
Abstract
Background:
Measurement of thyroglobulin (Tg) in the washout fluid of fine-needle aspirates (FNA-Tg) is useful for diagnosis of lymph node (LN) metastasis in papillary thyroid carcinoma (PTC). However, the cutoff value of FNA-Tg in the preoperative state is not defined clearly. This study aimed to evaluate the optimal cutoff value of preoperative FNA-Tg according to serum Tg level.
Methods:
FNA-Tg was measured in 135 PTC patients (160 LNs) for preoperative diagnosis of cervical LN metastasis.
Results:
Of the 160 LNs, 119 (74%) were surgically removed and 110 (69%) were diagnosed as malignant. When we adopted a FNA-Tg of 1.0 μg/L as the cutoff value, the sensitivity and specificity were 99% and 76%, respectively. FNA-Tg levels were correlated with serum Tg levels (Pearson's coefficient 0.42, p=0.002) and the FNA-Tg levels of 12 of the 50 benign LNs were above 1.0 μg/L. We classified the LNs into two groups according to serum Tg level regardless of anti-Tg antibody status: a low Tg group (≤1.0 μg/L, n=22, 14%) and a high Tg group (>1.0 μg/L, n=138, 86%). In the low Tg group, the sensitivity and specificity of the FNA-Tg cutoff value of 1.0 μg/L were 93% and 100%, respectively. In the high Tg group, the sensitivity and specificity of the FNA-Tg cutoff value of 19.0 μg/L were 93% and 100%, respectively. A Tg ratio (FNA-Tg level divided by serum Tg level) of 0.5 gave an improved diagnostic performance (sensitivity, 98%; specificity, 98%) in the high Tg group.
Conclusions:
FNA-Tg levels in the preoperative state are affected by serum Tg levels when they exceeded 1.0 μg/L. For the preoperative diagnosis of metastatic cervical LNs, it seems reasonable to employ different cutoff values of FNA-Tg depending on serum Tg levels. We propose the use of an optimal cutoff value of FNA-Tg of 1.0 μg/L in patients with low serum Tg levels and a Tg ratio of 0.5 in those with high serum Tg levels irrespective of thyroglobulin antibody status.
Introduction
P
Since its measurement was first proposed in 1992 (5), there have been a number of studies addressing the role of FNA-Tg (6). However, there are still uncertainties in the optimal cutoff value of FNA-Tg because many factors can affect it, including the presence or absence of the thyroid gland, the serum thyrotropin (TSH) level, anti-thyroglobulin antibody (TgAb) status, differences in FNA technique and in Tg assay kit performance, as well as variability in the production of Tg by metastatic cancer cells in LNs (6,7).
Recently, a meta-analysis indicated that a FNA-Tg value of 1.0 μg/L is the optimal cutoff. However, the diagnostic performance of FNA-Tg was poorer in patients before thyroidectomy than postoperatively (6). FNA-Tg levels are expected to be higher in patients with thyroid glands because Tg secreted by normal thyroid can affect the FNA-Tg level due to contamination with blood during the procedure (8,9) Studies on the FNA-Tg cutoff value in patients with thyroid glands are limited and inconclusive (8 –14).
The aim of this study was to evaluate the optimal cutoff value of FNA-Tg for preoperative diagnosis of cervical LN metastasis in patients with PTC according to serum Tg level. We hypothesized that FNA-Tg levels might be affected by serum Tg levels when the concentration of the latter was high enough.
Materials and Methods
Patients
We included patients with PTC in whom FNA-Tg was measured for evaluation of lateral cervical LNs before thyroid surgery between 2008 and 2011 in the Asan Medical Center (Seoul, Korea). We only included patients who underwent initial surgery in our institution. We excluded patients with histories of thyroid surgery or in whom preoperative serum Tg, TgAb, or TSH were not measured. One hundred thirty-five patients were eligible for analysis. Preoperative serum Tg was measured before FNA in 66 patients (49%), within 2 weeks from FNA in 18 patients (13%), and after 2 weeks from FNA in 51 patients (38%).
All patients underwent total thyroidectomy with prophylactic central neck dissection and 100 (74%) of them also underwent simultaneous therapeutic lateral neck dissection. The primary tumors of all the patients were PTCs and 134 (99%) of them had the classical variant, while 1 had the diffuse sclerosing variant. This study was approved by the Institutional Review Board of our institution.
