
Abstract
Background:
Extranodal extension (ENE) is a documented negative prognostic factor in patients with papillary thyroid cancer (PTC). ENE is presumed to manifest in larger lymph nodes. Yet, to date, no study has proven this. This is a pilot study that specifically examines the size distribution of positive lymph nodes manifesting ENE in patients with PTC.
Methods:
An Institutional Review Board approved review examined the size of all lymph nodes demonstrating ENE in postoperative PTC patients that underwent surgery for PTC under the care of a single surgeon between 2004 and 2014. All patients in the study had regional metastatic lymph nodes with ENE. Analysis of the size distribution for all lymph nodes with ENE was performed.
Results:
A total of 47% of lymph nodes with ENE were ≤10 mm.
Conclusions:
Results indicate that clinically nonevident, small lymph nodes are at risk of harboring aggressive disease biology reflected in ENE. A total of 47% of all nodes fell within Randolph et al.'s classification of “small” lymph nodes, while 59% of the nodes with ENE were <1.5 cm—the threshold size that was deemed to be prognostically significant by Ito et al. It is apparent that clinically nonevident regional lymph nodes can have adverse histologic features and that the previous presumption that nodes with ENE only appear in clinically evident, macroscopic nodes is flawed.
Introduction
U
Furthermore, the presence of disease spread outside of the capsule of the lymph node, referred to as ENE, has emerged as an important prognostic variable. Growing evidence has demonstrated that ENE represents an aggressive phenotype of well-differentiated papillary thyroid cancer (PTC). Various prognostic studies have identified ENE as a harbinger of developing distant metastases, leading to an increased risk of recurrence, and a worse disease-free survival, increasing both the likelihood of tumor persistence and the development of systemic disease (4,5). These prognostic studies served as a platform on which this pilot study was developed.
A widely held presumption in thyroid cancer management is that small lymph nodes are innocent and that ENE only occurs in lymph nodes that have reached the threshold size to be deemed clinically evident. Randolph et al. concluded that “nodal size (microscopic/low volume vs. macroscopic/clinically apparent), number of positive nodes, and presence of extranodal spread importantly relate to the main nodal prognostic parameter of recurrence” (1). Furthermore, Lango et al. stated that ENE “can only be discerned when macroscopic tumor deposits are examined” and that “ENE is exceedingly unlikely with microscopic nodal disease” (5).
However, to date, no study has attempted to correlate the size of positive lymph nodes with the presence of ENE. In this preliminary pilot study, the size of metastatic lymph nodes that manifest ENE is evaluated specifically in order to determine whether lymph node size correlates with the ability of a cancer to break through the overlying capsule. The current study investigates the presumed innocence of smaller lymph nodes by assessing the size distribution of lymph nodes with ENE and aims to redefine clinically relevant lymph nodes.
Materials and Methods
This retrospective study was an Institutional Review Board approved review of 83 lymph nodes demonstrating ENE removed from 56 patients, treated for well-differentiated PTC from 2004 to 2014 by a single surgeon (M.L.U.) at Mount Sinai Beth Israel Medical Center in New York City. During the course of this 10-year study, the surgeon's philosophy on the performance of prophylactic central compartment node dissection has evolved and is currently based on a variety of features of the primary tumor and the overall disease process, such as the presence of lateral compartment adenopathy. Patient age at the time of surgery ranged from 11 to 84 years old. These 56 patients were identified from a cohort of more than 850 patients with a diagnosis of PTC who were operated upon by the surgeon during this time interval. As a pilot study, only those patients in whom the pathology report indicated ENE were included in this study. Pathology slides and reports were reviewed by a senior pathologist (B.M.W.). ENE was defined as extension outside the lymph node capsule with identification of tumor in perinodal soft tissues (e.g., fat, skeletal muscle, other).
Lymph nodes with ENE were measured for their maximum diameter. The total number of extracted lymph nodes, the number of nodes demonstrating ENE, the size of the metastatic focus of disease within the lymph node, and the patient's disease stage were noted. Complete data sets, such as number of positive lymph nodes, number of lymph nodes examined, and the size of the metastatic focus of disease, were not available for all patients because this information was not routinely reported. The current study spanned 10 years. However, the data are skewed toward the latter years due to increased attention being paid to the importance of reporting ENE.
