
Abstract
Background:
Permanent hypoparathyroidism after total thyroidectomy is a rare but potentially serious iatrogenic complication. The aim of this study was to investigate the rate of recovery from postoperative, permanent hypoparathyroidism in patients undergoing thyroidectomy without parathyroid autotransplantation.
Methods:
This study was a prospective case series with a postoperative follow-up of up to 3 years. We enrolled patients with thyroid cancer who underwent total thyroidectomy with central compartment dissection, with or without lateral neck dissection, and who had postoperative permanent hypoparathyroidism, defined as serum levels of intact parathyroid hormone (PTH) <15 pg/mL for at least 1 year. In the postoperative follow-up period, the serum levels of PTH and calcium were measured regularly. Recovery from permanent hypoparathyroidism was defined as return to normal serum levels of PTH (15–65 pg/mL) and calcium (8.5–10.1 mg/dL) without calcium and/or vitamin D supplementation.
Results:
In the 1467 patients who underwent total thyroidectomy, 22 presented with permanent postoperative hypoparathyroidism. In 5 of these 22 patients, the PTH levels increased steadily and returned to normal in 27.6±2.9 months, after which supplementation of calcium and vitamin D could be discontinued.
Conclusions:
Although recovery from permanent hypoparathyroidism is rare, patients should be monitored for serum PTH levels so that unnecessary treatments such as calcium and vitamin D supplementation can be avoided.
Introduction
H
To prevent postoperative hypoparathyroidism following total thyroidectomy, the parathyroid glands may be preserved in situ, and/or the resected or devascularized parathyroid glands may be autotransplanted. Many reports have shown that parathyroid autotransplantation, which involves transplantation of the removed parathyroid glands after total thyroidectomy, reduces the incidence of permanent hypoparathyroidism (12 –15). According to the current understanding, recovery from permanent hypoparathyroidism resisting for one year after total thyroidectomy is impossible without parathyroid autotransplantation.
With this in mind, the aim of this study was to investigate the recovery of parathyroid function in patients with permanent hypoparathyroidism following total thyroidectomy without parathyroid autotransplantation.
Materials and Methods
Study design and patients
Between January and December 2011, thyroid cancer patients who underwent thyroidectomy at the Thyroid Cancer Center, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea, were considered for inclusion in this study. Of these, patients who had a history of thyroid surgery or radiotherapy or a benign condition were excluded. The remaining patients who underwent total thyroidectomy with ipsilateral central compartment node dissection with or without lateral neck dissection were monitored for hypoparathyroidism postoperatively for at least one year, and those with permanent hypoparathyroidism were included in the study. Patients undergoing parathyroid autotransplantation were not included in in this study as these patients all recovered normal parathyroid function within one year. All study patients were followed up for two to three years.
The Institutional Review Board of Gangnam Severance Hospital, Yonsei University College of Medicine (Seoul, Korea) approved this study. Owing to the retrospective nature of the study, neither patient approval nor informed consent was required.
Outcome measures
Permanent hypoparathyroidism was defined as serum levels of intact parathyroid hormone (PTH) <15 pg/mL for at least one year and a requirement for vitamin D and/or calcium supplementation to maintain normocalcemia persisting for at least one year after thyroidectomy. The serum levels of PTH were determined using a standard radioimmunoassay (Nichols Institute, San Clemente, CA; reference range, 15–65 pg/mL). Serum calcium levels (normal range, 8.5–10.1 mg/dL) were measured and corrected for albumin concentration (16). Postoperative symptomatic hypocalcemia was defined as serum calcium <8.5 mg/dL or the presence of any symptoms or signs of hypocalcemia, such as numbness and paresthesia of the fingertips, toes, or perioral area, and/or signs of tetany (e.g., Chvostek's or Trousseau's sign). Patients were prescribed dietary supplementation of vitamin D and/or calcium as needed. After discharge, the serum calcium and PTH levels were measured on postoperative days 10, 30, 60, 90, 180, and 360 and every 6 or 12 months thereafter in the outpatient clinic. After the PTH levels recovered to normal (15–65 pg/mL), dietary supplementation of vitamin D and/or calcium was suspended. The time for recovery from permanent hypoparathyroidism was defined as the time from initiation of vitamin D and/or calcium supplementation to the time when the serum calcium recovered to 8.5–10.1 mg/dL and the patient showed no signs or symptoms of hypocalcemia after calcium or vitamin D supplementation discontinuation.
