
Abstract
Background:
The aim of this review is to assess data available on iodine nutrition status in lactating mothers residing in countries with mandatory and voluntary iodine fortification programs and/or iodine supplementation.
Summary:
A systematic review was conducted by searching articles published between 1964 and 2013 in Pub Med, ISI Web, and Cochrane Library using iodine nutrition, lactation, iodine supplementation, and iodine fortification as keywords for titles and/or abstracts. Relevant articles were included if they reported urinary iodine concentration (UIC) in lactating mothers and, if determined, the type of iodine fortification program and/or iodine supplementation. Forty-two studies met the inclusion criteria. Among these, 21 studies assessed lactating mothers in countries with a mandatory iodine fortification program, 17 studies were from countries with voluntary and/or without iodine fortification programs, and four studies assessed iodine nutrition status in lactating mothers undergoing iodine supplementation. Among countries with mandatory iodine fortification programs, the range of salt iodization level in lactating mothers with a UIC <100 μg/L was between 8 and 40 ppm, whereas among lactating mothers with UIC >100 μg/L, it was between 15 and 60 ppm. Levels of UIC <100 μg/L were observed among lactating women in India, Denmark, Mali, New Zealand, Australia, Slovakia, Sudan, and Turkey, whereas in countries such as Chile, Iran, Mongolia, New Guinea, and Nigeria, the median or mean of UIC was >100 μg/L. There was a median or mean UIC <100 μg/L in nearly all lactating mothers residing in countries where implementation of universal salt iodization program was voluntary, including Switzerland, Australia, New Zealand, Ireland, and Germany. However, in some countries with voluntary iodine fortification programs, such as the United States, Spain, and Japan, a mean or median UIC of >100 μg/L has been reported.
Conclusions:
Although universal salt iodization is still the most feasible and cost-effective approach for iodine deficiency control in pregnant and lactating mothers, UIC in lactating mothers of most countries with voluntary programs and in areas with mandatory iodine fortification is still within the iodine deficiency range, indicating that iodine supplementation in daily prenatal vitamin/mineral supplements in lactating mothers is warranted. However, further investigations are still recommended in this regard.
Introduction
I
According to criteria of the World Health Organization (WHO), the Iodine Global Network (IGN; previously the ICCIDD), and the United Nations Children's Fund (UNICEF), median urinary iodine concentration (UIC) in a representative sample of schoolchildren provides an adequate assessment of a population's iodine nutrition in response to salt iodization programs. However, it may not reflect the status in pregnant and lactating women, whose iodine requirements are greater (6). There is much evidence indicating suboptimal iodine status among pregnant and/or lactating women, despite iodine sufficiency among schoolchildren in countries designated as iodine sufficient (7 –13).
On the other hand, to eliminate iodine deficiency, in almost all countries, only table salt or cooking salt is mandated to be iodized, as it is feasible, cheap, safe, rapidly effective, and widely accepted (6). In some countries such as Australia and New Zealand, mandatory iodine fortification of salt is used in the bread-making process (14,15). Data available from countries with a mandatory iodine fortification program reveal that they achieved great success in the control and elimination of iodine deficiency among the general population. However, some groups, such as pregnant and/or lactating women, with higher iodine requirements have remained iodine deficient (8 –10,16). Moreover, where iodization of this type of salt is still voluntary, this can be a real constraint in eliminating iodine deficiency (17).
Furthermore, based on WHO/ICCIDD/UNICEF recommendations, in countries whose populations are considered iodine sufficient (assessed by the median UIC in schoolchildren), pregnant and lactating women have no need for iodine supplements (18). However, recent NHANES data have shown that more than half of pregnant women in the United States have iodine deficiency, and major societies have recommended iodine supplementation of 150 μg daily during pregnancy and lactation (19,20).
Hence, to the best of the authors' knowledge, this review explores for the first time the information available regarding iodine nutrition status in lactating mothers residing in countries with mandatory and voluntary iodine fortification programs and/or iodine supplementations.
Methods
Search strategy
This systematic review of all papers, published between October 1964 and November 2013, was conducted using the electronic databases MEDLINE, the Cochrane Library CENTRAL, and ISI Web of Science. Additional searches were conducted using World Health Organization (
Study selection and data extraction
Two of the authors (P.N. and P.M.) conducted the search independently. Once the search was completed, the title and abstract of the studies identified were scanned to exclude studies that were obviously irrelevant. The full texts of the remaining studies were retrieved, and all relevant articles were identified. Criteria for inclusion of studies in the systematic review were: all articles were human studies, lactating women as target participants were assessed, the UIC in mean or median values were reported, and type of iodine fortification program or iodine supplementation had been determined. Any duplicate publications were excluded as well as any potentially relevant articles lacking full texts.
