
Abstract
Background:
Voice changes commonly occur from thyroidectomy and may be due to neural or nonneural causes. Such changes can be a source of significant morbidity for any patient, but thyroidectomy in the professional singer carries special significance. We test the hypothesis that the career of singers and professional voice users is not impaired after neural monitored thyroid surgery.
Methods:
A quantitative analysis of pre- and postoperative neural monitored thyroid surgery voice outcomes utilizing three validated vocal instruments—Voice Handicap Index (VHI), Singing Voice Handicap Index (SVHI), and Evaluation of Ability to Sing Easily (EASE)—in a unique series of professional singers/voice users was performed. Additional quantitative analysis related to final intraoperative electromyography (EMG) amplitude, the time to return to performance, and vocal parameters affected during this interval was performed.
Results:
Twenty-seven vocal professionals undergoing thyroidectomy were identified, of whom 60% had surgery for thyroid cancer. Pre- and postsurgery flexible fiberoptic laryngeal exams were normal in all patients. Return to performance rate was 100%, and mean time to performance was 2.26 months (±1.61). All three vocal instrument mean scores, pre-op vs. post-op, were unchanged: VHI, 4.15 (±5.22) vs. 4.04 (±3.85), p=0.9301; SVHI, 11.26 (±14.41) vs.12.07 (±13.09), p=0.8297; and EASE, 6.19 (±9.19) vs. 6.00 (±7.72), p=0.9348. The vocal parameters most affected from surgery until first performances were vocal fatigue (89%), high range (89%), pitch control and modulation (74%), and strength (81%). Final mean intraoperative EMG amplitude was within normal limits for intraoperative stimulation and had no relationship with time to first professional performance (p=0.7199).
Conclusions:
Neural monitored thyroidectomy, including for thyroid malignancy, in professional voice users is safe without any changes in three different voice/singing instruments, with 100% return to performance. Intraoperative EMG data at the conclusion of surgery and postoperative laryngeal exam were normal in all patients. Specific vocal parameters are transiently affected during the postoperative recovery phase, which is important to outline in the consent process of this unique patient population and may provide insight into the physiologic state of the larynx subsequent to thyroid surgery.
Introduction
T
Several recent surveys suggest that a majority of surgeons in the United States are currently employing intraoperative neural monitoring (IONM), with rates of use of 53% among general surgeons and up to 65% amongst otolaryngologists (3,4). In addition, unpublished 2015 American Thyroid Association (ATA) Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer prepared by Haugen et al. state that intraoperative neural stimulation (with or without monitoring) may be used to facilitate nerve identification and confirm neural function. These ATA 2015 guidelines also recommend that voice assessment and laryngeal exam at thyroidectomy be performed in accordance with the recently published AAO-HNS guidelines (1). The American Head and Neck Society Invasive Thyroid Cancer guidelines also recommend preoperative laryngeal exam in all patients with thyroid cancer (5).
While there are many studies in the literature reporting on subjective and objective voice recovery after thyroid surgery, this paper is the first to report on consecutive patients who are professional singers and professional voice users undergoing neural monitored thyroid surgery, utilizing established vocal instruments and targeted questions on pertinent vocal parameters.
Materials and Methods
Internal review board approval was obtained prior to study commencement. A prospective database of professional singers and professional voice users undergoing thyroid surgery by a single surgeon (GWR) at our institution was maintained from August 2002 to March 2014. The key element for enrolment was that the patient was considered a “voice professional” in that voice was specifically and significantly involved in the patient's profession. IONM was performed in all surgeries in compliance with the International Neural Monitoring Study Group Guidelines for recurrent laryngeal nerve (RLN) and external branch of superior laryngeal nerve (EBSLN) monitoring and involved general anesthesia and monitoring with endotracheal tube intubation (1,6,7). This included repetitive vagal, RLN, and EBSLN stimulation at 1 to 2 mA during surgery. All patients were intubated with number 7 or 8 endotracheal tubes; no attempt was made to undersize the endotracheal tube. Pre- and postoperative laryngeal assessment was achieved with office fiberoptic exam in all patients, in compliance with AAO-HNS and American Head and Neck Society Guidelines (1,5). Preoperative evaluation was typically performed by fiberoptic office laryngeal exam within 1–2 weeks prior to surgery. Time to postoperative survey evaluation varied but was typically performed several months after surgery.