Ultrasonography and FNA
All patients underwent neck US examination with an HDI 5000 or IU22 scanner (Philips Medical Systems, Bothell, WA) with a 12.5 MHz linear phased-array transducer. Experienced radiologists performed US-guided FNA on suspicious metastatic or indeterminate lateral cervical LNs the long diameters of which in the transverse plane were equal to or greater than 0.5 cm. US features suggestive of a metastatic LN were round shape (long axis to short axis ratio <1.5), absence of an echogenic hilum, microcalcification, cystic changes, and peripheral blood flow on color Doppler images (15).
US-guided FNA was performed with free-hand technique using a 23 gauge needle connected to a 10 mL syringe. The contents of the needle were expelled onto a slide and smeared with a second slide. The slides were immediately immersed in 95% ethanol. Immediately after biopsy, the same needle and syringe were washed with 1 mL of normal saline solution and the washout fluid was sent to the laboratory for Tg assays (7).
Measurement of Tg, TgAb, TSH, and FNA-Tg
Serum Tg, TgAb, and TSH were measured as part of the preoperative work-up. Serum Tg and FNA-Tg were measured using an immunoradiometric assay (Tg-pluS RIA kit; BRAHMS AG, Henningsdorf, Germany) with a functional sensitivity of 0.2 μg/L, a coefficient of variation of 20%, and an analytical sensitivity of 0.08 μg/L. Serum TgAb levels were measured using a radioligand assay (anti-Tg RIA kit; BRAHMS AG) with a functional sensitivity of 20 IU/mL. Serum TSH levels were measured with an immunoradiometric assay (TSH-CTK-3 kit; DiaSorin S.p,A., Saluggia, Italy) with a functional sensitivity of 0.07 mU/L (7).
Definitions
A final diagnosis of cervical LN metastasis of PTC was based on histologic or cytologic findings. Malignant LNs were defined if there was histologic confirmation of metastasis and benign LNs were defined if there was no evidence of metastasis in histology or cytology.
Positive TgAb was defined as a serum TgAb value ≥60 IU/mL according to the manufacturer's instructions. When serum TgAb was undetectable (<20 IU/mL) or low but detectable (20–59 IU/mL), serum TgAb status was defined as negative.
The Tg ratio was defined as the FNA-Tg level divided by the serum Tg level, and the Tg difference was defined as the FNA-Tg level minus the serum Tg level (11,12).
Statistics
R version 3.0 and R libraries survival, car, Hmisc, Cairo, and pROC were used to analyze data (R Foundation for Statistical Computing,
Continuous variables are presented as medians with interquartile range (IQR), and the Wilcoxon rank-sum test was used to compare medians. Categorical variables are presented as numbers with percentages, and the χ2 test was used for comparisons. Serum Tg and FNA-Tg values were transformed logarithmically and analyzed. The correlation of FNA-Tg with serum TSH or serum Tg level was evaluated using Pearson's correlation coefficient and with serum TgAb was evaluated using Wilcoxon rank-sum test. We performed receiver operating characteristic (ROC) curve analysis to determine the optimal cutoff value of FNA-Tg for the diagnosis of LN metastasis and obtained the area under the receiver operating characteristic curve (AUROC) value. The diagnostic performances of FNA-Tg cutoff values were compared using sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), diagnostic accuracy, and AUROC values (16). All p values were two sided, with p<0.05 considered statistically significant.
