
Abstract
Background:
Adult studies have shown that iodine-123 (123I) is as effective as 131I in detecting metastatic disease in patients with differentiated thyroid carcinoma. However, the type and administered activity of radioiodine used for diagnostic imaging of metastatic thyroid cancer has not been well studied in children. Here we describe our institution's experience with using 123I in diagnostic radioiodine scans in children with differentiated thyroid carcinoma.
Methods:
Every patient with differentiated thyroid carcinoma who completed diagnostic scanning followed by radioiodine therapy at our institution over the past 8 years was included in this retrospective chart review. Patient age, sex, presentation of thyroid disease, past medical history, thyrotropin, thyroglobulin, and antithyroglobulin antibodies were recorded. A single nuclear medicine radiologist evaluated all scans.
Results:
Thirty-three subjects completed 37 pairs of scans at a mean age of 13.4 years (range 6–17 years). The majority of subjects were female (81%) and had papillary thyroid cancer (91%). For diagnostic scanning, 5 received 2 mCi of 131I, 21 received 2 mCi of 123I, and 11 received 3 mCi of 123I. There was no statistically significant difference in rate of discordant scan pairs when comparing 131I and 123I (20% and 23% respectively, p=0.9). The detection of metastatic pulmonary disease on diagnostic scanning was not improved by increasing the dose of 123I from 2 mCi to 3 mCi (10% rate of missed lung detection with 2 mCi 123I vs. 20% with 3 mCi 123I).
Conclusions:
123I is effective for use in diagnostic radioactive iodine scans in children with differentiated thyroid cancer. The primary advantages of using 123I include decreased radiation exposure and avoidance of stunning. However, in children there is a possibility of missed detection of metastatic pulmonary disease.
Introduction
C
The main disadvantage of 131I in diagnostic scanning for local and distant metastatic disease is thyroid tissue “stunning.” This phenomenon occurs when the small diagnostic dose of 131I causes radiation injury to thyroid tissue and interferes with iodine uptake with subsequent administration of the larger therapeutic 131I dose (9). There is evidence that administration of even low doses of diagnostic 131I “stuns” thyroid cancer cells, making them less avid for the higher doses of 131I used for treatment purposes a short time later (6,10 –13).
To avoid the risk of stunning, many thyroid cancer treatment centers have shifted to using 123I in diagnostic scanning for metastatic thyroid disease. Adult studies have shown that diagnostic scans using 123I are as effective as those using 131I through comparison with posttreatment 131I scans or Tg measurements (6,7,14). Posttreatment scanning following high-dose 131I treatment can be considered a gold standard imaging technique since it has been found to be more sensitive than pretreatment low-dose 131I scans and since it can detect foci of uptake not previously seen on low-dose pretreatment scans in 10–30% of cases (6,15,16). The sensitivity of diagnostic scans using 131I has been found to be related to the dose administered (15).
Although the utility of 123I in diagnostic scanning for DTC has been shown in adults, this has not yet been documented in children with DTC. Furthermore, the optimal dose of 123I for use in diagnostic scanning in children with DTC has not been established. The main objective of this study was to describe our institution's experience using 123I in diagnostic whole-body scanning in children with DTC through comparison with 131I posttreatment scans. We also sought to determine if an increased dose of 123I (from 2 mCi to 3 mCi) provides better detection of metastatic pulmonary disease in children with DTC. We hypothesized that 123I would be as effective as 131I in diagnostic scanning as previously seen in adults and that increasing the dose of 123I would result in better concordance rates between pre- and posttreatment scans.
Materials and Methods
All consecutive patients with DTC and evidence of metastatic thyroid tumor treated at Ann and Robert H. Lurie Children's Hospital of Chicago who completed diagnostic scanning followed by RAI therapy at our institution from 2005 to 2013 were included in this retrospective review. This study was approved by the Lurie Children's Institutional Review Board. All patients had previously undergone total thyroidectomy and lymph node dissection, with the exception of one patient with follicular thyroid carcinoma who did not undergo lymph node dissection. Serum levels of thyrotropin (TSH), Tg, and anti-Tg antibodies obtained around the time of RAI dosing were recorded. Tg was measured using Siemens Immulite 2000®, a chemiluminescent assay with a lowest detectable limit of 0.2 ng/mL.
