
Abstract
Background:
The choroid is a rare site of thyroid cancer metastases, and has been described in patients with evidence of advanced breast, lung, and prostate carcinomas. To the authors' knowledge, only seven reported cases exist with choroidal metastasis secondary to papillary thyroid carcinoma (PTC). This study describes an additional patient with metastatic PTC with simultaneous appearance of choroidal mass and cutaneous deposits while on systemic therapy with a tyrosine kinase inhibitor (TKI). These infrequent sites of metastasis are typically associated with a dismal prognosis following the diagnoses. However, this patient has not shown evidence of choroid or cutaneous recurrence one year following local targeted and systemic therapy.
Patient findings:
The case is presented of a 70-year-old male with widely metastatic PTC to the lymph nodes, lung, and mediastinum who was found to have choroidal metastasis six years after his initial diagnosis.
Summary:
The patient was asymptomatic and was found to have an incidental right choroidal mass on routine ophthalmology exam. Magnetic resonance imaging of the orbit revealed an isolated right choroid lesion suspicious for melanoma or metastasis. Concurrent to this discovery, he was noted to have progression of the lung and mediastinal disease along with new dermal lesions on the chest wall suspicious for dermal metastasis. Both the choroid and dermal metastases occurred while being on a TKI. Given his previous history of male breast carcinoma, a biopsy of the choroid was performed, which confirmed PTC. The patient developed endophthalmitis and subsequently underwent enucleation of the right eye. The choroid mass was completely excised, measured 3.5 mm×9.5 mm with negative margins, and histopathology was consistent with metastatic PTC. Pulmonary, mediastinal, and cutaneous lesions regressed after external beam radiation therapy, following which systemic therapy was changed to a different multikinase inhibitor.
Conclusion:
A rare and unique case is reported of choroidal metastasis from PTC that presented with concurrent new dermal metastasis in addition to lung and mediastinal lymph node progression. Furthermore, the patient developed choroid and dermal lesions while on a TKI and remained stable without recurrence in these regions after switching to an alternate multikinase inhibitor.
Introduction
T
Patient
A 70-year-old male with history of male breast cancer, status post resection and radiation, in remission, psoriatic arthritis on chronic steroids, and osteoporosis was diagnosed with PTC in 2006, and subsequently underwent total thyroidectomy and central neck dissection. Pathology showed multifocal PTC on the left, classical type by histologic criteria, 1.7 cm in maximal dimension, with gross extrathyroidal extension involving the innominate vein and laryngeal nerve. Four out of 10 lymph nodes were positive for metastasis in the central neck bilaterally, the largest measuring 4.6 cm in greatest dimension. Because of significant gross disease remaining postoperatively and involvement of the innominate vein and the laryngeal nerve, he received an empiric dose of 314 mCi of 131I. His stimulated thyroglobulin at the time of ablation was 167 ng/mL, with undetectable thyroglobulin antibodies (Fig. 1). Post-treatment whole body scan showed activity in the thyroid bed and no extrathyroidal uptake. The thyroglobulin remained persistently elevated on thyroid hormone suppression, and follow-up imaging with fludeoxyglucose positron emission tomography/computer tomography (FDG PET/CT) showed avid lesions in bilateral lateral cervical lymph nodes. He then underwent a salvage bilateral modified radical neck dissection. Pathology showed 2/14 Level IV/V lymph nodes on the right and 3/10 level IV/V lymph nodes on the left positive for metastatic PTC with extranodal extension. He was referred to the authors' center for further management, and given the significant extracapsular involvement and gross disease left behind after extensive surgery, he received external beam radiation therapy (6300 cGy in 35 fractions) to the surgical bed, bilateral neck, and superior mediastinum (Fig. 1). The thyroglobulin reached a nadir at 2.5 ng/mL with negative antibodies while on thyroid hormone suppression. However, in the following months, the thyroglobulin rose to 18 ng/mL with negative antibodies, and FDG PET/CT showed several new lung nodules that were nonglucose avid. Given his PET-negative pulmonary nodules and aggressive disease, he received a second dose of 131I (313 mCi; Fig. 1). The post-treatment scan showed uptake in the mediastinum and right infrahilar region of the lung corresponding to the known lesions.
