
Abstract
Background:
Race/ethnicity may be a newly recognized risk factor for Graves' disease.
Objective:
The aim of this study was to examine the prevalence of thyrotoxicosis by race/ethnicity in Americans aged 12–49 years using three National Health and Nutritional Examination Surveys (NHANES).
Methods:
Data were analyzed from 17,939 participants in NHANES III (1988–1994), NHANES 1999–2002, and NHANES 2007–2010 with available thyroid function test results. Thyrotoxicosis was defined as a serum thyrotropin (TSH) of ≤0.1 mIU/L or subjects taking methimazole or propylthiouracil, and overt thyrotoxicosis was defined as high serum thyroxine and a serum TSH of ≤0.1 mIU/L. Logistic regression was performed accounting for the complex sampling design of NHANES, and the results from all three NHANES surveys were combined using a random-effects model.
Results:
There were 75 study participants with point prevalent thyrotoxicosis, representing a pooled prevalence of 0.4% for Americans aged 12–49 years. Prevalent thyrotoxicosis was nearly three times more likely in non-Hispanic black subjects compared with non-Hispanic whites (OR=2.9 [CI 1.5–5.7]), while there was no difference between the prevalence of thyrotoxicosis in Mexican Americans compared to non-Hispanic whites (OR=1.2 [CI 0.6–2.4]; I 2 for heterogeneity=0% for both). Among 27 patients with overt thyrotoxicosis, the odds ratio was 8.7 [CI 0.7–112.6] for non-Hispanic blacks and 4.6 [CI 0.4–59.3] for Mexican Americans compared with non-Hispanic whites.
Conclusions:
The results suggest there are race/ethnicity differences in the prevalence of thyrotoxicosis. Future studies should address whether these differences are due to heritable factors, environmental exposures, or a combination of both.
Introduction
G
Much is unknown about the risk factors for Graves' disease. Recently, our group showed that amongst U.S. active duty service personnel, the incidence of Graves' disease is more common in blacks and Asian-Pacific Islanders compared with whites (5). Because it is possible that those results reflect something specific to the military environment, the present study determined whether the same pattern of racial disparities in Graves' disease is seen amongst civilians. Data from three large cross-sectional surveys of the civilian non-institutionalized U.S. population (the National Health and Nutritional Examination Surveys [NHANES]) were used to document the prevalence of thyrotoxicosis (defined as a serum TSH ≤0.1 mIU/L or subjects taking methimazole or propylthiouracil) according to race/ethnicity. Because Graves' disease was not specifically reported in these studies, the prevalence of thyrotoxicosis in the population aged 12–49 years was used as a proxy for Graves' disease prevalence. In this age group, outside of special subpopulations (excluded from the analysis), thyrotoxicosis is rarely caused by anything other than Graves' disease (2 –4).
Methods
NHANES study design
The NHANES program is directed by the United States National Center for Health Statistics (6). Its objective is to generate representative health and nutritional information databanks that are freely available for public health research. Data were analyzed from NHANES III (1988–1994) (7), NHANES 1999–2002 (8,9), and NHANES 2007–2010 (10,11) because these surveys assessed thyroid function and could thus be used to determine the prevalence of thyrotoxicosis.
NHANES consists of stratified multistage probability sampling of the civilian noninstitutionalized U.S. population. Oversampling of certain population subsections is deliberately performed to provide adequate samples for data analysis. In NHANES III, young children, older people, non-Hispanic blacks, and Mexican Americans were oversampled (12). Similar oversampling occurred in 1999–2002 with the addition of low-income persons. In 2007–2010, adolescents were no longer oversampled, but all Hispanics were oversampled in addition to the groups previously mentioned (13). Data are collected in two stages. First, health interviews are conducted in participants' homes. Then health measurements (including laboratory collections) are undertaken in mobile examination centers. Of those people screened, 76–80% underwent the complete survey procedure (14). Raw survey data are weighted to population estimates by the National Center for Health Statistics to ensure nationally representative data.
