
Abstract
Background:
The use of radioactive iodine therapy (RAIT) is increasing in thyroid cancer management. The association between RAIT at high doses and leukemia is well known, but studies of this association in a large population are lacking. This study aims to investigate the association between RAIT and leukemia in the context of current practice.
Methods:
Retrospective analysis of a 542,845 person-year (PY) follow-up of thyroid cancer patients was conducted using the Korean National Health Insurance claims database between January 2008 and December 2013. Patients were categorized according to RAIT dose (no RAI; low dose, ≤30 mCi; moderate dose, 31–100 mCi; high dose, 101–150 mCi; and very high dose, >150 mCi).
Results:
Among 211,360 thyroid cancer patients, 72 (0.03%) patients developed leukemia during follow-up (median 877 days). The cumulative incidence of leukemia per 105 person-year (PY) was 9.8 in the no RAI [95% confidence interval (CI) 6.4–14.4]; 6.1 [CI 1.7–15.7] in the low-dose; 8.6 [CI 3.2–18.7] in the moderate-dose; 29.5 [CI 18.3–45.1] in the high-dose; and 20.9 [CI 11.7–34.4] in the very high-dose groups. The hazard ratios were elevated significantly in the high- and very high-dose groups (HR 3.1 and 2.1, respectively, p<0.001) when compared with the no RAI group.
Conclusions:
RAIT exceeding 100 mCi was strongly associated with the development of leukemia in a nationwide, population-based study, while lower RAIT doses were not. Considering the favorable survival of patients with thyroid cancer and the potential harm of RAIT, physicians need to consider the pros and cons of RAIT when using this treatment option.
Introduction
R
Rates of RAIT ranged from 38% to 61% of patients with thyroid cancer between the 1980s and early 1990s in the United States (4). A recent study using the Surveillance, Epidemiology and End Results (SEER) database reported that the proportion of patients receiving RAIT has increased from 6.1% to 48.7% in the period between 1973 and 2006 (5). In Korea, RAIT increased from 31.2% in 1999 to 40.9% in 2008 based on an epidemiologic survey conducted by the Korea Central Cancer Registry in 2011 (2).
Although effective, RAIT has several adverse effects. Although RAI is taken up almost exclusively by thyroid tissue, some RAI accumulates in the salivary glands and stomach via the sodium–iodide symporter (6). Acute side effects including sialadenitis, xerostomia, nausea, vomiting, stomatitis, and thyroiditis can occur as early as within 10 days after RAIT, and many of these side effects are reversible (3,7). However, chronic side effects including salivary gland dysfunction can develop up to one year after RAIT and the effects can be permanent (3,8).
Another potential chronic serious complication of RAIT is the development of secondary cancers, especially in patients who received high RAI doses (9,10), although recent studies are proposing that even low-dose RAIT could be related to the risk of developing secondary malignancies. In a large European cohort study, an increased risk of solid cancers and leukemias was observed with increasing cumulative activity of RAI administered, with excessive absolute risks of 14.4 for solid cancers and 0.8 for leukemia per GBq (approximately 27 mCi) during a 105 person-year (PY) follow-up (11). Another study using the SEER database indicated a 25% increase in the risk of secondary malignancies for patients with a history of RAIT, especially salivary gland cancers and leukemias (12). A meta-analysis by Sawka et al. also showed that the risk of leukemia increased in subjects with thyroid cancer who had received RAIT, with a relative risk (RR) of 2.5 (13).
The hematopoietic system is well known for its radiosensitivity. Many studies regarding atomic bomb incidents demonstrated that the risk of leukemia was significantly increased in survivors of the Hiroshima and Nagasaki bombings (14,15). Furthermore, cleanup workers exposed to low-dose radiation in Chernobyl were also at risk for leukemia, and the relationship between radiation dose and leukemia was linear (16). However, the effects of medical radiation such as RAIT on hematopoietic malignancy have not been well studied. Rubino et al. reported the relationship between cumulative RAIT dose and leukemia in a European cohort study; however, the number of patients in each subgroup was relatively small (n=6,841) and did not include the entire patient population with thyroid cancer in one country, which might have led to a selection bias in their results (11). Kim et al. reported an elevated risk of leukemia with a rising tendency of RAI usage using the SEER database; however, information about the doses of RAIT was lacking in the study (12).
