
Abstract
Background:
Papillary thyroid carcinoma (PTC) has an excellent prognosis. Although rare, PTC invasion into the upper aerodigestive tract can adversely affect patient prognosis and quality of life. This study investigated the impact of tumor excision on the prognosis and postoperative status of patients with PTC invasion of the larynx.
Methods:
Data on PTC patients who underwent surgery at the author's institution between April 1981 and March 2010 were retrospectively reviewed, and 55 patients with thyroid cartilage invasion were enrolled. Curative resection was performed for all patients, and laryngeal function was preserved or reconstructed when possible.
Results:
Of the 55 patients, 40 and 15 patients had superficial and intraluminal invasion of the larynx, respectively. The 10-year disease-specific survival rates were 81.0% and 61.4% in patients who underwent surgery for superficial and intraluminal invasion of the larynx, respectively. Only two patients (3.6%) had an isolated locoregional recurrence in the larynx. Four patients (7.3%) underwent total laryngectomy during the initial surgery or surgery for laryngeal recurrence. Permanent stoma remained in 26 patients (47%): 14 with laryngeal invasion, and 12 with invasion of other aerodigestive structures. The number of invaded aerodigestive structures including the larynx was correlated with the presence of permanent stoma.
Conclusions:
In many patients, PTC invasion of the larynx remained at the thyroid cartilage or paraglottic space. Most patients did not require total laryngectomy. Good locoregional control was achieved with surgical tumor excision in patients with laryngeal invasion. Distant metastases were the major cause of death in patients with PTC invasion of the larynx.
Introduction
P
The surgical management of locally advanced thyroid carcinoma includes complete tumor resection and functional preservation or reconstruction of surrounding structures. Although complete resection for intraluminal invasion into the aerodigestive tract is supported, controversy exists regarding the use of shave excision versus complete resection for tumors of the aerodigestive tract. Shave excision has been reported to be as effective as complete resection in terms of locoregional control and survival in thyroid carcinoma patients without direct intraluminal involvement of the aerodigestive tract (10 –13). Conversely, complete resection has been supported because of the higher recurrence rate and worse survival associated with shave excision (14 –18). Furthermore, although the use of radioactive iodine and external beam radiation therapy as postoperative adjuvant treatments for locally advanced thyroid cancer is generally accepted, their effectiveness against aerodigestive tract invasion has not been established (19 –23).
Comparisons of complete resection and shave excision for the treatment of PTC invasion of the aerodigestive tract have been reported, whereas the impact of tumor excision on functional outcomes and locoregional recurrence risk has been rarely reported. In this study, the effect of tumor excision on the prognosis and postoperative status of patients with PTC invasion of the larynx was investigated.
Materials and Methods
A retrospective chart review of PTC patients who underwent surgical treatment at Kyoto Medical Center and Kusatsu General Hospital between April 1981 and March 2010 was performed. Patients with PTC invasion of the larynx were enrolled. Cricoid cartilage, ring-like cartilage of the larynx, is involved in maintaining the laryngeal framework and plays a small role in laryngeal functions such as speaking and swallowing. Laryngeal function can be compromised by tumor invasion into the cricoarytenoid joint. Thus, it is believed that both cricoid cartilage and tracheal invasion can be identified based on laryngeal function. Data were collected on patients with thyroid cartilage invasion with or without cricoid cartilage invasion. The institutional review board approved this study. Patient confidentiality was maintained, and informed consent was obtained from all patients.
Computed tomography (CT) or magnetic resonance imaging (MRI) and endoscopic examination were used for preoperative evaluation. Intraluminal invasion of the larynx and trachea was evaluated by endoscopic examination. In cases with suspected esophageal invasion, gastrointestinal fiberscopy was performed preoperatively. Invasion of the inner thyroid cartilage lamina, paraglottic space, and lining of the larynx was evaluated by CT or MRI. Gross invasion and pathological angiogenesis of the larynx were evaluated by endoscopic examination. Preoperative examinations evaluated invasion depth from the thyroid cartilage to the laryngeal mucosa. Tumor invasion depth was classified into four types: invasion up to the inner thyroid cartilage, limited paraglottic space invasion, diffuse paraglottic space invasion, and intraluminal invasion.
