
Abstract
Background:
Renal cell carcinoma can metastasize to uncommon sites, for example, the thyroid gland where metastases are rarely found. To determine the patient survival and the time between cancer diagnosis and thyroid metastasis, we analyzed a large patient cohort from our hospital records and performed a systematic review.
Patients and Methods:
Patients diagnosed between 1978 and 2007 with thyroid metastases from renal cell carcinoma were retrospectively identified from the hospital database. A systematic literature search was performed for publications describing at least three cases of thyroid metastasis from renal cell carcinoma. Case data from the identified studies were collected and used to determine the survival data.
Results:
We identified 34 patients (19 females) from our hospital records with a mean age of 67 years (range, 33–79) when thyroid metastasis was diagnosed. Median time to primary metastasis after resection of renal cell carcinoma was 6.5 years (range, 0–25) with a single case of synchronous metastasis. Median survival after primary metastasis was 4.7 years (95% confidence interval [CI]: 1.8–7.6). The systematic review included 32 studies with 285 patients. Case data could be extracted for 202 patients. Median time to thyroid metastasis (without synchronous cases) was 8.8 years (95% CI: 7.5–10.1). Median actuarial survival after thyroid metastasis was 3.4 years (95% CI: 2.2–4.6). Total thyroidectomy was not associated with a better survival compared to partial thyroidectomies.
Conclusions:
Time to thyroid metastasis of renal cell carcinoma can be very long, and survival after thyroidectomy is favorable compared to metastasis to other sites.
Introduction
R
Although the thyroid gland is extremely well perfused, it is a rare site of clinically relevant metastatic disease (9). Only 2–3% of thyroid malignancies are of metastatic origin. Nevertheless, in autopsy studies microscopic metastases can be found in 4–24% of thyroid glands (3,10) and commonly originate from breast, lung, skin, renal, and gastrointestinal carcinomas (9,11). If the renal cell carcinoma metastases are confined to the thyroid gland, thyroidectomy can prolong the overall survival but does not cure the disease. Most of these patients die from disseminated disease (8,11,12) with an estimated 5-year survival rate of approximately 50%.
Because thyroid metastases of renal cell carcinomas are extremely rare, little is known about the time to metastasis and the overall survival. There are many case reports, however one has to assume that they are biased toward long survival times (13). Most of the case series report fewer than 20 patients with the exception of two studies reporting 36 and 37 cases (11,14). Thus, we reviewed our patient database for patients with renal cell carcinoma metastasis to the thyroid gland covering a 29-year period and compared our results with published data from case series. By combining the data, we are able to present survival data based on 236 case data.
Materials and Methods
Patients
All patients with thyroid metastasis after total nephrectomy for primary renal cell carcinoma performed between January 1978 and December 2007 were identified from the patient databases of the Department of Surgery and Department of Urology at the University Hospital Heidelberg, Germany. Only patients with thyroid metastases with histologically proven origin from renal cell carcinoma were included in the study. Patients with papillary, follicular, medullary, or anaplastic thyroid cancer were not included.
Metastases diagnosed within 1 month of primary diagnosis of renal cell carcinoma were considered synchronous metastases.
The demographic and clinical variables, including age, sex, type of thyroid surgery, mortality, and course of tumor and metastasis progression were extracted from the databases. Patients had regular follow-up visits at the university's outpatient clinic.
Literature search for systematic review
A structured MEDLINE literature search for case series reports on thyroid metastasis from renal cell carcinoma was performed independently by two investigators (Beutner and Bork). In May 2014 the PubMed database was searched using the following search string: (“Carcinoma, Renal Cell”[Mesh] OR “Kidney Neoplasms”[Mesh]) AND (“Thyroid Gland”[Mesh] OR “Thyroid Diseases”[Mesh] OR thyroid) AND (“Neoplasm Metastasis”[Mesh] OR metastasis OR metastases OR metastatic).
Based on the information in title and abstract, studies were selected for full text review. Only studies meeting the following criteria were included in the review: reporting at least three cases of renal cell carcinoma metastasis to the thyroid, reporting at least one of the following: time between renal cell carcinoma treatment and thyroid metastasis; survival or follow-up after thyroid resection; or survival or follow-up after kidney resection. Studies indicating the incidence of thyroid metastasis were included without systematically searching for these data. Finally, the reference lists of the reviewed studies were examined for articles not found by the PubMed search. Data extraction was performed by Beutner and verified by Lüthi. Summary data (count, mean, median, etc.) as well as single case data were extracted from the reports. Missing summary data were calculated from the case data if possible. For two studies (14,15) survival data were derived from Kaplan-Meier plots.
Time periods were calculated using the time of nephrectomy and thyroidectomy. If these data were missing, time of diagnosis of renal cell carcinoma or metastasis was used. Diagnoses of thyroid metastasis within 1 month after nephrectomy and cases in which thyroidectomy predated the diagnosis of renal cell carcinoma (to avoid negative time periods skewing the mean time between nephrectomy and thyroidectomy) were considered synchronous cases.
If the year of thyroid metastasis was not given, it was estimated based on observation period and duration of follow-up.