Surveys were used to collect pre- and postoperative patient responses to predetermined vocal instruments: Voice Handicap Index (VHI), Singing Voice Handicap Index (SVHI) and Evaluation of the Ability to Sing Easily (EASE). p-Values were calculated using Fishers' exact test. Additional questions relating to the time to return to performance, vocal factors affected, and vocal training during the postoperative period were documented. These factors were generated by the authors of this study based on analysis of existing vocal instruments including the ones used in this study (VHI, SVHI, and EASE) and were selected as likely important to the professional singers peri-operatively. Data was collected on the use of vocal training in the recovery phase, including the extent to which vocal training was used. Analysis of degree of vocal training and time to first performance was performed using one-way analysis of variance testing. Analysis of mean RLN final intraoperative monitoring EMG amplitude and relationship to time to return to performance was performed using linear regression analysis. Statistical analysis was performed in Excel and GraphPad Prism (GraphPad Software, Inc., San Diego, CA).
Results
Twenty-seven professional voice users undergoing thyroid surgery during the study period participated in data collection. The average age was 44.8 years (range 17–76 years). Ten subjects were male and 17 female. Surgical pathology was malignant in 17 (61%) and benign in 10 patients (39%). Twelve of seventeen (70%) patients with malignancy received radioactive iodine treatment. All patients had visual identification and effective IONM neural stimulation of all EBSLNs and all RLNs at risk with EMG recording. All patients had normal laryngoscopic examinations before and after surgery.
The number (proportion) of patients in each genre of performance was as follows: classical/operatic, 12/27 (44%); religious (including 1 gospel, 1 Jewish cantor, and 3 choir), 5/27 (19%); pop/rock, 7/27 (25%); country and blues/folk, 3/27 (11%); Motown, 1/27 (4%); Broadway/musical theatre, 2/27 (7%); music teachers, 2/27 (7%); and other (1 voice over artist and 1 television meteorologist), 2/27 (7%). Some patients indicated multiple genres of performance (Fig. 1).

Percentages of different genres of singers in our study (some patients indicated multiple genres of performance).
One hundred percent of patients returned to full professional performance, with their first postoperative performance occurring with a mean time of 2.26 months from surgery (range 0.5–8 months). We define this period—the time from surgery to first postoperative professional voice performance—as the “recovery phase.” During this recovery phase, all patients had normal speaking voice and normal laryngoscopic examination. Vocal parameters affected during the recovery phase were vocal fatigue (89%), vocal strength (81%), high range (89%), low range (22%), pitch control and modulation (74%), projection (55%), and amplitude (52%) (Fig. 2).