Superficial invasion of the larynx was defined as laryngeal invasion up to the inner thyroid cartilage lamina or limited invasion of the paraglottic space by preoperative evaluation. The appropriate surgical method (shave excision or framework resection) for superficial invasion was selected based on the intraoperative findings or intraoperative cryosection analysis. Intraluminal invasion of the larynx was defined as invasion of the larynx lining or diffuse paraglottic space invasion by CT or MRI or gross invasion or pathological angiogenesis of the larynx by endoscopic examination. The appropriate surgical method for intraluminal invasion was selected based on the intraoperative gross findings or intraoperative pathological findings. PTC invasion into other organs was also examined.
Shave excision or framework resection were performed for superficial invasion of the larynx. Shave excision, which involves the sharp separation of the superficially invading tumor from the thyroid cartilage, was performed when tumor infiltration did not reach the inner thyroid cartilage lamina. Framework resection, which involves resection of the cartilage or limited paraglottic tissue penetrated by the tumor, was performed when tumor infiltration reached or extended into the inner thyroid cartilage lamina but remained in the paraglottic space. Partial laryngectomy, vertical hemilaryngectomy (VHL), subtotal laryngectomy, or total laryngectomy was performed for intraluminal invasion of the larynx. Subtotal laryngectomy, in which more than half of the larynx is resected, was performed to restore phonetic function in these patients. This procedure involves reconstruction of the larynx to ensure adequate size for voice production and to reduce aspiration risk.
Curative resection was defined as tumor resection margin negativity confirmed by intraoperative pathological diagnosis. Curative resection was performed for all PTC patients with invasive extrathyroidal extension, and laryngeal function was preserved or reconstructed when possible. Curative resection was performed with the aid of an operating microscope when necessary. An operating microscope was used for shave excisions of laryngo-tracheal cartilage, widespread muscle layer resection of the esophagus, and partial resection of the recurrent laryngeal nerve (RLN). Sharper images of organ structures can be obtained under a high-power field of a surgical microscope, thus allowing for more accurate tumor excision from the organ. During surgery, multiple margin samples were sent for frozen section analysis to confirm margin negativity pathologically. In patients with positive margins, additional resection was performed until a negative margin was achieved. Intraoperative cryosection analysis was done to preserve as much normal tissue adjacent to the tumor as possible and improve functional outcomes. Surgical management was adapted for laryngeal involvement.
Prognosis, locoregional recurrence rates, and postoperative status were examined in patients with laryngeal invasion. Postoperative status included the rate of closing of the tracheal stoma and time to return to normal diet intake. Closing of the tracheal stoma reflected the absence of airway stenosis and aspiration. Normal diet intake reflected adequate nutrition. For patients with intraluminal invasion of the larynx and/or esophagus, a nasogastric feeding tube was inserted for two weeks. Oral intake for patients with superficial invasion was initiated in the early postoperative period according to each patient's individual condition. Dysphagia rehabilitation was begun after video fluoroscopy in patients with intraluminal invasion and those with superficial invasion with inadequate oral intake as a result of aspiration.
The Mann–Whitney, chi-square, or Cochran–Armitage trend test was used to compare variables. Survival curves were constructed using the Kaplan–Meier method and compared using the log-rank test. A p-value of <0.05 was considered statistically significant. All statistical analyses were conducted using Ekuseru-Toukei 2012 software (SSRI Co. Ltd.).
Results
During the study period, 103 out of 803 PTC patients had laryngeal invasion. Of these, 55 patients (13 male; 23.6%) with thyroid cartilage invasion with or without cricoid cartilage invasion were enrolled, and 48 patients with cricoid or cricotracheal invasion without thyroid cartilage invasion were excluded. Laryngeal invasion by PTC was detected at the time of initial diagnosis in 29 patients and at the time of relapse in 26 patients. Of the 55 enrolled patients, 48 patients (83%) were referred from other institutions for their surgical treatment.
The mean age at the time of surgery for laryngeal invasion was 62 years (range 19–83 years). The follow-up duration after surgery for surviving patients was 7.4±5.5 years. None of the patients received radioactive iodine treatment for postoperative ablation of laryngeal invasion. Of 55 patients with laryngeal invasion, 14 patients (25%) had lung metastasis prior to laryngeal surgery. However, respiratory functions were not poor, and lung metastasis spread was not aggressive in these patients (Table 1).
Of 55 patients with thyroid cartilage invasion, 45 patients (82%) had tumor invasion into the cricoid cartilage.
SD, standard deviation.
Forty patients with superficial invasion underwent shave excision (n=6) or framework resection (n=34), and 15 patients with intraluminal invasion underwent endolaryngeal surgery. Of the 15 patients with intraluminal invasion, partial laryngectomy was performed in four patients, VHL in two patients, and subtotal laryngectomay in six patients. In our series, three patients (5.5%) underwent total laryngectomy for laryngeal invasion.