Results
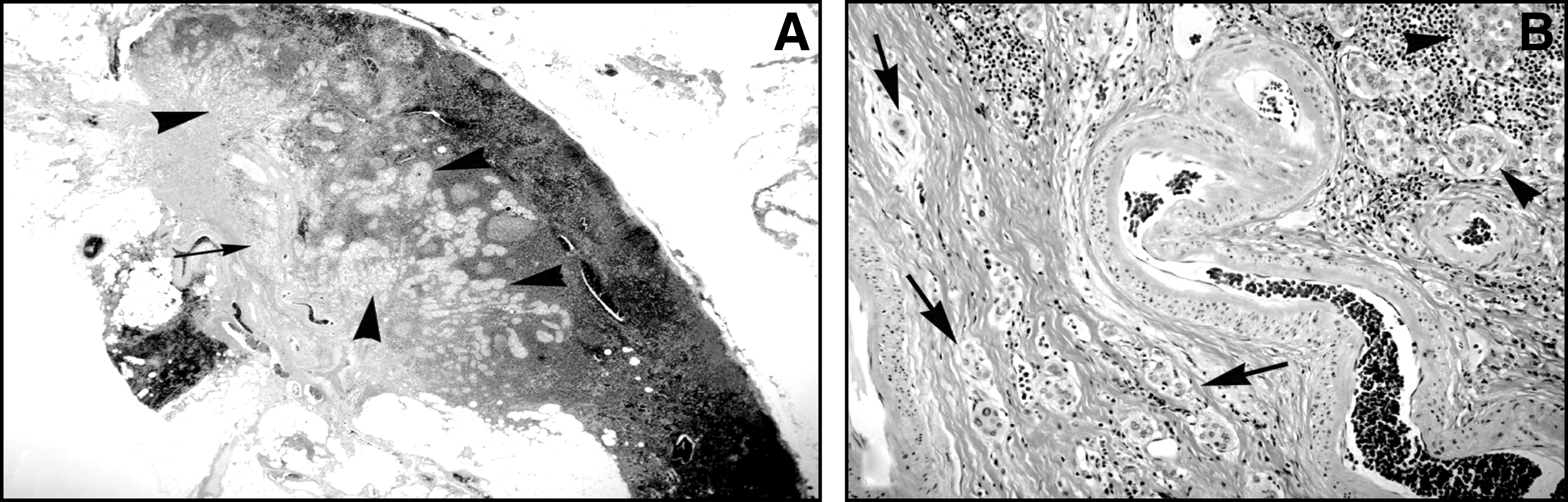
Lymph nodes manifesting ENE ranged from 1.6 mm to 4.1 cm. The number of nodes manifesting ENE in a single patient ranged from one to nine nodes. Thirty-nine lymph nodes (47%) were ≤10 mm in diameter (Table 1). Within this category, 17 nodes (20.5%) were ≤5 mm in diameter, and 22 (26.5%) were between 6 and 10 mm in diameter. Twenty-four nodes (28.9%) were between 11 and 20 mm, and the remaining 20 nodes (24.1%) were ≥21 mm. Only one (1.2%) of the lymph nodes with ENE in this series was >30 mm. It is important to note that the recorded measurement of the node reflects the maximum diameter of the lymph node, but the size of the metastatic deposit was often smaller than the nodal diameter (Figs. 1 and 2). It should be noted that slides from some of the older cases were not available for review of the area of the node encompassed by tumor. Because the College of American Pathologists (CAP) protocols in the past have not required standardized reporting for ENE, the growing awareness of the importance of ENE has led the clinicians at the authors' institution to request that the presence of ENE become a routine part of pathologic reporting; this explains the preponderance of ENE cases in the latter years of this study (Fig. 3).


Reporting of ENE over time.
While the majority of lymph nodes were completely effaced by metastatic deposits, there were lymph nodes manifesting ENE where as little as 50% of the cross-sectional area was consumed by tumor. Table 2 indicates the range of pathology of primary tumors. Eleven out of 56 patients underwent surgery for thyroid cancer after initial surgery at an outside institution. Distribution of the primary tumor favored a higher stage, with 26 out of 45 being T3 or T4a.