If several studies originated from the same institution, the latest report with the most data available was included. However, relevant data from earlier studies were considered for data extraction. Five studies originated from the Mayo Clinic, Rochester, Minnesota (16 –20); most of them did not report the time period covered or whether data had already been published. Thus, we excluded data from Czech et al. (16) and Smith et al. (19) from the systematic review, because it is reasonable to assume that they were reported by Ivy (17). Furthermore, two cases reported by Wychulis et al. (20) were most likely also reported by Ivy (17) and were excluded from the data of Ivy adjusting the summary data accordingly. Furthermore, three studies were excluded due to duplicate publication (21 –23).
Statistical analysis
All data were collected and summarized in Microsoft Excel 2010. Statistical analysis was performed with IBM SPSS Statistics version 20 (IBM, Armonk, NY) and R 2.12.1 (The R project for statistical computing, Vienna, Austria).
Time to thyroid metastasis was the time from primary nephrectomy to diagnosis of thyroid metastasis (if this information was missing in published studies, time of thyroidectomy was used). Survival data are overall survival data irrespective of cause of death. Median and mean survival and their 95% confidence intervals are based on Kaplan-Meier analysis performed in SPSS. Confidence intervals of relative annual survival were calculated using the “log” method in the R package “survival”.
Meta-analysis of the incidence data was performed with the R package “meta” using log (incidence) as effect size in a random effects model (DerSimonian-Laird).
Results
Patients from own hospital records
For this study 34 patients could be identified with renal cell carcinoma metastases in the thyroid gland. All patients underwent a nephrectomy at a median age of 55 years (range, 33–79) and 19 of the patients were females (56%) (Table 1 and 2 (second to last line)). For one patient metastasis was diagnosed at the same time as the renal cell carcinoma (T3M1), for all other patients metastases were diagnosed more than 1 month after renal cell carcinoma. Most patients had T3 renal cell carcinomas (n=16), only one was T1 and nine were T2; for the remaining eight no data were available (24). Median time from diagnosis of renal cell carcinoma to diagnosis of primary metastasis was 6.5 years (95% confidence interval [CI]: 5.4–11.5 years) and from renal cell carcinoma to diagnosis of thyroid metastasis was 8.0 years (95% CI: 5.7–12.2 years). In 22 patients location of primary metastasis was the thyroid (65%), of whom 9 patients (41%) had additional metastases to other organs at the time of primary diagnosis. All patients had histologically confirmed thyroid metastases of clear cell renal carcinoma.
Year estimated based on case descriptions or publication year.
Data from Mayo Clinic, Rochester, MN (possibly duplicate case reports).
Without 2 cases already published in Wychulis, 1964 (20).
Without 8 cases already published in Iesalnieks 2007 (33).
Patients–total, number of patients described in the study, including patients with metastases to locations other than thyroid; Patients–with thyroid met, number of patients with thyroid metastases; Case data, number of case descriptions with survival data; S, only summary data available; Centers: S, single center study, M, multicenter study; na, no data available.
Without two cases already published in Wychulis 1964 (20).
Estimate.
Without eight cases already published in Iesalnieks 2007 (33).
One case was 11 years after right renal cell carcinoma and synchronous to left renal cell carcinoma.
Sync, number of synchronous cases; time to metastasis w/o synchronous cases, cases diagnosed with thyroid metastasis within 1 month of renal cancer diagnosis were excluded; solitary, number of cases with solitary thyroid metastasis; TT, total thyroidectomy; HT, hemithyroidectomy; ST, subtotal thyroidectomy; DP, Dunhill procedure; other/any, either number of cases with other procedures than listed before (if type of procedure was indicated) or number of any thyroidectomies (not further specified in the report); n.d., no data given.
Treatment and survival
Renal cell carcinoma metastases to the thyroid were treated by curative thyroidectomy in 28 patients. Approximately half of these patients underwent total thyroidectomy, the remaining patients either had partial thyroidectomy or surgery data were not available (Table 2). Six patients were only treated with palliative intent, in one patient debulking surgery was performed while the other five had no thyroid resection (Table 2).
Median follow-up after primary diagnosis of metastasis was 2.8 years. At the end of the study 22 patients had died and 6 were lost to follow-up (Table 2). In 18 patients the renal cell carcinoma and its metastasis, respectively, could be identified as cause of death. Median overall survival after primary diagnosis of metastasis was 4.7 years (95% CI: 1.8–7.6) for all patients and 5.9 years (95% CI: 3.6–8.3) for patients with curative thyroidectomy. Median overall survival after primary treatment of renal cell carcinoma was 16.6 years (95% CI: 10.3–22.8) and there was no statistically significant difference between patients with curative and palliative thyroid metastasis treatment (p=0.64, hazard ratio [HR]=1.27, 95% CI 0.46–3.5).
Systematic review
The PubMed search identified 640 reports matching the query, and after review 32 reports could be identified fulfilling the inclusion criteria for this systematic review (Fig. 1). Seven studies were excluded because fewer than 3 cases of thyroid metastasis were reported and 4 studies were excluded because they were subsets of later reports (16,19,21 –23). In 2 cases, reports with overlapping case data were included, however, data from the later report with more data were adjusted by subtracting the already published cases (14,17). In total, the studies report on 285 patients with renal cell carcinoma metastasis to the thyroid and for 202 patients case data were available. The case data comprise 92 females, 84 males, and 60 patients without sex information (Table 1). Mean age at nephrectomy was 57 years and at thyroidectomy 65 years (Table 2). Mean age was independent of sex (nephrectomy: females, 55.8 years, males, 56.6 years, p=0.64; thyroidectomy: females, 65.1 years, males, 64.0, p=0.42, t test).