Scans
A total of 37 pairs of pretreatment and posttreatment scans were evaluated by one nuclear medicine radiologist to determine concordance. Scans were considered concordant when similar areas of uptake were seen on both the diagnostic and treatment scan and discordant when there were different areas of uptake seen on the scan pairs. Most of the diagnostic scans in this case series were the initial staging scans that were done approximately 6 weeks after thyroidectomy. The interval between diagnostic and treatment scans was typically 1–2 months. Patients were either withdrawn from thyroid hormone replacement 2 weeks prior to scanning or were given recombinant TSH (Thyrogen®) to increase TSH level and improve scan sensitivity.
Patients who received 131I for diagnostic scanning were given 2 mCi in accordance with the protocol in place prior to our institution's switching to 123I for diagnostic scanning. Patients who received 123I for diagnostic scanning were given either 2 mCi or 3 mCi. Diagnostic scanning was performed 24 hours after oral ingestion of radioiodine. The 131I treatment dose was based on diagnostic scan uptake, the age and body surface area of the child, and the serum Tg level. Posttreatment scanning was performed 7 days after the administration of 131I.
Statistical analysis
Concordance rates were calculated using the following equation: number of concordant scans/total number of scans compared×100. Concordance rates among the two types of radioisotopes were compared using a two-tailed chi-square test.
Results
A total of 33 patients completed 37 pairs of scans. For diagnostic scanning, 5 patients received 2 mCi of 131I, 21 patients received 2 mCi of 123I, and 11 patients received 3 mCi of 123I. Patient characteristics are outlined in Table 1. The mean age was 13.4 years with a range of 6 to 17 years. The majority of patients were female (81%) and had either papillary thyroid cancer (n=30; 91%) or follicular thyroid carcinoma (n=3; 9%). One patient with follicular thyroid carcinoma had Hürthle cell changes (patient ID 13). Two patients developed secondary thyroid cancers; one 5 years after treatment for neuroblastoma (ID 2), the second (ID 17) 14 years following treatment for pre-B-cell acute lymphocytic leukemia (ALL). The patient with neuroblastoma did not receive any irradiation; however, the patient with ALL had received total body irradiation. Scan results are displayed in Table 2 along with TNM stage (17), TSH, Tg, and anti-Tg antibody levels when available. There was no statistically significant difference in rate of discordant scan pairs between 131I and 123I (20% for 131I and 23% for 123I; p=0.9), and prediagnostic scan TSH levels were appropriately elevated in all discordant scan pairs (range 36.24–270.3 μU/mL).
FTC, follicular thyroid carcinoma; PTC, papillary thyroid carcinoma.
Scan descriptions listed in bold are considered discordant.
Thyroglobulin antibodies: reference range, <20 IU/mL.
Patient with a history of neuroblastoma.
Patient with a history of ALL.
Patient with recurrent disease, previously treated with 131I 8 years prior.
Abs, thyroglobulin antibodies; CT, computed tomography; Dx, diagnostic; N/A, not available; RAI, radioactive iodine; Tg, thyroglobulin; TSH, thyroid stimulating hormone; Tx, treatment.
Diagnostic scans were concordant with treatment scans in four of the five scan pairs when 2 mCi of 131I was used, and the diagnostic scans did not miss detection of lung disease. However, one patient (ID 4-A) was determined to have possible stunning with decreased uptake seen on the treatment scan compared with the diagnostic scan (Fig. 1).