Eleven and seven patients had locoregional and distant recurrence, respectively. For locoregional recurrence, lesions were located on the upper aerodigestive tract in four patients, the larynx in two patients, the trachea in one patient, and the esophagus in one patient. Isolated locoregional recurrence in the larynx occurred in two patients (3.6%). These patients were managed with total laryngectomy and an additional framework resection. As a result, a total of four patients (7.3%) underwent total laryngectomy. Three patients who underwent total laryngectomy during the initial surgery were unsuitable for intubation because of massive intraluminal invasion of the larynx. Airway control was achieved by tracheostomy and laryngofissure surgery under local anesthesia and stratified mediastinal tracheotomy under a percutaneous cardiopulmonary support device.
The 10-year disease-specific survival rates were significantly shorter in patients who underwent surgery for intraluminal invasion of the larynx than for those who underwent surgery for superficial invasion of the larynx (61.4% vs. 81.0%; p=0.0441; Fig. 1).
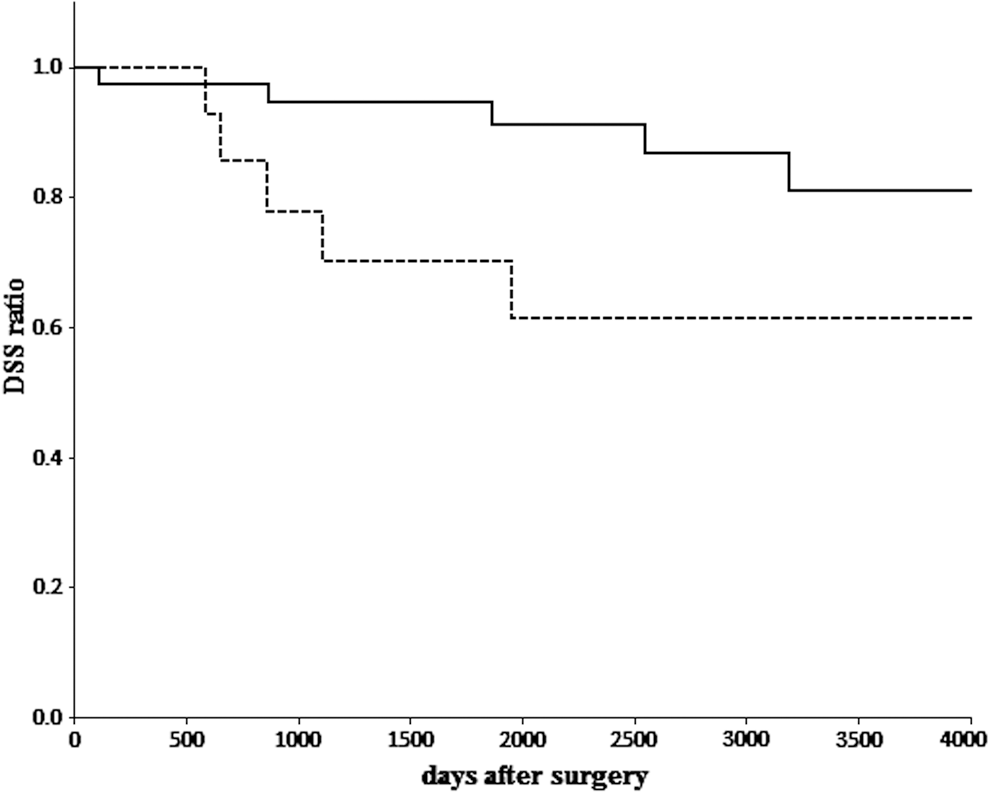
Comparison of disease-specific survival rates between patients with superficial and intraluminal invasion of the larynx. The solid line represents patients with superficial invasion of the larynx (n=40). The dotted line represents patients with intraluminal invasion of the larynx (n=15). Ten-year disease-specific survival rates were calculated using the Kaplan–Meier method and compared using the log-rank test. The 10-year disease-specific survival rate was significantly longer in the superficial invasion group than in the intraluminal invasion group (81.0% vs. 61.4%; p=0.0441).
