
Abstract
Background:
Vascular malformations and hemangiomas of the thyroid gland are rare disorders. The first case of a patient with recurrent high-flow arterio-venous malformation of the right thyroid gland involving the right endolarynx is presented.
Patient findings:
In June 2013, a 42-year-old female patient presented to the surgical department with recurrent hoarseness and a soft, vibrating mass on the right side of her neck. In 1993, she underwent right subtotal hemithyroidectomy with embolization on the day before surgery for a high-flow arterio-venous malformation of the thyroid gland. Diagnostic work-up in 2013 demonstrated a complex recurrent high-flow arterio-venous malformation on the right side of her neck involving the endolarynx. Full function of the right vocal fold could not be ascertained. The lesion was embolized again and excised the following day. Intraoperative gross bleeding and scar tissue prevented visualization and monitoring of the recurrent laryngeal nerve. Gross bleeding was also noted on hemithyroidectomy after embolization in 1993. No therapy was needed for the endolaryngeal part of the lesion. Histology showed large arterio-venous malformations with thyroid tissue. She remains well without signs of recurrence 18 month later but with a definitive voice handicap.
Summary:
This is the first report of a recurrent high-flow arterio-venous malformation originally developing from the right thyroid gland involving the right endolarynx. Counseling, diagnostic, and therapeutic work-up of the patient was possible only with an interdisciplinary team. The endolaryngeal part of the hemangioma dried out after embolization and completion hemithyroidectomy. Her hoarseness has greatly improved but a definitive voice handicap remains.
Conclusion:
High-flow arterio-venous malformations of the thyroid gland are a rare disease, and recurrent lesions have not been reported. Interdisciplinary management of these patients is mandatory due to the complex nature of the underlying pathology. Recurrence might develop after long free intervals.
Introduction
O
Patient
In June 2013, a 42-year-old physiotherapist presented to the department with symptoms of increasing hoarseness, exertional dyspnea, laryngeal globus sensation, and dysphagia. A nontender, soft, vibrating mass was palpable in the right side of her neck with a barely visible scar from a previous subtotal hemithyroidectomy. Physical examination was otherwise unremarkable with no signs of asymmetry. Her general condition and appetite were good. Her body mass index was 23 kg/m2. She denied night sweats or recent weight loss.
Past Medical History
The patient's medical history includes essential hypertension and treatment for hyperthyroidism in 1989. She underwent a subtotal right hemithyroidectomy together with the lobus pyramidalis in 1993 for a benign arterio-venous malformation. A few months before surgery in 1993, she had infectious mononucleosis. Her symptoms in 1993 were similar, with increasing hoarseness and palpable vibration in the right side of her neck. A preoperative magnetic resonance imaging (MRI) scan suggested a high-flow arterio-venous malformation. Angiography indicated continuity of the hemangioma into the larynx, but laryngoscopy did not reveal any alterations.
The day before surgery, embolization with “Fibrospum-particles” (fibrin sponge particles) was carried out. Despite embolization, intraoperative gross bleeding was noted in the surgical records, and the patient required two units of red packed cells after surgery. Postoperative laryngoscopy showed thickening and inflammation of the right vocal cord without signs of recurrent laryngeal nerve impairment. Her hoarseness improved, and she had no problems working as a physiotherapist, which included loud talking to her elderly and often deaf clients.
Reassessment of her past medical history revealed angioma-like bluish skin lesions of her forearms during puberty with spontaneous regression before the age of 20. Her family history did not reveal any hereditary or chronic diseases. Biopsy of the lesion in her neck had never been attempted. There was no history of trauma to her neck. A follow-up MRI in 1998 was unsuspicious. However, a follow-up MRI in 2002 (Fig. 1A) demonstrated recurrence of an angiomatoid tumor. Until then, the patient was asymptomatic.