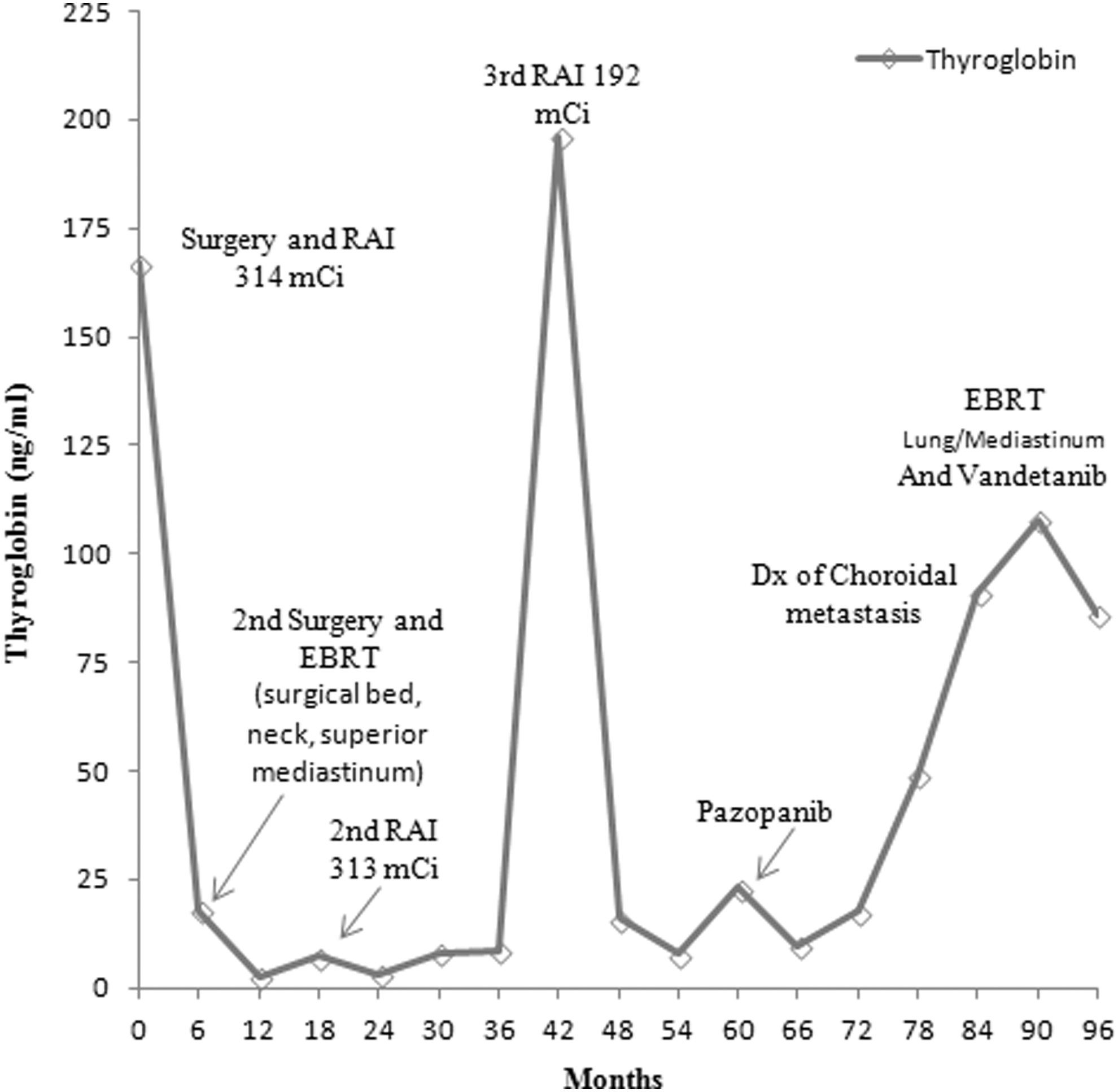
Thyroglobulin levels on thyroid hormone suppression (negative thyroglobulin antibodies).
