified as: A, monotonic increasing through visits 1–3; B, visit 2 greater than (+) or less than (−) both visit 1 and visit 3 (hypothyroid visit different from both euthyroid). Thus, B+ represents a peak at visit 2, B− denotes a valley at visit 2.
TSH, thyrotropin; fT4, free thyroxine.
HuMAP
Figure 1 illustrates the results of repeated upper extremity motor testing in the Recovery subgroup. Performance was slower when subjects were hypothyroid on all motor tasks (Table 3). The greatest percentage change was in complex fine-motor time. Perceived “slowing of movement,” a yes–no clinical item on the clinical hypothyroidism scale (7), was increased at visit 2 when the subjects were hypothyroid (percent of subjects endorsing this symptom). Paired comparisons of the same measures between visits 1 and 2 in the whole group were significant (see Supplementary Tables).
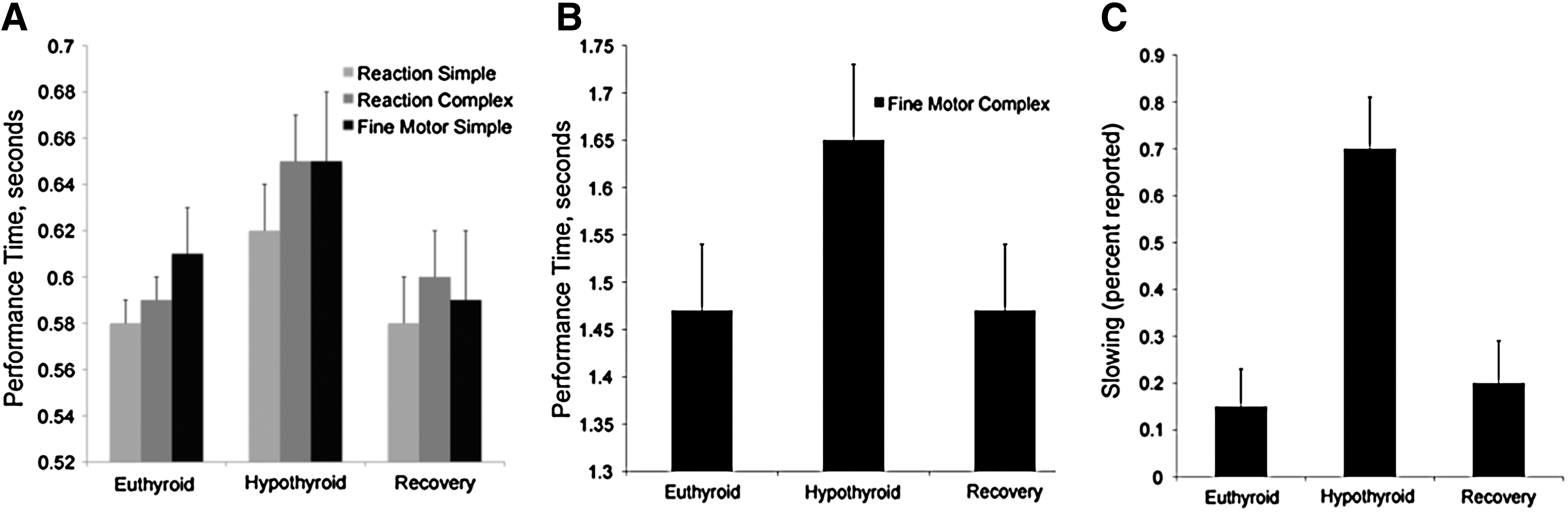
Fine-motor and reaction times. Human Motor Assessment Panel (HuMAP) motor performance and reaction times were measured at three visits during the study and their perceived slowing was rated during the same visits. (
Percent of group reporting subjective slowed movement on clinical interview entered on last row for comparison. F- and p-values were computed from a standard MANOVA repeated measures analysis of each variable. Visits 1–3 p-value computed from a paired t-test. N=19 (1 of 20 subjects completed psychometric testing and driving studies, but not HuMAP testing).
Shape of the trend line connecting data points for the three visits was classified as: A, monotonic increasing through visits 1–3; or B, visit 2 greater than (+) or less than (−) both visit 1 and visit 3 (hypothyroid visit different from both euthyroid). Thus, B+ represents a peak at visit 2, B− denotes a valley at visit 2.
HuMAP, human motor assessment panel.