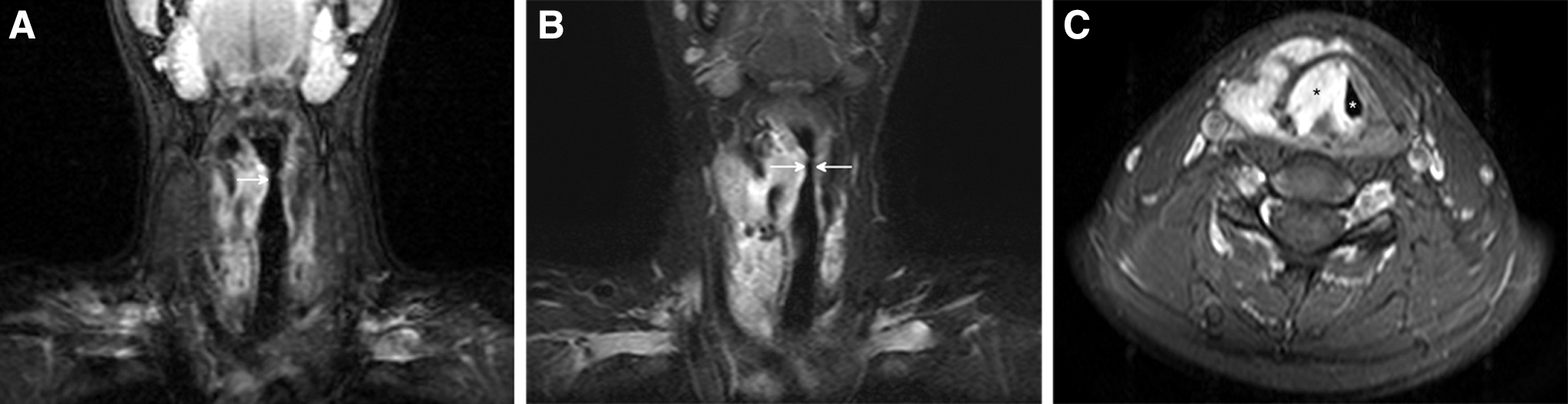
Magnetic resonance imaging (MRI) scans 2002 and 2013 with recurrent arterio-venous malformation. (
In 2006, laryngoscopy (see corresponding case report in VideoEndocrinology [10]) evidenced development of a bulging mass from her right Morgagni fossa. According to a repeat MRI and ultrasound in 2006, this was interpreted as a recurrent angioma of the right endolarynx and neck. After 2008, laryngoscopy showed laryngeal penetration with saliva and retention of mucus in the right piriform sinus.
Recent Medical History
In May 2013, she was referred to an endocrine specialist and for an MRI by her general practitioner (GP) for a two-month history of increasing hoarseness. Since 2000, the patient was treated with levothyroxine for hypothyroidism. Ultrasound of the neck showed recurrence of a vascularized mass on the right. Outpatient scintigraphy excluded autonomy of the thyroid (technetium uptake 0.19%), and her thyrotropin was slightly depressed on levothyroxine therapy, but thyroid function tests were otherwise normal. A thyroiditis screen was negative. Parathyroid hormone and calcium levels were normal. The MRI (Fig. 1B and C) showed a large, diffusely growing angioma characterized by early contrast agent uptake already at the beginning of the arterial phase with a tumor-blush and arterio-venous shunts. Laryngoscopy showed an unchanged appearance of the mass at the right endolarynx. Decreased right vocal cord function was evident, and the patient complained of increasing hoarseness and foreign body sensation. She refused further assessment or interventional therapy and requested excision of the lesion. Prior to surgery, gastro-esophageal regurgitation disease was excluded, as well as disturbance of esophageal motility, osteophytes of the neck, and other reasons for dysphagia and globus sensation. At that time, her medication included angiotensin-II receptor antagonists, a beta-blocker, and levothyroxine.
Surgery
In August 2013, the patient underwent embolization of the lesion followed by surgical excision one day later. On completion hemithyroidectomy, no clear boundaries were detected. Instead, extensive scar tissue, freshly thrombosed tissue after effective embolization and nonembolized soft, grossly bleeding paratracheal tissue on the right was resected. The left part of the thyroid gland was palpable in a rather hard fibrous capsule and not resected. No signal was obtained with repeated intraoperative neuromonitoring via the vagus nerve and the right recurrent laryngeal nerve. Surgical treatment of the endolaryngeal extension of the hemangioma was not attempted. Recovery from surgery was unremarkable, and the patient left the hospital two days after surgery, with minor limitations of phonation.