Results
Of the 2396 patients who underwent thyroid operation at our hospital during the study period, 2169 patients were considered for inclusion in this study. Altogether, 227 patients were excluded because of a previous thyroid surgery or radiotherapy (103 patients) or a benign condition (124 patients). Of the remaining 2169 patients, 475 patients underwent partial thyroidectomy, while 1467 patients (67.6%) underwent total thyroidectomy; among these, 22 patients (1.01%) who experienced permanent postoperative hypoparathyroidism were included in this study.
The demographic and clinicopathologic characteristics of the 22 patients with permanent postoperative hypoparathyroidism analyzed are shown in Table 1. This group included more women (n=18) than men (n=4) and the mean age was 45.5±12.2 years (range, 22–77 years). The resected primary tumors were 1.02±0.78 cm in size, and 10 patients (45.4%) presented with multiple tumors. Seventeen patients (77.3%) had primary tumor lesions that were extrathyroidal extensions. None of the patients had distant metastases, such as lung, bone, or brain metastasis, but 13 patients (59.1%) had central compartment metastases, and 5 patients (22.7%) had lateral compartment metastases. Out of the 1467 patients who underwent total thyroidectomy, the proportion of patients who underwent removal of the inferior parathyroid was 37.9%, while the proportion of such cases in the 22 patients with permanent hypoparathyroidism was 68.2%. The mean number of removed parathyroid glands was 1.05±0.84. The mean number of harvested central nodes was 8.4±5.3. The 22 study patients were followed up for 32.4±3.0 months (range, 30–36 months), and 5 patients showed recovery of parathyroid function after a mean period of 27.6±2.9 months.
SD, standard deviation.
The changes in serum PTH levels were measured in each of the 22 patients with permanent postoperative hypoparathyroidism. All patients had a drop in the serum PTH levels that remained below normal for at least 1 year after total thyroidectomy. In 6 out of these 22 patients, the PTH levels returned to normal within the study period; however, one of these 6 patients was not classified as recovery due to continued serum hypocalcemia and a continued dependency on vitamin D supplementation (Fig. 1, solid line).