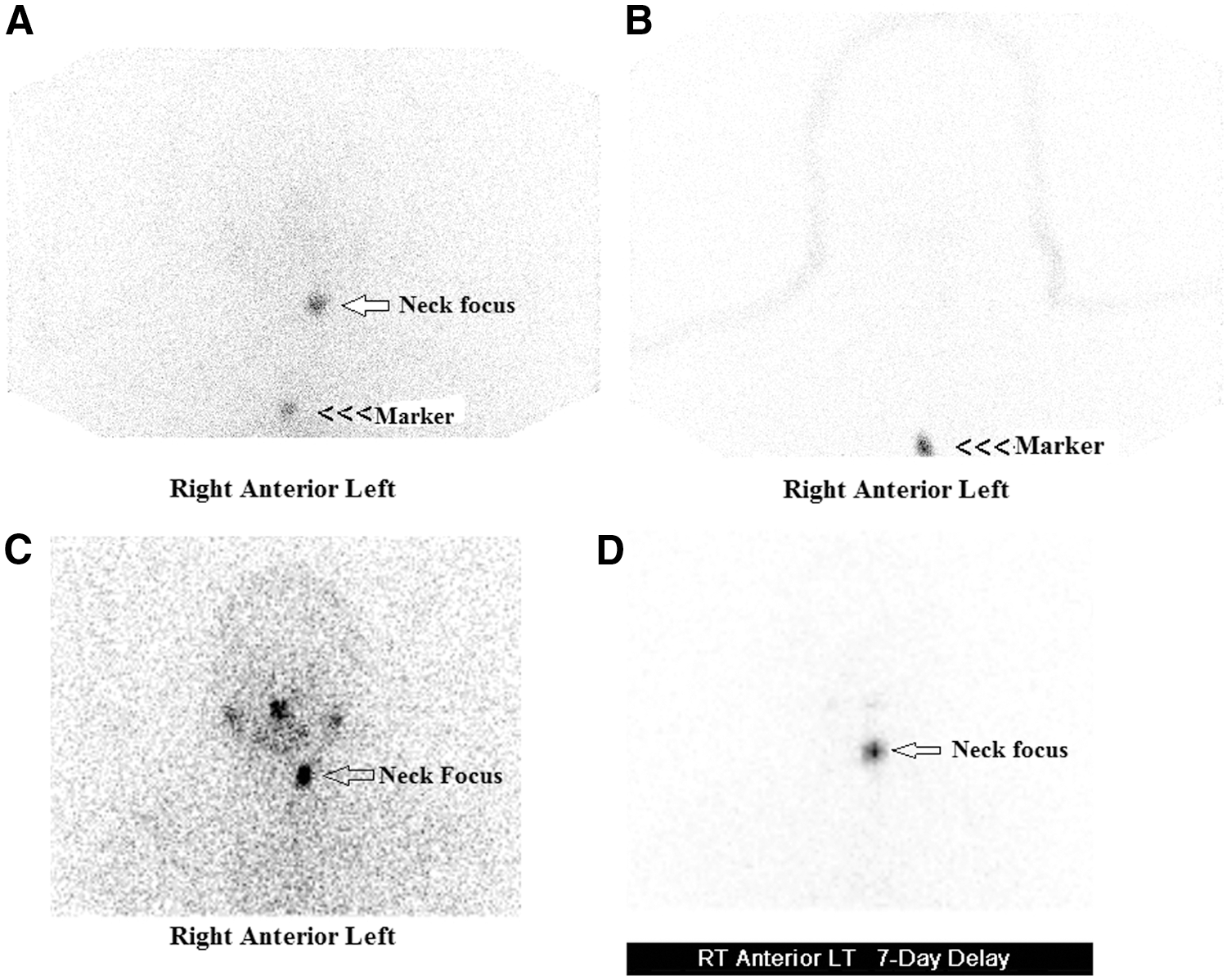
Patient ID 4: Images displaying possible “stunning.”
Diagnostic scans were concordant with treatment scans in 18 of the 21 scan pairs when 2 mCi of 123I was used. Figure 2 shows representative concordant scan images of patient ID 6. Two patients (ID 10, ID 14) were noted to have lung uptake on their treatment scans that was not previously visualized on diagnostic scanning. One patient (ID 19) had a negative diagnostic scan but went on to treatment due to a rising thyroglobulin level, which revealed a neck focus. Two patients (ID 11-B and ID 24) were noted to have mediastinum uptake on treatment scan consistent with thymus tissue which was not visualized on the diagnostic scan. These two patients were still considered to have concordant scans, as both sets of scans showed uptake in the neck representing local metastatic disease. Thus, 10% of diagnostic scans dosed with 2 mCi of 123I missed lung uptake and 5% were falsely negative.