Follow-up
In the weeks that followed, the patient experienced an inflammatory reaction of her right endolarynx with severe hoarseness (see report in VideoEndocrinology [10]). She underwent an intensive voice rehabilitation program. Laryngoscopy showed a diffusely red, edematous, and fixed right vocal cord in median position. The patient was seen several times after the procedure in the otolaryngology department with the bluish angioma on her right vocal cord still visible. Regression of the endolaryngeal angioma was first noted two months after surgery. Ten months after surgery, the patient continued to have a significantly reduced vocal capacity, and exertional dyspnea continued to be a problem without objective signs of impairment of lung function. No stridor at rest was audible. One year after surgery, the right vocal cord swelling and inflammation had significantly reduced. The vocal cords now were of porcelain color on both sides. There was respiratory loss of function of the right vocal cord, with normal function of the left vocal cord. The edema of the right sinus piriformis decreased with only a small amount of mucus retention. It remained unclear whether dysfunction of the right recurrent laryngeal nerve was due to the completion hemithyroidectomy or a result of chronic compression and inflammation of the right endolarynx pre- and postoperatively.
Histopathology
The primary resection received by the pathology department in November 1993 was 4.0 cm×3.0 cm×1.3 cm with a weight of 12 g, as well as a lobus pyramidalis of 1.5 cm×1.0 cm×1.0 cm. The larger specimen consisted of thyroid glandular tissue with extensive venous and arterial blood vessels, the latter being predominantly thrombosed after embolization (Fig. 2A and B). The lobus pyramidalis did not show thyroid tissue but rather skeletal muscle, fatty and connective tissue with arterio-venous malformation. A histological diagnosis of angioma racemosum was made.
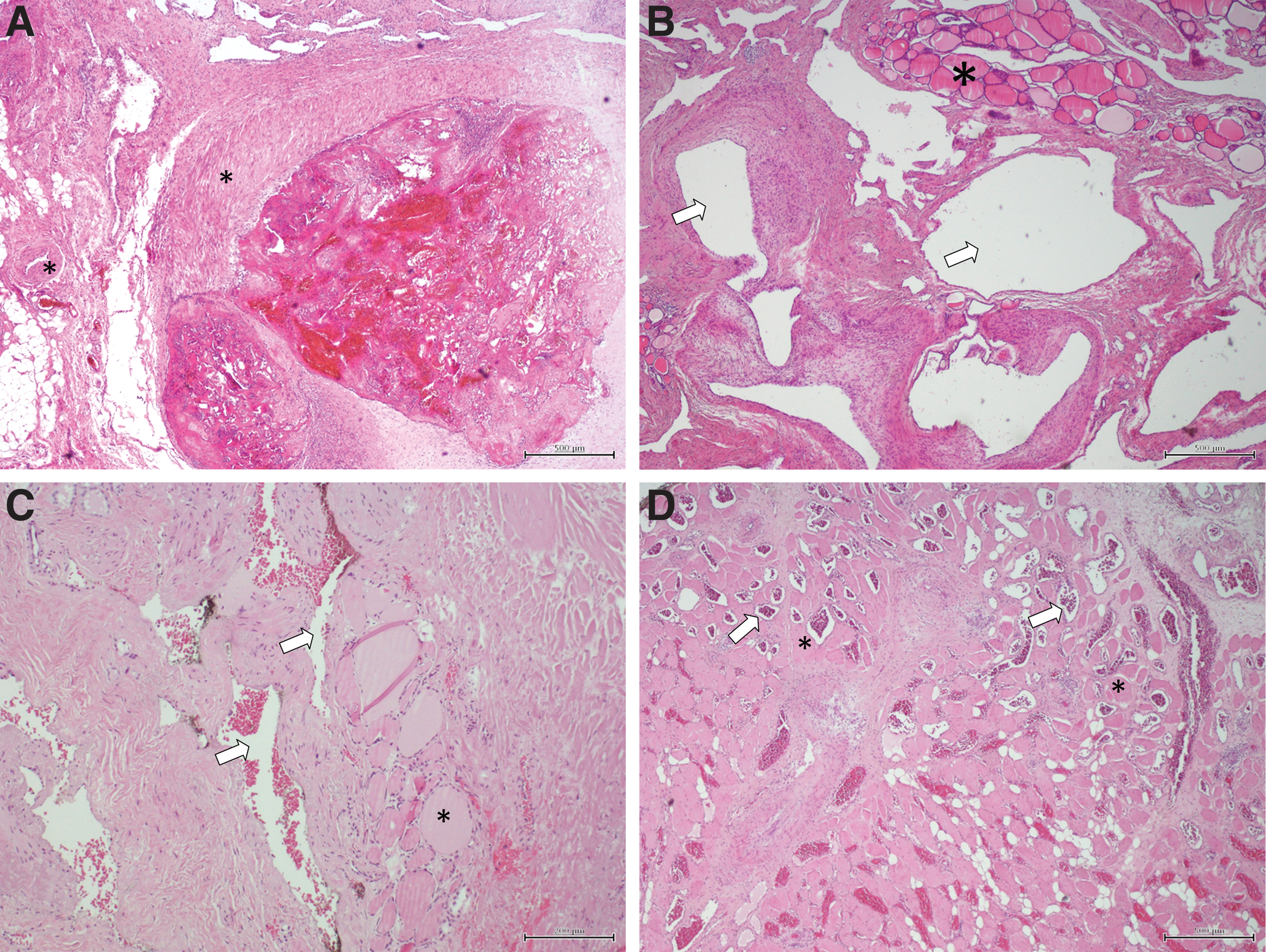
Histology of arterio-venous malformation 1993 and 2013. (
The recurrent surgical specimen received in the pathology department in August 2013 was 7.5 cm×3.0 cm×1.3 cm with a weight of 16.5 g and therein a 2.5 cm diameter, inhomogeneous nodule with reddish-brown cut surface. Microscopy revealed only few thyroid follicles surrounded by irregular arterial, venous, and cavernous vascular channels (Fig. 2C and D). A macroscopic nodule was consistent with a large parathyroid gland and therein extensively anastomosing blood vessels (histology not shown). Surrounding soft tissue, including musculature, was also involved in the vascular malformation.
