
Abstract
Background:
Fatigue that persists post-treatment is commonly reported by thyroid cancer (TC) survivors.
Methods:
A systematic review of published English language randomized controlled trials (RCTs) on interventions for management of persistent post-treatment fatigue in TC was conducted. This review excluded studies on short-term interventions used in preparation for radioactive iodine diagnostic scans or treatment. An electronic search was executed in six databases and supplemented by a hand search. Two reviewers independently reviewed all citations from the electronic search and relevant full-text studies. Two abstractors independently critically appraised included studies and abstracted the data. The data were qualitatively summarized.
Results:
A total of 1086 unique citations and 25 full-text studies were reviewed. Four studies summarizing the results of three RCTs were included. The interventions included: combination triiodothyronine with levothyroxine (L-T4) therapy compared to L-T4 alone (one RCT), reduction in degree of thyrotropin (TSH) suppression using L-T4 compared to maintenance of TSH suppression (one RCT), and supervised exercise compared to inactivity (two RCTs examining different fatigue outcomes in same population). Trial duration ranged from 10 weeks to six months. All trials had limitations, and the number of TC survivors included in respective RCTs ranged from 15 to 36. Hormonal treatment RCTs had mixed fatigue outcome results within respective trials. However, multiple measures suggesting improvement in fatigue were reported following the exercise intervention.
Conclusions:
There is paucity of RCTs to guide evidence-based management of persistent post-treatment fatigue in TC survivors. RCTs of interventions for prevention or treatment of fatigue in TC survivors are needed.
Introduction
T
A scoping review was conducted recently in which the breadth of published literature relating to post-treatment fatigue in TC survivors was examined (4). In that overview of the literature, several randomized controlled trials (RCTs) of interventions for treatment of fatigue in this population were identified, and a need for an in-depth systematic review of such trials was indicated (4). The primary objective in this systematic review was to identify and critically appraise published RCTs of interventions for management of persistent post-treatment fatigue in TC survivors.
Methods
Eligibility criteria for studies
The primary inclusion criterion for this systematic review was RCTs of interventions for management of persistent post-treatment fatigue of adult TC survivors. The target population was TC survivors aged ≥18 years, whose disease was of any histologic subtype and who had completed primary treatment (surgery with or without other treatment). In order to be eligible for inclusion, more than half the study population was required to consist of TC survivors, or a TC subgroup data analysis needed to be reported. Although studies on individuals with a history of pediatric TC were eligible for review, the majority of patients in included studies were required to be aged ≥18 years of age during the trial. There was no specific requirement relating to disease stage or disease status. Studies primarily focusing on TC patients around the time of TC treatment (e.g., first six months around first surgery or radioactive iodine treatment) or those focusing on preparation procedures for radioactive iodine treatment or scanning were not eligible for inclusion. Pharmacologic (including hormonal) or nonpharmacologic interventions were included. Trials were required to report at least one quantitative measure of fatigue in respective intervention and control arms, at one or more time points after randomization. Duplicate publications reporting the same outcome measurements in the same population at the same time point were excluded. Included studies were required to be reported in the English language, due to insufficient resources for translation.
Information sources and searches
In order to identify trials for this review, a librarian information specialist (J.Z.) developed detailed search strategies for each database searched, which were based on the search strategy developed for Ovid Medline, but revised appropriately for each database. The search strategy used a combination of controlled vocabulary and free-text terms for identifying randomized trials, including search terms for TC and fatigue. Details of the current Medline search strategy are provided in the Appendix. The following electronic databases were searched: Medline (Ovid) 1946 to June Week 1 2014, MEDLINE In-Process & Other Non-Indexed Citations (Ovid) June 11, 2014, Embase (Ovid), 1974 to 2014 June 11, PsycINFO (Ovid) 1806 to June Week 1 2014, Cochrane Central Register of Controlled Trials (Ovid) to May 2014, and CINAHL (EBSCO) 1980 to May 2014. The hand search consisted of the screening of potentially relevant review articles, clinical practice guidelines, or original studies by one reviewer (J.T.), after considering advice from co-author content experts (A.M.S., J.J.). Duplicate citations among various searches were manually removed, in order to identify unique citations.