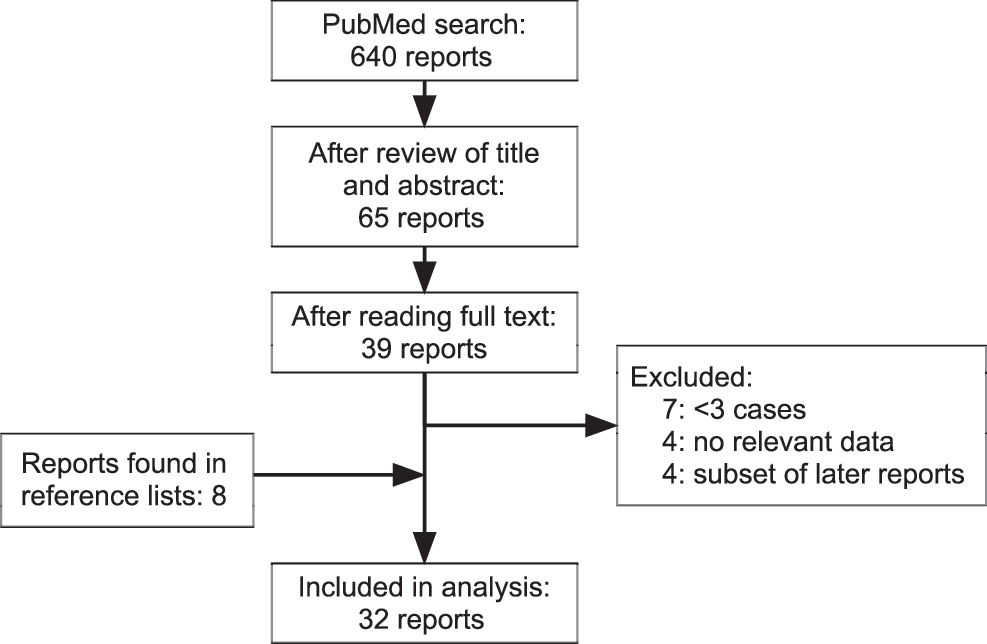
Flowchart of literature search for systematic review.
Twelve studies reported the incidence of thyroid metastases of renal cell carcinoma based on the number of thyroidectomies performed, and 13 studies based on the number of thyroid malignancies. The incidence based on thyroidectomies performed was 0.8 per 1000 thyroidectomies (95% CI: 0.6–1.2) and based on malignant thyroids 6.8 per 1000 (95% CI: 4.4–10.5), however, there was considerable heterogeneity between the analyzed studies (I2 around 70%) (Figs. 2 and 3).
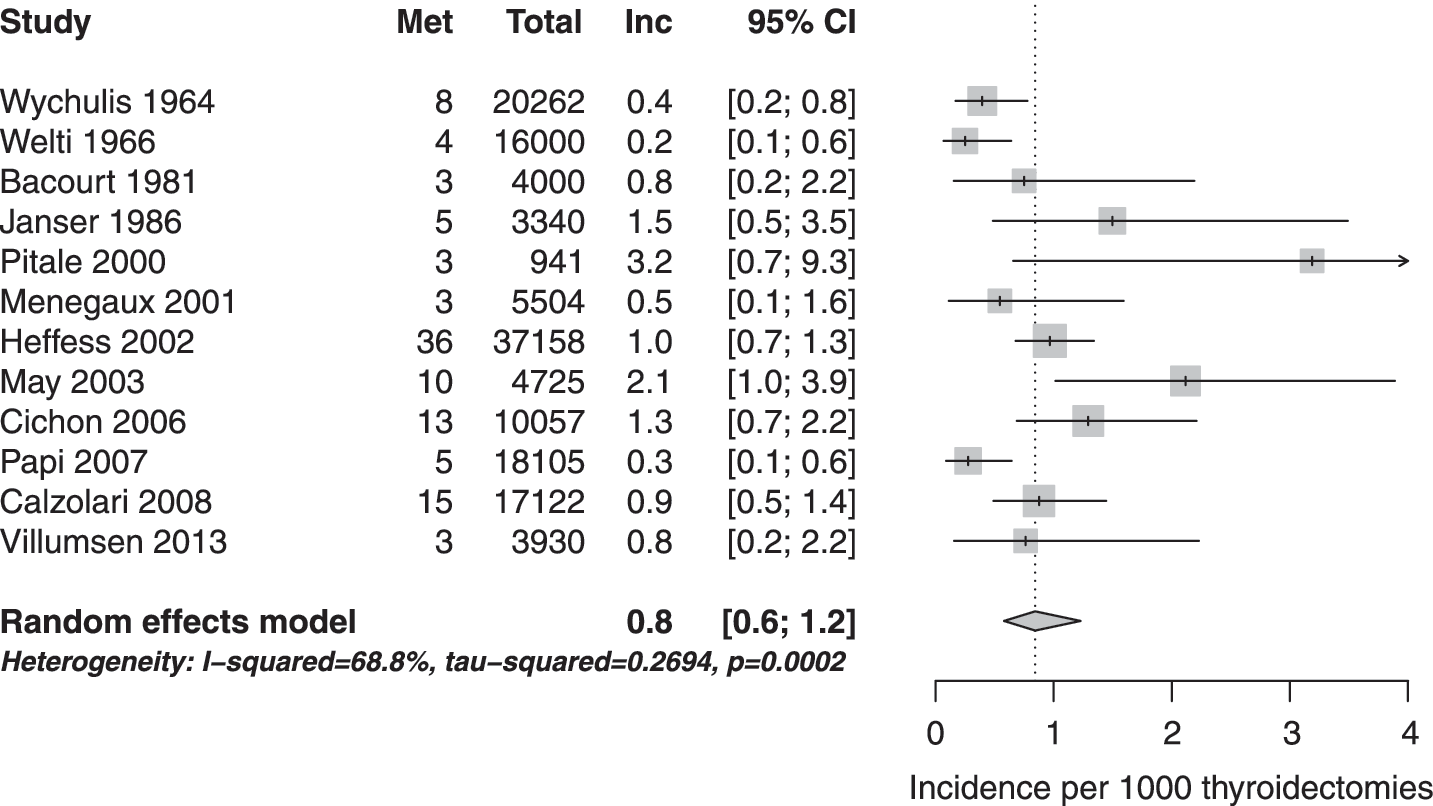
Forest plot: incidence of thyroid metastases per thyroidectomies. Incidence of thyroid metastasis from renal cell carcinoma per 1000 thyroidectomies. Met: patients with thyroid metastases (n=108), total: number of thyroidectomies (n=141,144), Inc: incidence per 1000 cases. 