Psychometric testing results, except for Trials A and B and digit forward and reverse, demonstrated a significant effect of time in the Recovery subgroup analysis (Table 4). Longitudinal trends across the three visits fell into two basic groups: (a) a peak or valley indicating an effect of worsening at visit 2, when subjects were hypothyroid, in contrast to the euthyroid visits 1 and 3; and (b) a monotonic trend of improvement across the three visits. Key results are shown in Figure 2, illustrating a decrease in digit symbol score and an increase in BDI score in subjects when hypothyroid, in contrast to the steady improvement in logical memory delayed recall scores across visits regardless of thyroid status.
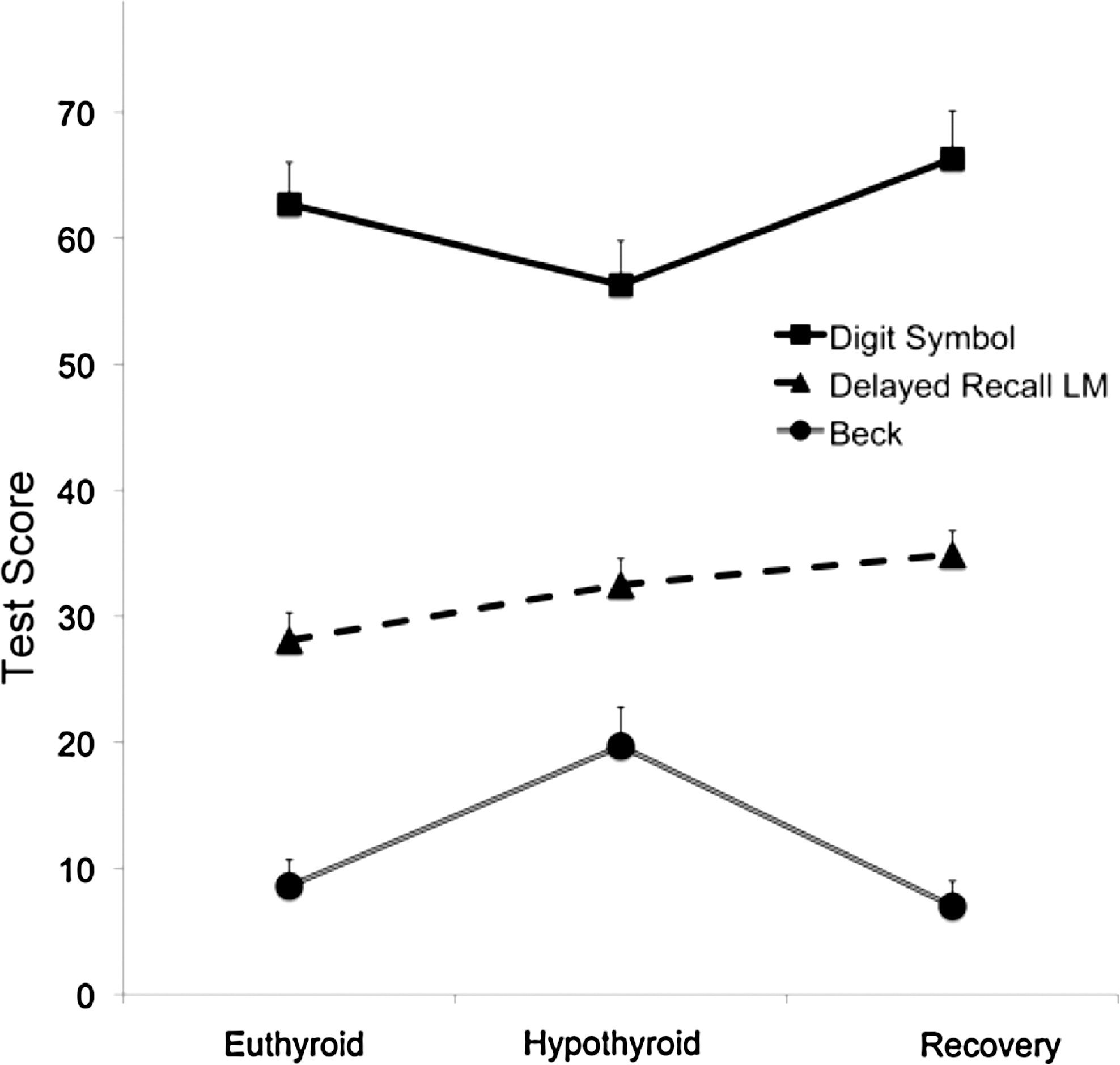
Psychometric testing. Speeded executive tasks such as Digit Symbol show worsening during visit 2 when subjects were hypothyroid (squares). Symptoms of depression from the Beck Inventory were also increased at this visit (circles). In contrast, delayed memory testing had a monotonic increasing trend to higher scores (triangles). Error bars are ±standard error of the mean; all trends are significant.