Study selection
Two team members (J.T. and A.M.S.) independently reviewed the citations retrieved from electronic searches for relevance, as well as any full-text studies deemed relevant by either reviewer from either the citation review phase or hand searching. In the case of duplicate publications on overlapping study populations, the larger or more recent study reporting data on the outcome of interest in the population of interest were preferentially included. A kappa statistic was calculated for estimation of agreement between reviewers on the following: (a) results of independent screening of citations, and (b) full-text review for inclusion in the study (using Confidence Interval Analysis Software, v2.2.0, T.N. Bryant, PhD, of the University of Southampton) (17). Consensus was achieved between reviewers on the final inclusion of full-text studies. In the event of difficulties achieving consensus, a third reviewer was available to resolve conflicts, if needed (J.L.).
Data abstraction, critical appraisal of included studies, and reporting of results
The flow of information through various phases of the review process was summarized in a PRISMA flowchart (18). Critical appraisal of studies and data abstraction were independently performed by two reviewers (A.S.G. and A.M.S.), using standardized abstraction forms. The Cochrane Risk of Bias Tool (19) was used to appraise quality of studies. Each abstracted data set was checked (by the other reviewer), and a final consensus data set was created after detailed discussion. Abstracted data, including relevant themes, were summarized in tabular and narrative form within the manuscript. It was anticipated, given the paucity of data in this field noted in the recent scoping review (4), that the data would not be amenable to a pooled meta-analysis, but the feasibility of a pooled analysis was re-evaluated upon completion of the data abstraction. For statistical comparisons performed in the primary studies, a p-value of <0.05 was assumed to be statistically significant.
Results
The flow of information through various phases of the review process is shown in Figure 1. In summary, 1086 unique citations were screened and 25 unique full-text articles were reviewed independently by two reviewers for consideration of inclusion (20 –45). There were four studies included in this systematic review (20 –23), although two of the studies (22,23) reported different fatigue