Herein, we investigated the association between RAIT and the development of leukemia in patients with thyroid cancer in the context of current practice using the National Health Insurance (NHI) database in Korea, which covers the entire population of the country.
Methods
Data source
Data were obtained from the NHI database of Korea. The NHI is the only public medical insurance system in Korea and is operated by the Ministry for Health, Welfare, and Family Affairs. The NHI database is believed to represent the entire Korean population because of the compulsory social insurance system that is required by law. All clinics and hospitals in Korea submit data on inpatients and outpatients, including information on diagnosis and medical costs, to the NHI to claim payments for patient care. This database is provided by the Korean Health Insurance Review and Assessment Service (HIRA), which has been established to build an accurate claim review and quality assessment system for the NHI (17,18).
Study population
The database identified 211,360 patients newly diagnosed with thyroid cancer between January 1, 2008, and December 31, 2013, with a total 542,845 PY follow-up. Thyroid cancer is classified with code C73.9 according to the International Classification of Diseases, 10th edition (ICD-10) (19). As the database does not include information about thyroid cancer histopathology, operational definitions were used to identify the actual subjects who had thyroid cancer. The operational definitions for patients with thyroid cancer were as follows: (1) inpatients who had undergone curative thyroid surgery, and (2) inpatients who had undergone less than a total thyroidectomy and claimed for a coding of thyroid cancer. To include only patients with newly diagnosed thyroid cancer during the study period, subjects who had prior thyroid cancer before this study began were excluded using these criteria: (1) inpatients who had satisfied the proposed operation definitions for thyroid cancer before the study period, (2) inpatients with a coding of thyroid cancer before the study period, and (3) outpatients who had claimed for a coding of thyroid cancer at least four times before the study period.
The ICD-10 leukemia classifications are C91 for lymphoid leukemia, C92 for myeloid leukemia, C93 for monocytic leukemia, C94 for other leukemias of specified cell type, and C95 for unspecified leukemia. Among subjects who satisfied operational definitions for thyroid cancer, inpatients with a coding of leukemia identified after surgery for thyroid cancer were defined as subjects of secondary leukemia. The exclusion criteria of leukemia were: (1) inpatients who had fulfilled operational definitions for leukemia before the study period, (2) outpatients who had claims coded for leukemia at least four times before the study period, and (3) patients diagnosed with leukemia before initial treatment for thyroid cancer or the first RAIT.
A single dose of (131I) RAI less than 25 mCi was arbitrarily defined as the dose for diagnostic purposes. To calculate the cumulative amount of RAIT for each patient, a single dose of RAI ≥25 mCi was included. To clarify the relationship of RAIT and the development of leukemia, patients were categorized into five groups according to the cumulative dose of RAI: (1) no RAI, (2) low-dose RAI (≤30 mCi), (3) moderate-dose RAI (31–100 mCi), (4) high-dose RAI (101–150 mCi), and (5) very high-dose RAI (>150 mC). Follow-up duration was calculated from the date of thyroid surgery in patients without RAIT, from the date of the initial RAI administration in patients with RAIT. The Institutional Review Board at Samsung Medical Center approved this study.
Statistical analysis
Groups were divided for analysis according to the cumulative dose of RAIT. Cumulative incidence of leukemia is presented as the number of events per 100,000 PY with 95% confidence intervals [CI], and Poisson distribution was used to calculate the CI. Estimates of the cumulative incidence of leukemia in each group were based on the Poisson distribution over a 6-year period as well as at 3-month intervals. The cumulative incidence was calculated from the date of thyroid surgery in the no RAI group, or the first date of RAIT in the RAIT groups. The hazard ratio (HR) between two groups of interest during follow-up was calculated using Cox proportional-hazards regression with adjustment for age and sex. Chi-square tests for trend were used to identify the association between RAIT dose and the development of leukemia. A p-value less than 0.05 was considered significant. All analysis was conducted using statistical software R version 2.15.3 for Windows (
Results
Patient characteristics
A total of 211,360 patients were newly diagnosed with thyroid cancer according to operational definitions during the study period. The number of patients per year was 25,437 in 2008; 30,582 in 2009; 33,081 in 2010; 38,310 in 2011; 42,702 in 2012; and 41,248 in 2013. Women accounted for 82% (n=174,201) of all patients. The mean age at diagnosis of thyroid cancer was 48 years and the median for follow-up duration was 877 days. Nearly one-half of the patients (49%, n=103,741) underwent RAIT with a median cumulative dose of 100 mCi. The doses and frequencies of RAIT for each group and other details are presented in Table 1.