Discussion
This is the third case of an arterio-venous malformation of the thyroid gland, and the first report of a recurrent high-flow arterio-venous malformation of the thyroid gland presenting as a complex lesion involving the right side of the neck and endolarynx. The lesions reported by Lizarralde et al. have been considerably smaller and wel- circumscribed lesions. In comparison, the patient was characterized by a recurrent diffuse infiltrating angioma (1). From other pathological entities featuring increased vascularity, namely hemangiomas in children, the call for multidisciplinary diagnosis and treatment has been widely accepted (11,12). The same should apply for thyroid disease with increased vascularity. Moreover, these patients should predominantly be treated by specialist teams. This is especially true for arterio-venous malformations, which do have a high rate of recurrence after subtotal resection (13). Kang et al. reported recurrence of high-flow arterio-venous malformations in up to a third of patients (14). Buckmiller et al., reporting on their experience with the treatment of a vascular lesions and its molecular biology, characterized arterio-venous malformations as tumors exhibiting malignant features (15). Therefore, embolization followed by resection is an accepted treatment standard (11,16). The indication for embolization followed by resection is less clear in cases where radical resection cannot be achieved, as in the present case with endolaryngeal continuity of the hemangioma. In such circumstances, embolization of the hemangioma, together with a subsequent wait-and-see approach, should be considered as a treatment option for future cases. In case of a remaining hemangioma, the patient should be reassured to wait in order to assess whether there is a dry-out phenomenon. Remaining arterio-venous lesions can be reassessed and a repeat embolization attempted. Alternatively, surgery remains an option as further treatment modality.
Footnotes
Acknowledgment
Thanks to Samuel Somers-Heslam, Cambridge, United Kingdom, for grammar revision.
Author Disclosure Statement
None of the authors report competing financial interests.