95% CI: 95% confidence interval. From Villumsen et al. (28) only cases from St. Olav's Hospital were included.
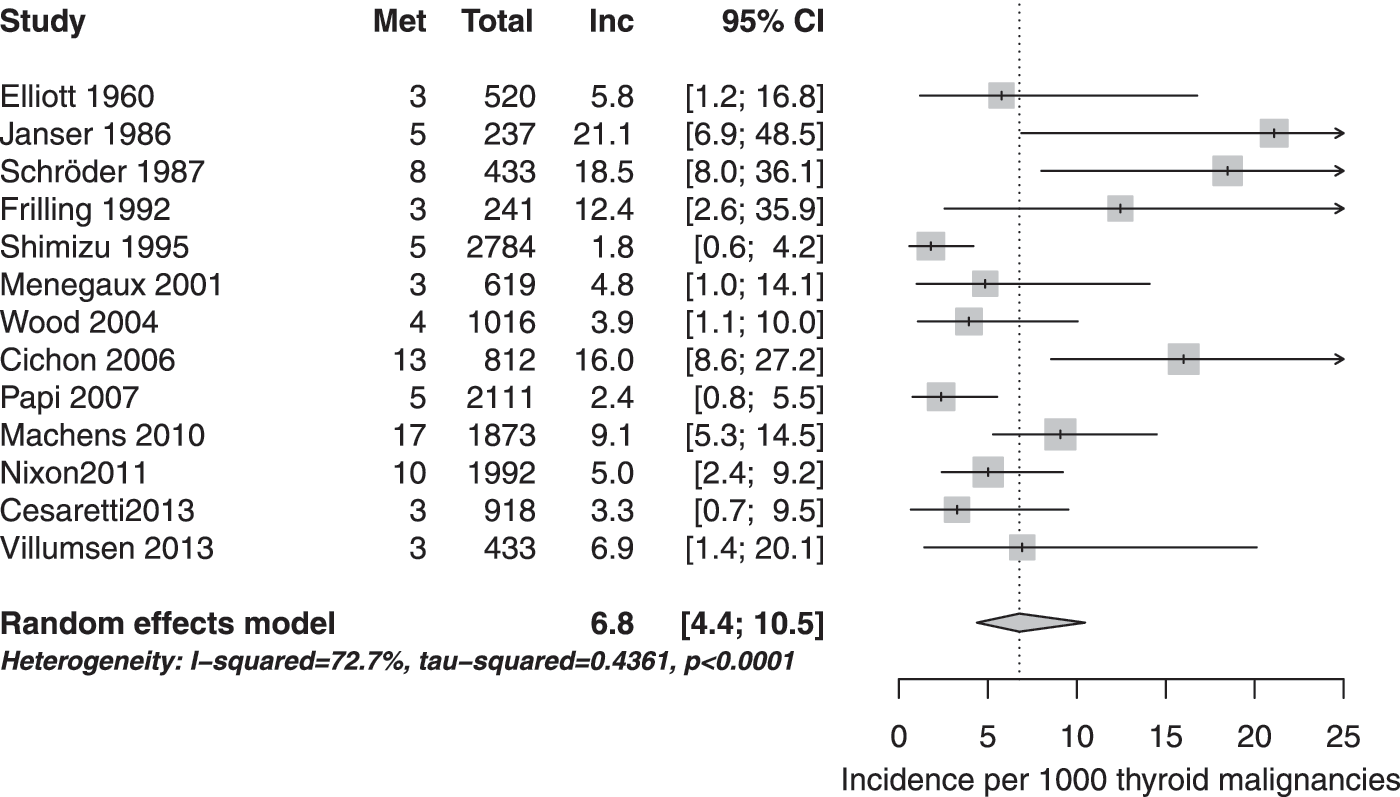
Forest plot: incidence of thyroid metastases per thyroid malignancy. Incidence of thyroid metastasis from renal cell carcinoma per 1000 thyroid malignancies. Met: patients with thyroid metastases (n=82), total: number of patients with thyroid malignancies (n=13,989), Inc: incidence per 1000 cases. 95% CI: 95% confidence interval. From Villumsen et al. (28) only cases from St. Olav's Hospital were included (Frilling et al. (54) is missing in Table 1, because the study did not provide survival data).