Fifty of 55 patients (91%) with laryngeal invasion also had PTC invasion into other aerodigestive tract structures including the trachea (n=35), esophagus (n=35), and RLN (n=33). For the 35 patients with tracheal invasion, three types of surgical methods were performed: shave excision (n=10), window resection including circumferential resection (n=19), and total laryngectomy for laryngeal invasion (n=3). For the 30 patients with esophageal invasion, two types of surgical methods were performed: muscle layer resection (n=26) and esophageal reconstruction after tumor resection (n=4). For the 33 patients with RLN invasion, three types of surgical methods were performed: RLN resection (n=11), partial layer resection of the RLN (n=1), and RLN reconstruction after nerve resection (n=21; Table 2). Of these 50 patients, 14 patients had three invaded aerodigestive tract structures, 20 had two invaded structures, 16 had one invaded structure, and five had laryngeal invasion alone. The number of invaded aerodigestive structures including the larynx was correlated with permanent stoma presence (p=0.00132). Closing of the tracheal stoma did not occur in 10 patients with three invaded structures, nine with two invaded structures, six with one invaded structure, and one with laryngeal invasion alone. Permanent stoma occurred more frequently in patients with tracheal invasion than in those with invasion into other aerodigestive tract structures (Table 3).
PTC, papillary thyroid carcinoma; RLN, recurrent laryngeal nerve.
Permanent stoma occurred more frequently in patients with tracheal invasion than in those with invasion into other aerodigestive structures.
The rate of closing of the tracheal stoma and time to return to normal diet intake were used to assess functional outcomes after surgery for laryngeal invasion (Table 4). A permanent stoma was present in 26 patients (47%) including 14 patients with superficial invasion and 12 with intraluminal invasion (three of whom underwent total laryngectomy). A permanent stoma was part of the surgical plan in nine patients who received subtotal laryngectomy to restore phonetic function at the expense of the airway and three patients who received total laryngectomy. Closing of the tracheal stoma was possible in the other 17 patients (31%), including 14 patients who received framework resection and three patients with intraluminal invasion. Of the 14 patients who received framework resection, the permanent stoma was caused by laryngotracheal invasion-associated large tracheal defects in four patients, bilateral RLN invasion in five patients, continuous aspiration without pulmonary complications in three patients (laryngeal framework resection and esophageal reconstruction for laryngoesophageal invasion, n=2; age-associated depression in swallowing function, n=1), laryngeal stenosis associated with laryngeal fistula in one patient, and postoperative cardiorespiratory depression in one patient. Meanwhile, the causes of permanent stoma in patients with intraluminal invasion were continuous aspiration in two patients who received VHL and dysphagia in one patient who underwent nerve resection for glossopharyngeal nerve invasion by parapharyngeal metastasis. Laryngeal invasion was implicated in permanent stoma in 5 out of 17 patients. A permanent stoma was associated with laryngeal invasion in 14 patients (25%), including nine patients who underwent subtotal or total laryngectomy.
d, days; FW, framework; Lx, laryngectomy; VHL, vertical hemilaryngectomy.
The mean time to postoperative oral intake was 25 days. Patients who underwent partial laryngectomy including VHL had a prolonged time to oral intake (Table 4).
Discussion
The present study found that, in many patients, laryngeal invasion by PTC remained at the thyroid cartilage or paraglottic space, and most patients did not require total laryngectomy. However, laryngeal invasion was accompanied by invasion into other aerodigestive structures in most patients. Good locoregional control was achieved with surgical tumor excision in patients with laryngeal invasion. All deaths were caused by distant metastases and not locoregional failure.
Thyroid carcinoma invades the endolarynx via three distinct pathways: (a) anterior invasion through the cricothyroidal membrane or cricoid cartilage, which with full tumor penetration presents as an anterior glottic or subglottic mass; (b) lateral invasion through the thyroid cartilage lamina, which presents as a vocal fold paralysis, submucosal mass, or intraluminal ulceration of the hemilarynx; and (c) posterior invasion around the back of the thyroid cartilage into the paraglottic space (10). PTC invasion of the endolarynx that occurs via the first or second pathway is surgically treated with partial or total laryngectomy, whereas partial or total pharyngolaryngectomy is used to treat PTC invasion occurring via the third pathway. However, thyroid carcinoma, unlike laryngeal or hypopharyngeal cancer in which the mucosa is involved, invades the larynx from outside the cartilage. In the present study, laryngeal invasion often remained at the thyroid cartilage or paraglottic space before invading the endolarynx.
In the present study, the 10-year disease-specific survival rates after surgery were 81% and 61.4% for the superficial and intraluminal invasion groups, respectively. Although intraluminal invasion into the larynx was associated with worse prognosis, more than 60% of patients with intraluminal invasion survived for at least 10 years. Conservative or reconstructive surgery of the larynx is necessary for the treatment of PTC invasion of the larynx because long-term patient survival is expected, even in cases with PTC penetration into the larynx.