Data from the studies included were extracted by two authors (P.N. and P.M.) independently on standardized forms developed for this review, and if any discrepancies were found, they were removed by consensus. The following data were extracted: first author, year of publication, country or location of study, iodine supplementation program, the level of iodization, year initiated for salt iodization program, type and dose of iodine supplementation, number of subjects, stage of postpartum, and mean or median UIC.
Results
The flowchart for this review is given in Figure 1. A total of 155 titles and abstracts were screened after the electronic search, of which 52 appeared potentially relevant and were assessed as full-text papers for inclusion. Twenty-five potential studies were excluded due to lack of inclusion criteria. The main reason for excluding an article was that it did not report any data for UIC in lactating mothers. An additional 15 publications were added from screening reference lists, yielding a total of 42 papers for inclusion in the present systematic review. Among these, 21 studies were conducted in countries with mandatory iodine fortification programs, 17 were from countries with voluntary and/or without iodine fortification programs, and four studies assessed iodine nutrition status in lactating mothers who had undergone iodine supplementation.
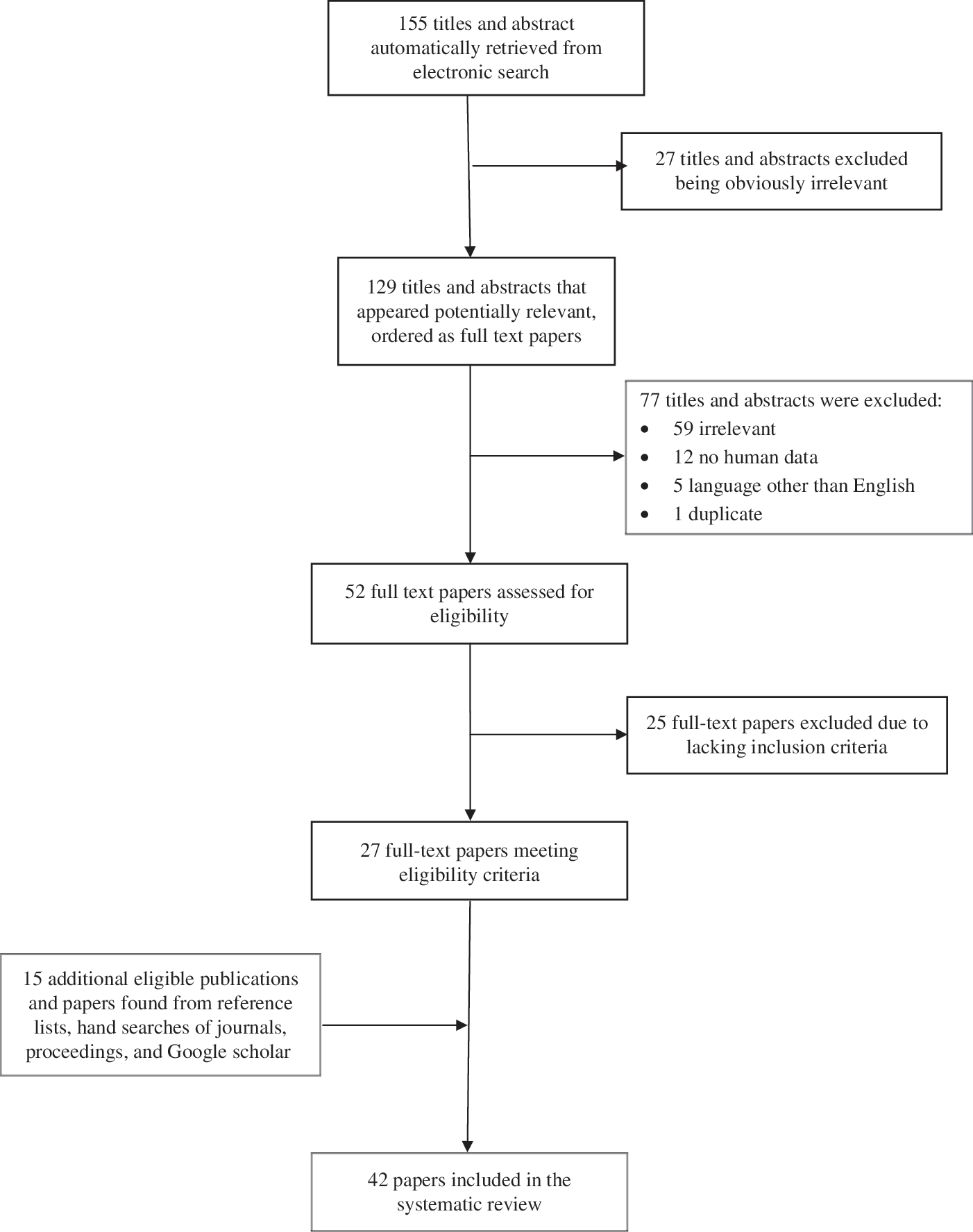
Flowchart for selection of studies for the present systematic review.
