
Abstract
Background:
Medical costs in the United States have been increasing disproportionally to gross domestic product, raising concerns about the sustainability of U.S. healthcare expenditures. Care of patients with thyroid disease has been identified as an area of medicine where cost increases have been pronounced.
Objectives:
The goals of this study were to identify potential drivers of the cost of hospitalization following thyroid surgery, and to understand which of these factors may be contributing to observed increases in cost from 2003 to 2011.
Methods:
A retrospective cross-sectional analysis of discharge data from the Nationwide Inpatient Sample (NIS) database for all admissions following thyroid lobectomy or total thyroidectomy in the years 2003, 2007, and 2011 was performed. Multiple regression analysis via a weighted generalized linear model was used to identify factors that were independently associated with high cost of hospitalization. Trend as well as subgroup analyses were then performed to identify which of these factors could be contributing to increasing costs.
Results:
There were 47,854 hospital admissions following total thyroidectomy or thyroid lobectomy identified in the years 2003, 2007, and 2011. The aggregate national cost of hospitalization increased from $198 million in 2003 to $373 million in 2011 in inflation-adjusted 2011 dollars. The weighted mean cost of hospitalization following thyroid surgery increased from $6154 to $8982 from 2003 to 2011 in inflation-adjusted 2011 dollars. Higher comorbidity score, total thyroidectomy, lymphadenectomy, western region, rural region, and certain postoperative complications were the factors most highly associated with increased hospital costs. Of these, an increasing proportion of patients with higher severity of illness score and an increasing proportion of patients undergoing total thyroidectomy and lymphadenectomy were implicated as the most likely contributors to the cost increases. The rate of total thyroidectomy and lymphadenectomy was found to be increasing for patients with both benign and malignant thyroid disease.
Conclusions:
According to the NIS data set, costs associated with hospitalization after thyroid surgery increased markedly from 2003 to 2011. This increase could be in part due to a growing proportion of sicker patients undergoing more extensive surgery, but a number of confounders in this study limit the conclusions. Further analysis of factors that could be associated with the rising costs of inpatient thyroid surgery should be undertaken.
Introduction
T
The surgical management of thyroid disease has become a significant economic burden in the United States. From 1996 to 2006, hospital charges from inpatient thyroidectomy for thyroid cancer have tripled on an aggregate basis and more than doubled per capita (5,8,13,14). The increasing use of novel surgical instruments, the rising incidence of well-differentiated thyroid cancer, changing inpatient characteristics, and complication rates have been shown to have a significant financial impact on thyroid surgery (3,8 –11). However, the main drivers of inpatient thyroid surgical costs remain largely unknown on a national level.
The objective of this study was therefore to utilize hospital discharge data from the Nationwide Inpatient Sample (NIS) to identify trends and primary drivers of cost attributed to thyroid surgery. It was hypothesized that the cost of thyroid surgery is increasing and can in part be attributed to the changes in the characteristics of inpatients undergoing surgery and changes in the types of surgery they are undergoing.
Methods
A cross-sectional analysis of hospital admissions following total thyroidectomy or thyroid lobectomy was performed using discharge data from the NIS, Healthcare Cost and Utilization Project (HCUP), and Agency for Healthcare Research and Quality (AHRQ) (15). The NIS is the largest all-payer inpatient care database in the United States, containing data from approximately eight million hospital stays each year from a stratified sample of 20% of non-federal U.S. hospitals in participating states. The International Classification of Disease, 9th revision (ICD-9) codes were used to identify all inpatient hospital stays for which the primary procedure listed was thyroid lobectomy or total thyroidectomy in the years 2003, 2007, and 2011 (Table 1).
Data were analyzed using SPSS Statistics for Windows v22 (IBM Corp., Armonk, NY). Variables with missing data for >10% of the populations were coded with a dummy variable to represent the missing data in regression analyses. Weights were applied to all data when calculating national estimates of admission characteristics, cost trends, and means. The “complex samples” function available within SPSS was used to account for weights and stratification during all regression analysis. This protocol was exempt from review by the Institutional Review Board of the University of California, Davis.