outcomes from the same study population and are considered one RCT (as confirmed via e-mail correspondence with the primary author). The kappa statistic for agreement at the citation review stage (N=1086) was 0.665 [confidence intervals (CI) 0.287, 1.044] and at the full-text review stage was 1.000 [1.000, 1.000] (i.e., complete agreement at full-text review stage). Of the 21 full-text studies that were reviewed but excluded, the reason for exclusion was: primary population focus not TC (21 studies) (25 –36,39 –43), no measure of fatigue (two studies) (37,38), not a RCT (one study) (44), and overlap of an included study (one study) (24).
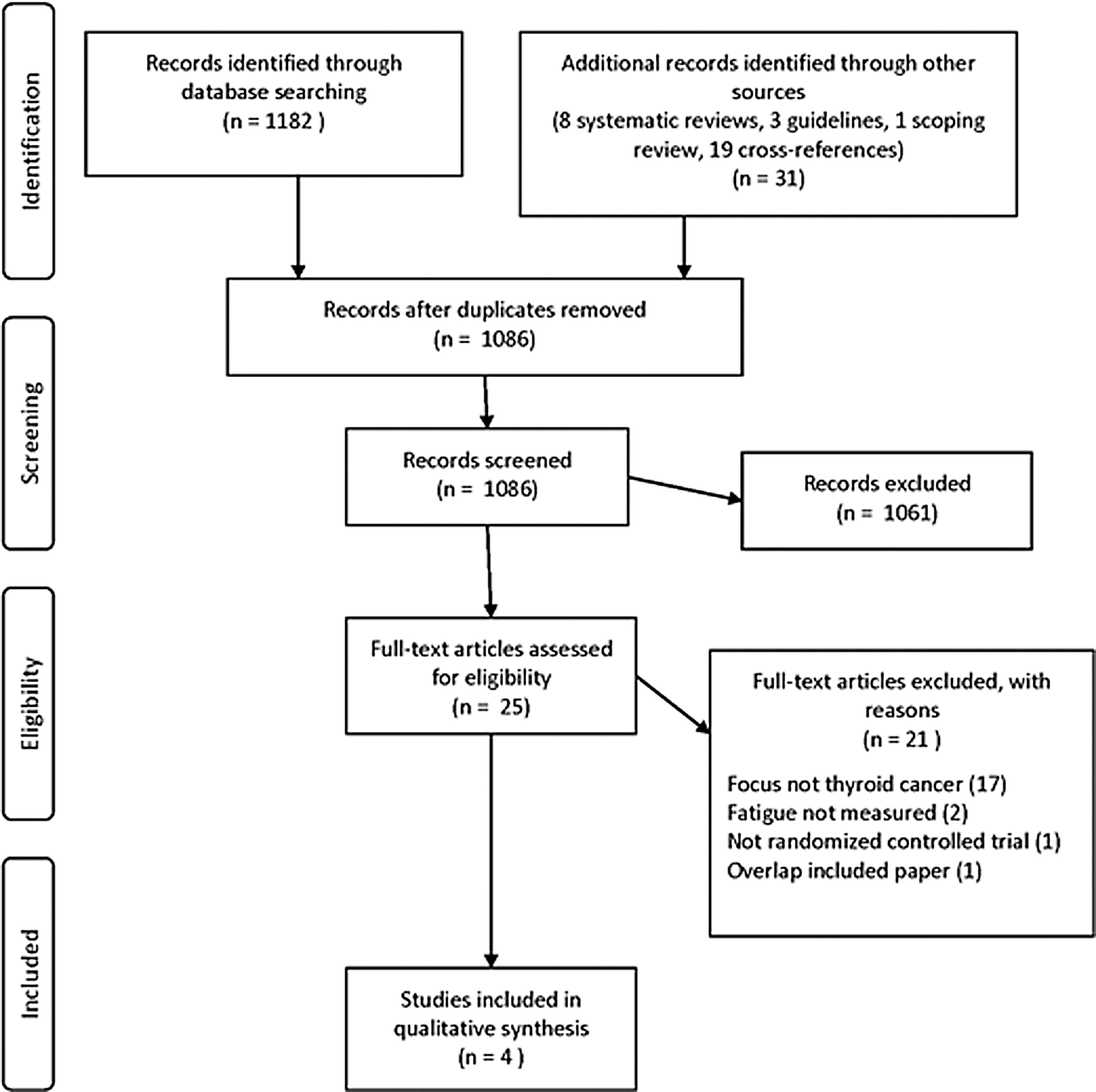
Summary of the process of study selection for this systematic review.
A description of the included RCTs is shown in Tables 1 and 2. The included trials were respective single-center studies, conducted respectively in European countries (20,21) or South America (22,23). In all included trials, the study populations were comprised of disease-free TC survivors on thyrotropin (TSH) suppressive therapy, a mean or median of more than five years since diagnosis (20 –23). The interventions studied include: combination triiodothyronine (T3) with levothyroxine (L-T4) therapy (i.e., combination T3/T4 therapy) compared to L-T4 alone (one RCT) (20), reduction in degree of TSH suppression using L-T4 (euthyroid L-T4) compared to maintenance of TSH suppression (one RCT) (21), and supervised exercise compared to inactivity (two studies examining different fatigue outcomes in same population, considered as one RCT) (22,23). The duration of interventions ranged from five weeks (2) to six months (21). One of the included trials reported a TC subgroup analysis from a larger trial of combination T3/L-T4 therapy, in which individuals with chronic autoimmune thyroid disease had also been recruited (20,24). One trial recruited only women (20), whereas the others recruited women and men, with women representing the majority of participants (21 –23).
SD, standard deviation; L-T4, levothyroxine; TSH, thyrotropin; SEM, standard error of the mean; RAI, radioactive iodine; IQR, interquartile range; fT4, free thyroxine.
This is a cross-over design randomized controlled trial, so each patient participated in each respective arm of the study and served as his or her own control.
†No reference for any prior validation data cited by the original authors for this scale.