The follow-up period was calculated from the date of thyroid surgery in patients without RAIT and from the date of the initial RAIT in patients with RAIT.
The chi-square test for trend showed a significant association between RAIT dose and the development of leukemia (p=0.001).
The hazard ratio was calculated by comparing each RAIT dose group to the reference, which is the no-RAI group.
p<0.001.
p=0.025.
CI, 95% confidence interval; No., number; PYR, person-years at risk; RAIT, radioactive iodine therapy.
Association of radioactive iodine therapy and leukemia
During the study period, 72 cases (0.03%) of leukemia occurred among the 211,360 patients with thyroid cancer. Twenty-six cases of leukemia were identified in the no RAI group, while 46 cases of leukemia were identified in the groups with RAIT (HR 1.68 [CI 1.04–2.72], p=0.03) (Table 1, Fig. 1).
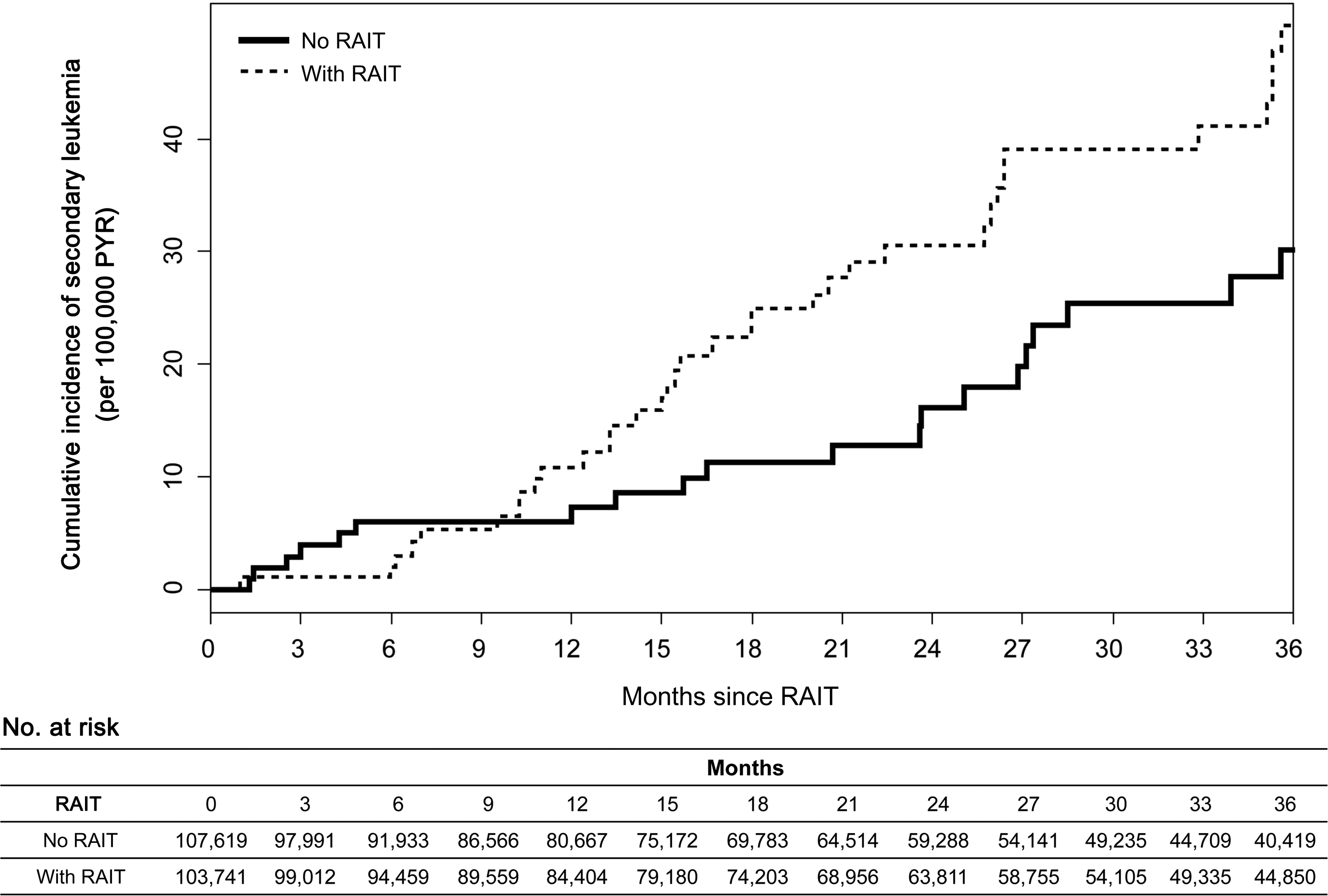
Cumulative incidence of leukemia during the follow-up period by the presence of radioactive iodine therapy (RAIT). Follow-up period was calculated from the date of the first RAIT administration. In subjects without RAIT, the starting point was the date of thyroid surgery. Number at risk means the number of subjects who were censored in each period. No., number; PYR, person-years at risk.