Cost was examined as our dependent variable. Hospital-related charges for each index admission were converted to the organizational cost per index case of providing care using cost-to-charge ratios provided by AHRQ for individual hospitals (16). Costs were then adjusted to 2011 U.S. dollars using data from the U.S. Bureau of Labor Statistics (17). Weighted means and confidence intervals (CIs) were calculated for inpatient hospital costs in each of the studied years. A one-way analysis of variance (ANOVA) test was utilized to assess the significance of differences between these means.
The independent variables included demographic factors, diagnostic and procedural information, hospital characteristics, and the occurrence of postoperative complications. Inpatient admission in the NIS data set is defined as any admission to hospital regardless of length of stay (LOS). Patients admitted for observational stays of less than 24 h have a LOS of 0. For each hospital admission, a diagnosis-related group (DRG) severity of illness classification is assigned by the AHRQ and recorded in the NIS database. This classification system is used by the AHRQ to stratify the extent of an individual's physiologic decompensation or organ system loss of function at the time of admission. Cases with a DRG severity of illness score of 3 or 4 were combined into a single subgroup given their limited numbers. ICD-9 diagnostic codes for thyroid disease were used to categorize patients as having benign, malignant, or other thyroid disease. Cases in which some type of lymphadenectomy in addition to thyroid surgery were identified using ICD-9 procedural codes for all types of concurrent lymphadenectomy (Table 1).
Hospital characteristics including size (small, medium, large), geographic location, urban/rural location, and teaching status were directly available from the NIS database. Hospital bed-size categories are defined by the NIS with integration of region, urban–rural designation, and teaching status. The number of beds listed for these categories varies according to these factors and is listed at
A generalized linear model (GLM) was used to identify factors that were independently associated with high hospital costs. A log-link was used, given that cost data were not severely skewed. This analysis was performed for the years 2003, 2007, and 2011 in order to evaluate for persistence of associations over the studied years. Factors were considered relevant high-cost associated factors if they were highly correlated (beta coefficient >1) with increased cost over two of the three sampled years (Table 2).
Reference groups are: Female sex, age <45 years, white race/ethnicity, lowest income quartile, comorbidity score 1, benign disease, thyroid lobectomy, large bed size, non-teaching hospital status, northeastern region, and urban region.
Income quartiles. For 2003: lowest <$35,999, lower middle $36,000–44,999, upper middle $45,000–59,999, highest>$60,000. For 2007 and 2011: lowest <$38,999, lower middle $39,000–47,999, upper middle $48,000–62,999, highest >$63000.
p<0.001.
Trends in the number of admissions with high-cost associated factors were then analyzed in order to determine which of these factors may be contributing to the observed increase in hospital costs. In order to compare the association of each of these high-cost associated factors with time, a simple logistic regression was performed with each of the selected factors used as the dependent variable (0/1) and time as the independent variable. High-cost associated factors were then ranked according to their association with time as measured by the size of the regression coefficient beta. Cochran–Armitage trend tests were used to determine the significance of these trends over the years 2003, 2007, and 2011. The percent of admissions with each of the relevant factors with significant trends was then plotted as a function of year.
Trends in the use of total thyroidectomy and lymphadenectomy were then compared between admissions with a primary diagnosis of benign versus malignant disease. A simple logistic regression was performed with total thyroidectomy and lymphadenectomy as the dependent variable (0/1) and time as the independent variable. Again, Cochrane–Armitage trend tests were used to determine the significance of these trends over the studied years. The percent of total admissions with total thyroidectomy and lymphadenectomy were plotted as a function of year.