‡Two studies reported respective different fatigue outcomes for the same trial population, so abstracted together.
T3, triiodothyronine.
Information on surgical histology, disease stage at diagnosis, and TC treatments were variably reported among trials (Table 1). A history of total thyroidectomy was reported in all participants in two trials (20,21), whereas surgical extent was not described in another trial (22,23). One trial specifically reported that all patients had undergone radioactive iodine remnant ablation (21), whereas this was not clearly reported but might be inferred in another trial, given that an inclusion criterion was a negative radioactive iodine scan (22,23); the radioactive iodine treatment history was not described in a third trial (20). Pretrial TSH measurements were below the reference range in all included studies (20 –23). Individuals with significant comorbidities were not allowed to participate in any of the included trials (20 –23). The percentage of randomized TC participants for which end-of-trial fatigue data were reported and analyzed ranged from 82.8% (24/29) (21) to 100% (36/36) (22).
The critical appraisal of included RCTs using the Cochrane Risk of Bias tool is summarized in Table 3. In summary, there were some limitations in reporting of the methods of all the trials, leaving some uncertainty in the assessment of various bias criteria (Table 3). The combination T3/L-T4 therapy trial (20) and the trial of restoration of euthyroidism (21) were blinded, whereas the exercise trial was unblinded, without clearly reported blinding of outcome assessors (i.e., research personnel calculating fatigue measure scores) (22). One trial was cross-over in design (20), such that participants were exposed to both treatment arms of the study. The final analyzed sample size of all of the trials was relatively small, ranging from 15 (20) to 36 (22,23) TC survivors, and none of the trials reported sample size justification in their methods. All trials lacked comprehensive reporting of adverse event details, but the authors of the combination T3/L-T4 therapy trial suggested that “side effects tended to be less after T4 plus T3 than after T4 alone” (20), and the authors of an exercise trial reported that no joint or muscle or other disease complications were noted in the exercise group (23). All of the trials excluded individuals with other significant comorbidities. None of the included trials was reported to be directly funded by industry, although T3 and L-T4 tablets were supplied by industry in one trial (20). Detailed compliance assessments were not reported in any of the trials, although the authors of the combination therapy trial indicated that patients reported taking their pills as directed (20).
Reference (19).
Quality appraisal category: Y, yes; U, unclear (e.g., reporting unclear); N, no.
Fatigue was a primary outcome in the exercise trial (22,23), but it appeared to be a secondary outcome in the other trials (20,21); fatigue was assessed by questionnaires in all trials (20 –23). In a trial of combination T3/L-T4 therapy compared to L-T4 alone (20), TSH suppression was maintained in both groups, and there were mixed results in fatigue outcomes (Table 2). For example, in this trial (20), in the Profile of Moods States questionnaire data (45), there was a significant improvement in the Fatigue-Inertia subscale (p=0.006) in the combination therapy group compared to the L-T4 group, but there was no significant difference in the Vigour-activity subscale of the same questionnaire and there was no significant difference in tiredness on a visual analogue scale (p>0.05). In a trial of euthyroid restoration (i.e., relaxation of TSH suppression by reduction in L-T4 dose) (21), the post-trial TSH (median 2.66 mIU/L) was significantly higher than in the control arm (median 0.012 mIU/L; p<0.001). In this trial, only one out of five subscales of the Multi-dimensional Fatigue Index-20 questionnaire (46) (i.e., the Reduced Motivation Subscale) was reported to be significantly better in the restoration of euthyroidism group compared to continued TSH suppression (p=0.003), with no significant between group difference for the other subscales (p>0.05). In the exercise trial (22,23), all three fatigue measures, including the Chalder Fatigue Scale (47), the Vitality domain of the Short Form-36 (SF-36) questionnaire (48), and the Qualification of Fatigue scale, were reported to significantly improve compared to baseline after 12 weeks of exercise training (p<0.05), but the between group difference was reported only for the Vitality domain of the SF-36, and it was significantly superior in the exercise group (p<0.05).