Iodine nutrition of lactating mothers in countries with a mandatory iodine fortification program
Among countries with mandatory iodine fortification programs, Australia (8) and New Zealand (21) have iodine fortification of bread, introduced in 2009. Denmark also has mandatory iodine fortification of bread in addition to a general salt iodization program since 2000 (22). The remaining countries have salt iodization programs. Mandatory iodine fortification was initiated before 1990 for Chile (23) and Slovakia (24), whereas this was done between 1990 and 2000 for India (25,26), Iran (27 –29), Mali (30), Mongolia (31), Nepal (32), New Guinea (33), Nigeria (34), Sudan (35), and Turkey (36). In countries where lactating mothers had UIC <100 μg/L, the salt iodization level ranged between 8 and 40 ppm, whereas it ranged between 15 and 60 ppm among lactating mothers with UIC >100 μg/L. UIC <100 μg/L was observed among lactating women in countries including India (25,26), Denmark (37), Mali (30), New Zealand (10), Australia (8), Slovakia (24), Sudan (35), and Turkey (36), whereas in countries such as Chile (23), Iran (27 –29), Mongolia (31), New Guinea (33), and Nigeria (34), the median or mean UIC in lactating mothers was >100 μg/L (Table 1). Sample sizes were >125 subjects only in China, India, Iran (Isfahan), Mali, Mongolia, Nepal, and Slovakia, and among these, China, India, Iran (Isfahan), and Mongolia had a mean or median UIC >100 μg/L.
Taking a supplement containing iodine.
Value given is the mean.
Value given is μg/day.
Value given is μg/g Cr.
SI, salt iodization.
Iodine nutrition of lactating mothers in countries with voluntary and/or without iodine fortification programs
Table 2 shows the iodine status of lactating mothers in different countries with voluntary and in those without iodine fortification programs. Iodine fortification was initiated between 1922 and 1992 in countries with voluntary iodine fortification programs. Salt iodization levels range between 15 and 100 ppm in these countries, with the United States (38 –42) and Germany (43) having the highest and lowest salt iodization level, respectively. There was a mean or median UIC <100 μg/L in nearly all lactating mothers residing in countries where implementation of a universal salt iodization program is voluntary, including Switzerland (7), Australia (44,45), New Zealand (46), Ireland (11), and Germany (43), although a mean or median UIC >100 μg/L has been reported in the United States (38 –42), Spain (12), and Japan (47). The sample sizes were >125 subjects only in Germany, Japan, and Switzerland, and a mean or median UIC >100 μg/L was observed only in Japan. The frequencies of countries with various levels of urinary iodine in lactating women according to mandatory and voluntary iodine fortification programs are presented in Table 3. Mean or median UIC of lactating mothers were >100 μg/L in >50% of countries with mandatory iodine fortification program, whereas this value was <33% in countries with voluntary iodine fortification programs.
Value given is μg/g Cr.
Value given is μg/day.
Value given is μmol/L.
Value given in the mean.
Mean or median.
Iodine nutrition of lactating mothers supplemented with iodine
The effects of iodine supplementation with different doses have been examined among lactating mothers in four countries, including the United States (48) and Italy (49) with voluntary, and New Zealand (50) and Morocco (21) with mandatory iodine fortification programs (Table 4). In the United States, effects of 150 μg iodine supplementation on maternal iodine status indicated that breast-feeding mothers did not receive the recommended intake of iodine. This was similar to New Zealand, where the daily supplementation of either 75 or 150 μg iodine for iodine-deficient lactating women was insufficient to restore an optimal iodine status (50). Even in Morocco with moderate to severe iodine deficiency, the median UIC in lactating women supplemented with 400 mg iodized oil remained <100 μg/L, although it was significantly improved compared to placebo users. In addition, maternal rather than infant supplementation provided adequate iodine status for lactating mothers and their infants (21). However, iodine supplementation with 200 and 50 μg provided iodine sufficiency among lactating women in Italy; compared to the women treated with a daily dose of 50 μg, those supplemented with an iodine dose of 200 μg had a higher UIC.