Comparisons of surgical outcomes have been primarily reported for PTC invasion into the airway. Few studies have investigated surgical outcomes for isolated locoregional recurrence within the airway or laryngeal recurrence. Furthermore, little is known regarding the relationship of excision range with postoperative laryngeal function. McCarty et al. (13) reported on the local control of laryngotracheal invasion in 40 patients with different histological subtypes of thyroid cancer. Two of 35 patients with superficial invasion who underwent cartilage shave procedures had isolated locoregional recurrence. Additionally, three patients, including one with isolated locoregional recurrence and two with intraluminal invasion, were managed with total laryngectomy. Gaissert et al. (15) reported the clinical outcomes of 82 thyroid cancer patients with laryngeal or tracheal invasion. In their study, 26 of 69 patients in the reconstruction group displayed local recurrence, and eight patients received an airway tube. In the reconstructed group, permanent tracheostomas were present in three patients at the time of initial surgery and eight patients with local recurrence. Total laryngectomy was performed for three patients in the salvage group. Wada et al. (11) reported the outcomes of 64 patients with laryngotracheal invasion by PTC. Thirteen patients underwent curative resection, including six pharyngolaryngoesophagectomies and two total laryngectomies, and six patients experienced local recurrence. Meanwhile, 33 patients underwent shave or partial resection (conservative surgery), and seven patients experienced local recurrence. In the present series, total laryngectomy was performed in four patients (7.3%) during the initial surgery for thyroid cartilage invasion or the surgery for isolated locoregional recurrence in the larynx. The total laryngectomy rate in all cases, including those with cricoid cartilage invasion (n=48), was only 3.9%. Three patients who underwent total laryngectomy during the initial surgery could not be intubated because of the presence of massive laryngeal tumors. Only two patients (3.6%) had an isolated locoregional recurrence in the larynx.
All fatalities (n=10) were caused by distant metastases, and no patient died from locoregional recurrence. The low rate of locoregional recurrence can be attributed to the surgical approach adopted, wherein pathologically negative margins were confirmed by frozen section analysis to reduce the risk of incomplete resection and to preserve as much adjacent healthy tissue as possible. Therefore, to ensure successful resection, margin negativity should be confirmed intraoperatively using cryosection analysis.
Partial frontolateral laryngectomy is an effective therapeutic option for early-stage glottic carcinoma and can be used to manage PTC invasion of the larynx, primarily intraluminal invasion. The functional outcomes of this surgical method were thought to be approximately reflected in patients with PTC invasion of the larynx. However, compared with the functional outcomes of partial frontolateral laryngectomy in early-stage glottic carcinoma, the present results indicate a higher rate of permanent stoma and longer period to return to normal oral intake in patients with PTC invasion of the larynx who underwent this procedure (24) The reason for the poor functional outcome included concurrent PTC invasion of the larynx and other aerodigestive structures, such as the RLN, trachea, and esophagus. PTC invades the aerodigestive tract from the outside and spreads peripherally to the inside. Indeed, a permanent stoma was associated with laryngeal invasion and invasion of other aerodigestive structures in 14 (25%) and 12 (22%) patients, respectively.
In the present study, the rate of thyroid cartilage invasion involving other aerodigestive structures exceeded 90%. The influence of the number of invaded aerodigestive structures on the likelihood of closing of the tracheal stoma was examined in 46 patients (nine patients who underwent total or subtotal laryngectomy were excluded), and it was found that PTC invasion of multiple aerodigestive structures may influence laryngeal functional outcomes. The involvement of two or more aerodigestive structures had a greater impact on closing the tracheal stoma than thyroid cartilage invasion alone or invasion of an aerodigestive structure other than the larynx. The number of invaded aerodigestive structures was correlated with permanent stoma risk.
Post-surgical external beam radiation therapy was not indicated for patients with laryngeal invasion. Unfortunately, distant metastasis frequently occurred, even in patients with good locoregional control, and became a leading cause of death.
In conclusion, laryngeal invasion by PTC remained at the thyroid cartilage or paraglottic space in many patients, and most patients did not require total laryngectomy. However, invasion into other aerodigestive structures was observed in most patients. Good locoregional control was achieved with surgical tumor excision in patients with laryngeal invasion. Distant metastases rather than locoregional failure was the major cause of death in patients with PTC invasion of the larynx.
Footnotes
Author Disclosure Statement
The author declares that no competing financial interests exist.