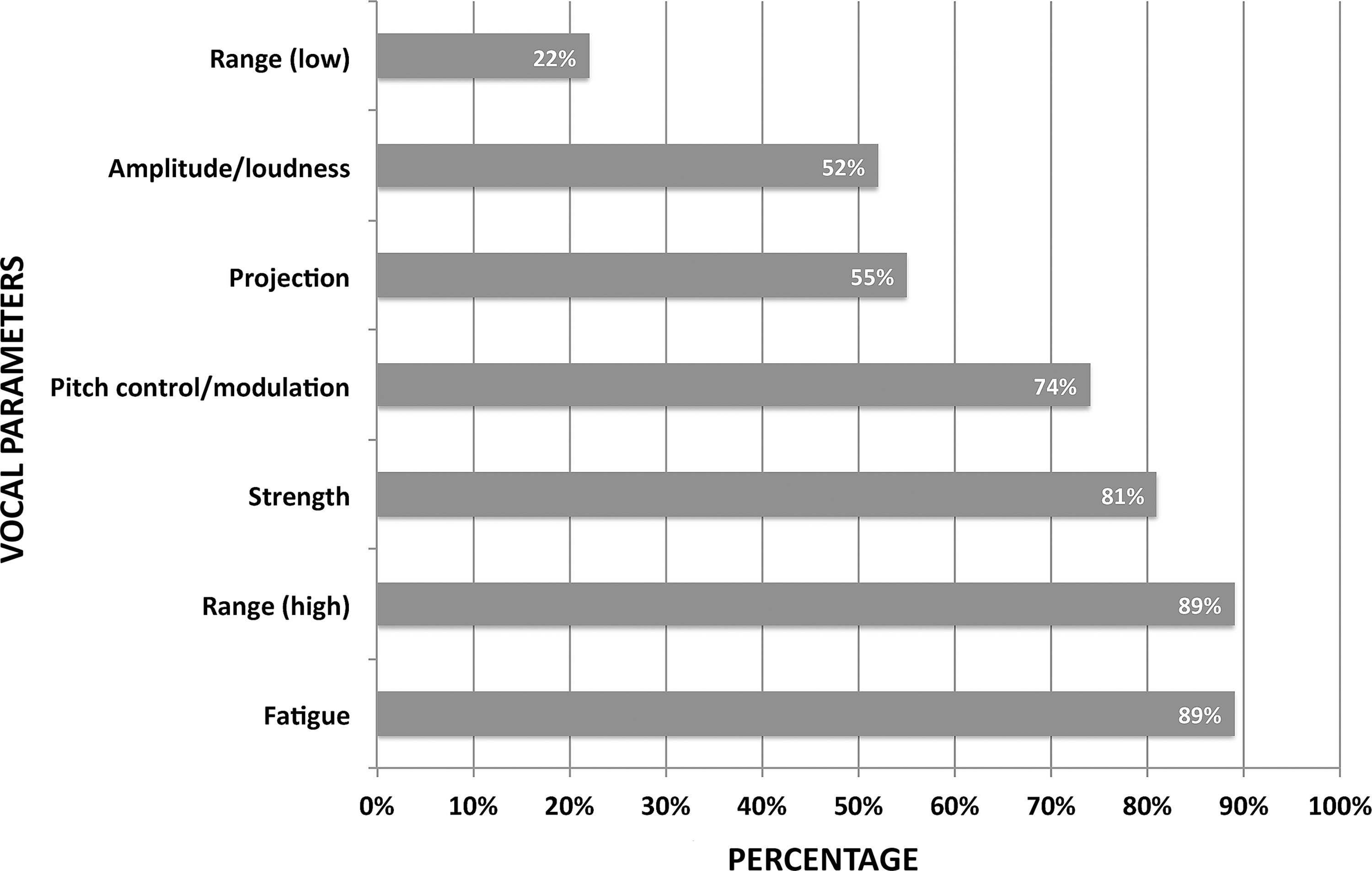
Different transient vocal deficiencies and their occurrence in our series.
Most vocal professionals utilized vocal training to some extent (67%) during the recovery phase. The breakdown of vocal training utilization by the group was none, 9/27 (33%); some, 11/27 (41%); and intense, 7/27 (26%). Among the patients employing vocal training during the recovery phase, 17/18 (94%) felt it was helpful in their return to professional vocal performance. Additional analysis was performed comparing vocal training intensity and the recovery phase duration. Vocal training was characterized as none, some (<3 days per week), or intense (daily vocal exercises). Mean data between these groups is illustrated in Figure 3. One-way analysis of variance testing between groups showed no statistical significance in return to performance time (p=0.3814).