To assess the relationship between doses of RAIT and the development of leukemia, HR was calculated according to the cumulative dose of RAIT. The development of leukemia was significantly elevated in the high- and very high-dose groups, as compared with the group without RAIT (HR 3.09, [CI: 1.74–5.51], p<0.001, and HR 2.08, [CI 1.09–3.94], p=0.025). In addition, the risk of leukemia was higher in those with RAIT at a dose >100 mCi than patients without RAIT (HR 2.55 [CI 1.54–4.23], p<0.001) (Fig. 2). However, the low- and moderate-dose RAIT groups did not show a statistically significant association with the development of leukemia (Table 1). The chi-square test for trend showed a significant association between RAIT dose and the development of leukemia (p=0.001). The cumulative risk for the development of leukemia increased significantly in patients with RAIT at >100 mCi as early as 9 months after RAIT compared with the no RAI group in the same period (HR 3.08 [CI 1.76–5.37], p<0.001) (Fig. 2).
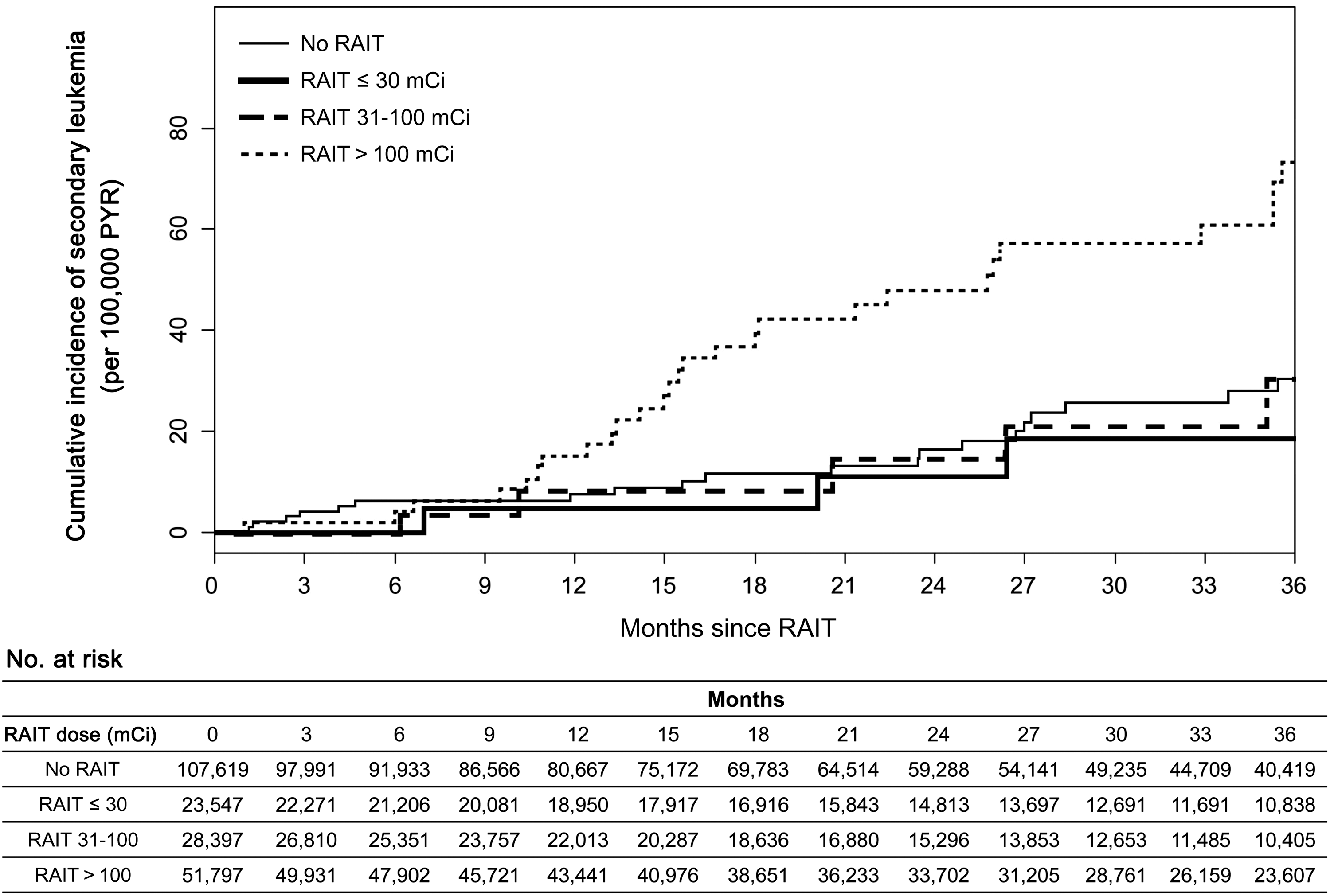
Cumulative incidence of leukemia during the follow-up period according to the cumulative dose of RAIT. Follow-up period was calculated from the date of the first RAIT administration. In subjects without RAIT, the starting point was the date of thyroid surgery. Number at risk means the number of subjects who were censored in each period.
Discussion
Our data conforms to the hypothesis that RAIT in patients with thyroid cancer is associated with the development of leukemia when using a nationwide, population-based database, which at 542,845 PY is the largest study that we are aware of. In this study, we found a strong association between RAIT and leukemia, especially in the high- and very high-dose groups who received RAI exceeding 100 mCi (HR 2.55, p<0.001), while there were no statistically significant associations in the low- and moderate-dose groups who received up to 100 mCi. These results are consistent with the previous report by Rubino et al. who reported an increased risk of leukemia in a European cohort (PY=77,955) with a relative risk (RR) of 4.3 in RAIT groups at a dose between 3.7 and 15.4GBq (100–500 mCi) (11).