A year and a half after the second radioactive iodine treatment, his thyroglobulin was 36 ng/mL with negative antibodies, and repeat FDG PET/CT showed increasing bilateral PET-negative pulmonary nodules. He received a third dose of 131I of 192.7 mCi, calculated by dosimetry (Fig. 1). The post-treatment scan showed multiple new foci of increased activity in the left lower lobe, superior mediastinum, and right supraclavicular regions (Fig. 2). Pulmonary nodules were stable for two years. However, after reaching a nadir at 7 ng/mL, the thyroglobulin rose to 64 ng/mL with negative antibodies and concomitant interval increase in size and glucose avidity of multiple pulmonary nodules on repeat FDG PET/CT as well as chest CT. At the time, none of the TKIs were FDA approved for treatment of metastatic well-differentiated PTC. Based on the available clinical data, off label systemic treatment with pazopanib 800 mg daily was instituted and in the following months (Fig. 1). The thyroglobulin on thyroid hormone suppression reached a nadir at 10 ng/mL with negative antibodies, and the lung nodules stabilized.
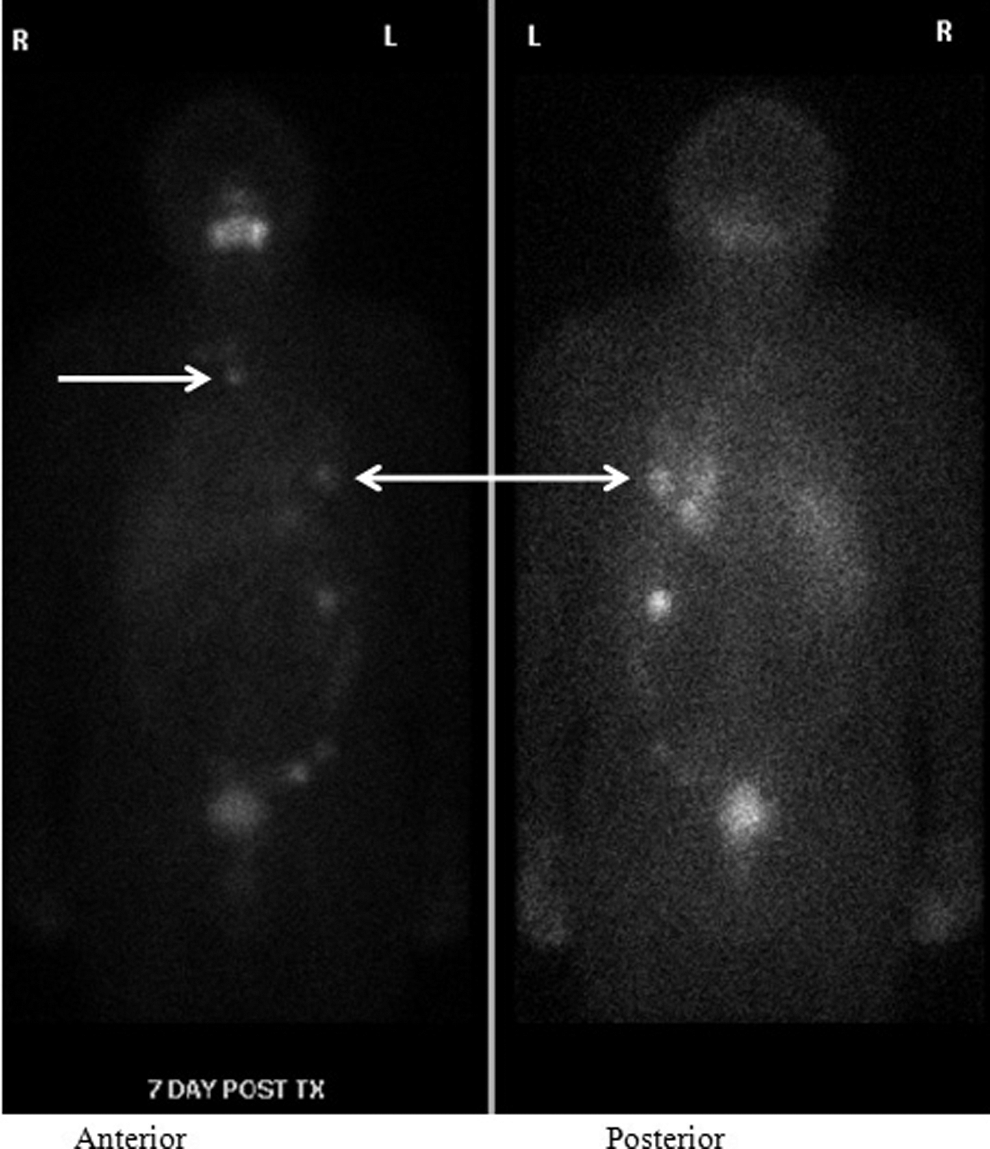
Seven-day whole body scan after radioactive iodine treatment. Multiple new foci of increased activity in the superior mediastinum and left lower lobe.