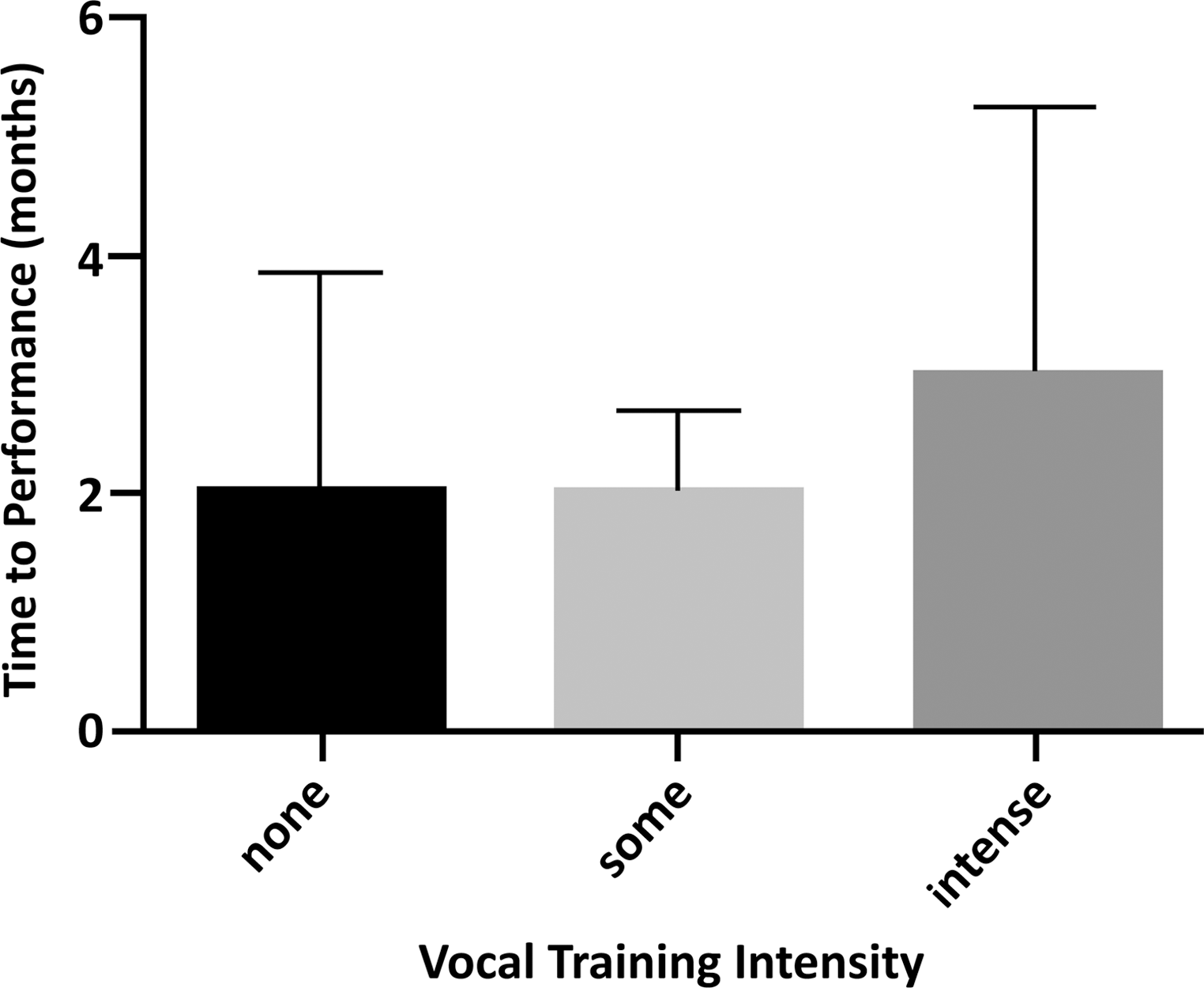
Training intensity and mean recovery time.
Although patients noted symptoms as described above during the initial postoperative period (i.e., while in their “recovery phase”), overall vocal instrument mean scores showed no statistically significant difference in pre-operative versus postoperative comparisons, indicative of successful vocal function preservation. Scores by vocal instrument (pre-op vs. post-op) were VHI (4.15 vs. 4.04, p=0.9301); SVHI (11.26 vs. 12.07, p=0.8297); and EASE (6.19 vs. 6.00, p=0.9348). The EASE instrument is further separated into a factor 1 subscale, capturing physical symptoms of vocal impairment and fatigue, and a factor 2 subscale that relates to mucosal issues such as edema or vocal fold pathology (8). Preoperative and postoperative EASE scores by factor were factor 1, 3.93 versus 2.85, p=0.4063, and factor 2, 2.63 versus 2.78, p=0.8648. The SVHI instrument categorizes responses into physical, functional, and emotional domains. Preoperative versus postoperative breakdown of scores was: physical, (4.63 vs. 5.22, p=0.6587); functional, (3.37 vs. 3.63, p=0.7985); and emotional, (3.26 vs. 3.22, p=0.9743).