Thyroid laboratory profiles were collected in NHANES participants aged ≥12 years in all three surveys. Subjects with missing TSH data were <10% of the planned sample, and NHANES analytic guidelines suggest that reweighting is probably unnecessary for this level of non-response (15). However, it was decided to reweight the data of those with available TSH measures for two reasons. The first reason was to ensure the analysis was consistent with Hollowell et al.'s classic NHANES study (16), which also reweighted subjects with available TSH data. Second, there were some sex, age decade, and race/ethnicity strata that had >10% missing TSH data. Because race/ethnicity was the focus of the study and the plan was to adjust for sex and age in secondary analyses, the samples were reweighted to ensure that they remained representative of the U.S. population using Lohr's method (17). Recognizing that other approaches to the issue of missing data are possible, the data were also reanalyzed using the original NHANES weights in sensitivity analyses (see Statistical Analysis) to confirm that the results were consistent across the original and reweighted data set.
Inclusion and exclusion criteria for analysis, and study population
Only those NHANES participants with available thyroid function test results aged between 12 and 49 years for whom any cause of thyrotoxicosis other than Graves' disease would be rare were included. Thus, pregnant women (with possible human chorionic gonadotropin-mediated physiological changes or thyrotoxicosis), women <12 months postpartum (with possible postpartum thyroiditis), and patients taking levothyroxine (with possible over-replacement) when specific medication usage was documented (NHANES 1999–2002 and NHANES 2007–2010); and patients taking any thyroid-related medication when medication usage was documented only as “thyroid/anti-thyroid medication” (NHANES III, thus excluding patients taking thyroid hormone replacement or anti-thyroid medication) were excluded.
Definition of race/ethnicity and data harmonization
The prevalence of thyrotoxicosis was analyzed in three self-reported racial groups: non-Hispanic whites, Mexican Americans, and non-Hispanic blacks. NHANES analytic guidelines suggest that sample sizes for non-Mexican American Hispanics, Asians, and Native Americans are too small for adequate estimation through the survey periods (13,18).
There were only minor differences in the definition of race/ethnicity from NHANES III and NHANES 1999–2002 to NHANES 2007–2010. In the earlier two surveys, non-Hispanics who indicated more than one race/ethnicity but then selected a predominant race/ethnicity (either white or black) were coded as non-Hispanic white or non-Hispanic black, respectively. In NHANES 2007–2010, participants self-identifying in this manner were coded as “other.”
Definitions of thyrotoxicosis and assays used
Where propylthiouracil or methimazole usage was documented in NHANES (NHANES 1999–2002 and NHANES 2007–2010), patients taking these medications were classified as thyrotoxic. If an individual had a suppressed serum TSH concentration (≤0.1 mIU/L), they were also considered to have thyrotoxicosis. This unambiguously low TSH cut-point was chosen because black people may have slightly lower normal TSH reference range compared with whites (16,19). As a secondary outcome, “overt” thyrotoxicosis was assessed, which was defined as serum TSH ≤0.1 mIU/L and serum thyroxine above the assay reference range. Note that total thyroxine was measured in NHANES III and free thyroxine was measured in NHANES 2007–2012. No overt thyrotoxicosis occurred in NHANES 1999–2002. Thus, this survey was omitted from this secondary analysis. Table 1 details the assays and their references ranges used for thyroid function testing in each NHANES survey.
NHANES, National Health and Nutrition Examination Survey; TSH, thyrotropin; T4, thyroxine.
Statistical analysis
The relationship between race/ethnicity and thyrotoxicosis was modeled using logistic regression and accounted for the complex sampling framework of NHANES. In combining NHANES surveys, two modeling approaches were used (20). In the primary analysis, a two-stage approach was employed whereby individual survey-specific effect estimates and standard errors for race/ethnicity were determined, and then combined using a random-effects model to generate an overall odds ratio (OR) and confidence interval (CI). The advantage of the two-stage model is that the analysis makes no assumptions about the homogeneity of results across the survey periods and can test for heterogeneity (20). In the secondary analysis, the three data sets were aggregated, and the relationship was assessed using a model that included a term for survey period. The value of this secondary approach lies in the ability to adjust for potential confounders in the setting of few events in each individual survey period, and is valid provided there is no heterogeneity in effects across studies (20). Aggregated, adjusted models were run controlling for sex, age, and cigarette smoking status (current smoker or nonsmoker). To explore the possibility that differential access to healthcare (leading to differing durations of thyrotoxicosis) between races/ethnicities biased the thyrotoxicosis prevalence estimates, sensitivity analyses were also performed using the two-stage approach in which all subjects with a known past history of thyroid disorders and those without medical insurance were excluded. Further sensitivity analyses were performed using the original NHANES subject weights, as well as on data sets excluding all subjects taking any medication that could be associated with a low TSH (glucocorticoids, octreotide, amiodarone, and lithium).