Results
There were 47,854 hospital admissions following total thyroidectomy or thyroid lobectomy in the years 2003–2011 identified in the NIS database. The weighted mean patient age was 51.5 years, and the weighted mean hospital cost of admission was $7666 in 2011 inflation-adjusted U.S. dollars. The majority of patients were female (80.1%) and white (55.5%). A total of 71.9% of patients had a DRG severity of illness score of 1, 25.1% had a DRG severity of illness score of 2, and 3% had a DRG severity of illness score of 3 or 4. Patients were well distributed across the socioeconomic spectrum. The majority of patients was treated for benign disease (61.8%) and underwent total thyroidectomy (60.3%). A total of 8.9% of patients underwent some type of lymphadenectomy in conjunction with their thyroid surgery (Table 3).
DRG, diagnosis-related group.
The number of patients admitted following total thyroidectomy or thyroid lobectomy increased by 13.7% from 2003 to 2011 (44,852 to 50,998). The aggregate national cost of all hospital admissions following total thyroidectomy or thyroid lobectomy increased by 88.7% from 2003 to 2011 (US$198 million to US$373 million). The weighted mean cost of hospitalization following total thyroidectomy of thyroid lobectomy increased by 45.1% from 2003 to 2011 (US$6154 to US$8932; Fig. 1). One-way ANOVA demonstrated that the difference in mean cost between each of the studied years was significant (p<0.001).
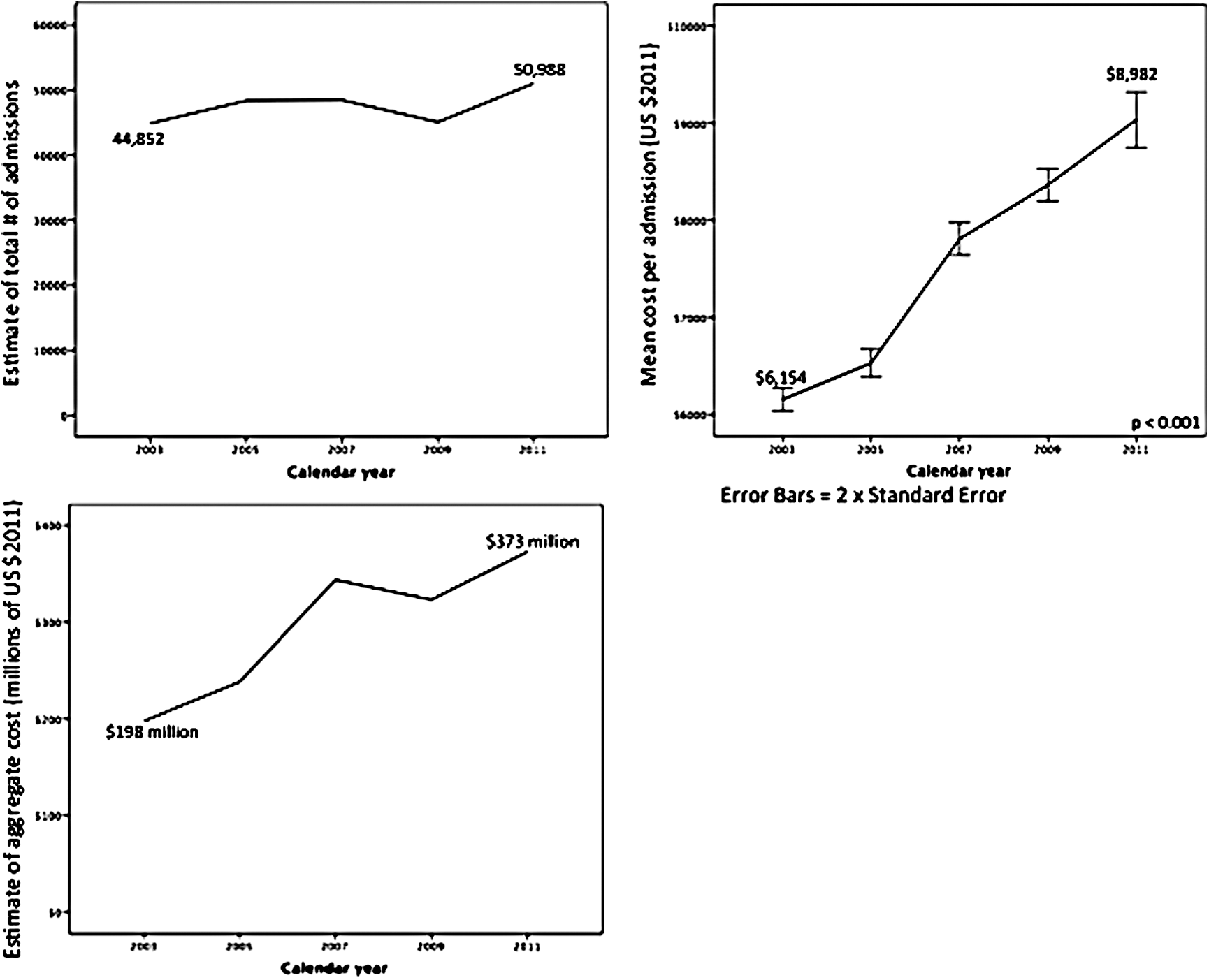
Trends in number of admissions and hospital costs following thyroid surgery 2003–2011.