All patients were adults and as mentioned earlier were intubated with number 7 or 8 endotracheal tubes with no intentions to undersize the endotracheal tube. There was no evidence of laryngeal trauma on postoperative laryngeal examination. Intraoperative EMG data was obtained in all patients. Final RLN EMG amplitude was within established normative ranges in all patients with a mean of 554.2 μV (range 200–1089 μV; SD=241.1 μV). This EMG data was analyzed relative to recovery time for patients and there was no relationship between mean final EMG amplitude and the time to first professional performance (p=0.7199).
Discussion
Thyroidectomy in the professional voice user carries significant risks to livelihood and earning capacity of patients and even has religious consequences in those engaged in religious vocal professions such as gospel/church singing and Jewish cantors. This study represents the only publication on vocal outcomes in a consecutive series of professional voice users undergoing thyroid surgery.
RLN injury rates
Intra-operative damage to the professional voice can result from neural etiologies like RLN and/or EBSLN injury as well as from non-neural etiologies (Table 1). Quoted rates of RLN paralysis are undoubtedly underestimates, coming from experienced head and neck endocrine centers, and are significantly affected by variable rates of postoperative laryngeal exams, which precludes extrapolation to lower-volume practice settings in which the majority of thyroid surgery is performed. The Scandinavian Quality Register reported a RLN paralysis rate of 4.3% with a 45% rate of postoperative laryngeal examination (9). The third BAETS Audit reported a 2.5% RLN paralysis rate with only 21.5% of patients receiving a postoperative laryngeal exam, but the BAETS RLN paralysis rate rose to 4.5% when a majority of the surgical population had routine laryngeal exams (10). Subjective evaluation of the voice by the surgeon and patient underestimates the incidence of RLN paralysis, which can be masked by postoperative glottic edema, contralateral vocal cord compensation, and in some, paresis states. Several data sources suggest that if laryngoscopy is performed routinely in a given thyroidectomy population, the rate of VCP is double the rate seen in a population examined only on the basis of vocal symptoms. A recent systematic review of 25,000 patients, all receiving postoperative laryngeal exam, showed a 9.8% rate of VCP, ranging from 2.3% to 26% (2). The importance of postoperative laryngeal exam in the professional voice user is paramount to excluding RLN paralysis reliably, to informing regarding EBSLN injury, and to excluding laryngeal injury from intubation. There is evidence that intervention within 3 months of neural injury significantly improves long-term outcomes, and this may be critical to the long-term employment prospects and earning capacity of the professional and nonprofessional voice user (1,11,12).
EBSLN, external branch of superior laryngeal nerve; RLN, recurrent laryngeal nerve; URTI, upper respiratory tract infection; VC, vocal cord; VCP, vocal cord paralysis.
The quality of life and health care costs associated with VCP are of heightened magnitude in the professional singer. VCP health care costs arise from repeated office visits and laryngoscopic assessments, voice laboratory evaluation, voice therapy, and rehabilitative interventions including injection laryngoplasty, reinnervation procedures, and formal thyroplasty (1). To the American economy, direct costs of assessing and managing laryngeal disorders is between $179 and $295 million annually (1,13). The potential for anxiety, adverse quality of life impact, diminished earning capacity, and loss of employment for the professional voice user undergoing thyroid surgery is significant.