Discussion
Persistent post-treatment fatigue in cancer survivors (also referred to as cancer-related fatigue) includes physical, mental, and psychological components and is associated with impairments in activities of daily living, social functioning, paid work capacity, and finances (49). Fatigue is the most distressing side effect of malignancy, and it interferes with daily life (49 –53). Persistent post-treatment fatigue is a relatively common complaint among TC survivors (4). Despite the high prevalence of this problem, in this systematic review, only four studies (20 –23) were identified summarizing three RCTs of interventions for management of fatigue, specifically in TC survivors. All of the trials were relatively small and had some methodological limitations. Furthermore, it is not clear that these studies were adequately powered to address whether they could significantly improve fatigue in this population.
In this review, mixed fatigue outcome results were found reported in a trial of combination T3/L-T4 therapy in a subgroup of TC survivors (20). Of note, in a prospective observational study in which 20 differentiated TC survivors who were on a stable L-T4 dose were treated with at least six months of LT-4/T3 combination therapy, six patients (30%) preferred the combination therapy as they reported feeling “more energized and simply felt better” (54). However, this study was nonrandomized, unblinded, and the authors reported no data on objective measures of fatigue, but instead a broad explanatory statement without any report of formal qualitative analysis of patient perceptions (54). In T3/L-T4 combination RCTs largely conducted in autoimmune thyroid disease, there is conflicting evidence of benefit in thyroid-related symptoms, psychological outcomes, and patient preferences, as compared to L-T4 therapy alone (55). Yet it is not clear whether it is appropriate to extrapolate data on efficacy of thyroid hormone therapies on fatigue outcomes in patients with autoimmune hypothyroidism to that of thyroidectomized TC survivors, particularly those on long-term TSH suppressive therapy. For example, Louwerens et al. reported that patients with autoimmune thyroid disease had significantly higher levels of fatigue compared to differentiated TC survivors, and the differences were not explained by biochemical thyroid hormone measurements (56). Furthermore, these authors reported a modest effect of the TSH receptor-Asp727Glu polymorphism in explaining fatigue in differentiated TC survivors, but not in individuals with autoimmune thyroid disease (56). Thus, the genetic characterization and etiology of fatigue in these respective disorders may be different. It is important to note that TC survivors with any significant comorbidities were excluded from the existing RCT on combination therapy, so the safety of this treatment approach in such cases is not established. It is clear that more research is needed to understand fully whether combination T3/T4 therapy is beneficial in improving persistent post-treatment fatigue in afflicted TC survivors, and which, if any, particular patients may benefit most from this approach. Optimization of dosing of combination therapy may also need to be established, ideally, using sustained release preparations, if they become readily available. Long-term outcome data are needed, particularly if the intention would be long-term treatment with combination therapy in lieu of L-T4 alone, for management of persistent post-treatment fatigue in TC survivors.
The impact of the extent of TSH suppression on fatigue in differentiated TC survivors is a very important clinical consideration. TC clinical practice guidelines have evolved, currently recommending that the TSH be kept in the low normal range in low risk differentiated TC patients with no evidence of disease recurrence (57,58). Furthermore, the risks of TSH suppression may outweigh the benefits in some patients with significant comorbidities (59). Thus, the need to re-evaluate the utility of long-term TSH suppressive therapy in disease-free differentiated TC survivors clinically is established. In this context, L-T4 dose reduction is not uncommonly buffered by patients' fear of worsening of fatigue. It is noteworthy that in the reviewed RCT from Eustatia-Rutten et al. (21), there did not appear to be any adverse fatigue consequences associated with relaxation of TSH suppression, and perhaps some limited evidence for improvement in motivation. The fatigue benefits of restoration of euthyroidism after TSH suppression remain unproven, but existing blinded RCT data suggest fatigue may not necessarily worsen with this approach. Moreover, the relationship between thyroid hormone parameters (in the supraphysiologic or physiologic range) and fatigue in differentiated TC survivors is unclear (21,56). Clearly more research is needed to examine the impact of relaxation in the degree of chronic TSH suppression on fatigue and other outcomes in TC survivors.