Time to thyroid metastasis did not differ significantly (p=0.164) between our patients' data and the case data of the systematic review (Fig. 4). Only the number of synchronous cases was clearly higher in the literature. Moreover, overall survival after thyroidectomy and nephrectomy did not differ significantly between our study and the collected case data (p=0.81 and p=0.30). Thus, for the remaining analyses we combined our data with data from the systematic review. Median time to thyroid metastasis was 7.0 years (95% CI: 5.3–8.7) and 8.8 years (95% CI: 7.5–10.1) if synchronous cases (<0.1 year) were excluded (Tables 3 and 4). However, in approximately 5% of the cases metastasis developed more than 18 years later. Median time to thyroid metastasis for females was 9.0 years and 8.0 years for males excluding synchronous cases (p=0.23, log rank test).

Time between nephrectomy and thyroid metastasis. Kaplan-Meier plot of the time to thyroid metastasis for all case data retrieved from the literature (solid line) and the patient data from this study (black dotted gray line). Dashed lines indicate 95% confidence intervals for case data from the literature.
Shorter survival after nephrectomy than after thyroidectomy due to a case of nephrectomy 3 years after thyroidectomy.
Without 2 cases already published in Wychulis 1964 (20).
Estimate.
Without 8 cases already published in Iesalnieks 2007 (33).
Based on data from dead patients (follow-up data of surviving patients not given).
Survival data in years calculated from case data or survival curves. Values given in the publications are marked with ‡.
Simple, standard median and mean of time to last contact or death; actuarial, Kaplan-Meier estimate of survival; nr, not reached, data were not sufficient to calculate the mean or median survival.
Time to event data for time from nephrectomy to thyroid metastasis based on the collected case data.
Mean and median from Kaplan-Meier analysis, N total number of cases. Lower part percent metastasis free after n years, N: patients at risk after n years.
Right part: data excluding synchronous cases (time to metastasis <0.1 years)
95% CI: 95% confidence interval.
Median overall survival after thyroidectomy was 3.4 years (95% CI: 2.2–4.6) and after nephrectomy 14.5 years (95% CI: 12.4–16.6; Tables 3 and 5; Fig. 5). Median overall survival after thyroidectomy and after nephrectomy was significantly better for females (5.0 years and 15.5 years) than for males (2.0 years and 12.1 years, p=0.003 and p=0.007).
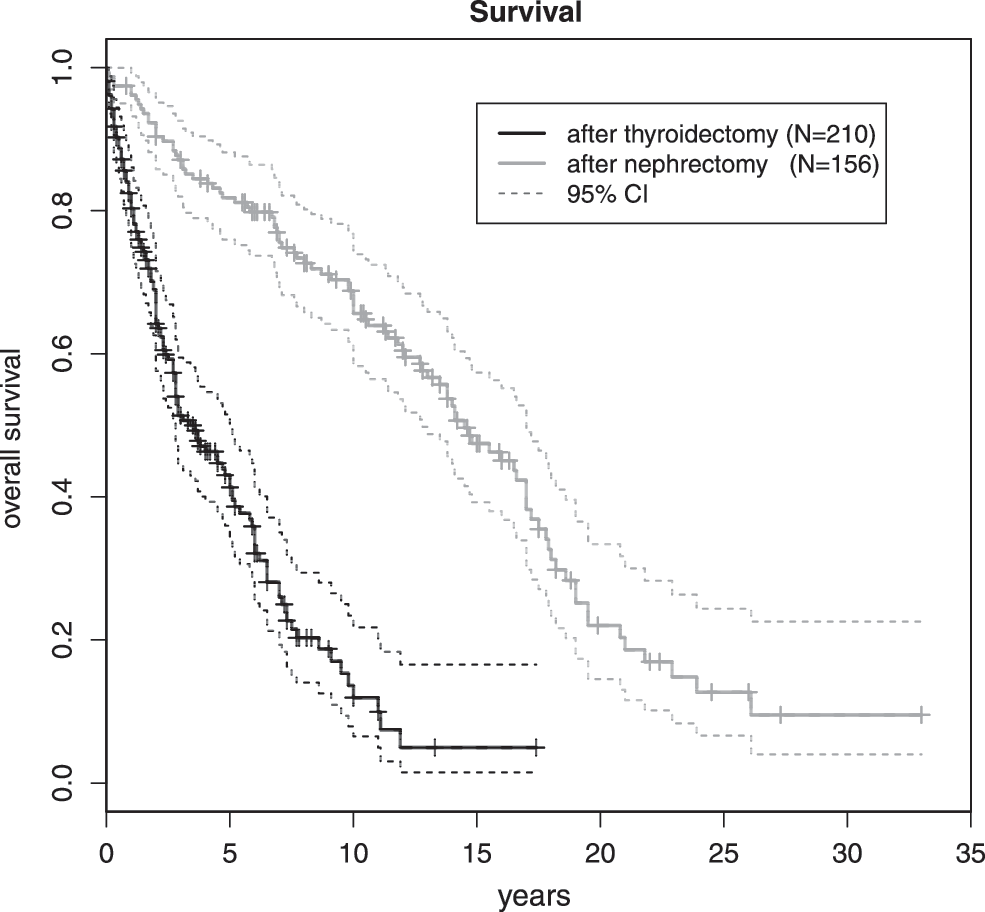
Overall survival. Overall survival after thyroidectomy (black) and after nephrectomy (gray) for all data (literature and this study combined). Dashed lines indicate 95% confidence intervals. Vertical marks indicate censored data. For detailed survival data see Table 5.