Results
Baseline characteristics of patients and LNs
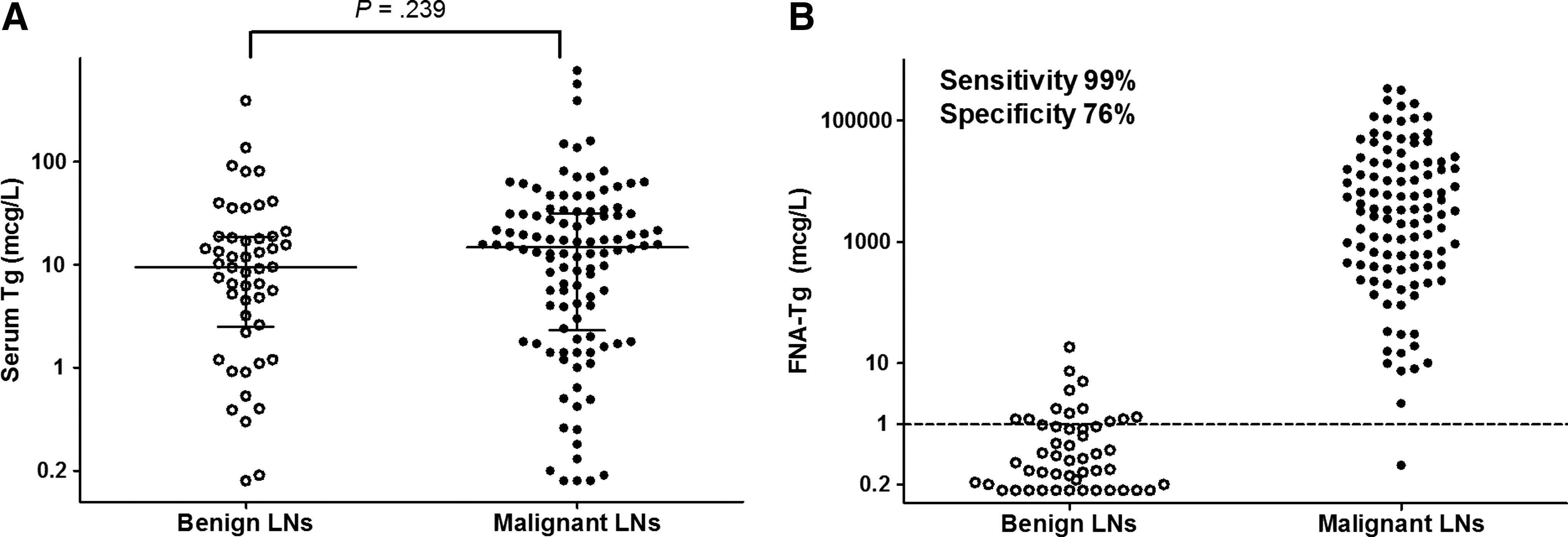
The median age of the 135 patients with PTC was 47 years (IQR 39–54), and 104 of them (77%) were female. In the 135 patients, a total of 160 cervical LNs were evaluated before surgery by FNA, with measurement of FNA-Tg. FNA for thyroid nodule was simultaneously performed in 91 LNs (57%). Ninety-five LNs (59%) were diagnosed as malignant after cytology, and surgically removed. Fifteen (9%) presented benign or indeterminate cytology, but were confirmed as malignant by final histology because their FNA-Tg values were high (median 20,300 μg/L, IQR 933–52,850 μg/L). Ultimately, 110 LNs (69%) were diagnosed as malignant. The remaining 50 LNs (31%) were diagnosed as benign by cytology and 9 (18%) of them were surgically removed. Primary tumor size, serum TSH level, serum TgAb status, and serum Tg level did not differ according to the diagnostic category of the LNs (Table 1, Fig. 1A). However, the median FNA-Tg level was significantly higher in the malignant LNs (median, 3285 μg/L; IQR 413–17,820 μg/L) than in the benign LNs (median, 0.3 μg/L; IQR 0.1–0.9 μg/L) (Table 1).
p values were determined by the Wilcoxon-rank sum test.
p values were determined by the χ2 test.
Continuous variables are presented as median with interquartile range.
Categorical variables are presented as number with percentage.
Values in parenthesis are percent or interquartile range.
LNs, lymph nodes; FNA-Tg, thyroglobulin in the washout fluid of needle aspirates; TgAb, thyroglobulin antibodies; negative TgAb, undetectable or TgAb <60 IU/mL; positive TgAb, TgAb ≥60 IU/mL.