Discussion
Previous literature has provided compelling evidence regarding the importance of size of metastatic nodes, number of positive nodes, and presence of ENE in terms of prognosis of patients with PTC. Since these prognostic studies have already indicated ENE as a surrogate for aggressive disease, this study aimed to determine what size of positive lymph nodes need to be considered for this poor prognostic feature. Randolph et al. proposed that lymph nodes in PTC be characterized into the following size categories: micrometastasis (0.2–2 mm), small (2–10 mm), intermediate (10–30 mm), and large (>30 mm) (1). That meta-analysis identified that nonclinically evident nodes (cN0) have a risk of recurrence of 2%, whereas patients with clinically evident nodes (cN1) have a 22% risk. The results from the current study indicate that clinically nonevident, small lymph nodes are at risk of harboring aggressive disease biology reflected in ENE. A total of 47% of all nodes with ENE in the current study fell within Randolph's characterization of being “small,” while 59% of the nodes with ENE were <1.5 cm, deemed by Ito et al. to be the clinically significant size criteria (1,6). This study suggests that the previous presumption that nodes with ENE only appear in clinically evident, macroscopic nodes is flawed.
The analysis in the current study was intended to challenge the presumption that lymph nodes measuring <1 cm are not clinically significant. This study did not determine the incidence of ENE in all positive lymph nodes, nor did it determine ENE based on lymph node size, but it did identify that 47% of the lymph nodes that manifest ENE were ≤10 mm. The presumption is that metastatic deposits in lymph nodes reach the extranodal environment only when those deposits reach a critical size and when they have consumed the entire lymph node. The current study refutes this belief. Since ENE has been shown to correlate with poor disease-free survival and recurrence rates in previous studies (4,5,7) and because the biology and timeline of ENE progression is unknown, it is important to identify the occurrence of ENE in small lymph nodes. This analysis suggests that there is a risk of missing ENE in positive lymph nodes ≤10 mm.
Although ENE is not officially recognized in American Joint Committee on Cancer disease staging, it has been shown to have a negative prognostic impact in a number of different studies (4,5,7). Yamashita et al. demonstrated in a study of 324 patients with micro-PTC that ENE, not macroscopic lymph node metastases, is predictive of disease recurrence and poor prognosis (4). Leboulleux et al. found that more than three metastatic nodes with ENE correlated with a higher rate of recurrence in patients with PTC when compared to patients who had fewer than three positive lymph nodes with ENE (8). Recently, a study by Lango et al. identified several outcome measures associated with ENE in patients with PTC: diminished probability of a biochemical complete response, increased probability of structural tumor persistence, as well as systemic disease progression (5). Ricarte-Filho et al. further confirmed that ENE predicts recurrence and death due to disease. This evidence from these published studies reinforces the importance of studying the lymph node size in which ENE is capable of manifesting.
The 2009 American Thyroid Association clinical practice guidelines instruct surgeons to perform lymph node dissections when either biopsy-proven and/or clinically evident lymph nodes are encountered (9). Lymph nodes ≤10 mm are often not clinically evident, and the current belief system, while acknowledging the significance of ENE, does not appreciate that ENE can occur in these smaller nodes and can break through the capsule without engulfing the entire node. Metastatic deposits in lymph nodes, as evidenced by this study, do not have to consume the entire lymph node before extending into the extracapsular environment. This demonstrates that ENE can be an earlier event before a lymph node reaches a critical size and before the deposit consumes the entire lymph node architecture. Although the size of the metastatic focus was not available for all 83 lymph nodes, the results still support this belief.
It is important to highlight the fact that only 56 of 850 patients with PTC were identified as having lymph nodes with ENE, and therefore it is evident that this is a rare finding. While it is important to recognize that smaller nodes with aggressive features, such as ENE, may not be clinically evident, this is not intended to serve as justification for the performance of routine prophylactic central compartment node dissection. Results from this investigation indicate that clinically nonevident, small lymph nodes are at risk of harboring aggressive disease biology reflected in ENE. It is apparent that clinically nonevident regional lymph nodes can have adverse histologic features, and this characteristic is not just confined to clinically evident, macroscopic nodes. While the literature has identified ENE as a poor prognostic feature, it is not clear whether the size of lymph nodes with ENE has a further bearing on the disease prognosis. A more extensive study, currently underway, will evaluate all sizes of positive lymph nodes, the size of the disease foci, and correlation with the presence of ENE. ENE should be mandated in the pathologic reporting of thyroid carcinoma, and physicians should take care to identify this negative prognostic factor.
Footnotes
Acknowledgment
This research was supported by a generous grant from the Mount Sinai Health System.
Author Disclosure Statement
No competing financial interests exist.