Leukemogenesis and secondary leukemia have been well demonstrated in survivors of nuclear accidents (14,15,20). Chernobyl cleanup workers who were exposed to a relatively low dose of external ionizing radiation, mainly gamma and x-rays, also had increased risks for hematologic malignancies and the excess relative risk of total leukemia was shown to be 3.44 per Gray unit (16). Several investigators also reported the possible harmful effects of natural background radiation such as radon or gamma radiation on the risk of childhood leukemia (21,22).
Unlike external radiation, RAI is a beta-ray emitter that is an uncommon cause of leukemia. Earlier studies reported that leukemia occurred after a total dose of more than 800 mCi and within a short interval between 2 and 6 months (10,23).
However, recent epidemiological studies have suggested that the occurrence of leukemia is prevalent even after exposure to lower RAIT doses (11,13). A meta-analysis by Sawka et al. reported that the RR of leukemia is significantly increased in patients with RAIT with a RR of 2.5 [CI 1.13–5.53], although they did not provide information on RAIT dose (13). Rubino et al. reported a RR of 4.3 [CI 0.7–34.9] for RAIT at a dose between 100 mCi and 500 mCi and a linear dose-response relationship with an excess absolute risk of 0.8 leukemias per GBq using a European cohort (11). However, Rubino et al. did not find a significant association below a 100 mCi dose. In this study, we also showed that RAIT at more than 100 mCi was associated with the development of leukemia with a HR of 2.55 [CI 1.54–4.23] (p<0.001) when compared with the no RAI group. We also demonstrate a dose-response relationship between RAIT dose and the development of leukemia by a chi-square test for trend (p=0.001). Interestingly, we did not observe an increased risk of leukemia in RAIT groups with a dose ≤100 mCi, findings that are consistent with the observation of Rubino et al. (11).