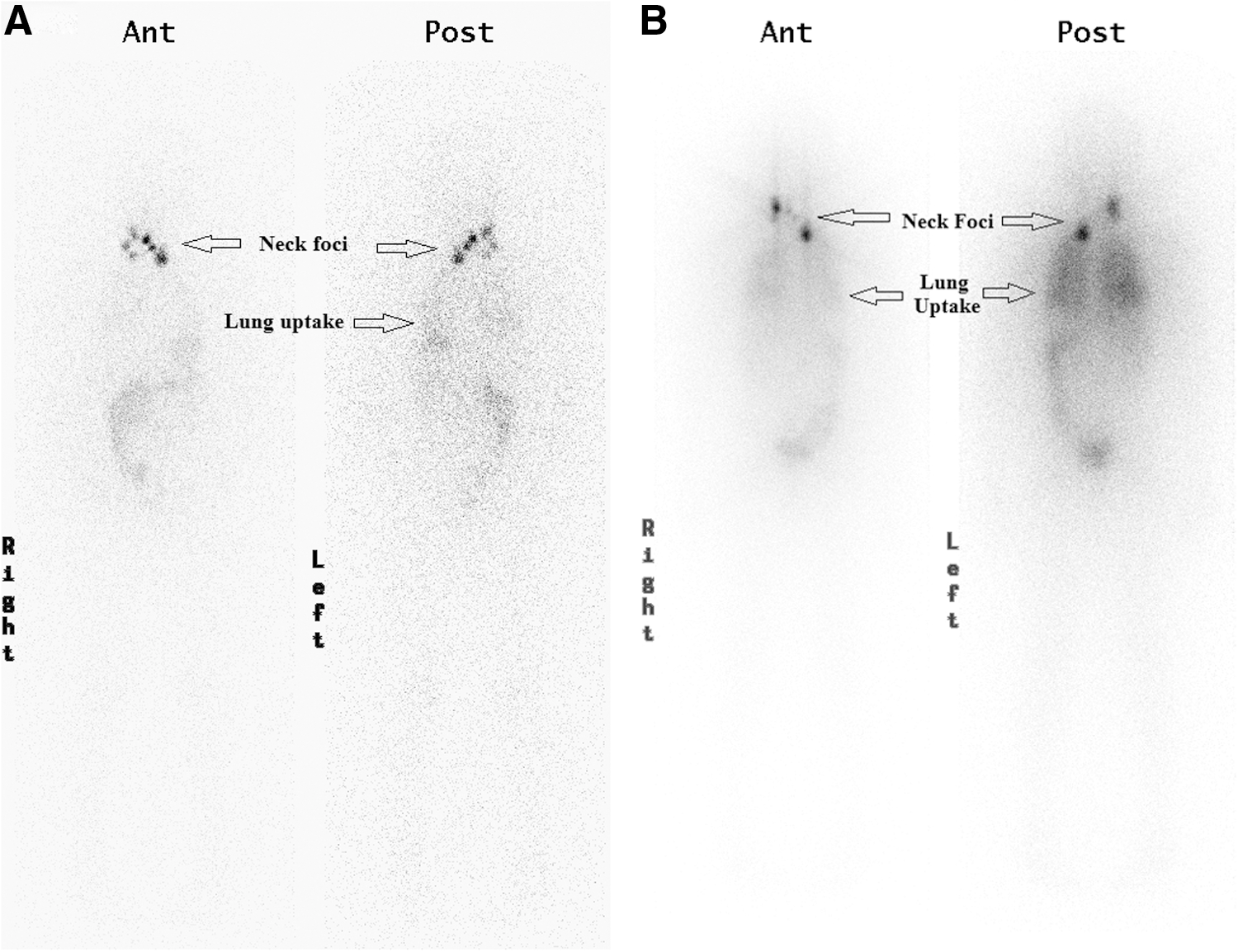
Patient ID 6: Images displaying concordant 123I and 131I scans.
There were 11 scan pairs in which 3 mCi of 123I was used as a diagnostic dose. Patient ID 31 represents an unusual case of a false positive RAI scan: she displayed neck and mediastinal uptake on both the diagnostic and treatment scans and additionally, diffuse lung uptake on the treatment scan. She had a low Tg level at the time of the 131I treatment scan and a CT scan of her chest was negative for lung nodules. Subsequent diagnostic scans with 123I in this patient did not display any RAI uptake. These findings likely represent a false positive initial diagnostic and treatment RAI scans. Thus patient ID 31 was excluded from the data analysis. In the remaining 10 patients, diagnostic scans were concordant with treatment scans in 6 of the 10 scan pairs, with all discordant treatment scans showing uptake in the mediastinum or lungs that was not previously seen on diagnostic scanning. Thus, of the 10 scan pairs, 2 (ID 27-A, 27-B)—or 20%—of diagnostic scans using 3 mCi of 123 I resulted in true missed lung uptake; 1 scan (ID 25) is a false negative scan; and 1 scan (ID 32) missed a mediastinal focus. Representative images of discordant scans of patient ID 27-A are displayed in Figure 3. Increasing the dose of 123I from 2 mCi to 3 mCi did not improve detection of metastatic lung disease (10% missed detection rate with 2 mCi vs. 20% with 3 mCi).