F- and p-values were computed from a standard MANOVA repeated measures analysis of each variable. Visits 1–3 p-values computed from a paired t-test.
MMSE, Mini Mental State Examination (range 0–30); LM, WAIS logical memory (range 0–40); AMNART, North American version of the National Adult Reading Test. Beck II Inventory cutoffs: 0–13, minimal depression; 14–19, mild depression; 20–28 moderate depression; and 29–63, severe depression. At visit 2 the Beck Inventory range was 3–49.
Shape of the trend line connecting data points for the three visits was classified as: A, monotonic increasing through visits 1–3; and B, visit 2 greater than (+) or less than (−) both visit 1 and visit 3 (hypothyroid visit different from both euthyroid). Thus, B+represents a peak at visit 2, B− denotes a valley at visit 2.
The mean BDI score at visit 2 was 19.7 (range 3–46), indicating mild to moderate depression. Because hypothyroidism was associated with a potentially clinically significant increase in depression, an analysis of the contributing items comprising the index was performed in the Recovery subgroup to probe in more detail (Table 5). Vegetative and anhedonic scores were notably increased at visit 2 (e.g., fatigue; loss of pleasure, interest, and energy; concentration difficulty and indecisiveness; and sleep and appetite alterations). Mood (crying and sadness) was moderately increased. In contrast, scores representing diminished self-image were not increased (worthlessness, self-dislike, feelings of punishment, pessimism, and dwelling on past failures; p=0.08–0.90). Exceptions to these generalizations were that suicidal thoughts/wishes were not significantly increased (p=0.08), and irritability, classified as a mood symptom, was notably elevated in the hypothyroid state (p=0.0009).
Values given for visits represent the mean for all subjects. Each Beck item score ranges from 0 to 3. Beck items are grouped conceptually as mood/self-image, anhedonic, and vegetative/mental categories.
Shape of the trend line connecting data points for the three visits was classified as: A, monotonic increasing through visits 1–3; B, visit 2 greater than (+) or less than (−) both visit 1 and visit 3 (hypothyroid visit different from both euthyroid); and C, visit 3 greater than (+) or less than (−) both visit 1 and visit 2.
Significant effects of hypothyroidism on psychometric tests and Beck item scores were supported by the whole group analysis of visits 1 and 2, notably improvements in global MMSE and delayed memory but worsening in processing speed (Digit Symbol) and Beck Inventory scores (see Supplementary Tables).
Driving simulator performance
Emergency braking on, off, and total times were significantly delayed by 8% on visit 2 (Fig. 3) when subjects were hypothyroid. Restoration of euthyroidism also restored the reaction time for braking. Divided attention errors were less frequent, and map-assisted driving times decreased, at visit 3 compared to both visit 1 and visit 2 (Table 6).

Driving simulator performance. Emergency braking reaction times are depicted in response to the sudden appearance of a stop sign. Total reaction time was divided between releasing the gas pedal and depressing the brake. Reaction times are longer during visit 2 when the subjects were hypothyroid. Error bars are ±standard error of the mean; all trends are significant.
Includes only subjects who had complete driving test data at all three visits. Reasons for incomplete data include: (a) nausea/motion sickness, (b) session terminated by crash/accident, (c) computer simulation error, and (d) subject protocol error. There was no difference in frequency of these events between visits.
Shape of the trend line connecting data points for the three visits was classified as: A, monotonic increasing through visits 1–3; B, visit 2 greater than (+) or less than (−) both visit 1 and visit 3 (hypothyroid visit different from both euthyroid); and C, visit 3 greater than (+) or less than (−) both visit 1 and visit 2. Thus, C− represents the trend where values at visits 1 and 2 are comparable, but are decreased at visit 3.