Value given is the mean.
Value given is μg/g Cr.
Estimated mean total iodine excretion based on 90% excretion corresponding to recommended dietary allowance intake (if adequate, this would be at least 261 μg).
V, voluntary; M, mandatory; PM, past midday; AM, after midnight.
Discussion
Iodine nutrition status during lactation
The success or failure of fortification programs in correcting iodine deficiency is determined by assessing median UIC every five years at a population level in schoolchildren aged 6–12 years (6), which serves as proxy for the general population. However, the controversy associated with this method is the use of a single median value, which may mask a significant proportion of the iodine deficient population, and different subgroups (pregnant and lactating women) possibly at high risk may be overlooked (6). In their latest recommendation (6), the WHO/ICCIDD/UNICEF proposed a median level of >100 μg/L urinary iodine be considered as iodine sufficiency for lactating mothers. The figures for urinary iodine are lower than daily iodine requirements, that is, 290 and 250 μg according to recommended dietary allowance and WHO recommendations, respectively, because of excretion of iodine by breast milk. On the Eastern Mediterranean coast of Spain, the median UIC for all lactating women newly enrolled in the “well-baby practice” program was 110.5 μg/L (range 9–875 μg/L), which indicates iodine deficiency in mothers, despite iodine sufficiency among schoolchildren (12). Moreover, the study by Andersson et al. from Switzerland reported that despite iodine sufficiency in the general Swiss population, mothers of 6- and 12-month-old infants were still iodine deficient (7). Even in China and Japan, which are considered iodine sufficient areas, the difference in median UIC of schoolchildren and pregnant and lactating women is approximately 50 μg/L for pregnant and 40 μg/L for lactating women in China, and >100 μg/L in both pregnant and lactating Japanese mothers (47,51).
Universal salt iodization (USI) guarantees adequate dietary iodine intake (52). Today, at least 128 countries have salt iodization programs, and so far, 37 of these have achieved adequate iodized salt consumption in ≥90% of households (53). However, a median UIC <100 μg/L has been observed among lactating mothers, even in countries with mandatory iodine fortification, such as India (25,26), Denmark (16,37), Mali (30), Nepal (32), New Guinea (33), New Zealand (10), Slovakia (24), Sudan (35), and Turkey (36). Reasons for this include remote regions with relatively little or no access to iodized salt and high losses of iodine from iodized salt (Mali); inadequate iodine content of household salt (Denmark); change in iodine content of food stuffs, infrequent use of iodized salt in households, and increase in noniodized salt use in commercial foods (New Zealand); relative humidity, type of packaging, and local practice for preparing and cooking with iodized salt (i.e., washing salt; Nepal); low consumption of iodized salt due to a popular belief that high intake of salt is associated with high blood pressure (New Guinea); lack of enforcement for iodization of industrial salt (Turkey); and last, but not least, insufficient production of iodized salt (Sudan). In India, the national average self-reported consumption of iodized salt is 76.1%, whereas only 51.1% of Indians consume iodized salt adequately (54).
Furthermore, it is important to note that in nearly all lactating mothers residing in European countries, including Switzerland (7), Spain (12), Ireland (11,55), and Germany (43,56), where implementation of the USI program is voluntary, there is a median UIC <100 μg/L. There are several obstacles and barriers that affect the iodine nutrition status of the general population, and in particular breast-feeding mothers, in countries with voluntary iodine fortification programs (i.e., USI). The data reveal insufficient progress in the optimum use of adequately iodized salt in households worldwide, and reasons for this trend include limited consumer awareness and availability of iodized salt. The quality and level of iodine are equally as important as its coverage. Recently, several countries identified inaccuracies between the labeled iodine content and iodine levels measured in salt used in households (54). Inconsistent production or limitations in quality-controlled iodization technology at the factory level, poor packaging, and ineffective transport channels may explain varying iodine levels and iodine loss, resulting in inadequate amounts of iodine in household salt. Another limitation is that the assessment of household consumption of iodized salt is not an optimal indicator for implementation of USI. For example, in the United States and Canada, despite approximately 70% of consumers actually choosing iodized salt for household use, only 15% of their daily iodine intake comes from iodized salt (57). Again, in Europe, of 40 countries, only 23 have some legislation or regulations in place covering USI at household levels. However, legislation covering processed food is rare, and only 50% of European countries have national monitoring programs (17).