In the only exercise RCT in TC survivors examining impact on fatigue, Vigario et al. reported that a supervised aerobic and stretching exercise program (twice weekly) significantly reduced fatigue compared to prescribed inactivity at 12 weeks (22,23). Exercise is a mainstay in recommended management of cancer-related fatigue in general oncology populations (60 –62). In meta-analyses of mostly short-term RCTs (i.e., typically 12–13 week outcomes) including mixed cancer survivors, physical activity significantly reduced cancer survivor post-treatment fatigue (63,64). However, most of this evidence was collected in breast cancer survivors, with none of the included trials focusing on TC (63,64). Long-term fatigue outcome data (i.e., measured at ≥12 months) have been reported from several cancer survivor physical activity trials (65 –70), yielding variable long-term sustainability of exercise participation in the intervention groups, and some uncertainty in long-term fatigue benefit. TC survivors on TSH suppressive therapy may face particular challenges with prolonged vigorous physical activity, given reported impairments in muscle bulk (assessed by mid-thigh girth) (22) and aerobic exercise performance (71 –73), compared to their euthyroid controls. Reported aerobic impairments in TC survivors on TSH suppressive therapy include: reduced peak aerobic exercise oxygen consumption (71,73), reduced exercise endurance (71,73), depressed anaerobic threshold (71,73), and slower heart rate and blood pressure recovery following physical activity (66), compared to euthyroid controls. Exercise impairments may be attenuated in younger DTC survivors with shorter duration of TSH suppressive therapy (74). Submaximal exercise responses may not be impaired in TC survivors (72), potentially suggesting that moderate physical activity may be better tolerated by some individuals. Yet little is known about the optimal type, intensity, or amount of exercise that is required to reduce the likelihood or severity of fatigue in TC survivors. As with general oncology populations, there is little known about ways to enhance long-term physical activity compliance or durability of fatigue benefit in TC survivors effectively. Furthermore, the effectiveness, feasibility, and affordability of individually supervised exercise programs compared to home- or community-based programs need to be considered.
Some strengths of this study include utilization of a systematic electronic search strategy developed by a library information specialist, duplicate independent review of citations and studies, and duplicate independent data abstraction and quality appraisal of included articles. A limitation of this study is not specifically searching for quality of life as an outcome in the electronic search strategy, although a recent systematic review of quality of life in TC survivors (13) and related cross-references had already been very recently screened as part of a preceding scoping review (4). Another limitation of this review is that it was restricted to RCTs, but in a recent scoping review (including observational studies) (4), it was found that the observational research in this area is largely focused on epidemiology and explanatory factors.
In summary, prospective observational and long-term outcome RCTs in the management of persistent post-treatment fatigue of TC survivors are needed. In the absence of such trials, it is reasonable for TC specialists to work with primary care physicians in excluding alternative treatable causes of fatigue and optimize thyroid function studies in keeping with current clinical practice recommendations on TC disease management (57,58). Yet this initial approach may not be sufficient for all patients. Consideration of current fatigue management guidelines outside of the direct area of TC is reasonable (60 –62), but indirect evidence from other populations, particularly those not treated with TSH suppression therapy (if applicable), should be interpreted with caution, and the relevant characteristics of each case need to be taken into account. There is currently insufficient evidence to routinely recommend the use of combination T3/L-T4 therapy or other nonstandard thyroid hormone treatments in this situation with the promise of significantly improving fatigue, but it is the hope of the authors that further high quality, long-term outcome research may better inform future clinical practice in that regard.
Footnotes
Acknowledgments
This work was funded in part by a University of Toronto Department of Medicine Strategic Innovation Fund Grant. A summer co-op research internship for J.T. was funded by the University Health Network Cancer Survivorship Program. A.S. currently holds a Chair in Health Services Research from Cancer Care Ontario, funded by the Ontario Ministry of Health and Long-term Care. The authors would like to thank A. Naeem and C. Marino for assistance retrieving some of the original articles for review and general administrative assistance.
Author Disclosure Statement
The authors have no competing interests to disclose relating to this manuscript.