Discussion
Thyroid hormone has protean and ubiquitous effects upon diverse body tissues. Thus, it is not surprising that neurological effects of hypothyroidism would be clinically consequential. However, physicians do not routinely warn their hypothyroid patients to avoid circumstances in which hypothyroid neurological impairment could be dangerous. Even the joint practice guidelines of the American Thyroid Association and the American Association of Clinical Endocrinologists fail to mention this concern (13). Accordingly, objective evidence of significant effects of hypothyroidism on neurological function and motor vehicle operation could justify admonitions against driving while hypothyroid, reflecting similar warnings given to patients impaired by medications or neurological dysfunctions. The findings with the greatest clinical relevance are the characterizations of depression and motor slowing following complete removal of thyroid hormone. Global subjective quality-of-life indicators declined significantly while subjects were hypothyroid, suggesting that measures of depression and of motor slowing are of clinical value. Slowed driving reaction times are relevant to driving safety recommendations for hypothyroid patients.
Other studies have documented changes in cognitive, psychological, and physiologic functioning associated with decreased thyroid hormone. Subtle working memory deficits have been found in subclinical hypothyroidism (14), and some deficits are reported persisting in patients after thyroid hormone replacement (15). The length and severity of hypothyroidism, lack of cross-sectional controls, and patient age may be factors for the failure to document improvement despite replacement (16,17). In clinically hypothyroid patients, deficits in working memory, attention, verbal learning, processing speed, and naming have been found, but not consistently across all domains (18 –21). Anxiety and particularly depression have been seen in hypothyroid patients in several studies (19,20,22,23). Delayed auditory and visual event–related potentials, indicators of disrupted central sensory processing, have also been found in hypothyroidism, although not always consistently with respect to early versus delayed peaks (24,25). Nonetheless, reversible decreased phosphorus energy metabolism has been previously demonstrated in the frontal lobes of hypothyroid patients evaluated in a similar study design (26), revealing alterations in brain biochemistry that corroborate this current study.
A recent driving study in thyroid hormone–withdrawn patients found no significant cognitive or motor function impairments relevant to driving (27). This study differed significantly from the present one in that it had a cross-sectional design comparing different groups of subjects, driving performance was not assessed directly by simulation but rather with a cognitive driving fitness test, and there was overlap in free triiodothyronine levels between groups. The study design was problematic because prior administration of recombinant human TSH (Thyrogen®) likely interfered with documentation of the euthyroid state. No previous studies, as far as can be ascertained, have reported measurements before, during, and after an induced measurable period of confirmed hypothyroidism documenting quantified motor and driving performance using this design; this report is unique in that respect.
Depression was assessed using the BDI, a validated self-report questionnaire. By examining the individual items of the BDI, it was found that the most robust effects on the total score comprised symptoms denoting fatigue, lack of energy, and vegetative change. These symptoms are nonspecific in that they are also associated with general medical conditions lacking depression per se. However, additional increased symptoms of sadness and crying indicate that in hypothyroidism, there is a true mood disorder and not simply an artifactual increase in BDI scores due to medical illness (28). Suicidal ideation was only marginally increased on the BDI item scores. Nonetheless, clinicians managing even transient hypothyroidism should remain alert to this danger. The absence of symptoms reflecting loss of self-esteem, guilt, and pessimism was a notable feature of the depression in this study group. Recovery of depression with thyroid hormone restitution was the rule.
Motor slowing was clearly evident in this study. Fine-motor movements of the hand slowed by 13%, and simple movement of the shoulder and arm by 7%. Reaction times also increased on both the HuMAP and driving simulator braking tasks. Upper extremity reaction times on the HuMAP increased by 7% (simple level) to 10% (complex level). Braking times were increased in the same range by 8.5%. To illustrate the potential significance of these results they were compared with the known motor slowing caused by alcohol ingestion (29). Powell et al. (30) found that visual reaction times increased by 8.2% at a blood alcohol concentration (BAC) of 82 mg/dL (17.8 mmol/L), similar in magnitude to the slowing observed in hypothyroidism, and representing an estimate of equivalence between effects of BAC and hypothyroidism. A BAC of 80 mg/dL (17.4 mmol/L) is the legal limit for driving in the United States. Several countries have legislated much lower limits, for example Sweden, where the limit is 20 mg/dL (4.3 mmol/L) based on alcohol-related risks noted at these levels. The relative risk of involvement in a casualty crash has been estimated as 1.8 for a BAC of 50 mg/dL (10.9 mmol/L) and 3.2 at a BAC of 80 mg/dL (31). Thus, the motor slowing in hypothyroidism as seen in this study is clinically significant, even if the reaction time equivalence between BAC and hypothyroidism is not exact. Additionally, supporting the relevance of these observations, subjects reported “slowed movements” when hypothyroid approximately three times more often at their structured clinical interview and affirmed both indecisiveness and difficulty with concentration two to three times more often on the BDI when hypothyroid. It has been shown that self-reported driving impairments often underestimate those determined by objective assessments (32).