The prevention and control of iodine deficiency is a continuous process, requiring sustained monitoring. Iodine deficiency has reemerged as a public health problem in countries where it was once under control, as seen in Guatemala, the Dominican Republic, Haiti, Mexico, Colombia, Thailand, and some regions of the former Union of Soviet Socialist Republics, Azerbaijan, Kazakhstan, and Kyrgyzstan (58 –60). Some developed countries (i.e., Australia, New Zealand, and the United Kingdom) have also experienced recurrences of iodine deficiency (61 –63).
Universal salt iodization or fortification of individual foods
Despite concerted efforts in many countries to reduce salt intake for the prevention of hypertension and cardiovascular diseases (64), concern has been expressed that decreasing salt consumption could increase the risk of iodine deficiency. Data from the Netherlands demonstrated that only with a 50% reduction in salt intake did iodine intake become inadequate for only a small percentage of the population, results that confirmed views of iodine experts that there is no conflict between salt reduction and iodized salt consumption (64). Furthermore, the association between salt restriction and iodine deficiency in adults indicated that in persons consuming low levels of iodine, salt restriction may cause iodine deficiency (65). In Germany, a slow but constant decrease in the use of iodized salt in processed foods since 2004 resulted in decreased UIC among schoolchildren after 2007 (43,66). A recent study conducted in adult Iranians revealed that decreased salt intake over a 10-year duration (2000–2010) led to an increased percentage of subjects with UIC <100 μg/L (67). However, the study by Charlton et al. conducted among nonpregnant and nonlactating in South African women demonstrated that low salt intakes have no effect on UIC (68).
Additional alternative vehicles for iodine fortification may be explored to complement reduced iodine intake in populations where iodized salt consumption decreases. Thus, other components in the diet have been fortified either by including iodized salt as an ingredient, for example with bread in Holland, Denmark, Australia, New Zealand, and Tasmania (14,15,22,69,70), or by giving animals iodine-enriched feeds that result in an increase in the iodine content of foods produced by these animals (e.g., eggs and milk in countries such as Thailand, Norway, and Finland), or by the direct addition of an iodine compound to sugar, fish sauce, and water (54,71 –73). Iodine supplementation with iodized oil or iodine tablets is recommended in areas with moderate to severe deficiency or in areas with insufficient access to iodized salt for some groups within the population (i.e., pregnant women and young children) (54). Although the Iodine Global Network does not yet support the iodization of individual foods, USI is still the most feasible and cost-effective approach for iodine-deficiency control worldwide.
Iodine fortification program (mandatory vs. voluntary)
The decision to implement mandatory fortification or voluntary fortification is often influenced by significant public health needs and the food industry. Compared to other countries worldwide, national commitment toward ensuring adequate iodine nutrition and its prevention is much weaker in most European countries, where use of iodized salt is often permitted but not required. Data available for 29 countries show that the use of iodized salt is voluntary in 16 countries and mandatory in 13, indicating that in most European countries, salt iodization is far from being universal (17). Those most in need of iodine supplementation are unfortunately not necessarily receiving it, a status exacerbated in areas where monitoring of iodine levels has not been updated.
Mandatory production of iodized salt with 40 ppm iodine concentrations for household consumption was begun in the Islamic Republic of Iran in 1994 (74,75). Four nationwide surveys show Iran has achieved great success in the control and elimination of iodine deficiency disorders following well-monitored national salt iodization programs (76). However, in two studies, the risk of iodine deficiency in some lactating mothers and breast-fed infants has been reported (27,29).
Switzerland also has a good monitoring program. If necessary, adjustments are readily made to the amount of iodine in iodized salt by federal decree, rather than the long drawn-out parliamentary process required in many other countries, resulting in adequate iodine status of both children and pregnant women (77,78). However, lactating women with higher iodine requirements have an inadequate intake of iodine (7).
In Tasmania, a voluntary iodine fortification program of iodized salt in bread had no impact on the iodine status of pregnant and lactating women (69). Following this, in Australia and New Zealand, mandatory iodine fortification of salt used in the bread-making process at the level of 14–28 μg/100 g was introduced in 2009, and results indicate that the fortification program may have benefited breast-feeding women. However, the iodine status remained inadequate in those not consuming iodine containing supplements (8,79).