FNA-Tg levels in benign LNs are correlated with serum Tg levels
As shown in Figure 1B, when we adopted a cutoff value of FNA-Tg of 1.0 μg/L, the sensitivity and specificity were 99% and 76%, respectively. The FNA-Tg levels of 12 of the 50 benign LNs (24%) were above 1.0 μg/L. To evaluate the factors influencing FNA-Tg levels in the cervical LNs, we examined the correlation of FNA-Tg levels with serum TSH level and with serum TgAb. Neither serum TSH level nor serum TgAb were correlated with FNA-Tg level in benign LNs (p=0.20, and p=0.74, respectively) or malignant LNs (p=0.60, and p=0.44, respectively). The FNA-Tg levels of malignant LNs were also not correlated with serum Tg levels (p=0.37). However, the FNA-Tg levels of benign LNs were significantly correlated with serum Tg levels (Pearson's coefficient 0.42, p=0.002) (Supplementary Fig. S1; Supplementary Data are available online at
Two different cutoff values of FNA-Tg according to serum Tg level
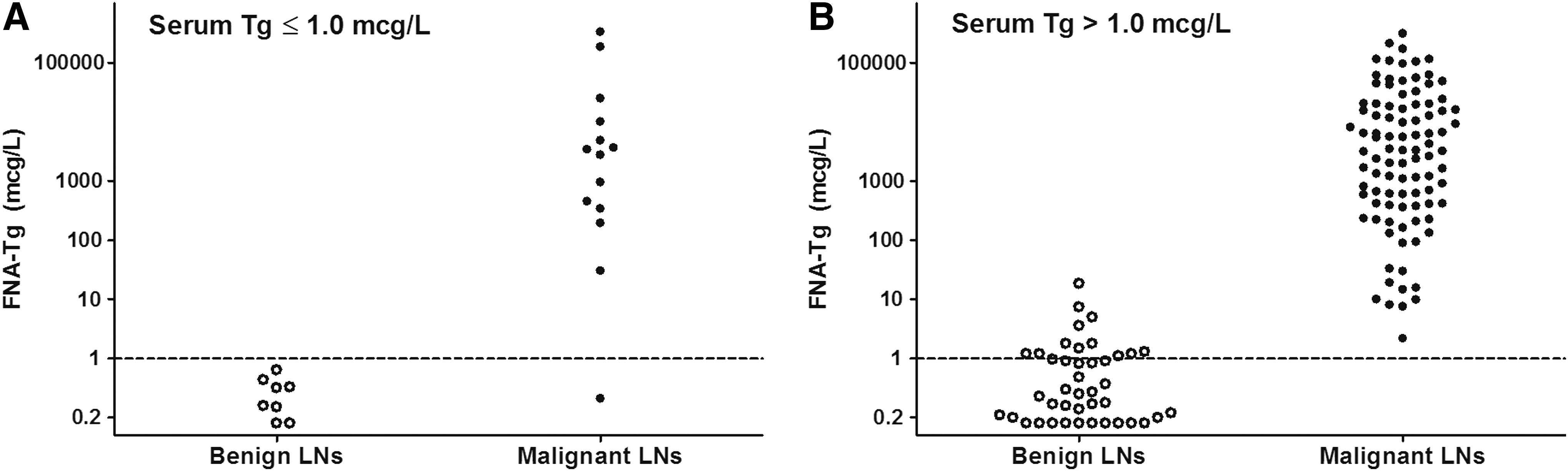
We divided the LNs into two groups according to their serum Tg levels: a low Tg group (serum Tg ≤1.0 μg/L, n=22, 14%) and a high Tg group (serum Tg >1.0 μg/L, n=138, 86%). There were no significant differences between the two groups except for serum TgAb positivity (Table 2).
p values were determined by the chi-square test.
p values were determined by the Wilcoxon-rank sum test.
Continuous variables are presented as median with interquartile range.
Categorical variables are presented as number with percentage.
Values in parenthesis are percent or interquartile range.
LN, lymph node; FNA-Tg, thyroglobulin in the washout fluid of needle aspirates; TgAb, thyroglobulin antibodies; negative TgAb; undetectable or TgAb <60 IU/mL; positive TgAb; TgAb ≥60 IU/mL; Tg ratio, FNA-Tg divided by serum Tg.