After two years of stability on pazopanib, a new retinal mass was noted incidentally in the right eye during a routine glaucoma evaluation. An orbital magnetic resonance imaging (MRI) scan showed an 8 mm right ocular choroidal mass (Fig. 3). The imaging characteristics of the choroidal mass were concerning for melanoma. Furthermore, given his history of both male breast cancer (disease-free longstanding) and metastatic PTC, he underwent vitrectomy and biopsy of the choroid for definitive diagnosis. The biopsy confirmed metastatic PTC. Unfortunately, he developed panendophthalmitis and underwent enucleation of his right eye. The choroid mass was completely excised and measured 3.5 mm×9.5 mm with negative margins. The tumor was positive for Periodic acid–Schiff (PAS), negative for Cytokeratin 20 (CK20), and demonstrated staining for pancytokeratin, cytokeratin 7 (CK7), thyroglobulin, and thyroid transcription factor (TTF), findings consistent with PTC.

Orbital magnetic resonance imaging with and without contrast. Hypointense 8 mm right ocular choroidal mass on T2 image.
Concurrent with the new diagnosis of the choroidal mass, he was also noted to have new dermal lesions on the chest wall suspicious for metastases. Additionally, there was increasing tumor burden in his left lung and mediastinum complicated by postobstructive pneumonia in the left lung. He underwent external beam radiation therapy (3000 cGY in 10 fractions) to the lower mediastinum, left hilum, left lower lobe, and chest wall metastases (Fig. 1). Pazopanib was discontinued, and off-label treatment with vandetanib 300 mg daily was initiated (Fig. 1). One year since radiation therapy, he has not had recurrence of dermal or choroidal metastases.
Discussion
This patient developed widespread dissemination of a well-differentiated PTC to the choroid and skin in addition to lymph nodes, lungs, and mediastinum. Metastases from PTC to the orbit are extremely rare. Of the differentiated thyroid cancers, PTC comprises about 85% of cases (1). PTC commonly metastasizes to regional lymph nodes, and hematogenous distant metastases occur in about 10% of patients, mainly to the lungs, bones, and brain (1). A recent review of the literature found 31 reported cases of orbital and/or ocular metastases from any cancer source during 1979–2012 (2). Twenty-two of 31 were choroidal metastatic cases from thyroid carcinoma, 15/22 cases from medullary and follicular thyroid carcinoma, and only 7/22 cases were PTC (3,5 –10). As in the present patient, choroidal metastases were reported later in the course of the disease. Hence, long-term outcomes are unavailable.