The results reported here, however, do not indicate that RAIT up to 100 mCi is safe from the perspective of developing leukemia because the CIs overlap. The dose–response relationship is supported by the linear no-threshold model, which is generally accepted for its relevance between radiation and carcinogenesis (14,24), and cancer risk is known to increase 0.05-fold for every 100 mSv increase. Although no statistically significant increase in the number of cancer cases has been observed below 100 mSv, the carcinogenic risk at even lower levels remains unclear (24). One plausible explanation is that the latency period for leukemia development in low-dose groups is longer than the latency period for high-dose groups. Given the relatively short follow-up of this study, we might have missed excess cases at low-dose RAIT exposures, which would become more evident with a longer follow-up. As for the late effects of radiation exposure, the excess risk of developing leukemia has been reported within 5 years after exposure, whereas the risk is around 10 years for solid cancers. Generally, the excess risk of leukemia markedly declines with time since radiation exposure (14).
Another possible explanation is that there could actually be a threshold RAIT dose in developing leukemia, possibly between 100 mCi and 150 mCi based on the results of this study.
However, the possibility of a threshold dose for developing leukemia was difficult to analyze because the RAIT doses are typically decided empirically and not by a dosimetric approach. Thus, the most frequently used doses were 30 mCi, 100 mCi, and 150 mCi. Therefore, we had to use RAIT doses based on categorical variables instead of linear variables. Moreover, the radioactivity of absorbed 131I may affect different organs to different degrees according to the distance from remnant thyroid tissue to target organ, type of target organs, and the percentage of 131I renal excretion. Therefore, the same dose of RAI may have a different radiation effect on the hematopoietic system in each individual.
Leukemia has been considered a late adverse effect of exposure to RAIT (25,26) and thus many studies on this issue excluded the development of leukemia within two years after RAIT in their analysis (11,13). However, we found that a statistically significant increase in the development of leukemia started as early as nine months. We suspect that the increase of leukemia in patients with RAIT is a real increase rather than a surveillance effect because the incidence remained stable until eight months after RAIT. In addition, thyroid cancer patients undergoing RAIT are not exposed to other medical irradiation treatment any more frequently than patients without RAIT based on clinical practice patterns in Korea. Thus, our results show that the radiation effect of RAIT on leukemia risk develops earlier than previous studies proposed and as early as nine months after RAIT. The plausible explanation for this early development of leukemia is as follows. The formation of oxidative stress is a main mechanism for both the therapeutic and side effects of RAIT. Exposure to RAI leads to oxidative stress via the generation of reactive oxygen species (27). Reactive oxygen species induce the peroxidation of lipids, which results in structural and functional damage to the cellular membrane, DNA strand breakage, and DNA base alterations (27,28). The frequency of micronuclei in the peripheral blood, which is an indicator of breaks in the chromosome, has been shown to increase as early as 2 days, peaks at 7 days, and slowly returns to the baseline frequency over 6–12 months after RAIT (29,30). Insufficient repair of potent chromosomal damage may lead to cancer development after radiation injuries (27,31). Although several large epidemiologic studies, including our study, did not prove that genetic instability was related to RAIT, chromosomal changes might induce leukemia even in the early periods after RAIT.
According to data from Statistics Korea (
Factors influencing the increased risk of developing leukemia, even in patients with thyroid cancer without RAIT, include genetic and environmental factors, as well as surveillance bias, which could affect the development of leukemia in patients with thyroid cancer during follow-up. Genetically, specific single nucleotide polymorphisms (SNPs), such as the MDM2-reference SNP 2279744 (rs2279744) were associated with an elevated risk of thyroid cancer and leukemia (32). A shared genetic susceptibility or unknown exposure to hazardous environmental materials might be possible causes for the occurrence of multiple malignancies. In addition, surveillance bias should be considered as another attributing factor. Surveillance bias is derived from an effort to find other health problems via frequent check-ups in subjects with cancer. Prior studies demonstrated a significantly elevated risk of secondary cancers around the time of diagnosis of thyroid cancer (2,33). However, Brown et al. reported that an increased risk of leukemia was maintained even with the exclusion of a three-year latency period (33), which meant surveillance bias was not a determinant factor of the increased risk of leukemia. Our previous report also suggested that the pattern of elevated risks in specific cancers was similar across the study period, although the latency period became shorter in patients who were recently diagnosed with thyroid cancer (2).