Overall survival after thyroidectomy or nephrectomy based on collected case data.
Mean and median from Kaplan-Meier analysis, N total number of cases.
Lower part: Survival after n years. N, patients at risk; E, number of events (i.e., death); 95% CI: 95% confidence interval.
Overall survival after thyroidectomy was independent of the type of surgery. Survival after total thyroidectomy did not differ from the survival after any partial thyroidectomy (HR=0.86, p=0.49; Fig. 6). Males had some survival advantage after total thyroidectomy (HR=0.55, p=0.095) without reaching statistical significance. In females no relevant difference could be observed (HR=1.29, p=0.49).
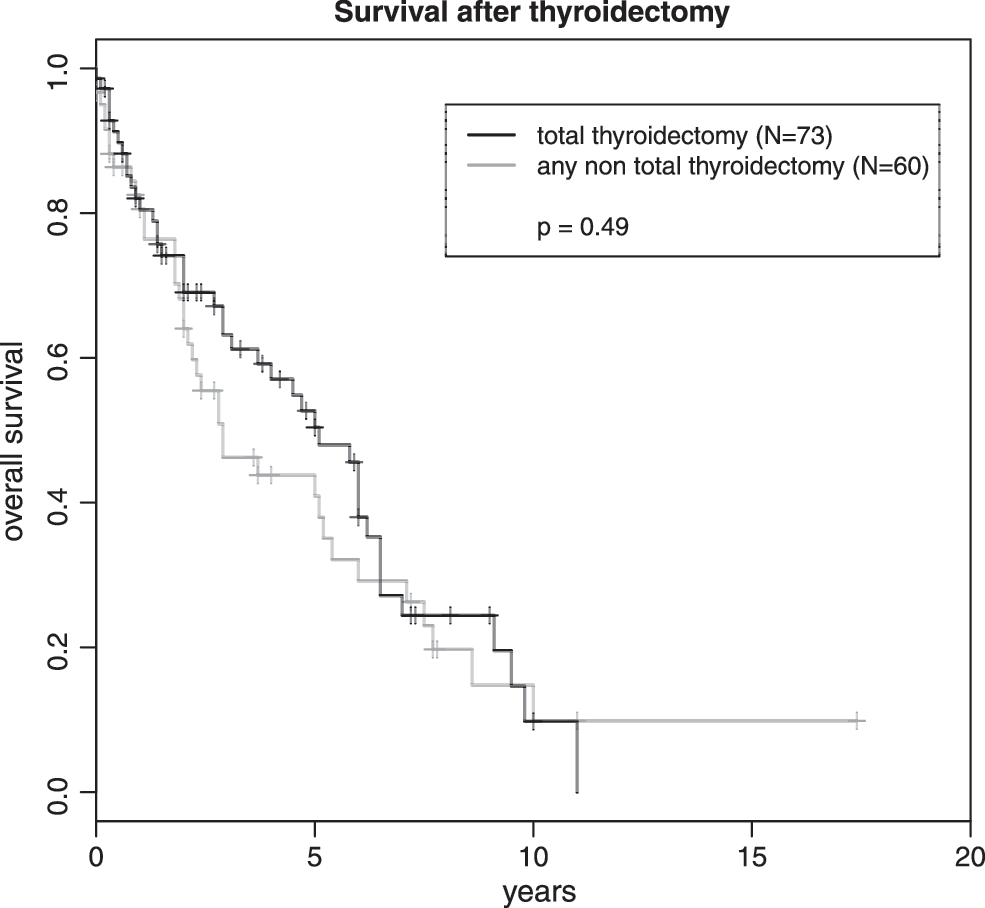
Overall survival and type of thyroidectomy. Overall survival after total thyroidectomy (black line) and any other nontotal thyroidectomy (gray line). Vertical marks indicate censored data.
During the long observation period of this systematic review no improvement with respect to time of survival after thyroidectomy could be observed. However, if case data were divided into quartiles according to the year of thyroid metastasis, time to thyroid metastasis significantly improved in the last quartile (diagnosis after the year 2000, p=0.01; Fig. 7). However, the rate of synchronous cases in the first two quartiles was considerably higher. To exclude this bias in favor of the recent cases, all cases with less than a month between nephrectomy and diagnosis of thyroid metastasis were omitted from further analysis. After excluding synchronous cases, statistical significance was lost (p=0.067) comparing all four quartiles. However, if patients with thyroidectomy up to the year 2000 are compared with patients operated after 2000, the difference was significant again (p=0.009). The median time to thyroid metastasis was 7.6 years (95% CI: 4.8–10.3) for patients with thyroid metastasis diagnosis up to 2000 and 11.0 years (95% CI: 8.3–13.7) after 2000. Because overall survival after thyroidectomy did not improve over the observation period, overall survival after kidney resection improved due to the longer time to thyroid metastasis.