A generalized linear model demonstrated a number of factors that were consistently, significantly, and highly correlated with elevated cost (Supplementary Tables S1–S4; Supplementary Data are available online at
Analysis of trends of these high-cost associated factors over time demonstrated that the number of admissions with many of these factors present was increasing with time. The largest proportional increases were seen in the number of admissions for patients with high comorbidity scores and those undergoing total thyroidectomy and lymphadenectomy. Significant but smaller proportional increases were also seen in the number of admissions for patients with black race/ethnicity, male sex, and a malignant diagnosis. There were no significant trends in occurrence of postoperative complications, or in the regional distributions of admissions (Fig. 2).
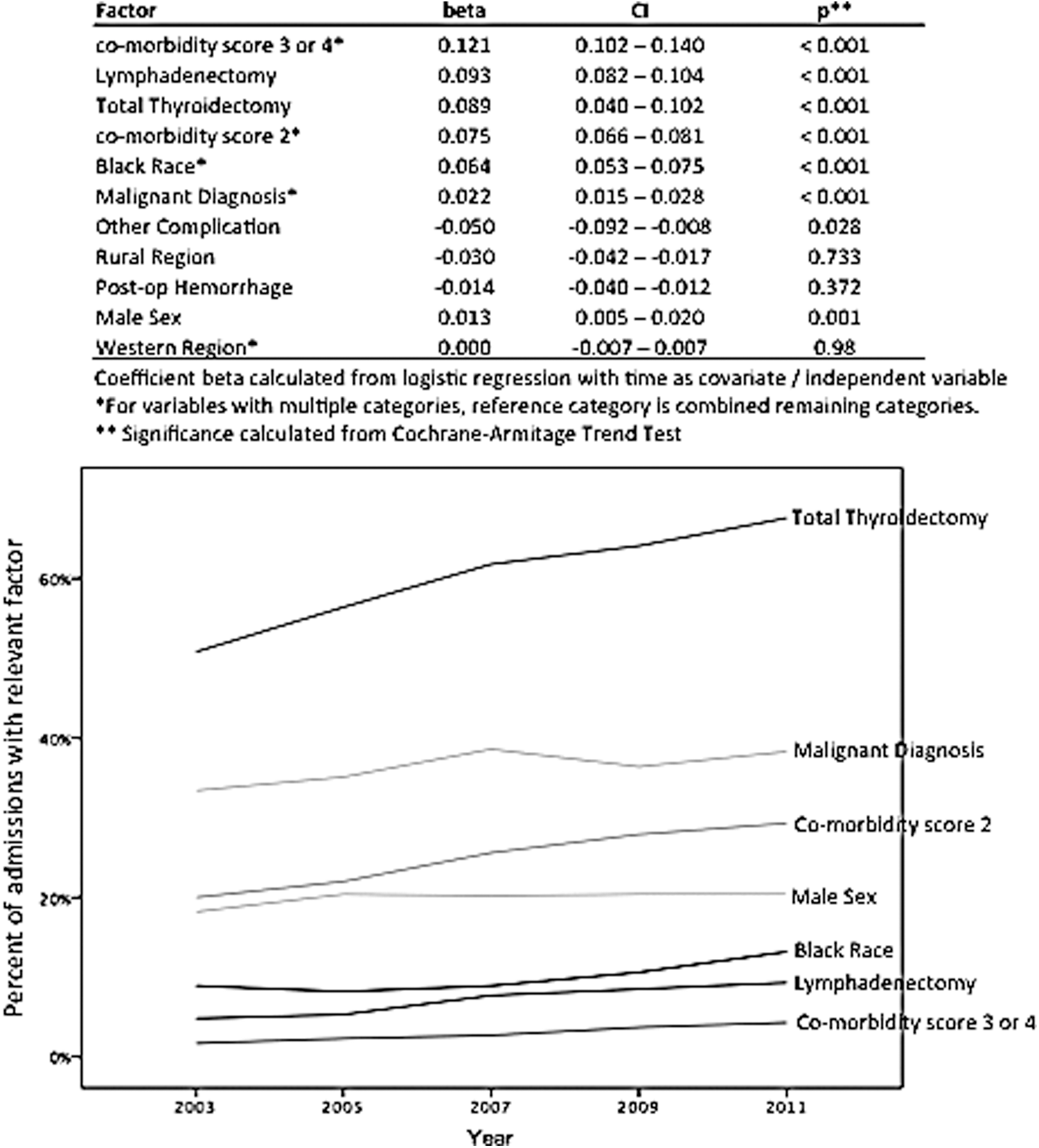
Potential drivers of cost increase.
Further trend analysis demonstrated that total thyroidectomy and lymphadenectomy are becoming more common for the treatment of both benign and malignant disease. The largest increase was seen in the use of total thyroidectomy for benign disease (40.3–61% of admissions for benign disease). Large increases were also seen in the percent of patients receiving total thyroidectomy for malignant disease (72.5–80.7%) and lymphadenectomy for malignant disease (16.5–28.4%; Fig. 3).