Monitoring of the EBSLN: 100% identification
The EBSLN is of critical importance in the professional singer, and the rate of injury can approach 58% (14 –16). The EBSLN innervates the cricothyroid muscle, causing vocal fold lengthening and tensing important in vocal projection and the higher registers of the voice—crucial elements to the professional voice. The EBSLN has been called the “nerve of Amelita Galli-Curci,” in reference to the famous 20th century operatic soprano whose voice was purportedly damaged irrevocably by EBSLN injury during thyroid surgery under local anesthesia (17,18). There is a paucity of information regarding cricothyroid muscle dysfunction after thyroidectomy. The real rate of EBSLN injury is not known because of the difficulty in diagnosing EBSLN paralysis on the glottis exam—we feel these injuries are infrequently thoroughly evaluated. EBSLN injury in a professional singer would be disastrous.
In the operative field, the EBSLN approaches the larynx in a space defined as the sternothyroid laryngeal triangle, also known as Joll's space, and it is at risk during superior pole management (Fig. 4). Recently it has been reported that the laryngeal head of the sternothyroid muscle represents a reliable anatomic landmark for the EBSLN (18,19). Visual identification of the EBSLN may not be possible in up to 20% of individuals, where the nerve is typically located deep to the fascia of the inferior constrictor muscle (20). In this context, electrophysiologic monitoring can facilitate quantifiable EMG response from the EBSLN in 100% of patients (21). This represents an advantage of neural monitoring, especially in the professional singer group, because visual identification is only possible in at most 80% of individuals, given the 20% of EBSLNs with a subfascial course. While laryngoscopic findings associated with EBSLN injury can be subtle and easily overlooked, reported findings can include posterior glottic rotation, inferior vocal cord positioning, and bowing on the paralyzed side (15,16). Given the variable and subtle fiberoptic findings on glottis exam in EBSLN paresis/paralysis, cricothyroid muscle EMG remains the gold standard in the diagnosis of EBSLN injury.
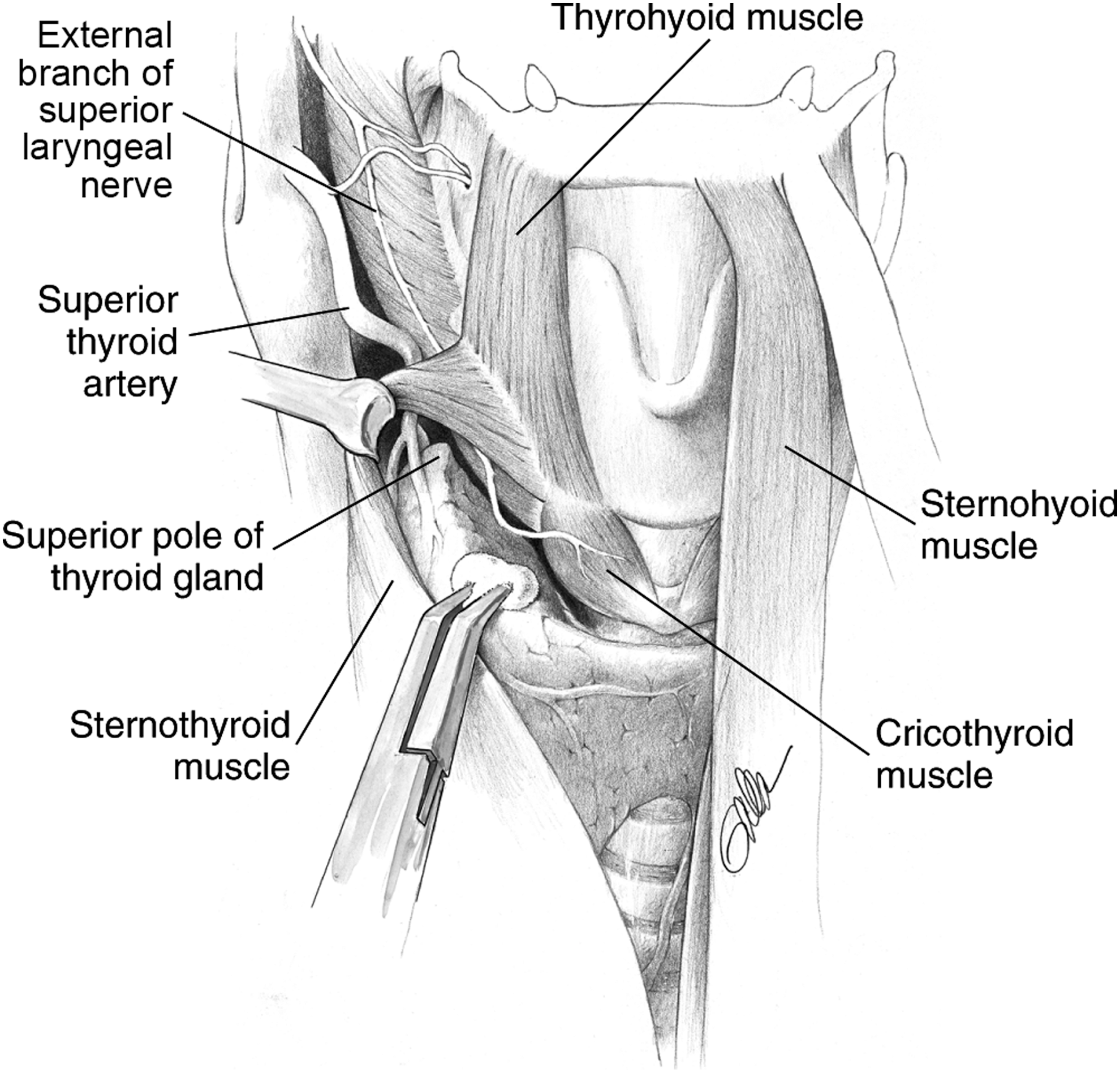
The external branch of the superior laryngeal nerve descends dorsolaterally to the internal and external carotids and then medially to enter the larynx. Reproduced with permission from Randolph GW, ed. 2013 Surgery of the Thyroid and Parathyroid Glands. Second edition. Elsevier Inc., Philadelphia, PA.
Voice changes: differential diagnosis