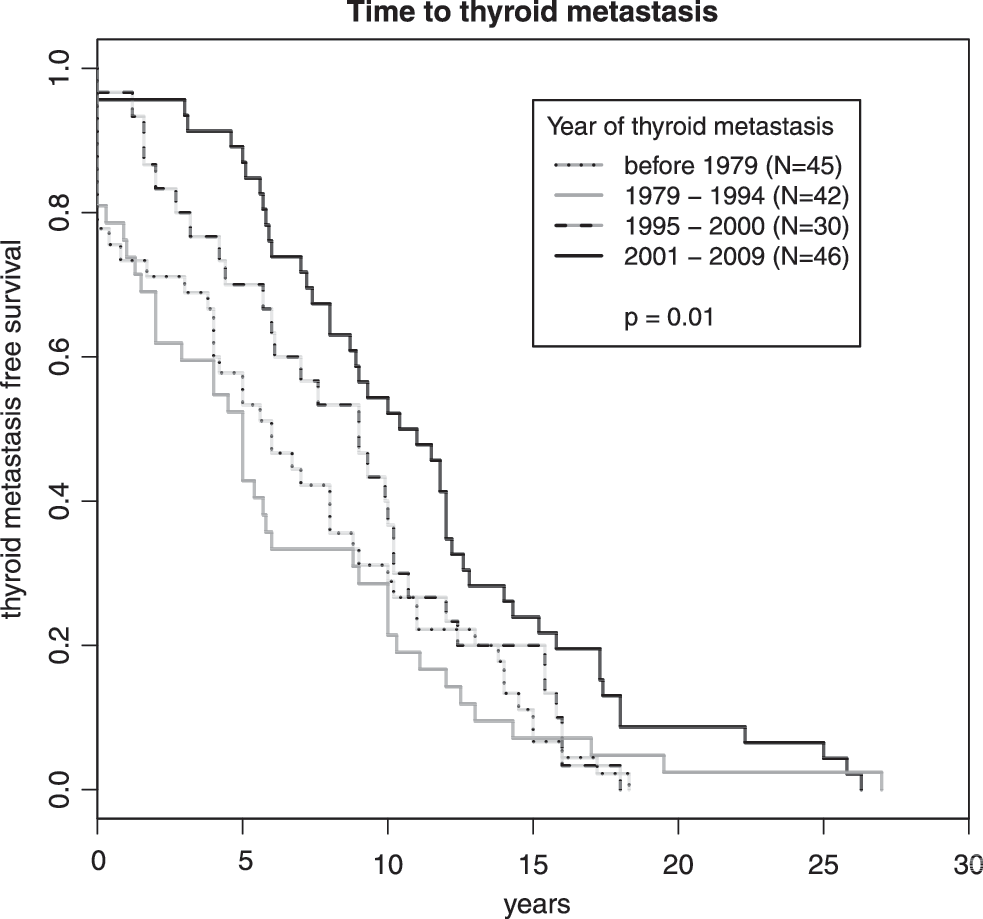
Time to thyroid metastasis during different periods. Case data from the literature and this study were divided in four approximately equally sized cohorts according to the year of thyroid metastasis. p value is for comparison of all four cohorts. Because earlier studies had more synchronous cases, results could be biased. Excluding synchronous cases (Δt≤0.1 years) p=0.067. Comparing only cases before and after December 2000: p=0.002 (all cases), p=0.009 (synchronous cases excluded). There were 17 cases alone in 2001 resulting in the unequal distribution in the last two periods.
Discussion
We could identify 34 patients with metastatic renal cell carcinoma to the thyroid from our database. This is the largest case series from a single center so far and only two other series reported more than 30 patients (11,14). Median time to thyroid metastasis after nephrectomy was 6.5 years and overall survival after thyroidectomy 4.7 years. The systematic review of the literature resulted in the identification of 32 studies reporting on 285 patients with survival data comparable to our study.
The median time to thyroid metastasis varies considerably in the literature ranging from 5 (17) to 10.3 years (14) for the larger case series. The median time to thyroid metastasis of our patients seems to be rather short in comparison, however some studies did not include synchronous cases. Our data remain within the 95% confidence interval from the collected case data of the systematic review. The overall survival times in our study did not differ significantly from other recent studies with comparable patient numbers.
In our patient population as well as in the patients collected from the systematic review data, males have a significantly shorter survival than females. Most likely this is due to the high age at which thyroid metastases are diagnosed and the shorter life expectancy of males (analysis was not age adjusted). On the other hand, in a similar study by Iesalnieks et al. (14) no sex difference in survival could be identified. Furthermore, survival after renal cell carcinoma metastasis to any location is better in males than in females (25,26), probably because metastasis to common sites occurs much earlier and thus at a lower age.