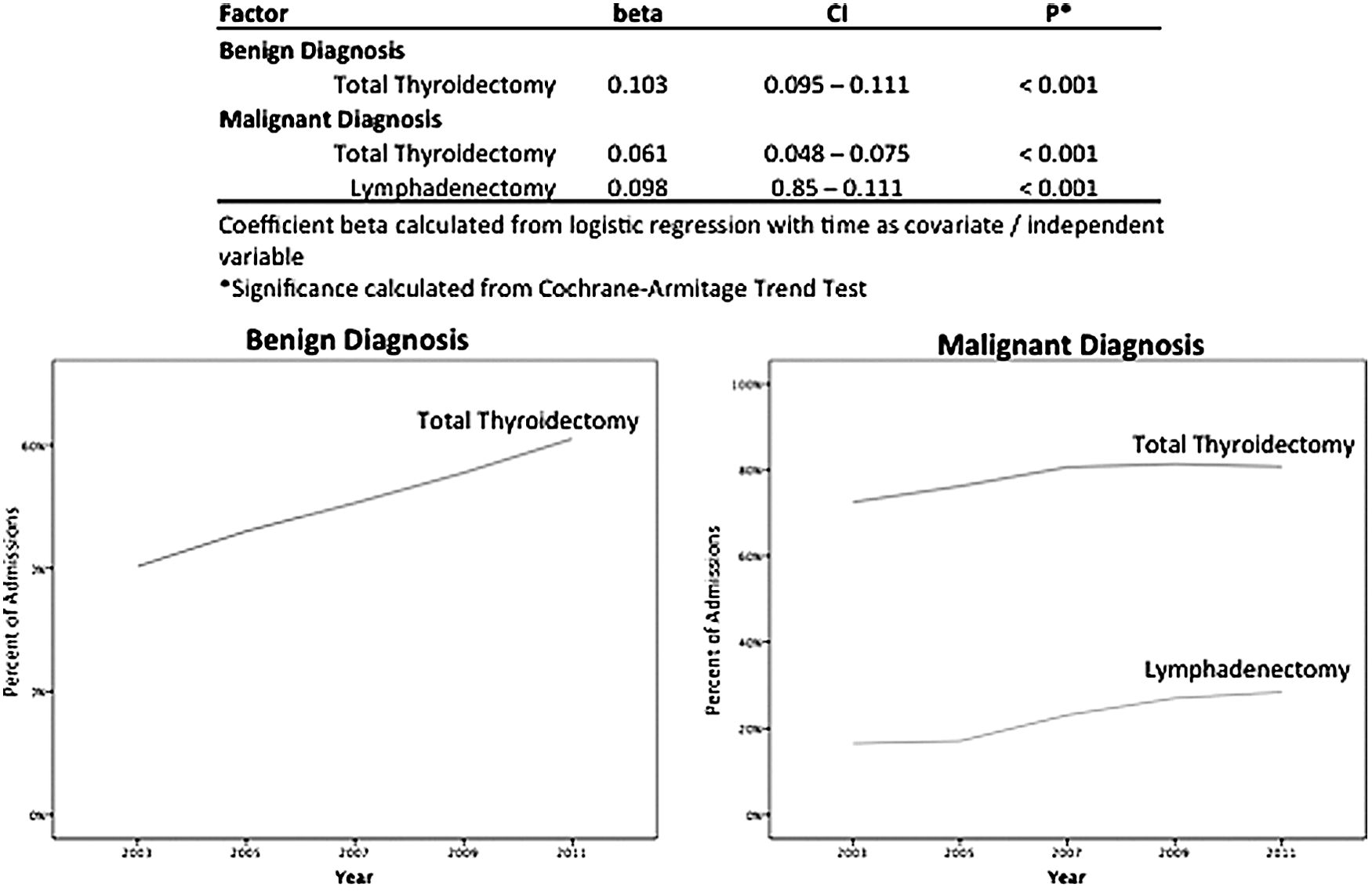
Trends in the use of total thyroidectomy and lymphadenectomy.
Discussion
U.S. healthcare is under considerable economic pressure due to concern that increases in federal spending on healthcare are outpacing increases in gross domestic product (18). Identifying areas of rising cost and potential drivers of these increases may help efforts to improve the financial sustainability of the healthcare system. The present analysis of NIS data suggests the total and mean cost of hospitalization following thyroid lobectomy and total thyroidectomy increased dramatically from 2003 to 2011. Using multivariate analysis, it was demonstrated that higher DRG severity of illness score, total thyroidectomy, lymphadenectomy, western region, rural region, and the occurrence of certain postoperative complications are highly associated with higher inpatient costs. Socioeconomic status, age, hospital teaching status, and hospital size did not demonstrate consistent associations with increased cost. Of the high-cost associated factors, trend analysis demonstrated that increases in the proportion of admissions with higher comorbidity score, following total thyroidectomy, and thyroidectomy with lymphadenectomy were likely major contributors to the observed increase in inpatient costs. Rates of postoperative complication and changes in the geographic distribution of thyroid surgery did not appear to be contributing to rising costs.
These observations describe a sicker population of inpatients undergoing a higher percentage of total thyroidectomies and lymphadenectomies. This is likely the result of recent trends to perform outpatient thyroid surgery on healthy patients with benign disease. These results are similar to a recent study by Sun et al. (5) who found a nationwide increase in per capita charges for inpatient thyroidectomies from 1996 to 2006. Their study showed that although there was in increase in inpatient thyroidectomy, a more significant rise in outpatient thyroidectomy has occurred over this time frame. Consistent with the present findings, which only included inpatient surgery, the percentage of procedures performed for a diagnosis of malignant thyroid neoplasm had markedly increased in the inpatient setting, with the inverse trend seen with outpatient surgery.