Although the United States began voluntary fortification of table salt to address iodine needs in 1924, the most recent NHANES survey (2005–2010) has shown that more than one third of American women of childbearing age and more than half of pregnant women have UIC <100 μg/L and <150 μg/L, respectively (19,80). Possible contributors to this change include a greater consumption of salt from processed foods, decreased use of dough conditioners in the baking industry, and limited levels of iodine used in cattle feed (81).
Iodine supplementation during lactation
Based on current evidence and lessons learned within the past decade, it appears that in some countries/areas, the iodine requirements of the most susceptible groups (pregnant and lactating women and children aged 6–24 months) are not always adequately met by iodized salt. Some studies voice concerns that despite using iodized salt, consumption levels of small children are below the levels required to achieve adequate iodine status.
To address the above situation, the WHO/UNICEF issued a joint statement in 2007 on “Reaching Optimal Iodine Nutrition in Pregnant and Lactating Women and Young Children,” recommending that besides strengthening USI programs, additional complementary strategies such as iodine supplements be considered to ensure optimal iodine nutrition for these groups (82).
Moreover, to ensure adequate iodine intake for pregnant and lactating women and infants younger than two years old, the WHO/ICCIDD/UNICEF have divided all countries into three groups (18). The first group is countries with effective and sustained salt iodization, whose pregnant and lactating women have no need for iodine supplements. The second group comprises countries with uneven or lapsed iodized salt distribution; effective USI should hence be implemented in conjunction with programs of public education, and iodine supplementation is still needed for pregnant and lactating women and for young children. The third group is countries with weak or negligible iodized salt distribution, where such populations (i.e., pregnant or lactating women, women of childbearing age, and children younger than two years of age) should receive daily iodine supplements.
Furthermore, considering the levels of iodine fortification ranging between 20 and 40 ppm in most countries, for a lactating mother, the adequate amount of iodine can only be ensured by a daily intake of 6 g of 40 ppm iodized salt. Unfortunately, this is not the case in most regions of the world, thus necessitating iodine supplementation to ensure adequate iodine nutrition in pregnant and lactating women.
However, the American Thyroid Association (ATA) and the Endocrine Society recommend that pregnant and lactating women take vitamin/mineral supplements containing 150 μg iodine daily. This recommendation is based on the most recent data from the NHANES survey (2005–2010), which indicated that 37.3% of American women of childbearing age have UIC <100 μg/L, while 55.8% of pregnant women have UIC <150 μg/L (19,20,83,84). Despite these data, only a few studies with small sample sizes specifically address the effect of iodine supplementation on the iodine nutrition status during lactation in both breast-feeding mothers and their infants, making it difficult to draw conclusions (48 –50).
Lastly, caution should be taken in interpreting results based on the fact that urinary iodine excretion reflects iodine intake over a short time period and the variation is huge, which affects the reliability of studies of iodine nutrition. Hence, the number of spot urine samples required to estimate iodine status in a population with a 95% confidence interval within precision ranges of±10% and±5% should be approximately 125 and 500, respectively (85).
Conclusion
To the authors' knowledge, this is the first systematic review that provides a summary of the iodine nutrition status among lactating mothers living in countries with voluntary or mandatory iodine fortification programs. The implementation and sustainability of universal salt iodization is still the optimal strategy for adequate iodine nutrition in pregnant and lactating mothers, although it is not a means in itself to achieve optimal iodine nutrition. The median UIC constitutes an index of success or failure of iodine fortification programs, which can be influenced by several factors, including inappropriate monitoring of the salt iodization program, inadequate government support, change in iodine content of food stuffs, infrequent use of iodized salt in households, increase in noniodized salt use in commercial foods, and inadequate amount of iodine in salt used in households. Regardless of mandatory and/or voluntary iodine fortification programs, for provision of adequate iodine nutrition among pregnant and lactating women, the ATA and the Endocrine Society recommend that universal salt iodization should be implemented in conjunction with 150 μg iodine supplementation in daily prenatal vitamin/mineral supplements. More investigations are still required in this regard.
Footnotes
Acknowledgments
This study was supported by a financial grant from Research Institute of Endocrine Sciences, Shahid Beheshti University of Medical Sciences. The authors express their appreciation and gratitude to Marzieh Atashkar for her assistance in accessing the full text of papers included in this study.
Author Disclosure Statement
None of the authors has any personal or financial conflicts of interest.