Some studies indicated that thyroid metastasis from renal cell carcinoma are more common in females than in males (11,13,27,28). This would support the hypothesis that thyroid metastasis requires a somehow diseased thyroid, which occurs more commonly in females. However, we could not observe a sex imbalance neither in our data nor in the summarized data. Actually, the number of males and females are virtually identical.
In 2008 Ieasalnieks et al. (14) reported a striking correlation between thyroid and pancreatic metastasis of renal cell carcinoma (31%) that had not been observed before. In our cohort, 11 patients (32%) developed pancreatic metastases as well. The incidence of pancreatic metastasis after nephrectomy of renal cell carcinoma is approximately 0.26% (29). Thus a coincidence of 30% just by chance in two studies is highly unlikely. Why this has not been observed earlier is open to speculation. It could be the smaller patient numbers in other studies, a less thorough follow-up, or some local factors (both studies were performed in neighboring areas in Germany).
Because the focus of the systematic review was on overall survival and time to metastasis, we decided to include only studies with at least three cases because we expected considerable bias including single or dual case reports. It is reasonable to assume that predominantly case reports with extreme survival or time to metastasis data are getting published thus skewing the results to longer time periods. Furthermore, a detailed review including case data has recently been published (13).
If several studies shared case data, we selected the study including all previous data for the systematic review. However, for some case series no study could be found to include them all together. For these studies, we opted for an unusual approach, to include some “duplicate” studies in the review, but adjusted the results of the later studies by removing cases already published to obtain the most comprehensive data collection possible without duplicates. Thus, data in the systematic review might differ from the published data.
Twenty studies provided data on the incidence of thyroid metastasis after renal cell carcinoma. Based on meta-analysis one can expect somewhat less than 1 thyroid metastasis per 1000 thyroidectomies and approximately 7 per 1000 thyroid malignancies. These are very rare cases in clinical practice, however, in the case of a history of renal cell carcinoma this potential diagnosis should be considered.
Most studies reported the time after thyroidectomy as follow-up time; rarely the actuarial survival data from Kaplan-Meier analysis was reported. However, most studies reported the survival data for each case allowing a Kaplan-Meier analysis per study (Table 5), as well as for all cases together. In total, we could collect 202 case descriptions from the literature; including the cases from this study, the case collection encompassed 236 patients. However, many of these data sets were incomplete, most notably the study by Iesalnieks et al. (14) for which only survival data after metastasis could be obtained from a Kaplan-Meier plot (35 cases).
Without synchronous cases, the median time to thyroid metastasis was 8.8 years based on 152 cases. In another recent meta-analysis the mean time to metastasis was estimated to be 8.8 years for 79 cases (13). Although that review also included single case reports, the time to metastasis is virtually identical. Similar results were obtained by the studies with the largest patient cohorts: median 10.3 years for 41 patients (14) or mean 9.4 years for 36 patients (11). Median overall survival after thyroidectomy was 3.4 years for 210 cases in this review and 5.2 years in the review by Sindoni et al. (13) that included 60 cases. This discrepancy is most likely due to the many single case reports included by Sindoni et al. (13), slightly overestimating the survival. In comparison, approximately half of studies in this review reported median survival times after thyroidectomy of less than 3 years.
Median survival after nephrectomy was 14.5 years for 156 patients in this review. In the study by Sindoni et al. (13), the overall survival after nephrectomy was not addressed, but again our data are comparable to the data from large studies such as the one by Heffess et al. (11) with a median survival of 12.3 years.
Median survival after any metastasis of renal cell carcinoma ranges from 1 to 2.3 years in recent studies (25,26,30,31). Thus, median survival after thyroid metastasis is clearly longer with 3.4 years found in the systematic review. Data for the 5-year survival rates after nephrectomy for renal cell carcinoma vary considerably in the literature from 15% to 82% (25,26,32). The 82% based on the systematic review are quite favorable. Kavolius et al. (25) had already noticed in 1998 that overall survival after renal cell carcinoma was better when metastasis was restricted to glands (thyroid, salivary gland, pancreas etc.). The 5-year survival rate was 63% compared to 44% overall (25). Eggener et al. (29,30) developed a risk score to predict survival after renal cell carcinoma metastasis using three risk categories. Comparing the survival data after metastasis from the systematic review to the survival data from Eggener et al. (29,30), thyroid metastasis would be associated with a favorable to intermediate risk.
Several studies showed that time to (any) metastasis would be a positive predictor for survival (8,25,30). However, we could not observe such a correlation, neither in our patient cohort nor in the case data of the systematic review.
Although the observation period of the systematic review covers more than 70 years, we could not find any improvement in overall survival after thyroid metastasis. Only the time between nephrectomy and thyroid metastasis has improved somewhat in recent years. While this can be due to better adjuvant treatments, we suspect it is more likely due to the improved diagnostic possibilities. Renal cell carcinoma can be detected much earlier with modern imaging techniques. While thyroid metastasis repeatedly prompted a search for renal cell carcinoma in the early studies, in later studies metastasis never preceded diagnosis of renal cell carcinoma.
With an incidence of 0.74% of all thyroid malignancies and 0.06% of all renal cell carcinomas (30), thyroid metastasis of renal cell carcinoma is extremely rare. Time to metastasis is very long and overall survival is quite favorable compared to metastasis to other locations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.