To assess the secondary outcome of overt thyrotoxicosis in NHANES III and NHANES 2007–2010, again logistic regression that accounted for the complex sampling framework of NHANES was performed.
The analyses were performed using SAS v9.3 (SAS Institute, Cary, NC) except for the random-effects models, which were performed in Stata v13.1 (StataCorp, College Station, TX).
Results
Data from 17,939 participants were analyzed across the three NHANES survey periods (10,558, 2663, and 4718, respectively). The characteristics of the included study population are detailed in Table 2. There were 75 (20 non-Hispanic white, 18 Mexican American, 29 non-Hispanic black, and eight other) people with prevalent thyrotoxicosis across all survey periods, representing a weighted total population thyrotoxic point prevalence of 0.3% [CI 0.2–0.4%] in 1988–1994, 0.2% [CI 0.0–0.5%] from 1999–2002, and 0.6% [CI 0.2–1.0%] from 2007–2010. Among the thyrotoxic cases, no subjects from 1999–2002 and one from 2007–2010 was taking methimazole or propylthiouracil, respectively. As noted above, patients taking antithyroid drugs were excluded from the NHANES III data set because they could not be separated from patients taking levothyroxine.
In the primary two-stage analysis, prevalent thyrotoxicosis was nearly three times more likely in non-Hispanic black subjects compared to non-Hispanic whites (OR=2.9 [CI 1.5–5.7]), while there was no difference between the prevalence of thyrotoxicosis in Mexican Americans compared to non-Hispanic whites (OR=1.2 [CI 0.6–2.4]; Fig. 1A and B). There was no heterogeneity in results across NHANES survey periods (p=0.4 for Mexican Americans vs. non-Hispanic whites, and p=0.8 for non-Hispanic blacks vs. non-Hispanic whites; I 2=0% for both). Table 3 details the percentage prevalence by race/ethnicity for thyrotoxicosis in each survey period.
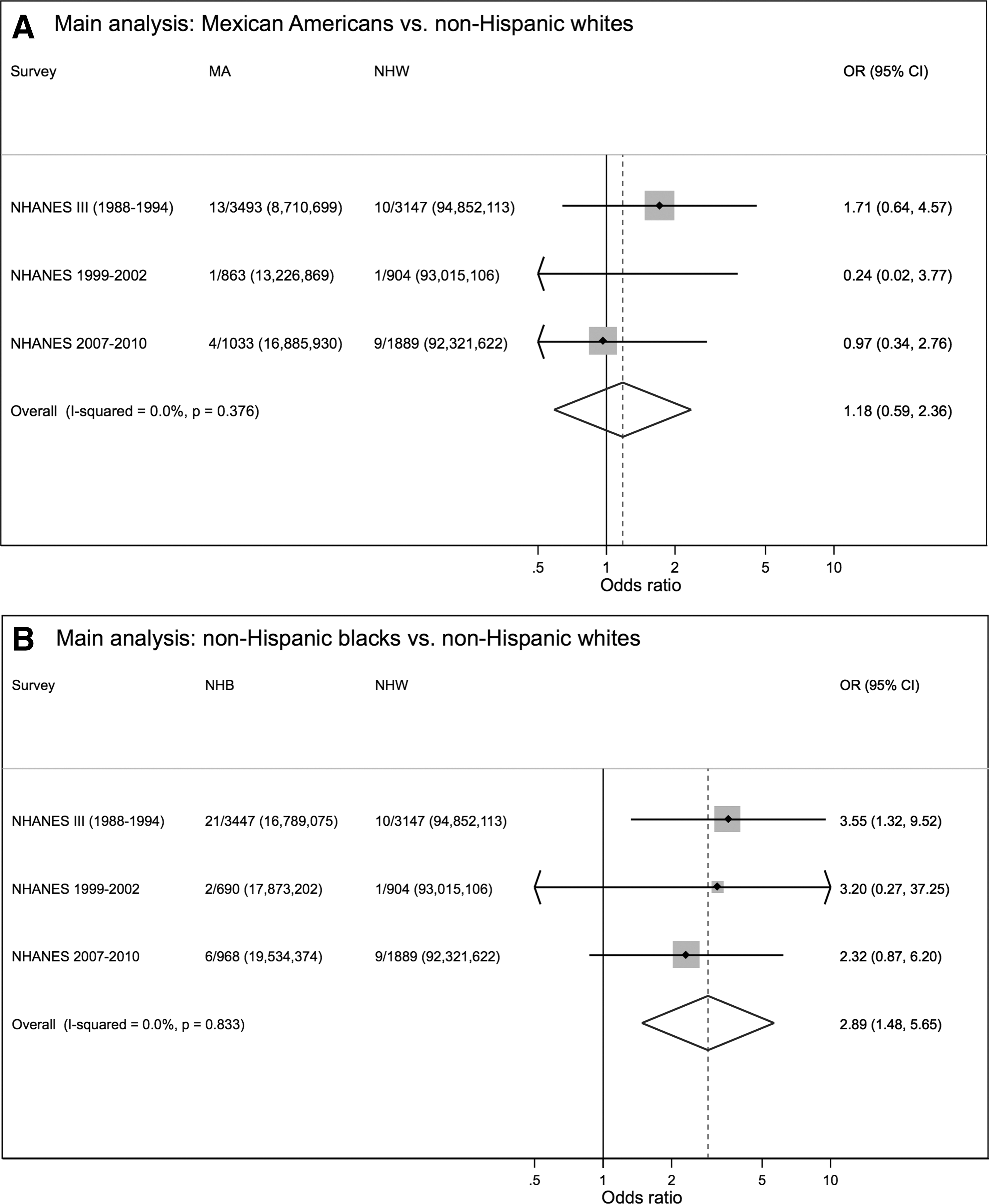
Two-stage, crude (main) analysis for thyrotoxicosis prevalence in (