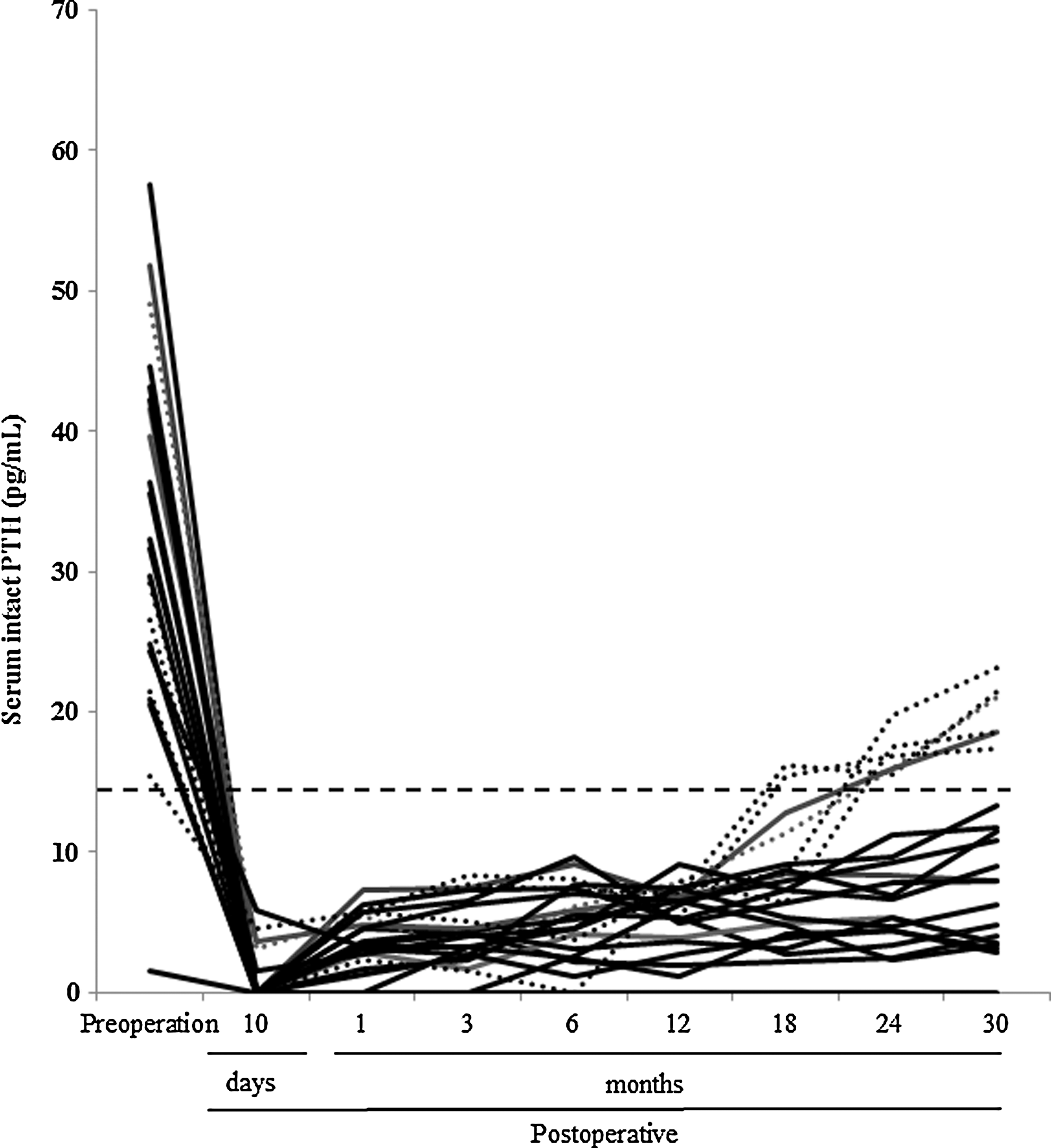
Chronological changes in intact parathyroid hormone (PTH) serum levels in patients with post-thyroidectomy hypoparathyroidism (n=22). The dotted lines represent data for patients in whom serum PTH levels returned to normal (n=5), while the continuous line represents data for the patient in whom calcium supplementation had to be resumed after recovery of serum PTH levels. The black horizontal dotted line represents the lower limit of the normal range of serum PTH levels (15 pg/mL).
In the other 5 patients, one patient recovered from the permanent hypoparathyroidism by 24 months after total thyroidectomy, while the remaining 4 patients recovered by 30 months (Table 2). Once the PTH levels were normal, the dietary supplementation of calcium and vitamin D was stopped in these 5 patients.
Normal serum parathyroid hormone (PTH) range, 15–65 pg/mL. The values highlighted in bold correspond to the period when calcium and vitamin D supplementation were no longer required by the patient.
Discussion
Hypoparathyroidism with hypocalcemia is a common complication associated with total thyroidectomy. In cases of thyroidectomy as a treatment for thyroid cancer, the rate of hypoparathyroidism is higher than that for benign conditions, likely owing to the need for central compartment node dissection with or without lateral neck dissection (5,17). In this study, all patients had thyroid cancer and underwent this type of total thyroidectomy. Although autotransplantation of parathyroid glands during total thyroidectomy can prevent postoperative hypoparathyroidism, this procedure was not performed in this study. Parathyroid function was monitored regularly in patients who presented with post-thyroidectomy hypoparathyroidism during a follow-up period of approximately 30 months; this is one of the few studies in which patients with this condition have been followed up for more than 2 years.