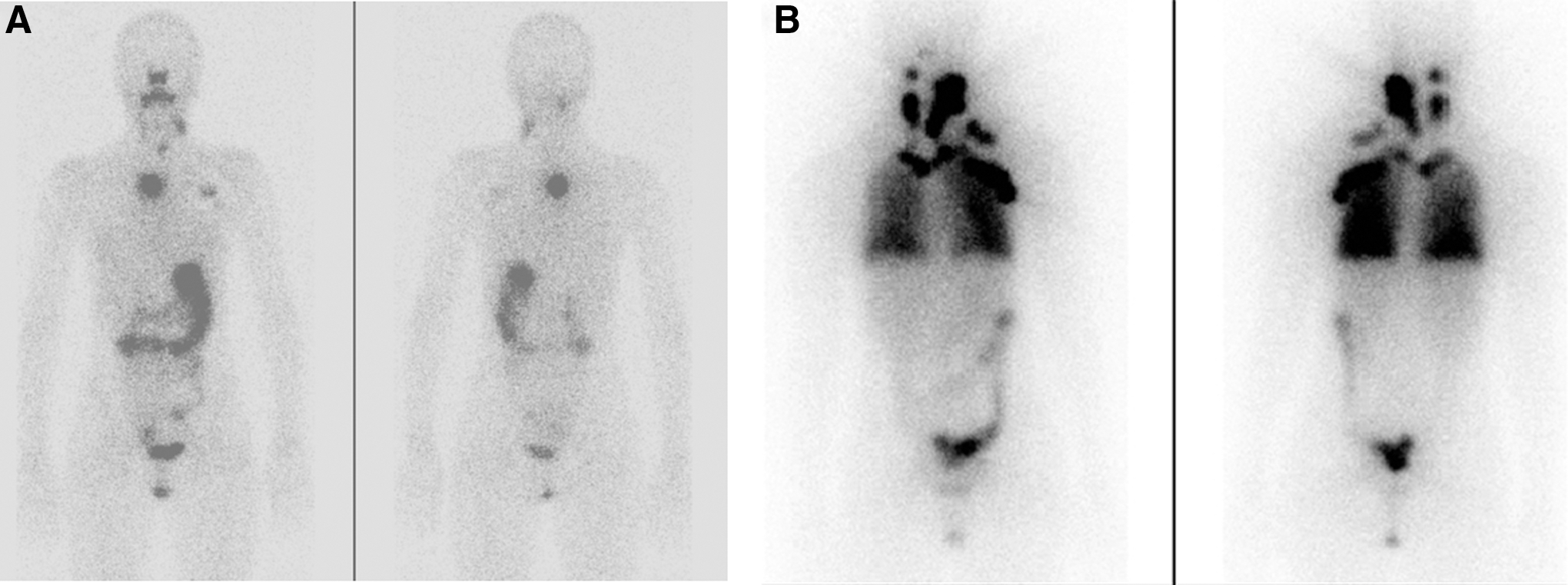
Patient ID 27: Images displaying discordant 123I and 131I scans.
To summarize, 20% (1/5) of 131I diagnostic scans were discordant with treatment scans compared with 23% (7/31) of 123I scans, a difference that was not statistically significant. Two 123I diagnostic scans were falsely negative, one using 2 mCi (ID 19) and the other using 3 mCi (ID 25). One 3 mCi 123I diagnostic scan was considered to be falsely positive and was excluded from our analysis. Detection of metastatic lung disease was not improved by increasing the dose of 123I from 2 mCi to 3 mCi.