Voice changes are also a common occurrence in patients who demonstrate intact vocal cord mobility on laryngeal exam post thyroidectomy. Our patients described transient voice changes during their recovery phase prior to their initial performance despite having no significant changes in their preoperative versus postoperative voice indices, overall. The nonneural factors related to postoperative voice change are listed in Table 1. Several large studies have reported subjective voice complaints in 30% to 87% in patients without neural injury (22 –27). Previous studies analyzing the objective phonoacoustic changes post thyroidectomy have reported reduced fundamental frequency, diminished vocal range, decreased maximum sound pressure and increased vocal jitter in over 80% patients tested (28 –30). For the professional voice user, the recovery phase is characterized by a range of transient vocal deficiencies, in our series, most commonly including vocal fatigue (89%), reduced vocal strength (81%), loss of high registers (89%), reduced pitch control/modulation (74%), and reduced projection (55%) (Fig. 2). Given that all of our patients had normal intraoperative stimulation EMG characteristics of the EBSLN and RLN during surgery, and normal postoperative laryngeal exam (albeit with poor sensitivity for EBSLN dysfunction) with normal speaking voices during the recovery phase, we hypothesize that these recovery phase vocal parameters may, at least in part, be referable to cricothyroid muscle myositis, which we believe may have led to the observed set of symptoms in the early postoperative period. The cricothyroid muscle, which is exceedingly thin with limited fascial covering, sits on the external larynx, directly in the operative field and is in direct contact with normal postoperative inflammatory seromatous elements in the postoperative wound. Currently there is no direct evidence to support this, although it is noted in the AAO guidelines as a possible source of voice change postoperatively after thyroid surgery (1). Our group is currently exploring this cricothyroid muscle myositis hypothesis in a porcine model.
Laryngeal dysfunction after any head and neck surgery requiring intubation is common, and often is from nonneural complications. Postoperative laryngeal dysfunction may be present in 6% to 70% in all surgeries requiring endotracheal intubation. Many of these problems such as glottic edema, cord lacerations, hemorrhage, granuloma, and vocal cord ulceration suggest direct trauma to the internal larynx related to intubation and tube position, unrelated to thyroidectomy and nerve trauma (31). One potential advantage of IONM may be the surgeon's ability to maintain awareness of the position of the endotracheal tube (ETT) within the larynx. A shift in ETT position will alert the surgeon through alteration of the EMG signal, who can then reposition the ETT reducing the chance of significant ETT motion/migration, or cuff trauma to the vocal cords.