Reaction and motor performance times could represent a bridge between simple motor performances and more complex generalized tasks, for example divided attention and map-guided driving. However, an increase was not observe in divided attention error, navigation error, or road violations (e.g., tailgating, speeding, line crossings, or failure to stop at signals) on the driving simulations when comparing initial euthyroid and second visit hypothyroid conditions. Rather, there were reduced errors and reduced traffic violations on the third, euthyroid recovery drive. A rebound improvement in performance following recovery from hypothyroidism, or a failure to make expected improvements in performance while hypothyroid, could both explain the observation. The second interpretation is favored because a similar rebound pattern was rarely seen on the other study measures.
It is shown that slowed braking reaction times in hypothyroidism are roughly equivalent to reaction slowing with a BAC of 80 mg/dL. However, in other driving domains, effects of transient hypothyroidism differ from alcohol intoxication; for example, divided attention error has been well documented (33,34). As long as there were no sudden emergencies requiring immediate responses, the subjects of this study appeared to have preserved simulated general driving performance while hypothyroid. Slowed reaction times appear to present the main safety threat in driving while hypothyroid.
In contrast to the consistent motor slowing on the HuMAP, which reverted to baseline levels in the recovery euthyroid state, psychometric testing demonstrated intriguing preservation of certain test performances during the course of the study. There were consistent improvements in global cognition, immediate and delayed story memory, and lexical retrieval, despite intervening hypothyroidism between the initial and recovery euthyroid states. Thus, despite declines in measures of attention, sequencing, and processing speed that might indicate impeded general cognitive function, verbal memory and global measures showed only improvement, likely due to test learning effects. This finding suggests that transient hypothyroidism spares episodic learning and memory retrieval mechanisms in the brain, in direct contrast to the conclusions of some studies (19) but consistent with several others (14,20). Future research will be required to assess the effects of more prolonged hypothyroid states on episodic memory and on the long-term reversibility of the cognitive deficits that were observed in this investigation.
A few caveats concerning this study are worthy of mention. There are potential causes of distractibility other than hypothyroidism that could have affected driving. The consequences of dealing with cancer are stressful, perhaps reflected in the quality of life and BDI scores. However, this factor cannot be assessed, since all of patients in this study had thyroid cancer. Multiple comparisons were not corrected for. Therefore, due caution suggests avoiding over-reliance upon the specific strength of results for single variables but rather to note the aggregation pattern of related measures associated with the same category, for example motor slowing. The lack of euthyroid recovery data in 12 of the 32 subjects is an additional limitation, although subgroup analysis supported consistency of results compared to the entire cohort. Finally, it should be emphasized that these results apply to the severely hypothyroid state seen with preparation for radioiodine scanning and does not provide evidence permitting extrapolation to milder degrees of hypothyroidism.
Nonetheless, these results, demonstrating significant motor and cognitive slowing on objective measures, provide support for clinical recommendations emphasizing caution when engaging in potentially dangerous activities during a severely hypothyroid state. It is not possible to predict when a sudden defensive driving maneuver might be called for, and the data from this study suggest that such a reaction would be significantly slower than normal. This provides objective evidence warranting admonitions against operating motor vehicles for profoundly hypothyroid patients and confidence in removing such stipulations upon restoration of a euthyroid state. Patients are considered to be euthyroid after administration of sufficient amounts of levothyroxine, over the course of four to six weeks, that result in normalization of TSH levels. However, this study was not designed to determine the minimal interval after levothyroxine replacement for restoration of normal driving performance.
Footnotes
Acknowledgments
This work was funded by a grant from Genzyme, a Sanofi company (Cambridge, MA). Genzyme had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript, or the decision to submit the manuscript for publication.
In addition, Dr. Ain is an employee of the Veterans Affairs Medical Center. The views expressed in this article are those of the authors and do not necessarily reflect those of the Veterans Affairs Medical Center.
Author Disclosure Statement
No competing financial interests exist.