Discussion
Our results demonstrate that 123I has comparable posttreatment scan concordance rates with low-dose 131I in diagnostic RAI scans in children with DTC. It is important to note that only five patients in this case series were given 131I diagnostic doses (compared with 32 who were given 123I). Rates of discordance in our study were similar to those published in adult studies where posttreatment scans differed in up to 30% of cases (6,15). In the patients in our study who received 131I for diagnostic scanning, discordance was only seen in one patient with possible stunning. While this would not change the management of this patient, it could play a role in her response to treatment. Of the seven discordant scans in patients who received 123I, the majority were due to missed metastatic pulmonary disease detection (4/7 scans), followed by missed mediastinal uptake (2/7 scans) and false negative diagnostic scans (2/7). One patient was determined to have a false positive scan. We also found that 3 mCi of 123I did not appear to be superior to 2 mCi in detecting metastatic lung disease in diagnostic scanning, although this analysis was not powered to determine the superiority of 3 mCi versus 2 mCi.
The primary advantages of using 123I in diagnostic scans in children include decreased radiation exposure and prevention of stunning. However, it appears that in children there is a possibility of missed detection of metastatic pulmonary disease. In our cohort of patients, lung disease was not missed when 131I was used in diagnostic scanning. However, only five patients received 131I for diagnostic scanning, of which two were determined to have lung metastases. Thus, we cannot draw conclusions on the superiority of 131I in the detection of lung metastases. A study by Sherman et al. found that 22% of scan pairs were discordant when comparing 131I pre- and posttreatment scans in adults with DTC (15). This same study found that pulmonary uptake foci were three times more likely to be discordant than were any other metastatic site in adults with DTC. Another study similarly found that patients with known distant metastatic disease have a high rate of discordance, approaching 63%, between 123I diagnostic and 131I treatment scans (8). Sherman et al. also determined that younger age at diagnosis and history of previous 131I treatment contributed to the likelihood of having a clinically significant discordant posttreatment scan (15). Other studies have likewise found that concordance rates decrease in patients who are treated with RAI for a second time (6,8). As we had a few patients in our cohort who were treated for a second time, this may have played a role in our rates of concordance. Of note, all of our patients treated for a second time (n=5) were given 123I for diagnostic scans, and among them, two patients (ID 25, ID 27-B) had discordant diagnostic scans, which gives a higher discordance rate of 40% for this subset of patients when compared with our entire study population.
Posttreatment scanning in one patient who received diagnostic 131I showed probable stunning, while there was no apparent stunning in those patients who received 123I for diagnostic scans. However, given the added benefit of decreased radiation exposure along with its lack of stunning, we believe that 123I should be used preferentially in diagnostic scanning in children with DTC given our comparable concordance data to 131I.
In this case series, one patient (ID 31) was noted to have lung uptake on her posttreatment scan, but she had a negative chest CT and an undetectable stimulated Tg. It is well known that RAI uptake can occur in a number of states other than DTC, including bronchiectasis and inflammatory lung tissue (8). This false positive scan is a reminder that while posttreatment scans have increased sensitivity, this is associated with a loss of specificity, and other diagnostic modalities need to be utilized at times to confirm disease status (15). We also observed two patients (ID 19 and ID 25) with a false negative 123I diagnostic scan who went on to treatment due to an elevated Tg level. False negative diagnostic scans using low-dose 131I are well recognized (16).
Children with DTC are more likely to develop pulmonary metastases than are adults, which makes the ability to detect pulmonary disease on diagnostic scanning even more important in the childhood population (1,2). Children with DTC and pulmonary metastases have excellent long-term survival with appropriate treatment, especially if the nodules are small enough that they are not visualized on chest X-ray.
DTC in children remains rare, thus these study results of a relatively large pediatric case series is the first to report the use of 123I in children. Furthermore, a number of patients in our series had distant metastatic disease. However, due to the retrospective study design of this case series, there are limitations in the conclusions we can extract. Data was collected retrospectively from a single institution, which limits generalizability. Definitive conclusions regarding the use of 131I and 123I in diagnostic scans are difficult to make since individual patients did not receive both types of scans. As we found, it is also difficult to distinguish false positive posttreatment scans from true disease. Further studies clearly need to be done in children with DTC to determine the optimal dose and timing for imaging following 123I administration, as it is possible that some foci might have delayed uptake rates. As a result, delayed imaging might pick up more lesions.
In conclusion, 123I is an effective scanning agent for initial evaluation and long-term tumor surveillance in children with DTC. However, pediatric endocrinologists and nuclear medicine radiologists need to be aware that metastatic pulmonary disease might not always be visualized on these types of diagnostic scans, particularly in children who require repeated 131I treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.