CI, confidence interval.
The results obtained from models using the aggregate data were almost identical, even after adjusting for sex, age, and smoking status (Table 4). The results did not change after excluding subjects with known thyroid disorders, excluding those without medical insurance, reverting to the original NHANES weights, and excluding patients taking medications that can be associated with a low serum TSH (Table 4).
OR, odds ratio; ref, reference; meds, patients taking glucocorticoids, octreotide analogues, amiodarone, and lithium.
As expected, there were small numbers of subjects with prevalent overt thyrotoxicosis (five non-Hispanic white, eight Mexican American, 11 non-Hispanic blacks, and three other subjects, respectively). In the two-stage analysis, the odds ratio for overt thyrotoxicosis in non-Hispanic blacks compared with non-Hispanic whites was 8.7 [CI 0.7–113.6; p for heterogeneity=0.06; I 2=73%), while for Mexican Americans compared with non-Hispanic whites it was 4.6 [CI 0.4–59.3; p for heterogeneity=0.06; I 2=72%).
Discussion
This study demonstrates that in the civilian non-institutionalized U.S. population aged 12–49 years, non-Hispanic blacks have a higher prevalence of thyrotoxicosis compared to non-Hispanic whites, while the prevalence of thyrotoxicosis among Mexican Americans was not significantly different from non-Hispanic whites. These results are consistent with our group's recent work assessing the incidence of Graves' disease in the U.S. military (5). Because Graves' disease accounts for the vast majority of thyrotoxicosis in young adults (2 –4), together these studies argue for racial differences in the occurrence of Graves' disease. The previous study also found that Asian-Pacific Islanders had a Graves' disease incidence that was similar to blacks. Because of sample size constraints, it was not possible to examine this population in NHANES.