In the low Tg group, the sensitivity and specificity of the FNA-Tg cutoff of 1.0 μg/L were 93% and 100%, respectively (Fig. 2A, Table 2). NPV and PPV were 89% and 100%, respectively. In this group, serum TgAb was positive in 17 cases (77%). There was only one case of a malignant LN with an FNA-Tg below 1.0 μg/L and typical papillary structures of atypical follicular cells in cytology; it had a low serum Tg level (0.49 μg/L) and was negative for TgAb (54 IU/mL).
The diagnostic performance of the FNA-Tg cutoff value of 1.0 μg/L according to serum Tg levels for the preoperative diagnosis of cervical LN metastasis in patients with PTC.
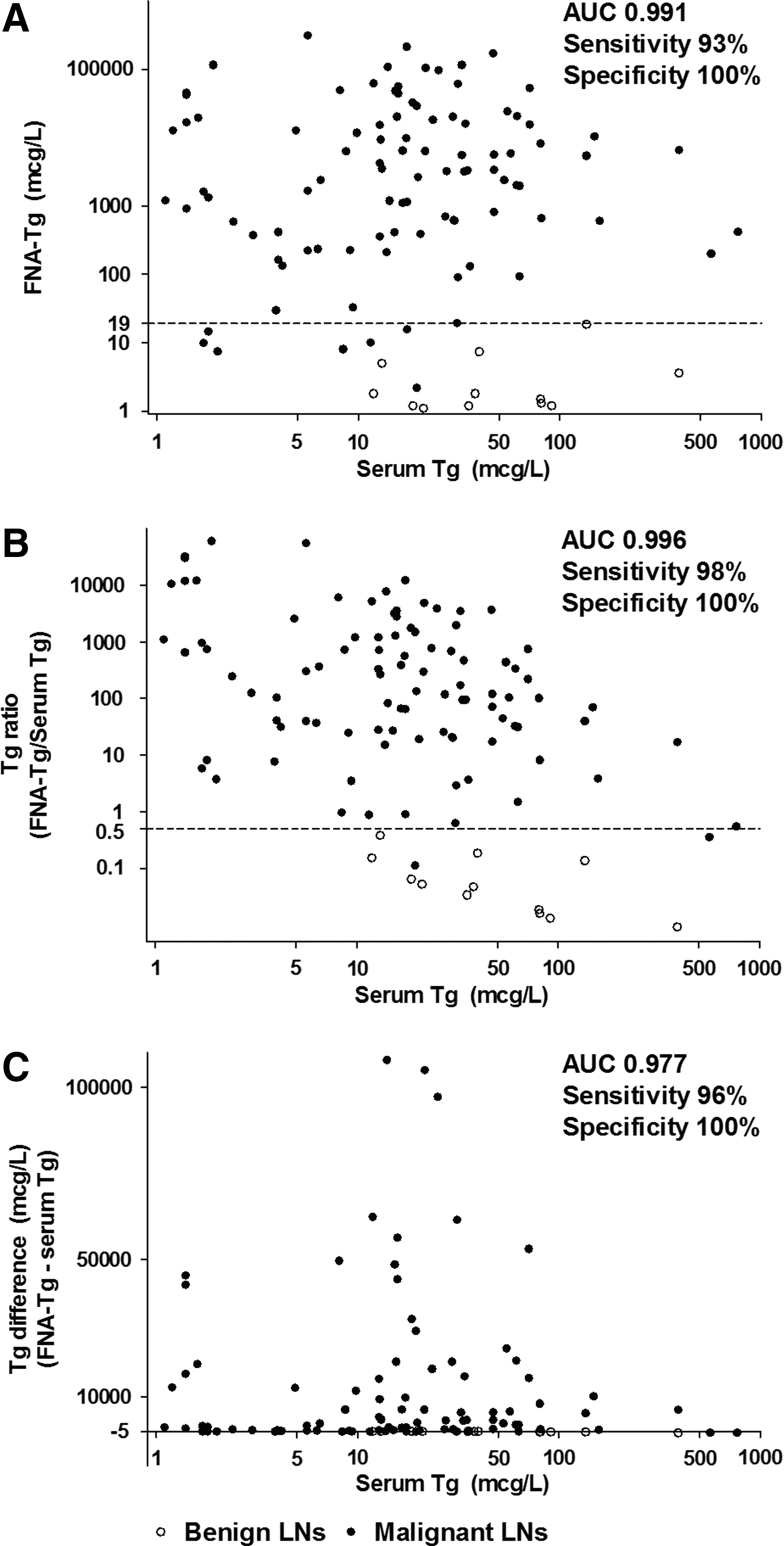
In the high Tg group, the sensitivity and specificity of the FNA-Tg cutoff of 1.0 μg/L were 100% and 71%, respectively. The FNA-Tg levels of 12 of 42 benign LNs (29 %) were above 1.0 μg/L (Fig. 2B). Therefore, we tried to identify an optimal FNA-Tg cutoff value in patients with high serum Tg by ROC curve analysis (Supplementary Fig. S2). The FNA-Tg cutoff value of 19.0 μg/L had the best diagnostic performance with 93% sensitivity and 100% specificity (AUROC 0.991) (Fig. 3A, Table 2). NPV and PPV were 63%, and 100%, respectively.