Interestingly, the present patient was asymptomatic when he was noted to have a choroidal mass during a routine glaucoma evaluation. Given his history of male breast carcinoma, PTC, and concern for melanoma, tissue biopsy was essential before deciding on treatment options. Previous case reports suggest diagnosis of choroidal metastases should be based on clinical examination and ultrasonography, and does not require tissue diagnosis (11 –13). However, given this patient's complicated history and the fact that he was chronically immunosuppressed from steroid treatment for his psoriatic arthritis, tissue biopsy was necessary, which confirmed the diagnoses of PTC. One of the potential complications of biopsy is endophthalmitis, which often necessitates enucleation of the eye, as in this case. Since choroidal metastases are extremely rare, there is no established standard of care for treatment. Treatment options for choroidal metastases secondary to PTC used in previous cases include 131I therapy and external beam radiation in nonradioiodine-avid lesions (3). Other treatment options reported are brachyradiotherapy using 125I episcleral radioactive plaque insertion (11), chemotherapy (8), and enucleation (6,8,10,11,14). Enucleation is usually considered in exceptional cases of metastatic lesions causing significant loss of vision and/or persistent symptoms such as pain (4). This patient's tumor was completely excised, and he did not undergo additional therapy with external beam radiation or 131I. He has done well, without evidence of recurrence in his choroid to date.
In the case of the present patient, since his metastatic disease progressed while on pazopanib, he was switched to a different TKI—vandetanib. There are several TKIs available, and each one differs depending on their targets or receptors. TKIs are involved in cell differentiation, survival, proliferation, and function (15). Pazopanib is a multitargeted TKI, principally targeting the VEGFR1–3, PDGFR-α, and PDGFR-β and c-KIT (16). A Phase II trial of pazopanib in patients with metastatic, rapidly progressive, radioiodine-refractory differentiated thyroid cancer reported partial response in 49% of the patients and none with a complete response. Progression-free survival rate at one year was 47%, but treatment was discontinued in 59% of the study patients (22 of 37) due to progression of disease (17). Pazopanib is not FDA approved for treatment of thyroid carcinoma but is considered an appropriate standard of care treatment option in patients with metastatic thyroid carcinoma in national evidence-based treatment guidelines (18). Vandetanib is a multitargeted TKI with potent activity against RET, EGFR, and VEGFR with anti-angiogenic effects (19). Vandetanib was FDA approved for treatment of medullary thyroid carcinoma in 2012 (20), and is currently being evaluated in a Phase III clinical trial for treatment of radioiodine refractory progressive metastatic differentiated thyroid cancer (21). The present patient had stable disease for almost a year after switching TKI therapy.
He also presented with dermal lesions concurrently with his choroidal mass. There are only two case reports in the literature describing the simultaneous occurrence of choroidal and skin metastases from a PTC. One case is from a tall-cell variant papillary carcinoma and the other from PTC (3,10). Both cases of choroidal metastases appeared in patients with advanced disease. The predilection of thyroid cancer skin metastases to localize to the upper body is documented in few case reports (22,23). The choroid, chest wall, face, and scalp have a rich capillary network that could explain simultaneous deposition of tumor emboli in these regions (3,4). In the present patient, a biopsy was not obtained from the chest-wall lesions prior to receiving external beam radiation for his lung masses. However, substantial regression in the size of cutaneous lesions after targeted radiation therapy suggests that these were consistent with dermal metastases.
In conclusion, this patient developed metastasis of PTC at two infrequent sites: the choroid and the skin. He responded well to enucleation as primary therapy of his choroidal metastasis and radiation therapy to his lung, mediastinum, and skin metastases. Another notable feature in this case was the stabilization of metastatic PTC upon switching multikinase inhibitors for systemic treatment. As TKIs have slightly different targets, it seems logical that switching TKI therapy after progression may provide further benefit in addition to local targeted therapies for specific metastatic lesions. PTC is the most common thyroid carcinoma, and even though hematogenous spread is rare in PTC, it is important to recognize that it can spread to unusual sites such as the choroid, and the patient may be asymptomatic.
Footnotes
Author Disclosure Statement
Whitney Goldner is a site Principal Investigator for AstraZeneca-sponsored multicenter Phase III study trial for vandetanib (VERIFY) to treat radioiodine refractory metastatic thyroid carcinoma, and was the site principal investigator for Eisai-sponsored multicenter Phase III trial for lenvatinib (SELECT) to treat radioiodine refractory metastatic thyroid carcinoma. No competing financial interests exist for the remaining authors.