The strengths of this study include the use of data from the NHANES program with its objective measurement of disease prevalence across large, representative samples of noninstitutionalized civilian Americans. The relatively consistent data acquisition and coding also allowed harmonization of data sets across time periods. Combining data from multiple survey periods using pooled analysis principles (20) increased the number of subjects and events to be analyzed while allowing for rigorous inclusion criteria that increases the specificity of the diagnosis. The associations were consistent across all analyses, including two-stage and aggregated (crude and adjusted) models and those using the more stringent definition of overt thyrotoxicosis. The sensitivity analyses are reassuring that any disparities in access to healthcare or medication use did not affect the relative prevalence estimates by race/ethnicity.
The survey power in NHANES III to detect a difference in thyrotoxicosis prevalence between non-Hispanic blacks and whites was greatest, and likely explains its statistically significant individual survey result compared with the other surveys. NHANES III was by far the largest of the surveys (by number of years and total number of subjects). Furthermore, while minority groups were oversampled in all surveys to improve power, the oversampling of non-Hispanic black subjects occurred to a greater degree in the earliest survey. Thus, in NHANES III, 32.6% of participants aged 12–49 years were non-Hispanic blacks representing 12.7% of the population, compared with 25.9% of participants representing 12.7% of the 1999–2002 population, and 20.5% of participants representing 13.1% of the 2007–2010 population. The decision was made to summarize, analyze, and present all surveys testing thyroid function because this provided the most complete data set available, provided larger numbers of cases and subjects for the aggregate analyses, and allowed a quantitative evaluation of whether trends in thyrotoxicosis prevalence by race/ethnicity were consistent across the surveys. Despite the smaller numbers in NHANES 1999–2002 and 2007–2010, the results were consistent in direction and magnitude with NHANES III, which is reflected in the lack of heterogeneity and the I 2 statistic.
Two previous studies assessing NHANES data have reported on thyrotoxicosis and race/ethnicity. Hollowell et al.'s classic study analyzed NHANES III (16). In the population subset designated “disease-free” (those without known thyroid disease, goiter, or taking thyroid medication), 0.7% of the non-Hispanic black population were estimated to have thyrotoxicosis (TSH <0.1 mIU/L) compared with 0.3% of non-Hispanic whites. No measure of statistical significance was reported for that result. No analysis was performed for the prevalence of thyrotoxicosis by race/ethnicity across age groups. The “disease-free” population included participants of all ages and thus subjects at risk for all causes of thyrotoxicosis. As discussed above, younger patients were exclusively analyzed in our analysis to ensure higher specificity for Graves' disease as the cause of thyrotoxicosis. However, the results of Hollowell et al. including older subjects appear consistent with the data in the younger population. Aoki et al. performed multinomial logistic regression on data from NHANES 1999–2002 (21). Using TSH <0.4 mIU/L as the definition of thyrotoxicosis, the authors found that non-Hispanic blacks had a higher prevalence (OR=3.18 [CI 1.7–5.7]) compared with whites. This less specific definition was chosen because of very low case numbers in NHANES 1999–2002. It was possible that the results found by Aoki et al. could have been due to the slightly lower TSH distribution seen in black people (16,19), rather than a clinically significant phenomenon.
Few other studies in the literature address the issue of race/ethnicity differences in Graves' disease occurrence. A single previous paper from Johannesburg, South Africa, concluded that the incidence of hyperthyroidism was less common in the black population compared with other racial groups in the 1970s, although study factors may be important in explaining that result (a hospital-based study, with a poorly urbanized black population compared with whites, and likely unequal access to healthcare) (22). While not population-based, two very small studies performed in the 1980s did suggest a differing propensity to either Graves' disease or Hashimoto's thyroiditis in black and white children respectively (23,24). The first study assessed patients and their relatives attending a pediatric endocrine clinic for thyroid autoimmune disorders (23). Despite roughly equal attendance at the clinic by black and white children across all endocrine diseases, 12 of 18 children with Graves' disease were black, while only 2 of 20 children with Hashimoto's disease were black. The second study assessed thyroid autoantibodies and thyroid function in children with type 1 diabetes mellitus (24). Hashimoto's thyroiditis and hypothyroidism were common, particularly in white patients. Graves' disease was less common. However, all three cases of Graves' disease (out of 158 patients) were in black children.