Cutoff values of FNA-Tg, Tg ratio, and Tg difference according to an ROC curve analysis for the preoperative diagnosis of cervical LN metastasis in patients with serum Tg levels >1.0 μg/L.
We also evaluated the optimal cutoff value by using Tg ratios and Tg differences from the ROC curve analysis. A Tg ratio of 0.5 had the best diagnostic performance: the AUROC was 0.996, with 98% sensitivity and 100% specificity (Fig. 3B, Table 2). NPV and PPV were 86% and 100%, respectively. The optimal cutoff value for the Tg difference was −5 from the ROC curve analysis with a sensitivity and specificity of 96% and 100%, respectively (AUROC 0.977). However, the values of the Tg difference were unevenly distributed (Fig. 3C).
As shown in Table 2, the diagnostic accuracy of the FNA-Tg cutoff of 1.0 μg/L in the low Tg group was 95%, and that of 19.0 μg/L in the high Tg group was 94%. The diagnostic accuracy of the Tg ratio cutoff of 0.5 in the high Tg group was 98% and it was not different according to TgAb status (p=0.14).
Discussion
In previous studies, a FNA-Tg level of 1.0 μg/L was suggested as the optimal cutoff value for diagnosis of malignant LNs in PTC patients (4,6,12). However, most of the subjects in those studies were evaluated postoperatively. Although 15 studies among 24 selected studies in a recent meta-analysis included patients with thyroid glands, the proportion of subjects evaluated in the preoperative state was low and many of them analyzed the cutoff value of FNA-Tg without discriminating the presence or absence of thyroid glands. Seven studies analyzed the optimal cutoff value of FNA-Tg only in preoperative patients but, their cutoff values were highly variable (6) (Table 3).
LN, lymph node; FNA-Tg, thyroglobulin in the washout fluid of needle aspirates; ROC, receiver operating curve; Tg ratio, FNA-Tg value divided by serum thyroglobulin value.
When we used an FNA-Tg cutoff value of 1.0 μg/L for preoperative patients, the specificity was limited because the FNA-Tg levels of benign LNs rose with increasing serum Tg level. Therefore, we used two different cutoff values of FNA-Tg depending on the serum Tg level. In patients with a low serum Tg (≤1.0 μg/L), the FNA-Tg cutoff value of 1.0 μg/L gave a good diagnostic performance, as it did in postoperative patients irrespective of TgAb status. In patients with a high serum Tg (>1.0 μg/L), a FNA-Tg of 19.0 μg/L was the optimal cutoff value. On the other hand, a Tg ratio of 0.5 had a better diagnostic performance than FNA-Tg itself or the Tg difference. This result indicates that using different cutoff values of FNA-Tg is more appropriate for preoperative diagnosis of cervical LN metastasis: a FNA-Tg of 1.0 μg/L in patients with low serum Tg levels, and a Tg ratio of 0.5 in patients with high serum Tg levels.