The mean time of return to professional vocal performance of 2.26 months from our study provides data to the patient and surgeon in monitoring vocal recovery post thyroidectomy and in providing expectations of time to return to professional performance subsequent to surgery, assuming no neural injury state exists. We found that it was our patients' perception that postoperative vocal training was very helpful in the recovery phase.
Capturing the spectrum of postoperative vocal recovery in professional singers is challenging. No ideal vocal instrument exists specifically for this group of patients. The VHI lacks particular relevance to singers, while the SVHI—though validated and targeted to singers—assumes a “diseased” voice. The EASE vocal instrument is perhaps the most potent tool, and uses a “healthy framework” without a presumption of disease (8). There is currently no accepted battery of voice instruments routinely applied to the professional singer undergoing thyroid surgery. We appreciate one of the limitations of our study is that EASE only recently became available and could only be applied to the more recent cohort of patients in our study. We feel utilization of all of these vocal instruments was beneficial in accurately generating a broad picture of professional voice recovery after thyroidectomy. The variable timeframe to postoperative survey evaluation is a weak point of our study but was necessitated by busy schedules of our patients and the long time frame over which our study population was necessarily drawn.
Key elements of operative approach in the professional singer
Numerous aspects of the operative approach to thyroid surgery in the professional singer warrant highlighting, and we feel underpin the successful preservation of vocal integrity in the professional voice user.
• Laryngeal exam. Postoperatively, the findings of fiberoptic laryngoscopy are the basic essential data set of laryngeal management.
• IONM. Intraoperatively, nerve monitoring provides invaluable functional information during thyroid surgery, with the knowledge that visually intact nerves do not equate with functionality, allows neural mapping and rapid and direct identification of the RLN and EBSLN course bilaterally in all patients. The study represents an analysis of a small group of patients operated by a single surgeon all of whom had surgery with neural monitoring, we therefore cannot comment that monitoring per se was the sole factor in our outcomes.
• Predictive quality of normative intraoperative EMG. This study is the first to report on the correlation of normal evoked postdissection EMG amplitudes with return to performance time in a series of professional voice users; full return to professional performance was associated with intraoperative EMG within the normative published ranges in all professional voice patients. Other studies have reported postdissection EMG amplitudes as a reliable positive predictor of intact vocal cord function (32 –34).
• Strap muscle and cricothyroid muscle management. Our preference in singers is to avoid strap muscle division including limited strap muscles incision of the laryngeal head of the sternothyroid muscle. While there is limited evidence on the effect of strap muscle division on vocal outcomes, preservation of extralaryngeal muscular integrity may benefit the professional singer by limiting perilaryngeal tissue denervation and global scarring (35,36).
• EBSLN monitoring. In a recent series, Darr et al. showed EBSLN endotracheal tube EMG activity is successfully measurable in 100% of patients (21). Monitoring therefore provides substantially improved EBSLN identification beyond what is available through visual inspection alone (which is at most 80%, given the subfascial course of the EBSLN in 20% of patients), a very significant advantage in professional singers.
Conclusion
Neural monitored thyroid surgery in professional voice users is safe and vocal performance is not impaired. Adherence to IONM Study Group guidelines and pre- and postoperative laryngeal assessment in compliance with the AAO-HNS voice guidelines complements specific intraoperative surgical techniques to maximize vocal integrity (1,6). In our series of singers and professional voice users return to performance occurred in 100% and there was a recovery phase of 2.26 months before performance status was reached, which has an application in preoperative counselling in this subgroup of patients.
Footnotes
Acknowledgments
This work was funded by the John and Claire Bertucci Thyroid Research Fund.
Author Disclosure Statement
No competing financial interests exist for any of the authors.