The results of the current study make military-specific exposures, for example those related to deployments, unlikely to be important in explaining the racial differences in Graves' disease occurrence seen in the previous study (5). The results may reflect genetic and/or environmental exposures. However, for the previous study, the unifying military culture could be expected to limit the role of contemporaneous environmental differences between races/ethnicities. This may be important, as those with Graves' disease develop TSH receptor antibodies (the mediator of Graves' disease pathophysiology) temporally close to diagnosis (25).
Genetics are thought to play a significant role in autoimmune thyroid disease occurrence (26). Genetic differences could explain this study's results if non-Hispanic black Americans carry and express alleles important in Graves' disease development at higher frequency than do non-Hispanic whites. Genes known to predispose to Graves' disease include human leukocyte antigens (HLA), particularly class II genes for HLA-DR, the TSH receptor, cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), cluster of differentiation 40 (CD40), and protein tyrosine phosphatase nonreceptor type 22 (PTPN22) (27,28). A few studies have assessed the frequency of specific HLA-DR alleles in black subjects, but they are all small, and findings have differed across studies (29 –34). Other than HLA, the authors are not aware of any data assessing the frequencies of susceptibility alleles in non-Hispanic black versus non-Hispanic white populations.
Stressful life events need to be considered as a possible mediator of the Graves' disease–race/ethnicity relationship. African Americans may be exposed to a greater frequency of negative stressful life events than Caucasians (35). Negative stressful life events may precede Graves' disease diagnosis (36), although most studies assessing this association are retrospective and carry the risk of recall bias (37). To be a coherent explanation for the results of the authors' two studies, Asian-Pacific Islanders (identified as having high incidence of Graves' disease in the previous military study, but unable to be assessed in the current study because of low sample size) would also need to be exposed to greater stressful life events, which may not be true (38,39). This hypothesis requires further investigation.
Thyrotoxicosis was used in young people as a proxy for Graves' disease. Although subjects for whom other causes of thyrotoxicosis would have been common (i.e., pregnant or postpartum women, and subjects taking levothyroxine) were excluded, it is likely that a very small number of the remaining thyrotoxic subjects suffered from other causes of disease (i.e., painless thyroiditis, subacute thyroiditis, or toxic nodular disease). However, these conditions have been shown to be very rare compared with Graves' disease in young people, and thus misclassification is unlikely to explain the findings (2 –4). The primary definition of thyrotoxicosis that was used—a suppressed serum TSH concentration—is also not completely specific because pituitary dysfunction or euthyroid sick syndrome could also yield low TSH levels. This is unlikely to be important because in ambulatory community dwelling subjects, these conditions are substantially less common than Graves' disease.
Other potential limitations need to be considered. The small number of cases in some subgroups limits the ability to test for more potential confounders/causal intermediates. However, other than recent stressful life events (36,37), the major known risk factors for Graves' disease (sex, age, and smoking) were accounted for in the adjusted models. The laboratory assays also changed between the study periods. This is unlikely to affect the conclusions materially because the definition of a suppressed TSH (≤0.1 mIU/L) is unambiguously outside of the reference range for each assay. In addition, the two-stage model allowed assessment for heterogeneity of results across study periods and was reassuring. A significant number of the thyrotoxic cases identified may have been subclinical. Thus, the generalizability of the present results to clinical disease could be questioned. However, as described above, the overt thyrotoxicosis analysis yielded the same pattern of race/ethnicity differences, and is consistent with the independent dataset of Graves' disease diagnoses made in military personnel (5).
In conclusion, this study and our previous work (5) suggest that race/ethnicity may be a risk factor for Graves' disease. If these associations are confirmed by other studies, future investigations should assess whether environmental exposures or genetic/epigenetic differences account for these changes. Finding the mechanisms of thyroid autoimmunity have the potential to lead to prevention of Graves' disease, and may also lead to insights into the pathways for other autoimmune disorders.
Footnotes
Acknowledgments
A Cancer Council Queensland PhD scholarship helped support Don McLeod. David Whiteman and Susan Jordan are supported by Research Fellowships from the National Health and Medical Research Council of Australia (APP1058522 and APP1061341, respectively). The funding organizations had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. This work was presented in part at ICE/ENDO 2014, Chicago, IL.
Author Disclosure Statement
The authors have nothing to declare.