Subjects treated with low-dose RAI did not show an elevated risk of secondary leukemias, at least in the early period after RAIT. In recent years, the majority of thyroid cancer cases have consisted of small tumors (T1) (34), and the survival benefit of RAIT has not been proven in low- and intermediate-risk groups. Current guidelines published by the American Thyroid Association recommend a minimum dose of RAI at 30 to 100 mCi to achieve successful remnant ablation for low-risk patients (35). Two randomized trials, the HiLo (36) and the ESTIMABL (37) trials, formally showed that a success rate of ablation was not inferior in low-dose RAI (30 mCi) groups compared with high-dose RAI (100 mCi) groups. Furthermore, a recent study reported no difference in long-term outcomes in patients treated with low-dose RAI (30 mCi) (38). Beyond treatment outcomes, the adverse effects of RAIT should also be considered. Even the absolute number of secondary leukemia cases was small in thyroid cancer patients with RAIT, but subjects with high-dose RAIT that exceeded 100 mCi had a significantly elevated risk of leukemia (HR 2.55, p<0.001), whereas the low- to moderate-dose groups (equal to or less than 100 mCi) did not. It is worth noting that the occurrence of leukemia should be considered as a serious comorbidity in survivors of thyroid cancer because patients with thyroid cancer have an excellent prognosis in terms of survival. Therefore, physicians need to weigh the risks and benefits of each RAIT dose, especially in patients with low risk thyroid cancer; only when the clinical benefits outweigh the small but absolute risks of leukemia should RAIT be considered.
There are some limitations to this study. First, enrollment in the study was done through operational definitions rather than pathologic diagnosis using the NHI (HIRA) database, because the NHI (HIRA) database is based on ICD-10 coding system for each payment claim. Although a quality assessment system for accurate claims has been well established, the database does not include information on histopathology. Therefore, we adopted operational definitions for identifying patients with thyroid cancer and leukemia. This might lead to under- or overestimation of the total number of patients. However, considering that the NHI is compulsory by law, it covers all residents without exception, and there are very few patients undergoing treatment abroad for thyroid cancer and leukemia; therefore, the chance of underestimation appears trivial. Furthermore, we compared the number of patients identified by operational definitions to the yearly number of patients registered in the Korea Central Cancer Registry, which is a well-established cancer registry based on patient histopathology, and found very similar incidence rates each year between the two databases (data not shown). Thus, we are quite confident that the operational definitions worked well in finding cases of thyroid cancer and leukemia. Second, the duration of follow-up for the study was relatively short. According to the NHI (HIRA) policy, which was established for accurate claim reviews and quality assessment, the database was not maintained after reviewing claims in order to protect personal information until 2006. Since 2007, information for claims has been organized for safe data storage, and therefore the follow-up duration was up to six years in the present study. Because some types of leukemias are reported that the elevated risk of carcinogenesis persists over 50 years after exposure in atomic bomb survivors (14), we cannot exclude the risk of late occurrence of leukemias. However, the excessive risk of most secondary leukemias declines markedly with increased time since radiation exposure (14), and it is predicted that the risk of leukemia in later periods might be less than that of the period within the first five years after RAIT. Additionally, the total follow-up of 542,845 PY, which is the highest ever according to review of the relevant literature, could compensate for the weakness of a relatively short follow-up period. For example, a European report used a follow-up of 77,956 PY to identify cases of leukemia in patients with thyroid cancer (11), and another large study using the SEER database presented a 408,750 PY follow-up of subjects in their analysis (5). Third, we included all patients with thyroid cancer rather than only differentiated thyroid cancer, which might benefit from RAIT after thyroid surgery because the NHI database did not have information on histopathology. However, a recent Korean report regarding the histological classification of thyroid cancer showed that over 98% of new cases of thyroid cancer are patients with differentiated thyroid cancer (2,39); therefore, this limitation should have little effect on the study results.
In conclusion, we report a significant association between RAIT in patients with thyroid cancer and risk of leukemia development during follow-up using a nationwide population-based database. However, an association with leukemia was only evident when the dose of RAIT exceeded 100 mCi with the HR of 2.55 compared with patients without RAIT. RAIT up to 100 mCi did not show an increase in the development of leukemia. Considering the very favorable prognosis of most thyroid cancers and the inherent adverse effects of RAIT, physicians need to consider the pros and cons of RAIT before treatment. However, these findings should not contraindicate RAIT in patients with thyroid cancer for whom therapeutic benefit is expected.
Footnotes
Author Disclosure Statement
No competing financial interests exist.