The shift toward outpatient thyroidectomy has been demonstrated to decrease overall costs associated with thyroid surgery, and has been embraced throughout the United States as a means of reducing healthcare costs. Multiple studies support that this is generally safe for healthy patients with benign disease (3,19). A recent comparison of overnight versus same-day discharge of thyroid surgery patients has shown that same-day discharge results in significant decreases in cost independent of the type of procedure performed, while being of comparable safety (6,20). The increase in inpatient costs of thyroid surgery that were observed could be attributed to cost savings from performing outpatient surgery on low-risk patients.
The incidence of thyroid cancer has dramatically increased over the past four decades, and the overall cost of caring for patients with thyroid disease is expected to rise as a result (20). A recent study estimated the U.S. national cost of care for well-differentiated thyroid cancer in 2013 to exceed $1.6 billion, with 41% of this cost attributed to initial treatment including work-up, surgery, and radioactive iodine, with significant increases expected in the coming years (9). The effects of malignancy on cost are seen in the present study through the independent association of a malignant diagnosis with higher hospital costs and the independent associations of total thyroidectomy with high hospital costs, which are more often performed for malignancy. The most dramatic increase was seen in the number of total thyroidectomies performed on patients with a preoperative diagnosis of benign disease. Given the cost implications of these changing practice patterns, their effect on clinical outcomes should be further researched to determine whether they are cost-effective.
Postoperative complications were observed to be associated with higher inpatient costs. However, the frequency of these complications was relatively low, and these associations were not shown to be statistically significant for postoperative hypocalcemia and wound infection. Postoperative hemorrhage and “other procedural complication” were highly associated with increased costs over the studied years. However, trend analysis did not demonstrate that they likely contributed to rising costs.
As with similar studies that have used hospital discharge data from the NIS database, this study has a number of limitations (2,4,21). Unaccounted confounders may be present, though a large number of relevant variables have been included from the NIS data sets. Factors relating to surgeon and hospital volume were not included, however, as this could not be accurately captured with the NIS data set, but could account for the observed geographic trends in this study. The coding of certain data points in the NIS database may not accurately represent certain clinical scenarios. This database does not provide details regarding central/lateral neck dissection in thyroidectomy, preventing a detailed analysis of the role of lymphadenectomy as a factor influencing cost. The NIS database also lacks information regarding hospital readmission and whether patients had previous surgery and/or radioactive iodine treatment. This could introduce bias in cost analyses regarding LOS, extent of surgery, and perioperative complications. Postoperative complications not charted at discharge may not be linked with thyroid surgery in the data set and could be underreported. In addition, the severity of complications is not accounted for in the data set.
Limitations specific to the diagnosis of thyroid nodules could also alter the interpretation of this study. For instance, some thyroid nodules coded as benign based on preoperative cytological classification will have a diagnosis of thyroid cancer following discharge. The current data set cannot account for this limitation. In addition, nodal disease in thyroid cancer was more likely to be identified in 2011 compared with 2003, given advancements in imaging during this period. Lastly, this study does not have a control surgical procedure for comparison of cost trends. Therefore, rising costs of hospitalization following thyroid surgery may represent an overall trend in cost reporting rather than a trend specific to thyroid surgery.
To the authors' knowledge, this is the first study to investigate drivers of hospital cost following inpatient thyroid surgery and to implicate certain factors as likely contributing to an observed dramatic cost increase from 2003 to 2011. Continued increases in the proportion of sicker patients and the rate of malignancy are likely to continue driving hospital costs higher. The clinical implications of the increasing use of total thyroidectomy and lymphadenectomy should be further examined, as this may present an opportunity to limit further cost increases.
Footnotes
Acknowledgments
This project was supported in part by the National Center for Advancing Translational Sciences, National Institutes of Health, through grant number UL1 TR 000002.
Author Disclosure Statement
No competing financial interests exist.