During thyroid surgery, the identification of the parathyroid glands is not always possible, and in cases of metastasis to the parathyroid glands, these glands also have to be resected. Moreover, various events can lead to parathyroid dysfunction, including trauma to, devascularization of, or inadvertent excision of the parathyroid glands. Even if the parathyroid glands are well preserved, PTH deficiency may still develop as a result of devascularization or atherosclerotic changes in the vessels supplying the parathyroid glands. To our knowledge, so far there are no studies evaluating patients in whom recovery of parathyroid function occurred more than a year after diagnosis.
Recovery from hypoparathyroidism in patients undergoing parathyroid autotransplantation is known to generally occur between 7 days and 1 month postoperatively (18). Conversely, in the present study, in the absence of autotransplantation, in 22 patients (approximately 1% of all total thyroidectomy patients included in this study), the PTH levels had not returned to normal at 1 year after total thyroidectomy. Of these, 2 patients recovered from hypoparathyroidism at 24 months, and 4 patients at 30 months, while the remaining 16 patients continued to have low PTH levels at 30 months. After the levels of PTH increased to the normal values, the supplementation of vitamin D and/or calcium was discontinued in 6 patients. However, vitamin D supplementation was resumed because of hypocalcemic symptoms in 1 of these 6 patients. Thus, the overall rate of recovery from hypoparathyroidism within 30 months was 22.7% (5/22 patients).
We hypothesize that the delayed recovery of parathyroid function observed in these 5 patients may have been due to the slow but steady recovery of blood flow via neovascularization occurring over the small surface area of the remaining parathyroid. In previous reports describing resection of the parathyroid glands followed by autotransplantation of 1 or 2 parathyroid glands, sliced into 1 mm×3 mm pieces and implanted into a separate muscle pocket in the sternocleidomastoid muscle (15,12,14), the autotransplanted parathyroid had a larger surface area for neovascularization than the preserved and not sliced parathyroid. The return of parathyroid function is generally observed within a month in patients with an autotransplanted parathyroid, while the patients in our study who recovered from hypoparathyroidism did so at least 24 months after the operation.
Another potential explanation for the delayed recovery of parathyroid function might be related to the central compartment node dissection. All patients in this study underwent total thyroidectomy with central compartment node dissection. Although we attempted to carefully preserve the branch of the artery and the vasculature in the parathyroid glands, devascularization of the parathyroid cannot be ruled out. Unlike autotransplantation of the parathyroid into a muscle with a good blood supply, neovascularization would occur slowly in devascularized parathyroid glands after central compartment node dissection, thereby delaying the recovery of parathyroid function.
There are also several potential mechanisms that could account for the role of exogenous PTH in the recovery of parathyroid cell function. Vitamin D and calcium are known to negatively regulate parathyroid function (19,20), and vitamin D and/or calcium supplementation after hypocalcemia may increase these inhibitory actions, resulting in the parathyroid recovery being impeded. In the natural history of hypoparathyroidism, the serum calcium does not fall upon reduction of the calcium supplement requirements, and the periods of hypocalcemia are relatively frequent. The remaining parathyroid tissue of such patients would have ample time to be stimulated by hypocalcemic events that inevitably must have occurred in their long history of true hypoparathyroidism.
In conclusion, the present study demonstrates that recovery from hypoparathyroidism secondary to total thyroidectomy may occur after two years after the initial diagnosis in patients not undergoing autotransplantation. Although this recovery from permanent hypoparathyroidism is relatively rare, the concerned patients should be monitored for recovery of parathyroid function so that unnecessary treatments, such as dietary supplementation of calcium and vitamin D, can be avoided.
Footnotes
Author Disclosure Statement
The authors declare that no competing financial interests exist.