It has been suggested that the cutoff value of FNA-Tg should equal the serum Tg level (i.e., a Tg ratio of 1.0) (11,17,18). It has been proposed that this approach could be useful in overcoming interference by serum Tg with FNA-Tg, and improving the diagnostic accuracy of FNA-Tg in patients with high serum Tg (6). However, no clear evidence supporting this view has been provided. In theory, the optimal cutoff value of the Tg ratio might be affected by the extent of blood contamination. One study reported that the theoretical maximum contamination of the needle washout fluid by blood was approximately 20% and that contamination was less than 5% in experiments measuring albumin concentration in FNA washout fluid (19). Furthermore, the FNA-Tg levels of metastatic LNs might be lower than the corresponding serum Tg levels in patients with an extensive disease burden if the Tg was produced by numerous other metastatic LNs and/or distant metastatic lesions. For these reasons, a Tg ratio cutoff value of 1.0 might have poor sensitivity and specificity. In the present study, the optimal cutoff value of the Tg ratio from ROC curve analysis was 0.5, with 98% sensitivity and 100% specificity. A Tg ratio of 1.0 had only 93% sensitivity and 96% specificity.
Previous analyses of data in thyroidectomized patients showed that FNA-Tg levels were significantly correlated with serum TSH and with serum TgAb status (7,9,12). In the present study, the preoperative FNA-Tg levels were only affected by serum Tg levels in the benign LNs, and FNA-Tg levels were not related to serum TSH or serum TgAb status. The median TSH level of our study patients was 2.3 mU/L, and TSH levels changed within a narrow range (IQR 1.5–3.5 mU/L). However, postoperative TSH levels after thyroidectomy should vary considerably due to levothyroxine treatment or administration of recombinant human TSH. Moreover, high preoperative serum Tg levels in patients with normal thyroid glands might saturate serum TgAb, so that serum TgAb would not affect levels of FNA-Tg. In our patients, the serum Tg level was significantly affected by TgAb status (median 15.8 μg/L in patients with negative TgAb; median 1.7 μg/mL in patients with positive TgAb).
It is well known that any minor insult to the thyroid gland such as FNA causes an increase in serum Tg and it may persist for 15 days (20). In this study, serum Tg was measured within 2 weeks after FNA in 18 patients (13%), but serum Tg levels were not elevated in these patients (p=0.31, data not shown). Moreover, the FNA-Tg levels were not affected by a simultaneous FNA procedure for thyroid nodules in patients with both benign and malignant LNs.
In this study, 22 LNs (14%) were associated with low serum Tg levels (≤1.0 μg/L) despite the presence of thyroid glands. Seventeen (77%) of them had positive serum TgAb, but 5 (23%) had negative TgAb. The reason for the low serum Tg in these 5 LNs is unclear, but their TgAb values were relatively high, ranging from 40.4 to 55.4, and this might have interfered with the serum Tg measurements (7). Spencer et al. (21) have indeed reported that TgAb classified as negative can interfere with the detection of serum Tg in many cases.
Our study has several limitations. First, it is a retrospective study and relatively small numbers of benign LNs were surgically removed. It is possible that some of the benign LNs harbored metastatic PTC. However, there were no recurrences in patients with the remaining benign LNs during a median of 23 months of follow-up. In addition, the NPV, PPV and diagnostic accuracy of the cutoff values may not be reliable because we performed FNA only for LNs with suspicious metastatic features revealed by US, as reflected in the high prevalence of metastatic LNs. NPV, PPV and diagnostic accuracy are directly related to the prevalence of disease (22). Second, this study is relatively small compared with previous series (12,23,24). However, most of the previous studies included both preoperative and postoperative patients (17,18,23,25,26). The noteworthy feature of the present study is the comprehensive analysis of FNA-Tg levels according to serum Tg in preoperative patients only. As far as we know, this is the first study suggesting the use of two different cutoff values for preoperative FNA-Tg levels according to their serum Tg levels in patients with PTC. This approach may be of clinical relevance.
In conclusion, FNA-Tg levels in the preoperative state were affected by serum Tg levels when they exceeded 1.0 μg/L. For the preoperative diagnosis of metastatic cervical LNs, it seems reasonable to use different cutoff values of FNA-Tg depending on serum Tg levels. We propose the use of an optimal cutoff value of FNA-Tg of 1.0 μg/L in patients with low serum Tg levels and a Tg ratio of 0.5 in those with high serum Tg levels irrespective of TgAb status.
Footnotes
Acknowledgments
This study was supported by grants (no. 2014-582) from the Asan Institute for Life Sciences, Seoul, Korea.
Author Disclosure Statement
No competing financial interests exist.